
Differences in Ethical Viewpoints among Civilian–Military Populations: A Survey among Practitioners in Two European Countries, Based on a Systematic Literature Review

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Background
3. Materials and Methods
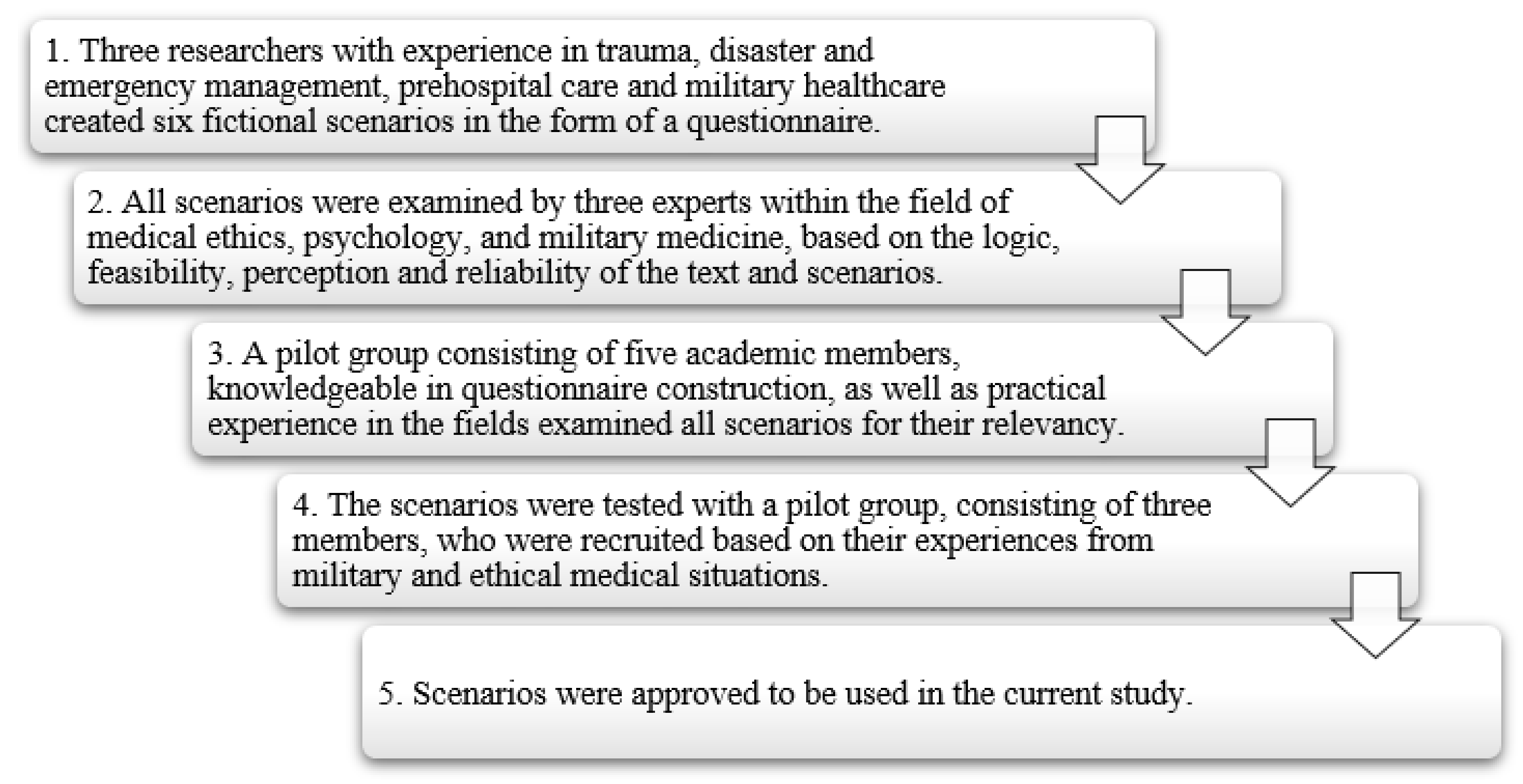
3.1. Design and Development of the Survey Tool
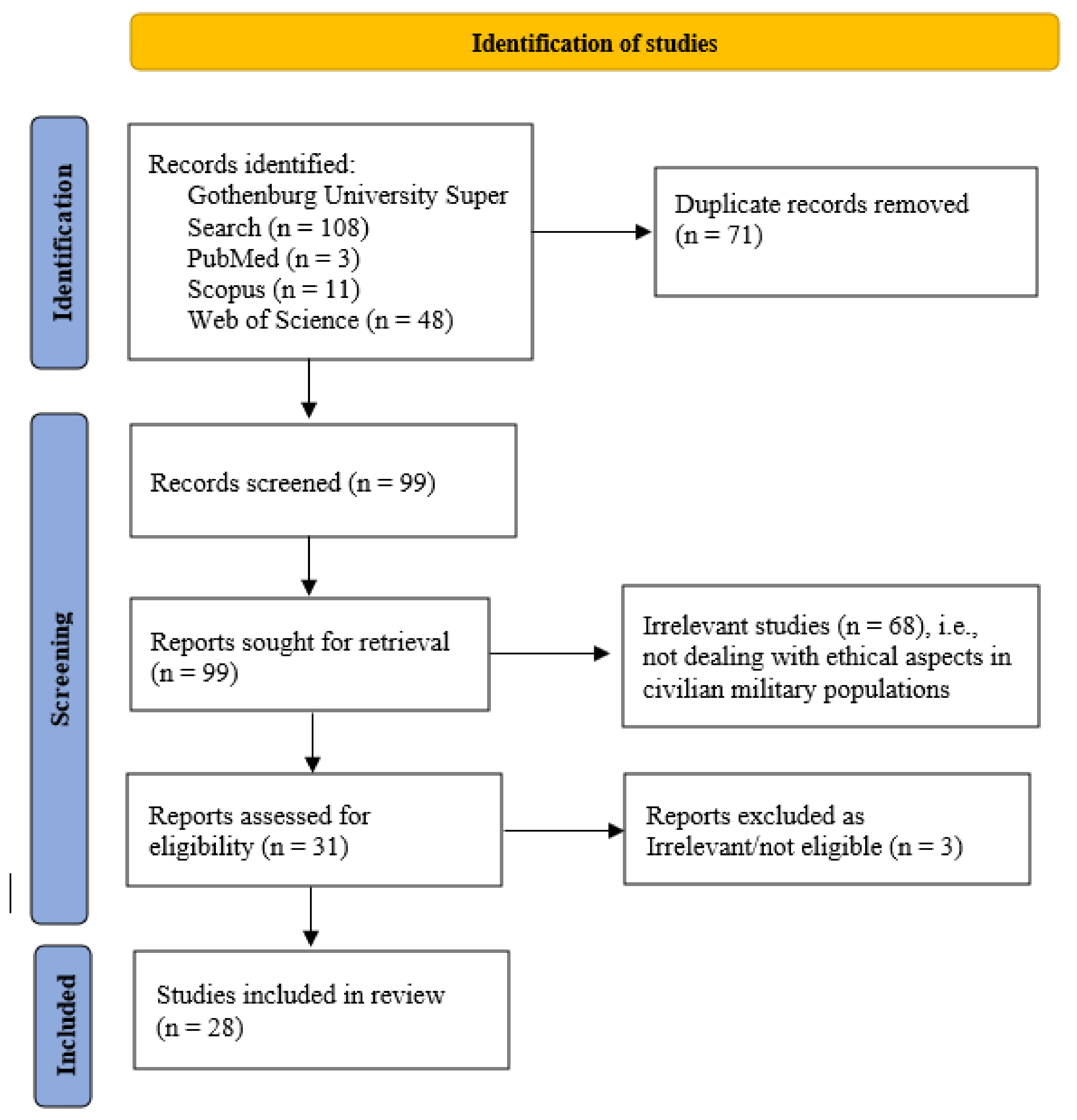
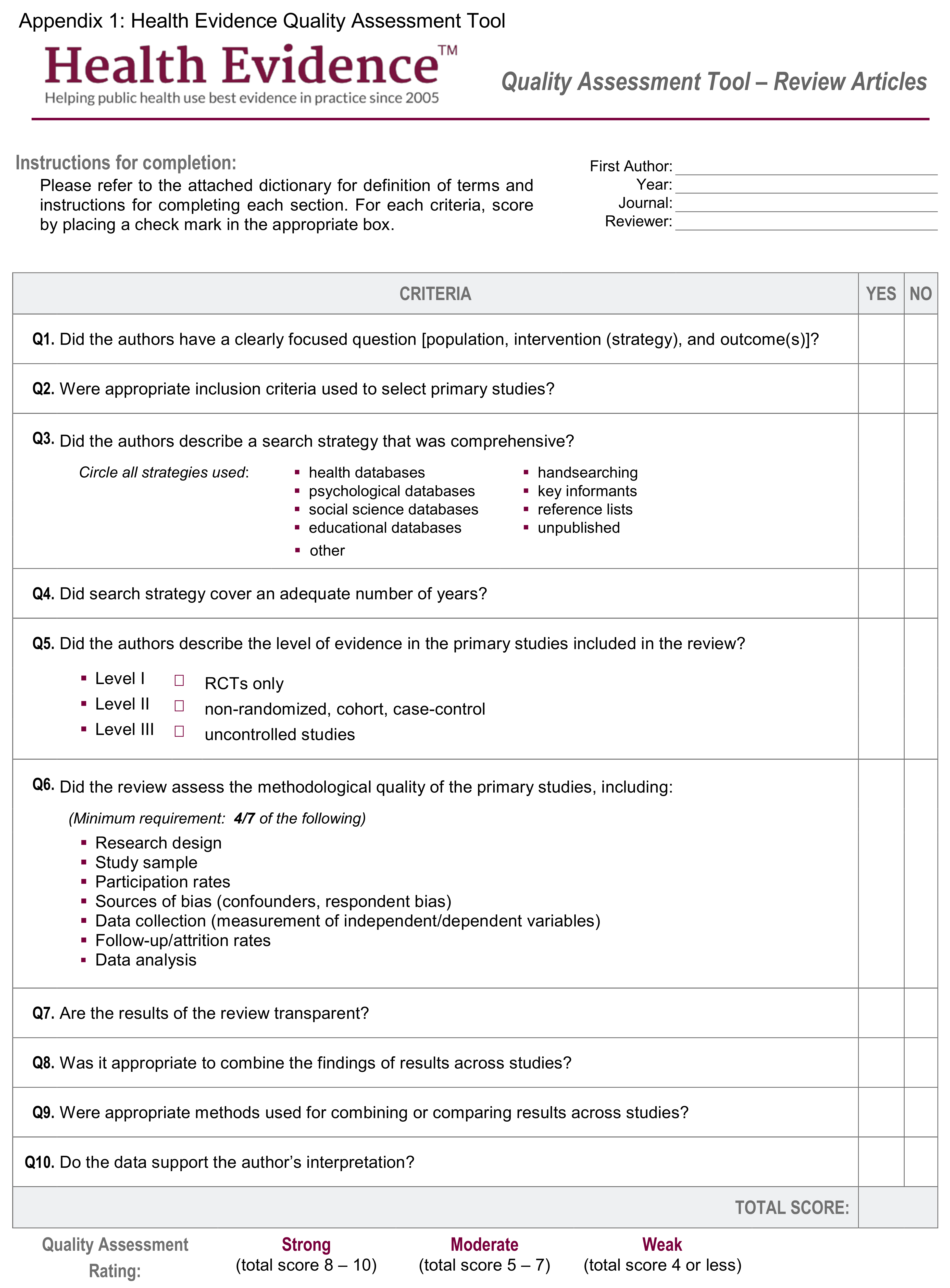
3.2. Identifying the Contents Necessary for Scenarios through a Systematic Literature Review
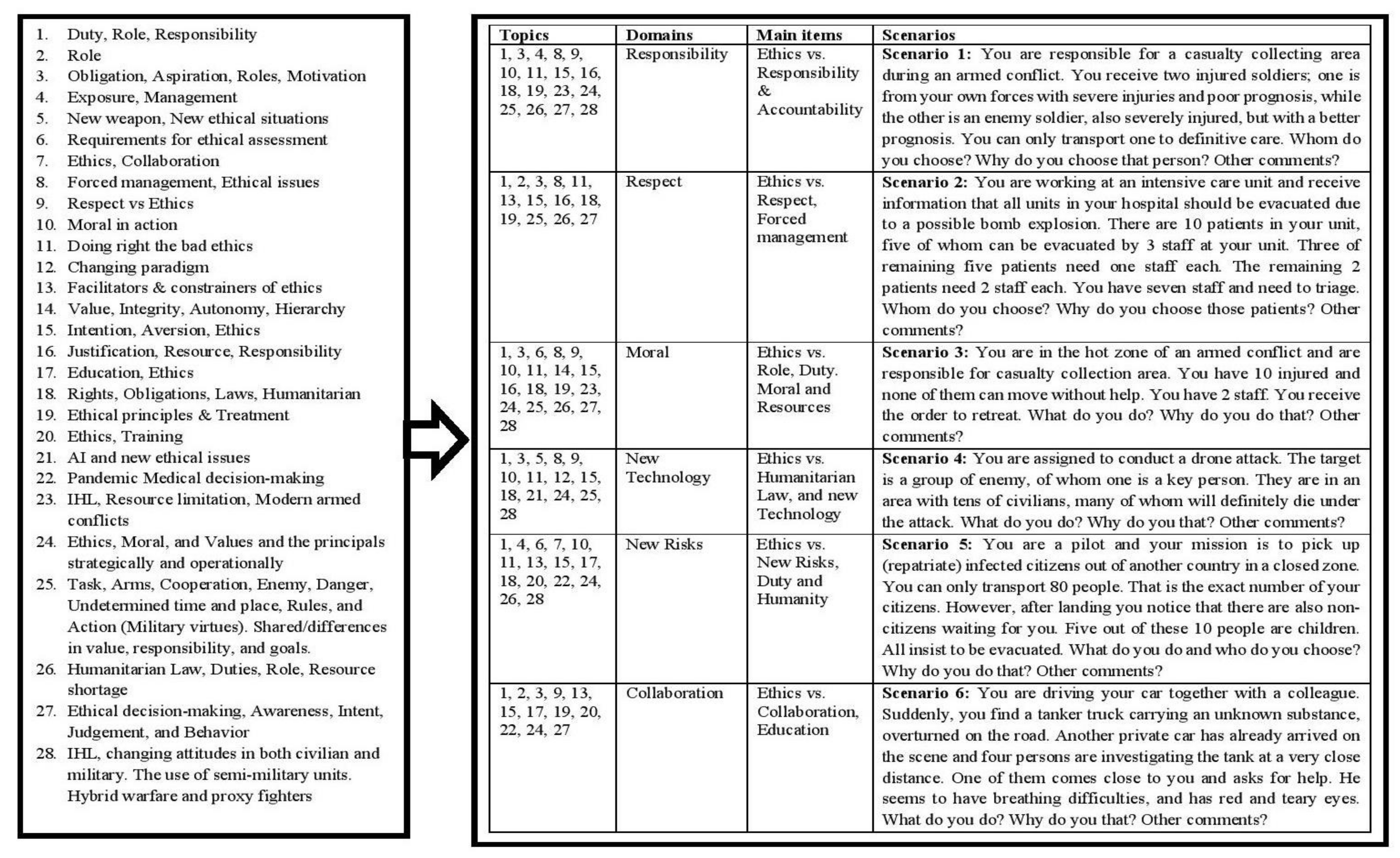
3.3. Identifying the Key Topics and Subjects for Each Scenario
3.4. Validating the Comprehensiveness of the Identified Content/Potential Scenarios
3.5. Face Validity of the Scenarios
3.6. Writing and Revising Scenarios
3.7. Scenarios
3.8. Testing Scenarios before the Main Study
3.9. Sample Population and Location
3.10. Questionnaire Distribution
3.11. Study Ethics
3.12. Statistical Analysis
4. Results
4.1. Summary of the Literature Review and the Core Findings
4.2. Online Survey—Summary of Findings—Main Results
4.3. Scenarios
5. Discussion
5.1. Theoretical and Practical Implication of the Study
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | QE | MA/Year/Country | Journal | Title | Topic/Main Scope | Items |
|---|---|---|---|---|---|---|
| 1 | S | O’Fallon, M.J., et al., 2005, USA | J Bus Ethics | A Review of the Empirical Ethical Decision-Making Literature: 1996–2003 | CE/A review summarizing the research on ethical decision-making from 1996–2003. Findings are summarized to high lighten the impact of dependent variable: awareness, intent, judgment, and behavior in ethical decision-making. | Awareness, intent, judgment, and behavior |
| 2 | M | Simonds, A.K., 2009, UK | Eur Resp J | Lives on the line. Ethics and practicalities of duty of care in pandemics and disasters. | CE/Highlighting the pandemic situation, focusing on health care duties’ ethical aspects and the roles of workforces and their safety. | Duty, Role Responsibility |
| 3 | M | Wiist, W.H., 2009, Canada | Am J Public Health | The role of public health in the prevention of war: rationale and competencies. | CM/The study described public health perspectives during war in support of public health. | Role |
| 4 | M | Jennings, P.L., 2011, USA | Mil Psychol | The Moralities of Obligation and Aspiration: Towards a Concept of Exemplary Military Ethics and Leadership | ME/The dynamics of military ethics based on two contrasting but complementary moralities—moralities of obligation and aspiration—and the two types of moral motivation, i.e., rule following and identity conferring. | Obligation Aspiration Roles, Motivation |
| 5 | S | Sousa, C., 2011, US | Global public health | Conflict, health care and professional perseverance: A qualitative study in the West Bank | CME/How military considerably affects civilians’ access to both urgent and preventive care by exposing healthcare providers to harassment and violence. | Exposure Management |
| 6 | W | Zehfuss, M., 2011, UK | Eur J Int Relation | Targeting: Precision and the production of ethics | CME/Praise for precision in producing Western warfare also reproduces a particular kind of ethics, based on the notion of non-combatant protection. | New weapon New ethical situations |
| 7 | M | Geale, S.K., 2012, Saudi Arabia | Disaster Prev manag | The ethics of disaster management. | CE/Emphasis on ethical management in disaster and emergencies and the need for disaster management system (communication, education and training, etc.). | Requirements for ethical assessment |
| 8 | S | Craft, J.L., 2013, USA | J Bus Ethics | A Review of the Empirical Ethical Decision-Making Literature: 2004–2011 | CE/A review summarizing the research on ethical decision-making from 2004 to 2011. Rest’s four-step model for ethical decision-making is used to summarize findings by dependent variable—awareness, intent, judgment, and behavior. A discussion of findings in each category is provided in order to uncover trends in the ethical decision-making literature. | Ethical decision-making, Awareness, Intent, Judgement, and Behavior |
| 9 | M | Hunt, M.R., 2014, Canada | Dev world bioethics | The Ethics of Engaged Presence: A Framework for Health Professionals in Humanitarian Assistance and Development Work. | CE/Health care professionals whose understanding and actions are consistent with the ethics of engaged presence develop, sustain and promote collaborative partnerships. | Ethics Collaboration |
