A Randomized, Placebo-Controlled, Pilot Clinical Trial to Evaluate the Effect of Supplementation with Prebiotic Synergy 1 on Iron Homeostasis in Children and Adolescents with Celiac Disease Treated with a Gluten-Free Diet




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants Selection
2.3. Ethics
2.4. Intervention
2.5. Sample Collection
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Morphological and Biochemical Parameters of Blood
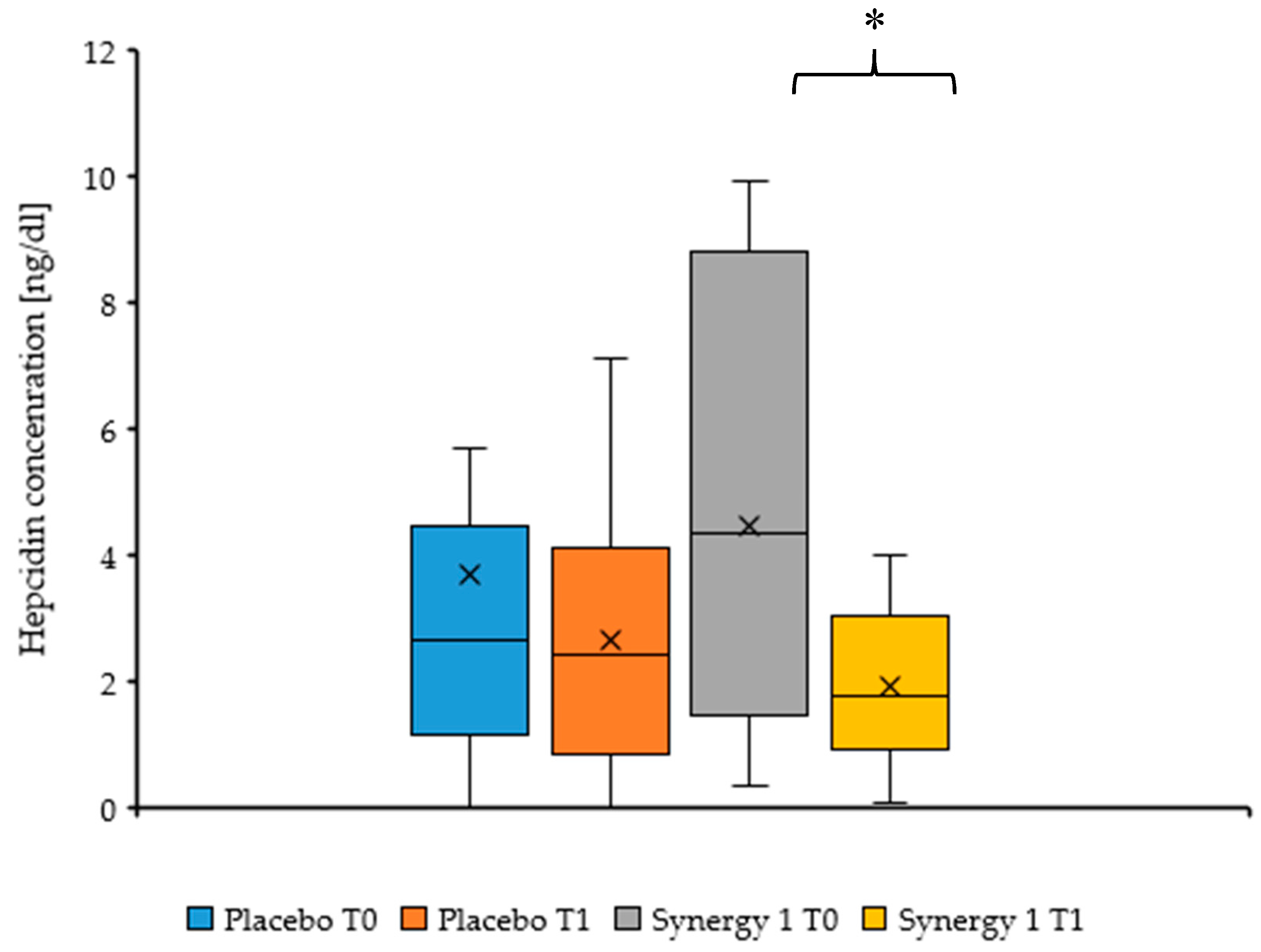
3.3. Hepcidin
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guandalini, S.; Assiri, A. Celiac disease: A review. JAMA Pediatr. 2014, 168, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Dickson, B.C.; Streutker, C.J.; Chetty, R. Coeliac disease: An update for pathologists. J. Clin. Pathol. 2006, 59, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Crocker, H.; Jenkinson, C.; Churchman, D.; Peters, M. The Coeliac Disease Assessment Questionnaire (CDAQ): Development of a patient-reported outcome measure. Value Health 2016, 9, A595. [Google Scholar] [CrossRef]
- Schumann, M.; Siegmund, B.; Schulzke, J.D.; Fromm, M. Celiac Disease: Role of the Epithelial Barrier. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Roma, E.; Roubani, A.; Kolia, E.; Panayiotou, J.; Zellos, A.; Syriopoulou, V.P. Dietary compliance and life style of children with coeliac disease. J. Hum. Nutr. Diet. 2010, 23, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Efthymakis, K.; Milano, A.; Laterza, F.; Serio, M.; Neri, M. Iron deficiency anemia despite effective gluten-free diet in celiac disease: Diagnostic role of small bowel capsule endoscopy. Dig. Liver Dis. 2017, 49, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Freeman, H.J. Iron deficiency anemia in celiac disease. World J. Gastroenterol. 2015, 21, 9233–9238. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Ganz, T. The role of hepcidin in iron metabolism. Acta Haematol. 2009, 122, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.; Song, S.H.; Lee, J.H.; Kim, H.-J.; Yang, H.R. Serum hepcidin levels and iron parameters in children with iron deficiency. Korean J. Hematol. 2012, 47, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Harper, J.W.; Holleran, S.F.; Ramakrishnan, R.; Bhagat, G.; Green, P.H.R. Anemia in celiac disease is multifactorial in etiology. Am. J. Hematol. 2007, 82, 996–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulec, S.; Anderson, G.J.; Collins, J.F. Mechanistic and regulatory aspects of intestinal iron absorption. AJP Gastrointest. Liver Physiol. 2014, 307, G397–G409. [Google Scholar] [CrossRef] [PubMed]
- Elli, L.; Poggiali, E.; Tomba, C.; Andreozzi, F.; Nava, I.; Bardella, M.T.; Campostrini, N.; Girelli, D.; Conte, D.; Cappellini, M.D. Does TMPRSS6 RS855791 polymorphism contribute to iron deficiency in treated celiac disease. Am. J. Gastroenterol. 2015, 110, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Manzanares, A.; Lucendo, A.J. Nutritional and dietary aspects of celiac disease. Nutr. Clin. Pract. 2011, 26, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [PubMed]
- Deora, V.; Aylward, N.; Sokoro, A.; El-Matry, W. Serum vitamins and minerals at diagnosis an follow-up in children with celiac disease. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Galli, G.; Esposito, G.; Lahner, E.; Pilozzi, E.; Corleto, V.D.; Di Giulio, E.; Aloe Spiriti, M.A.; Annibale, B. Histological recovery and gluten-free diet adherence: A prospective 1-year follow-up study of adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2014, 40, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Bardella, M.T.; Velio, P.; Cesana, B.M. Coeliac disease: A histological follow-up study. Histopathology 2007, 50, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and Nutrient deficiencies: A revive. Clin. Nutr. 2016, 35, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Theethira, T.G.; Dennis, M.; Leffler, D.A. Nutritional consequences of celiac disease and gluten-free diet. Expert Rev. Gastroenterol. Hepatol. 2014, 8, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Thomson, T.; Dennis, M.; Higgins, L.A.; Lee, A.R.; Sharrett, M.K. Gluten-free diet survey: Are Americans with celiac disease consuming recommended amounts of fiber, iron, calcium and grain foods? J. Hum. Nutr. Diet. 2005, 18, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Yeung, C.K.; Glahn, R.E.; Welch, R.M.; Miller, D.D. Prebiotics and Iron Bioavailability-Is There a Connection? J. Food Sci. 2005, 70, R88–R92. [Google Scholar] [CrossRef]
- Marciano, R.; Santamarina, A.B.; De Santana, A.A.; Silva, M.D.L.C.; Amancio, O.M.S.; Do Nascimento, C.M.D.P.O.; Oyama, L.M.; De Morais, M.B. Effects of prebiotic supplementation on the expression of proteins regulating iron absorption in anaemic growing rats. Br. J. Nutr. 2015, 113, 901–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupa-Kozak, U.; Drabińska, N.; Jarocka-Cyrta, E. The effect of oligofructose-enriched inulin supplementation on gut microbiota, nutritional status and gastrointestinal symptoms in paediatric coeliac disease patients on a gluten-free diet: Study protocol for a pilot randomized controlled trial. Nutr. J. 2017, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Drabińska, N.; Jarocka-Cyrta, E.; Markiewicz, L.H.; Krupa-Kozak, U. The Effect of Oligofructose-Enriched Inulin on Faecal Bacterial Counts and Microbiota-Associated Characteristics in Celiac Disease Children Following a Gluten-Free Diet: Results of a Randomized, Placebo-Controlled Trial. Nutrients 2018, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, I.R.; Korponay-Szabo, M.L.; Mearin, A.P.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branksi, D.; Catasssi, C.; Lelgeman, M.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- WHO. Iron Deficiency Anaemia: Assessment, Prevention, and Control. A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- U.S. National Institutes of Health. Available online: https://clinicaltrials.gov/ (accessed on 27 February 2017).