| 10 | M | Rebera, A.P., 2014, Italy | Sci engin ethics | On the Spot Ethical Decision-Making in CBRN Response: Approaches to on the Spot Ethical Decision-Making for First Responders to Large-Scale Chemical Incidents | CE/The ethical issues in long-term CBRN experiences were noted as forced participation, forces restraint, triage by ‘gross’ criteria, assumed consent, forced decontamination, undermining dignity, assumed contamination, competing ambition, and full disclosure. | Forced management Ethical issues |
| 11 | W | Baker, G.H., et al., 2015, USA | Joint Force Quarter | Vertical and horizontal respect: a two-dimensional framework for ethical decision making | ME/Vertical respect (hierarchical line) and horizontal respect (human relationships), can together represent a practical framework in ethical decision-making. | Respect vs. Ethics |
| 12 | M | Lazar, S., 2015, USA | Ethics | Risky Killing and the Ethics of War | CME/The moral distinction of killing between civilian and soldier in wars. | Moral in action |
| 13 | M | Mileham, P., 2016, US | Defense Scur analysis | Human conflict and universal ethics (part 2) | CME/Focus on the difficulties of conceiving what is good theoretically, and doing what is right practically in armed conflicts. | Doing right the bad ethics |
| 14 | M | Weiss, T.G., 2016, USA | Glob Policy | Ethical Quandaries in War Zones, When Mass Atrocity Prevention Fails | CME/Focus on moving away from input and output-based decisions towards outcomes. | Changing paradigm |
| 15 | S | Young, S.S., 2016, USA | Glob Qual Nurs Res | Conflict and Care: Israeli Healthcare Providers and Syrian Patients and Caregivers in Israel. | CE/Supportive and hindering systemic elements contributing to the healthcare provider-patient-caregiver relationship. | Facilitators & constrainers of ethics |
| 16 | M | Rochon, C., 2016, Canada | J Law Med Ethics | Are Military and Medical Ethics Necessarily Incompatible? A Canadian Case Study. | CME/Focus on the overlap of the military and medical ethics in terms of integrity and values. Physicians’ autonomy and soldiers’ hierarchal line. | Value, Integrity Autonomy Hierarchy |
| 17 | W | Bywater, M., 2017, UK | J Int Human Legal Stud | Classical and Political Humanitarianisms in an Era of Military Interventionism and the War on Terror | ME/The changes in belligerents’ response to armed conflicts and how the intention, documentation, and reporting of violence will bolster military intervention. | Intention Aversion Ethics |
| 18 | S | Leider, J.P., 2017, USA | Am J Public Health | Ethical guidance for disaster response, specifically around crisis standards of care: a systematic review. | CE/The crisis standard of cares in disaster focused on ethical justification in triage, preparation responsibilities, resources, and social utilities. | Justification Resource Responsibility |
| 19 | S | Burkle, F.M., 2019, USA | Disaster Med Public Health Prep | Health Care Providers in War and Armed Conflict: Operational and Educational Challenges in International Humanitarian Law and the Geneva Conventions, Part II. Educational and Training Initiatives | CME/Utilizing a historical framework addressing the transformation of the education and training of humanitarian health professionals from the Cold War to today and future recommendations. | Education Ethics |
| 20 | W | Schussler, L., 2019, USA | JAMA surgery | Protecting surgeons and patients during wars and armed conflicts: importance of predeployment training on the Geneva conventions and International Humanitarian Law | CE/Surgeons must join the effort to ensure that their training and that of other health care personnel, in their rights and obligations under the Geneva Conventions and International Humanitarian Law are fundamental to ensure effective humanitarian aid and its advocacy. | Rights Obligations Laws Humanitarian |
| 21 | M | Zarka, S., 2019, Israel | Bioethics | Humanitarian medical aid to the Syrian people: Ethical implications and dilemmas. | CE/Challenges in medical care for civilians: ethical principles implementation and new ethical dilemmas, e.g., standard of treatment, cultural differences, etc. | Ethical principles & Treatment |
| 22 | M | Lundberg, K., 2019, Sweden | Nursing Ethics | Dual loyalties: Everyday ethical problems of registered nurses and physicians in combat zones | CME/Reasons for civilian registered healthcare professional not undertaking combat duties were that it was not in their role, not according to ethical codes or humanitarian law or a breach towards patients. Reasons for undertaking combat duties were that humanitarian law does not apply or has to be treated pragmatically or that it is a case of force protection. Shortage of resources and competence were reasons for both doing and not doing military tasks. Under some circumstances, they could undertake military tasks: when under threat, if unseen or if not needed for healthcare duties. | Humanitarian Law, Duties, Role, Resource shortage |
| 23 | M | Pingree, C.S., 2020, USA | HEC forum | Medical Ethics in Extreme and Austere Environments | CME/Focus and emphasize on ethical challenges and promotes individual physician training in both medical and ethical decision-making. | Ethics Training |
| 24 | M | Cawthorne, D., 2020, Denmark | Sci Eng Ethics | An Ethical Framework for the Design, Development, Implementation, and Assessment of Drones Used in Public Healthcare | CE/The emergence of fifth bioethics principles from artificial intelligence ethics: explicability. | AI and new ethical issues |
| 25 | M | de Vries, P., 2020, The Netherland | J Mil Ethics | Virtue Ethics in the Military: An Attempt at Completeness | ME/There are seven virtues of character and the intellectual virtue of practical wisdom, i.e., responsibility, competence, comradeship, respect, courage, resilience, discipline, and practical wisdom (corresponding military praxis of task, arms, cooperation, enemy, danger, undetermined time and place, rules, and action). These virtues provide clear and practical guidance on the standards of excellence and how one ought to behave in a comprehensive use of narrative in turn provides a context for elaboration on the virtues and their role in successful military operations. | Task, Arms, Cooperation, Enemy, Danger, Undetermined time and place, Rules, and Action |
| 26 | M | Hertelendy, A.J., 2021, USA | Int J Qual Health Care | Crisis standards of care in a pandemic: navigating the ethical, clinical, psychological and policy-making maelstrom | CE/A shift in crisis standard of care in pandemic from an individual to a population-based and the focus has profound consequences on how clinical decisions are made at the point of care. | Pandemic Medical decision-making vs. Ethics |
| 27 | M | Shanks Kaurin, P. 2021, USA | Strat Stud Quart | An “Unprincipled Principal”: Implications for Civil-Military Relations | CME/Discusses separate spheres, shared responsibility, and the place of moral values and normative commitments in Civil–Military relationship. There are some principals in this relationship that may have the right to be wrong but there is a need for guidance of those working operationally about how they should act when the moral and normative values of their principal are called into question. | Ethics, Moral, and Values and the principals strategically and operationally |
| 28 | S | Khorram-Manesh, A., 2021, Sweden | Front Public Health | Estimating the number of civilian casualties in modern armed conflicts- A Systematic Review | CME/A systematic review, pointing out the increasing number of public health emergencies and armed conflicts with particular attention on the challenges on the field. Deficient casualty counting during modern conflicts due to organizational, political or strategic reasons, the international organizations responsible for collecting such data (the International Federation of Red Cross and Red Crescent and International Institute of Humanitarian Law) face difficulties in accessing the conflict scene, resulting in under-reported, unreliable, or no-reported data. | IHL, Resource limitation, Modern armed conflicts |
Appendix C. Converting Topics to Subjects through Content Analysis

Appendix D. Subgroups Characteristics and Responses
| General Information | Polish | Swedish | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Military | 69 | 4 | 22 | 6 |
| Civilian | 19 | 6 | 30 | 43 |
| Military | 19 | 1 | 1 | 0 |
| Military Physician | 31 | 2 | 18 | 4 |
| Civilian Physician | 15 | 1 | 20 | 18 |
| Military Nurse | 0 | 0 | 2 | 0 |
| Civilian Nurse | 4 | 5 | 10 | 25 |
| Others (administration + Paramedic) | 19 | 1 | 1 | 2 |
| Total | 88 | 10 | 52 | 49 |
| Scenario 1 | Polish | Swedish | ||
|---|---|---|---|---|
| Own | Enemy | Own | Enemy | |
| Military | 17 | 54 | 9 | 16 |
| Civilian | 6 | 19 | 24 | 52 |
| Military Female | 0 | 1 | 0 | 0 |
| Military Male | 9 | 9 | 0 | 1 |
| Civilian Physicians Female | 0 | 1 | 4 | 14 |
| Civilian Physicians Male | 3 | 11 | 7 | 13 |
| Military Physicians Female | 0 | 2 | 2 | 2 |
| Military Physicians Male | 0 | 31 | 7 | 11 |
| Civilian Nurse Female | 2 | 3 | 5 | 20 |
| Civilian Nurse Male | 1 | 3 | 8 | 3 |
| Military Nurse Female | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 0 | 2 |
| Others Female | 0 | 1 | 0 | 2 |
| Others Male | 8 | 11 | 0 | 0 |
| Total | 23 | 73 | 33 | 68 |
| Scenario 2 | Polish | Swedish | ||
|---|---|---|---|---|
| Leave Some | Take All | Leave Some | Take All | |
| Military | 50 | 2 | 18 | 7 |
| Civilian | 40 | 2 | 63 | 8 |
| Military Female | 1 | 0 | 0 | 0 |
| Military Male | 18 | 0 | 1 | 0 |
| Civilian Physicians Female | 2 | 0 | 14 | 2 |
| Civilian Physicians Male | 31 | 0 | 17 | 1 |
| Military Physicians Female | 1 | 0 | 4 | 0 |
| Military Physicians Male | 14 | 0 | 12 | 6 |
| Civilian Nurse Female | 4 | 0 | 20 | 4 |
| Civilian Nurse Male | 3 | 1 | 10 | 1 |
| Military Nurse Female | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 1 | 1 |
| Others Female | 0 | 1 | 2 | 0 |
| Others Male | 16 | 2 | 0 | 0 |
| Total | 90 | 4 | 81 | 15 |
| Scenario 3 | Polish | Swedish | ||||||
|---|---|---|---|---|---|---|---|---|
| Retreat | Leave | Stay | Medevac | Retreat | Leave | Stay | Medevac | |
| Military | 43 | 22 | 5 | 2 | 5 | 6 | 5 | 8 |
| Civilian | 11 | 8 | 2 | 2 | 19 | 30 | 8 | 13 |
| Military Female | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Male | 14 | 5 | 0 | 0 | 0 | 0 | 1 | 0 |
| Civilian Physicians Female | 0 | 0 | 0 | 0 | 6 | 5 | 2 | 2 |
| Civilian Physicians Male | 8 | 3 | 1 | 1 | 5 | 8 | 2 | 4 |
| Military Physicians Female | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 3 |
| Military Physicians Male | 20 | 10 | 1 | 0 | 5 | 4 | 3 | 5 |
| Civilian Nurse Female | 1 | 2 | 1 | 1 | 5 | 13 | 1 | 4 |
| Civilian Nurse Male | 2 | 2 | 0 | 0 | 2 | 4 | 2 | 3 |
| Military Nurse Female | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| Others Female | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 |
| Others Male | 8 | 5 | 4 | 2 | 0 | 0 | 0 | 0 |
| Total | 54 | 30 | 7 | 4 | 24 | 36 | 13 | 21 |
| Scenario 4 | Polish | Swedish | ||||||
|---|---|---|---|---|---|---|---|---|
| Fire Drone | Don’t Fire | Call Superior | Un-Decided | Fire Drone | Don’t Fire | Call Superior | Un-Decided | |
| Military | 17 | 31 | 2 | 1 | 4 | 10 | 2 | 6 |
| Civilian | 8 | 9 | 0 | 1 | 15 | 40 | 2 | 2 |
| Military Female | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Male | 11 | 5 | 1 | 1 | 0 | 1 | 0 | 0 |
| Civilian Physicians Female | 0 | 1 | 0 | 0 | 2 | 8 | 1 | 0 |
| Civilian Physicians Male | 3 | 4 | 0 | 0 | 7 | 9 | 1 | 0 |
| Military Physicians Female | 0 | 1 | 0 | 0 | 0 | 3 | 0 | 1 |
| Military Physicians Male | 1 | 18 | 0 | 0 | 4 | 5 | 1 | 5 |
| Civilian Nurse Female | 2 | 3 | 0 | 0 | 3 | 14 | 0 | 2 |
| Civilian Nurse Male | 3 | 0 | 0 | 1 | 3 | 7 | 0 | 0 |
| Military Nurse Female | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| Others Female | 0 | 1 | 0 | 0 | 0 | 2 | 0 | 0 |
| Others Male | 4 | 7 | 1 | 0 | 0 | 0 | 0 | 0 |
| Total | 25 | 40 | 2 | 2 | 19 | 50 | 4 | 8 |
| Scenario 5 | Polish | Swedish | ||
|---|---|---|---|---|
| As Planned | Others | As Planned | Others | |
| Military | 11 | 59 | 15 | 9 |
| Civilian | 7 | 22 | 35 | 33 |
| Military Female | 0 | 1 | 0 | 0 |
| Military Male | 4 | 15 | 0 | 1 |
| Civilian Physicians Female | 1 | 0 | 8 | 8 |
| Civilian Physicians Male | 3 | 15 | 11 | 6 |
| Military Physicians Female | 0 | 2 | 3 | 1 |
| Military Physicians Male | 1 | 30 | 11 | 6 |
| Civilian Nurse Female | 0 | 5 | 7 | 15 |
| Civilian Nurse Male | 2 | 2 | 8 | 3 |
| Military Nurse Female | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 1 | 1 |
| Others Female | 1 | 0 | 1 | 1 |
| Others Male | 6 | 11 | 0 | 0 |
| Total | 18 | 81 | 50 | 42 |
| Scenario 6 | Polish | Swedish | ||||||
|---|---|---|---|---|---|---|---|---|
| Help | Avoid | Alert | Instruct | Help | Avoid | Alert | Instruct | |
| Military | 38 | 10 | 13 | 11 | 13 | 6 | 8 | 0 |
| Civilian | 12 | 2 | 6 | 5 | 21 | 9 | 39 | 0 |
| Military Female | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Male | 9 | 2 | 3 | 4 | 0 | 0 | 1 | 0 |
| Civilian Physicians Female | 0 | 0 | 1 | 0 | 7 | 1 | 9 | 0 |
| Civilian Physicians Male | 10 | 0 | 1 | 3 | 6 | 4 | 9 | 0 |
| Military Physicians Female | 2 | 0 | 0 | 0 | 1 | 2 | 1 | 0 |
| Military Physicians Male | 18 | 3 | 3 | 7 | 12 | 2 | 6 | 0 |
| Civilian Nurse Female | 1 | 1 | 2 | 1 | 2 | 4 | 16 | 0 |
| Civilian Nurse Male | 0 | 1 | 2 | 1 | 6 | 2 | 3 | 0 |
| Military Nurse Female | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Military Nurse Male | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| Others Female | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 |
| Others Male | 8 | 5 | 7 | 0 | 0 | 0 | 0 | 0 |
| Total | 50 | 12 | 19 | 16 | 34 | 17 | 47 | 0 |
References
- Velasquez, M.; Claire, A.; Shanks, T.; Meyer, M.J. What is Ethics? 2010. Available online: https://www.scu.edu/ethics/ethics-resources/ethical-decision-making/what-is-ethics/ (accessed on 24 November 2021).
- Baker, G.H.; Wallis, J.; Jason, E. Vertical and Horizontal Respect: A Two-Dimensional Framework for Ethical Decision-Making; National Defense University Press: Washington, DC, USA, 2015; Available online: https://ndupress.ndu.edu/Media/News/News-Article-View/Article/607603/vertical-and-horizontal-respect-a-two-dimensional-framework-for-ethical-decisio (accessed on 24 November 2021).
- Lantz, G. Applied Ethics: What Kind of Ethics and What Kind of Ethicist? J. Appl. Philos. 2000, 17, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L. History and theory in “applied ethics”. Kennedy Inst. Ethics J. 2007, 17, 55–64. [Google Scholar] [CrossRef]
- Turner, E.; Passmore, J. Mastering Ethics. In Mastering Executive Coaching; Passmore, J., Underhill, B.O., Goldsmith, M., Eds.; Routledge: London, UK, 2018. [Google Scholar] [CrossRef]
- Nantel, J.; Weeks, W.A. Marketing ethics: Is there more to it than the utilitarian approach? Eur. J. Mark. 1996, 30, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Whysall, P. Marketing Ethics–An Overview. Mark. Rev. 2000, 1, 175–195. [Google Scholar] [CrossRef]
- Furman, G.C. The ethic of community. J. Educ. Adm. 2004, 42, 215–235. [Google Scholar] [CrossRef]
- Schlegelmilch, B.B.; Öberseder, M. Half a Century of Marketing Ethics: Shifting Perspectives and Emerging Trends. J. Bus. Ethics 2010, 93, 1–19. [Google Scholar] [CrossRef]
- Murphy, P.E. Marketing Ethics at the Millennium: Review, Reflections, and Recommendations. In The Blackwell Guide to Business Ethics; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2017; pp. 165–185. [Google Scholar] [CrossRef]
- Östman, L.; Näsman, Y.; Eriksson, K.; Nyström, L. Ethos: The heart of ethics and health. Nurs. Ethic 2017, 26, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.-A.; Chrysochou, P.; Mitkidis, P.; Ariely, D. Human decision-making biases in the moral dilemmas of autonomous vehicles. Sci. Rep. 2019, 9, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Khorram-Manesh, A.; Lönroth, H.; Rotter, P.; Wilhelmsson, M.; Aremyr, J.; Berner, A.; Andersson, A.N.; Carlström, E. Non-medical aspects of civilian–military collaboration in management of major incidents. Eur. J. Trauma Emerg. Surg. 2017, 43, 595–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorram-Manesh, A.; Burkle, F.M.; Goniewicz, K.; Robinson, Y. Estimating the Number of Civilian Casualties in Modern Armed Conflicts–A Systematic Review. Front. Public Health 2021, 9, 765261. [Google Scholar] [CrossRef]
- Pless, N.M.; Maak, T.; Waldman, D.A. Different Approaches Toward Doing the Right Thing: Mapping the Responsibility Orientations of Leaders. Acad. Manag. Perspect. 2012, 26, 51–65. [Google Scholar] [CrossRef]
- Schaubroeck, J.; Hannah, S.T.; Avolio, B.J.; Kozlowski, S.; Lord, R.G.; Trevino, L.K.; Dimotakis, N.; Peng, A.C. Embedding Ethical Leadership within and across Organization Levels. Acad. Manag. J. 2012, 55, 1053–1078. [Google Scholar] [CrossRef] [Green Version]
- Munoz-Chereau, B.; González, Á.; Meyers, C.V. How are the ‘losers’ of the school accountability system constructed in Chile, the USA and England? Comp. A J. Comp. Int. Educ. 2020, 1–20. [Google Scholar] [CrossRef]
- O’Fallon, M.J.; Butterfield, K.D. A Review of The Empirical Ethical Decision-Making Literature: 1996–2003. J. Bus. Ethic 2005, 59, 375–413. [Google Scholar] [CrossRef]
- Schwartz, M.S. Ethical decision-making theory: An integrated approach. J. Bus. Ethics 2016, 139, 755–776. [Google Scholar] [CrossRef]
- Bywater, M. Classical and Political Humanitarianisms in an Era of Military Interventionism and the War on Terror: Ambiguity, Prescription, Jus in Bello and Jus ad Bellum. J. Int. Humanit. Leg. Stud. 2017, 8, 33–112. [Google Scholar] [CrossRef]
- de Vries, P. Virtue Ethics in the Military: An Attempt at Completeness. J. Mil. Ethic 2020, 19, 170–185. [Google Scholar] [CrossRef]
- Vanclay, F.; Baines, J.T.; Taylor, C.N. Principles for ethical research involving humans: Ethical professional practice in impact assessment Part I. Impact Assess. Proj. Apprais. 2013, 31, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Greene, J.D. Beyond Point-and-Shoot Morality: Why Cognitive (Neuro) Science Matters for Ethics. Ethics 2014, 124, 695–726. [Google Scholar] [CrossRef] [Green Version]
- Philip, T.M.; Gupta, A.; Elby, A.; Turpen, C. Why Ideology Matters for Learning: A Case of Ideological Convergence in an Engineering Ethics Classroom Discussion on Drone Warfare. J. Learn. Sci. 2017, 27, 183–223. [Google Scholar] [CrossRef]
- Amir, K.-M. Ethical aspects of disasters. In Handbook of Disaster and Emergency Management, 2nd ed.; Goniewicz, K.-M., Dulebenets, H., Eds.; Kompendiet: Göteborg, Sweden, 2021. [Google Scholar] [CrossRef]
- Lazar, S. Risky Killing and the Ethics of War. Ethics 2015, 126, 91–117. [Google Scholar] [CrossRef]
- Naushad, V.A.; Bierens, J.J.; Nishan, K.P.; Firjeeth, C.P.; Mohammad, O.H.; Maliyakkal, A.M.; ChaliHadan, S.; Schreiber, M.D. A systematic review of the impact of disaster on the mental health of medical responders. Prehosp. Disaster Med. 2019, 34, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Simonds, A.K.; Sokol, D.K. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur. Respir. J. 2009, 34, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Morganstein, J.C.; Ursano, R.J. Ecological disasters and mental health: Causes, consequences, and interventions. Front. Psychiatry 2020, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Khorram-Manesh, A.; Yttermyr, J.; Sörensson, J.; Carlström, E. The impact of disasters and major incidents on vulnerable groups: Risk and medical assessment of Swedish patients with advanced care at home. Home Health Care Manag. Pract. 2017, 29, 183–190. [Google Scholar] [CrossRef]
- Khorram-Manesh, A. Facilitators and constrainers of civilian–military collaboration: The Swedish perspectives. Eur. J. Trauma Emerg. Surg. 2018, 46, 649–656. [Google Scholar] [CrossRef] [Green Version]
- Khorram-Manesh, A.; Goniewicz, K.; Burkle, F.M.; Robinson, Y. Review of Military Casualties in Modern Conflicts—The Re-emergence of Casualties From Armored Warfare. Mil. Med. 2021, usab108. [Google Scholar] [CrossRef]
- Khorram-Manesh, A.; Dulebenets, M.A.; Goniewicz, K. Implementing Public Health Strategies-The need for Educational Initiatives: A Systematic Review. Sustainability 2021, 18, 5888. [Google Scholar] [CrossRef]
- Lundberg, K.; Kjellström, S.; Sandman, L. Dual loyalties: Everyday ethical problems of registered nurses and physicians in combat zones. Nurs. Ethics 2019, 26, 480–495. [Google Scholar] [CrossRef]
- Pingree, C.S.; Newberry, T.R.; McMains, K.C.; Holt, G.R. Medical Ethics in Extreme and Austere Environments. HEC Forum 2020, 1–12. [Google Scholar] [CrossRef]
- Rebera, A.P.; Rafalowski, C. On the Spot Ethical Decision-Making in CBRN (Chemical, Biological, Radiological or Nuclear Event) Response: Approaches to on the Spot Ethical Decision-Making for First Responders to Large-Scale Chemical Incidents. Sci. Eng. Ethics 2014, 20, 735–752. [Google Scholar] [CrossRef] [PubMed]
- Burkle, F.M.; Kushner, A.L.; Giannou, C.; Paterson, M.A.; Wren, S.M.; Burnham, G. Health care providers in war and armed conflict: Operational and educational challenges in international humanitarian law and the Geneva conventions, part II. Educational and training initiatives. Disaster Med. Public Health Prep. 2019, 13, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Cathleen, S. Sigismund of Sweden as foreigner in own kingdom. In Dynastic Change; Rodrigues, A.M.S.A., Silva, M.S., Spangler, J., Eds.; Routledge: London, UK, 2019. [Google Scholar]
- Finch, J. The vignette technique in survey research. Sociology 1987, 21, 105–114. Available online: https://www.deepdyve.com/lp/sage/the-vignette-technique-in-survey-research-4SSZb1xoNO?key=sage (accessed on 25 November 2021). [CrossRef]
- Atzmüller, C.; Steiner, P.M. Experimental vignette studies in survey research. Methodol. Eur. J. Res. Methods Behav. Soc. Sci. 2010, 6, 128–138. [Google Scholar] [CrossRef]
- Antes, A.L.; Dineen, K.K.; Bakanas, E.; Zahrli, T.; Keune, J.D.; Schuelke, M.J.; DuBois, J.M. Professional decision-making in medicine: Development of a new measure and preliminary evidence of validity. PLoS ONE 2020, 15, e0228450. [Google Scholar] [CrossRef] [Green Version]
- Reibling, N.; Ariaans, M.; Wendt, C. Worlds of Healthcare: A Healthcare System Typology of OECD Countries. Health Policy 2019, 123, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Graneheim, U.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurs. Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McMaster University. National Collaborating Center for Methods and Tools. Health Evidence Quality Assessment Tool. Available online: https://www.nccmt.ca/knowledge-repositories/search/275 (accessed on 24 November 2021).
- Rayyan. Inteligent Systematic Review. Available online: https://www.rayyan.ai/ (accessed on 25 November 2021).
- Derse, A.R.; Schiedermayer, D. Practical Ethics for Students, Interns, and Residents, 4th ed.; BookBaby: Pennsauken Township, NJ, USA, 2017. [Google Scholar]
- Harvey, N.; Holmes, C.A. Nominal group technique: An effective method for obtaining group consensus. Int. J. Nurs. Pract. 2012, 18, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Internetowy System Aktów Prawnych (ISAP). Ustawa z Dnia 5 Grudnia 1996 r. O Zawodach Lekarza i Lekarza Dentysty. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU19970280152 (accessed on 24 November 2021).
- Swedish National Constitution. Svensk författningssamling. (n.d.). Lag om Ändring i Lagen (2003:460) om Etikprövning av Forskning Som Avser Människor. Available online: https://www.lagboken.se/Lagboken/start/skoljuridik/lag-2003460-om-etikprovning-av-forskning-som-avser-manniskor/d_181354-sfs-2008_192-lag-om-andring-i-lagen-2003_460-om-etikprovning-av-forskning-som-avser-manniskor (accessed on 24 November 2021).
- Swedish Parliament. Sveriges Riksdag. (n.d.). Lag (2003:460) om Etikprövning av Forskning Som Avser Människor Svensk Författningssamling 2003:2003:460 t.o.m. SFS 2021:612—Riksdagen. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-2003460-om-etikprovning-av-forskning-som_sfs-2003-460 (accessed on 24 November 2021).
- Pocock, S.J. The simplest statistical test: How to check for a difference between treatments. BMJ 2006, 332, 1256–1258. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A. Values and ethics: Attributes influencing self-esteem and cognitive style of adolescents. Int. J. Home Sci. 2020, 6, 384–388. [Google Scholar]
- UNESCO. Ethics Education Programme; UNESCO: Paris, France, 2020; Available online: https://en.unesco.org/themes/ethics-science-and-technology/ethics-education (accessed on 24 November 2021).
- Spadaro, A. COVID-19: Testing the Limits of Human Rights | Australian Human Rights Institute. Eur. J. Risk Regul. 2020, 11, 317–325. Available online: https://www.humanrights.unsw.edu.au/on-guard/general/covid-19-testing-limits-human-rights (accessed on 22 December 2021). [CrossRef] [Green Version]
- Hertelendy, A.J.; Ciottone, G.R.; Mitchell, C.L.; Gutberg, J.; Burkle, F.M. Crisis standards of care in a pandemic: Navigating the ethical, clinical, psychological and policy-making maelstrom. Int. J. Qual. Health Care 2021, 33, mzaa094. [Google Scholar] [CrossRef] [PubMed]
- Craft, J.L. A Review of the Empirical Ethical Decision-Making Literature: 2004–2011. J. Bus. Ethics 2013, 117, 221–259. [Google Scholar] [CrossRef]
- Rodney, P.A. What We Know About Moral Distress. Am. J. Nurs. 2017, 117, S7. [Google Scholar] [CrossRef]
- Hem, M.H.; Molewijk, B.; Gjerberg, E.; Lillemoen, L.; Pedersen, R. The significance of ethics reflection groups in mental health care: A focus group study among health care professionals. BMC Med. Ethics 2018, 19, 54. [Google Scholar] [CrossRef]
- Löfquist, L. Virtue Ethics and Disasters. In Disasters: Core Concepts and Ethical Theories; O’Mathúna, D., Dranseika, V., Gordijn, B., Eds.; Advancing Global Bioethics; Springer: Cham, Switzerland, 2018; Volume 11. [Google Scholar] [CrossRef] [Green Version]
- Council of Europe. Congress of Local and Regional Authorities of the Coucil of Europe. Strengthening Public Ethics: New Practical Guides; Congress of Local and Regional Authorities: Strasbourg, France, 2019; Available online: https://www.coe.int/en/web/congress/home/-/asset_publisher/FR3MTvSnicL5/content/strengthening-public-ethics-new-practical-guid-1 (accessed on 24 November 2021).
- Goniewicz, K.; Burkle, F.M.; Horne, S.; Borowska-Stefańska, M.; Wiśniewski, S.; Khorram-Manesh, A. The Influence of War and Conflict on Infectious Disease: A Rapid Review of Historical Lessons We Have Yet to Learn. Sustainability 2021, 13, 10783. [Google Scholar] [CrossRef]
- Goniewicz, K.; Carlström, E.; Hertelendy, A.J.; Burkle, F.M.; Goniewicz, M.; Lasota, D.; Richmond, J.G.; Khorram-Manesh, A. Integrated Healthcare and the Dilemma of Public Health Emergencies. Sustainability 2021, 13, 4517. [Google Scholar] [CrossRef]
- Burkle, F.M., Jr. Challenges of Global Public Health Emergencies: Development of a Health-Crisis Management Framework. Tohoku J. Exp. Med. 2019, 249, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Allen, G.M.; Parrillo, S.J.; Will, J.; Mohr, J.A. Principles of disaster planning for the pediatric population. Prehosp. Disaster Med. 2007, 22, 537–540. [Google Scholar] [CrossRef]
- Slim, H. Humanitarian Ethics: A Guide to the Morality of Aid in War and Disaster; Hurst & Company: London, UK, 2015. [Google Scholar]
- Leider, J.P.; DeBruin, D.; Reynolds, N.; Koch, A.; Seaberg, J. Ethical Guidance for Disaster Response, Specifically Around Crisis Standards of Care: A Systematic Review. Am. J. Public Health 2017, 107, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R. Internal War and International Law. In The Future of the International Legal Order; Princeton University Press: Princeton, NJ, USA, 2019; Volume 3, pp. 81–121. [Google Scholar]
- Ford, R.M.; Rawluk, A.; Williams, K.J.H. Managing values in disaster planning: Current strategies, challenges and opportunities for incorporating values of the public. Land Use Policy 2019, 81, 131–142. [Google Scholar] [CrossRef]
- Khorram-Manesh, A. Europe on Fire; Medical Management of Terror Attacks—New Era and New considerations. In Bull. Emerg. Trauma; 2016; 4, pp. 183–185. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5118569/ (accessed on 22 December 2021).
- Khorram-Manesh, A.; Burkle, F.M.; Phattharapornjaroen, P.; Ahmadi Marzaleh, M.; Sultan, M.A.; Mäntysaari, M.; Carlström, E.; Goniewicz, K.; Santamaria, E.; Comandante, J.D.; et al. The Development of Swedish Military Healthcare System: Part II-Re-evaluating the Military and Civilian Healthcare Systems in Crises Through a Dialogue and Study Among Practitioners. Mil. Med. 2021, 186, e442–e450. [Google Scholar] [CrossRef]
- Khorram-Manesh, A.; Mortelmans, L.J.; Robinson, Y.; Burkle, F.M.; Goniewicz, K. Civilian-Military Collaboration before and during COVID-19 Pandemic—A Systematic Review and a Pilot Survey among Practitioners. Sustainability 2022, 14, 624. [Google Scholar] [CrossRef]
- Billsten, J.; Benderix, Y. Implementation of user organizations in Swedish health care and social services for persons with substance use disorders. Nordic Soc. Work Res. 2019, 11, 277–289. [Google Scholar] [CrossRef] [Green Version]
- Burkle, F.M. Triage and the lost art of decoding vital signs: Restoring physiologically based triage skills in complex humanitarian emergencies. Disaster Med. Public Health Prep. 2018, 12, 76–85. [Google Scholar] [CrossRef]
- Schussler, L.; Burkle, F.M., Jr.; Wren, S.M. Protecting Surgeons and Patients During Wars and Armed Conflicts: Importance of Predeployment Training on the Geneva Conventions and International Humanitarian Law. JAMA Surg. 2019, 154, 683–684. [Google Scholar] [CrossRef]
- Cawthorne, D.; Robbins-van Wynsberghe, A. An ethical framework for the design, development, implementation, and assessment of drones used in public healthcare. Sci. Eng. Ethics 2020, 26, 2867–2891. [Google Scholar] [CrossRef]
- Evetts, G.E. Aeromedical evacuation in the humanitarian and disaster relief environment of Op RUMAN. J. R. Army Med. Corps 2019, 165, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Titus, E.; Lemmer, G.; Slagley, J.; Eninger, R. A review of CBRN topics related to military and civilian patient exposure and decontamination. Am. J. Disaster Med. 2019, 14, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Jennings, P.L.; Hannah, S.T. The moralities of obligation and aspiration: Towards a concept of exemplary military ethics and leadership. Mil. Psychol. 2011, 23, 550–571. [Google Scholar] [CrossRef]
- Sousa, C.; Hagopian, A. Conflict, health care and professional perseverance: A qualitative study in the West Bank. Glob. Public Health 2011, 6, 520–533. [Google Scholar] [CrossRef] [PubMed]
- Zehfuss, M. Targeting: Precision and the production of ethics. Eur. J. Intern. Relat. 2011, 17, 543–566. [Google Scholar] [CrossRef]
- Geale, S.K. The ethics of disaster management. Disaster Prev. Manag. 2012, 21, 445–462. [Google Scholar] [CrossRef] [Green Version]
- Hay, C. The obligation to resist oppression. In Kantianism, Liberalism, and Feminism; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Hunt, M.R.; Schwartz, L.; Sinding, C.; Elit, L. The ethics of engaged presence: A framework for health professionals in humanitarian assistance and development work. Dev. World Bioeth. 2014, 14, 47–55. [Google Scholar] [CrossRef]
- Wiist, W.H.; Barker, K.; Arya, N.; Rohde, J.; Donohoe, M.; White, S.; Lubens, P.; Gorman, G.; Hagopian, A. The Role of Public Health in the Prevention of War: Rationale and Competencies. Am. J. Public Health 2014, 104, e34–e47. [Google Scholar] [CrossRef]
- Mileham, P. Human conflict and universal ethics (part 2). Def. Secur. Anal. 2016, 32, 97–111. [Google Scholar] [CrossRef]
- Rochon, C.; Williams-Jones, B. Are Military and Medical Ethics Necessarily Incompatible? A Canadian Case Study. J. Law Med. Ethics 2016, 44, 639–651. [Google Scholar] [CrossRef]
- Young, S.S.; Lewis, D.C.; Gilbey, P.; Eisenman, A.; Schuster, R.; Seponski, D.M. Conflict and Care: Israeli Healthcare Providers and Syrian Patients and Caregivers in Israel. Glob. Qual. Nurs. Res. 2016, 3, 2333393616666584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, T.G. Ethical Quandaries in War Zones, When Mass Atrocity Prevention Fails. Glob. Policy 2016, 7, 135–145. [Google Scholar] [CrossRef]
- Knudson, M.M.; Elster, E.A.; Bailey, J.A.; Johannigman, J.A.; Bailey, P.V.; Schwab, C.W.; Kirk, G.G.; Woodson, J.A. Military-Civilian Partnerships in Training, Sustaining, Recruitment, Retention, and Readiness: Proceedings from an Exploratory First-Steps Meeting. J. Am. Coll. Surg. 2018, 227, 284–292. [Google Scholar] [CrossRef]
- O’Mathúna, D.P.; Dranseika, V.; Gordijn, B. (Eds.) Disasters: Core Concepts and Ethical Theories; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef] [Green Version]
- Zarka, S.; Farhat, M.; Gidron, T. Humanitarian medical aid to the Syrian people: Ethical implications and dilemmas. Bioethics 2019, 33, 302–308. [Google Scholar] [CrossRef]
- Shanks, K.P. An “Unprincipled Principal”: Implications for Civil-Military Relations. Strateg. Stud. Q. Perspect. 2021, 15, 50–68. Available online: https://0-www-jstor-org.brum.beds.ac.uk/stable/27032896 (accessed on 2 January 2022).
- Goulia, P.; Mantas, C.; Dimitroula, D.; Mantis, D.; Hyphantis, T. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect. Dis. 2010, 10, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ives, J.; Greenfield, S.; Parry, J.M.; Draper, H.; Gratus, C.; Petts, J.I.; Sorell, T.; Wilson, S. Healthcare workers’ attitudes to working during pandemic influenza: A qualitative study. BMC Public Health 2009, 9, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGill University. Rayyan for Systematic Review. Available online: https://libraryguides.mcgill.ca/rayyan/gettingstarted (accessed on 24 November 2021).
- Magnussen, L.I.; Carlstrøm, E.; Sørensen, J.L.; Torgersen, G.-E.; Hagenes, E.F.; Kristiansen, E. Learning and usefulness stemming from collaboration in a maritime crisis management exercise in Northern Norway. Disaster Prev. Manag. 2017, 27, 129–140. [Google Scholar] [CrossRef]
- Sultan, M.A.S.; Løwe Sørensen, J.; Carlström, E.; Mortelmans, L.; Khorram-Manesh, A. Emergency Healthcare Providers’ Perceptions of Preparedness and Willingness to Work during Disasters and Public Health Emergencies. Healthcare 2020, 8, 442. [Google Scholar] [CrossRef]
- International Federation of Red Cross and Red Crescent Societies. Ethics in Disaster Response—IFRC. Available online: https://www.ifrc.org/en/what-we-do/disaster-management/responding/ethics-in-disaster-response/ (accessed on 24 November 2021).


| Poland | Sweden | |||||||
|---|---|---|---|---|---|---|---|---|
| <34 Years | 35–44 Years | 45–54 Years | >55 Years | <34 Years | 35–44 Years | 45–54 Years | >55 Years | |
| Military | 9 | 4 | 6 | 0 | 1 | 0 | 0 | 0 |
| Military Physician | 1 | 5 | 20 | 7 | 2 | 6 | 5 | 9 |
| Civilian Physician | 4 | 6 | 1 | 3 | 7 | 8 | 10 | 10 |
| Military Nurse | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 |
| Civilian Nurse | 4 | 2 | 1 | 2 | 14 | 7 | 7 | 5 |
| Others | 16 | 1 | 2 | 1 | 2 | 0 | 0 | 0 |
| Total | 34 | 18 | 31 | 13 | 27 | 21 | 22 | 25 |
| Female | 10 | 49 | ||||||
| Male | 88 | 52 | ||||||
| Scenarios/Groups | Groups | P | Groups | P | Groups | P | Groups | P | Groups | P | Groups | P |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A. Military vs. Civilian | B. Swedish vs. Polish | |||||||||||
| a. Swedish | b. Polish | c. All | a. Civilians | b. Military | c. All | |||||||
| One: You are responsible for a casualty collecting area during an armed conflict. You receive two injured soldiers; one is from your own forces with severe injuries and poor prognosis, while the other is an enemy soldier, also severely injured, but with a better prognosis. You can only transport one to definitive care. Whom to choose and why? | 9/25 Military and 24/76 civilian choose own soldier | 0.008 | 17/71 Military and 6/25 civilian choose own soldier | 0.02 | 26/96 military and 30/101 civilians choose own soldier | 0.59 | 24/76 Swedish and 6/25 Polish civilians choose own soldier | <0.0001 | 9/25 Swedish and 17/71 Polish military choose own soldier | 0.11 | 33/101 military and 23/96 civilians choose own soldier | 0.17 |
| Two: You are working at an intensive care unit and receive information that all units in your hospital should be evacuated due to a possible bomb explosion. There are 10 patients in your unit, five of whom can be evacuated by three staff at your unit. Three of remaining five patients need one staff each. The remaining two patients need two staff each. You have seven staff and need to triage. Whom do and why? | 18/25 Military and 63/71 civilian leave someone behind | <0.00001 | 50/52 Military and 40/42 civilian leave someone behind | 0.29 | 68/77 military and 103/113 civilians leave someone behind | 0.007 | 63/71 Swedish and 40/42 Polish civilians leave someone behind | <0.0001 | 18/25 Swedish and 50/52 Polish military leave someone behind | 0.0001 | 81/96 military and 90/94 civilians leave someone behind | 0.49 |
| Scenario 3: You are in the hot zone of an armed conflict and are responsible for casualty collection area. You have 10 injured and none of them can move without help. You have two staff. You receive the order to retreat. What do you do and why? | 5/24 Military and 19/70 civilian follow order to retreat | <0.00001 | 43/72 Military and 11/23 civilian follow order to retreat | 0.0001 | 48/96 military and 30/93 civilians follow the order to retreat | 0.04 | 19/70 Swedish and 11/23 Polish civilians follow order to retreat | <0.0001 | 5/24 Swedish and 43/72 Polish military follow order to retreat | <0.0001 | 24/94 military and 54/95 civilians follow the order to retreat | 0.0006 |
| Scenario 4: You are assigned to conduct a drone attack. The target is a group of enemy, of whom one is a key person. They are in an area with tens of civilians, many of whom will definitely die under the attack. What do you do and why? | 4/22 Military and 15/59 civilian follow order to fire drones | <0.00001 | 17/51 Military and 8/18 civilian follow order to fire drones | 0.07 | 21/73 military and 23/77 civilians follow order to fire drones | 0.76 | 15/59 Swedish and 8/18 Polish civilians follow order to fire drones | <0.0001 | 4/22 Swedish and 17/51 Polish military follow order to fire drones | 0.004 | 19/81 military and 25/69 civilians follow order to fire drones | 0.36 |
| Scenario 5: You are a pilot and your mission is to pick up (repatriate) infected citizens out of another country in a closed zone. You can only transport 80 people. That is the exact number of your citizens. However, after landing you notice that there are also non-citizens waiting for you. Five out of these 10 people are children. All insist to be evacuated. What do you do and whom do you choose? Why do you do that? Other comments? | 15/24 Military and 35/68 civilians choose to evacuate as ordered | <0.00001 | 11/70 Military and 7/29 civilian choose to evacuate as ordered | 0.34 | 26/94 military and 42/97 civilians choose to evacuate as ordered | 0.052 | 35/68 Swedish and 7/29 Polish civilians choose to evacuate as ordered | <0.0001 | 15/24 Swedish and 11/70 Polish military choose to evacuate as ordered | 0.005 | 50/92 military and 18/99 civilians choose to evacuate as ordered | 0.0001 |
| Scenario 6: You are driving your car together with a colleague. Suddenly, you find a tanker truck carrying an unknown substance, overturned on the road. Another private car has already arrived on the scene and four persons are investigating the tank at a very close distance. One of them comes close to you and asks for help. He seems to have breathing difficulties, and has red and teary eyes. What do you do? Why do you that? Other comments? | 8/27 Military and 39/69 civilian chose to alert responsible civil agency | <0.00001 | 13/72 Military and 6/25 civilians chose to alert responsible civil agency | 0.10 | 51/99 military and 33/94 civilians chose to alert responsible civil agency | 0.049 | 39/69 Swedish and 6/25 Polish civilians chose to alert responsible civil agency | <0.0001 | 8/27 Swedish and 13/72 Polish military chose to alert responsible civil agency | 0.27 | 47/96 military and 19/99 civilians chose to alert responsible civil agency | 0.0001 |
| Scenarios | Groups | p |
|---|---|---|
| a. Swedish Male vs. Swedish Female | ||
| 1 | 22/52 male and 11/49 female | 0.056 |
| 2 | 41/50 male and 40/46 female | 0.27 |
| 3 | 12/50 male and 12/44 female | 1.0 |
| 4 | 14/45 male and 5/36 female | <0.039 |
| 5 | 31/48 male and 19/44 female | 0.09 |
| 6 | 19/53 male and 28/45 female | 0.19 |
| b. Polish Male vs. Polish Females | ||
| 1 | 21/86 male and female 2/10 females | <0.0001 |
| 2 | 82/85 male and female 8/9 | <0.0001 |
| 3 | 52/86 male and female 2/9 | <0.0001 |
| 4 | 22/60 male and female 3/9 | <0.0001 |
| 5 | 16/89 male and female 2/10 | <0.0009 |
| 6 | 16/87 male and female 3/10 | <0.002 |
| c. All Females vs. Males | ||
| 1 | 13/59 females and 43/138 choose own soldier | <0.0001 |
| 2 | 48/55 females and 123/134 civilians leave someone behind | <0.0001 |
| 3 | 14/53 females and 64/136 males follow the order to retreat | <0.0001 |
| 4 | 8/42 females and 36/100 males follow order to fire drones | <0.0001 |
| 5 | 21/54 females and 47/137 males choose to evacuate as ordered | <0.0016 |
| 6 | 31/55 females and 35/148 males chose to alert responsible civil agency | 0.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khorram-Manesh, A.; Goniewicz, K.; Phattharapornjaroen, P.; Gray, L.; Carlström, E.; Sundwall, A.; Hertelendy, A.J.; Burkle, F.M. Differences in Ethical Viewpoints among Civilian–Military Populations: A Survey among Practitioners in Two European Countries, Based on a Systematic Literature Review. Sustainability 2022, 14, 1085. https://0-doi-org.brum.beds.ac.uk/10.3390/su14031085
Khorram-Manesh A, Goniewicz K, Phattharapornjaroen P, Gray L, Carlström E, Sundwall A, Hertelendy AJ, Burkle FM. Differences in Ethical Viewpoints among Civilian–Military Populations: A Survey among Practitioners in Two European Countries, Based on a Systematic Literature Review. Sustainability. 2022; 14(3):1085. https://0-doi-org.brum.beds.ac.uk/10.3390/su14031085
Chicago/Turabian StyleKhorram-Manesh, Amir, Krzysztof Goniewicz, Phatthranit Phattharapornjaroen, Lesley Gray, Eric Carlström, Alice Sundwall, Attila J. Hertelendy, and Frederick M. Burkle. 2022. "Differences in Ethical Viewpoints among Civilian–Military Populations: A Survey among Practitioners in Two European Countries, Based on a Systematic Literature Review" Sustainability 14, no. 3: 1085. https://0-doi-org.brum.beds.ac.uk/10.3390/su14031085