- Yasuda, K.; Dawson, H.D.; Wasmuth, E.V.; Roneker, C.A.; Chen, C.; Urban, J.F.; Welch, R.M.; Miller, D.D.; Lei, X.G. Supplemental Dietary Inulin Influences Expression of Iron and Inflammation Related Genes in Young Pigs. J. Nutr. 2009, 139, 2018–2023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, J.K.; Yasuda, K.; Welch, R.M.; Miller, D.D.; Lei, X.G. Supplemental Dietary Inulin of Variable Chain Lengths Alters Intestinal Bacterial Populations in Young Pigs. J. Nutr. 2010, 140, 2158–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohta, A.; Ohtsuki, M.; Baba, S.; Takizawa, T.; Adachi, T.; Kimura, S. Effects of fructooligosaccharides on the absorption of iron, calcium and magnesium in iron-deficient anemic rats. J. Nutr. Sci. Vitaminol. 1995, 41, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Delzenne, N.; Aertssens, J.; Verplaetse, H.; Roccaro, M.; Roberfroid, M. Effect of fermentable fructo-oligosaccharides on mineral, nitrogen and energy digestive balance in the rat. Life Sci. 1995, 57, 1579–1587. [Google Scholar] [CrossRef]
- Laparra, J.M.; Tako, E.; Glahn, R.P.; Miller, D.D. Supplemental inulin does not enhance iron bioavailability to Caco-2 cells from milk- or soy-based, probiotic-containing, yogurts but incubation at 37 °C does. Food Chem. 2008, 109, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Laparra, J.M.; Glahn, R.P.; Miller, D.D. Assessing potential effects of inulin and probiotic bacteria on Fe availability from common beans (Phaseolus vulgaris L.) to Caco-2 cells. J. Food Sci. 2009, 74, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Vitali, D.; Radić, M.; Cetina-Čižmek, B.; Vedrina Dragojević, I. Caco-2 cell uptake of Ca, Mg and Fe from biscuits as affected by enrichment with pseudocereal/inulin mixtures. Acta Aliment. 2011, 40, 480–489. [Google Scholar] [CrossRef]
- Christides, T.; Ganis, J.C.; Sharp, P.A. In vitro assessment of iron availability from commercial Young Child Formulae supplemented with prebiotics. Eur. J. Nutr. 2018, 57, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, E.G.H.M.; Schaafsma, G.; Muys, T.; Van Dokkum, W. Nondigestible oligosaccharides do not interfere with calcium and nonheme-iron absorption in young, healthy men. Am. J. Clin. Nutr. 1998, 67, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petry, N.; Egli, I.; Chassard, C.; Lacroix, C.; Hurrell, R. Inulin modifies the bifidobacteria population, fecal lactate concentration, and fecal pH but does not influence iron absorption in women with low iron status. Am. J. Clin. Nutr. 2012, 96, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Daya, H.; Lebwohl, B.; Lewis, S.K.; Green, P.H. Celiac disease patients presenting with anemia have more severe disease than those presenting with diarrhea. Clin. Gastroenterol. Hepatol. 2013, 11, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Rahim, M.W.; See, J.A.; Lahr, B.D.; Wu, T.T.; Murray, J.A. Mucosal recovery and mortality in adults with celiac disease after treatment with a gluten-free diet. Am. J. Gastroenterol. 2010, 105, 1412–1420. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Diagnosed Celiac Disease Gluten-free diet for at least 6 months Age: 4–18 years old Normalization of Tissue Transglutaminase Antibody (TTGA) level Written consent from parents/caregivers | Iron deficiency anemia 1 Iron deficiency 2 Immunoglobulin A (IgA) deficiency Treatment with oral formulas in the 2 months prior to the study Therapy by antibiotics or probiotics/prebiotics in the 2 months prior to the study Chronic inflammatory disorders |
| Total Sample | Intervention Group (Synergy 1) | Placebo Group (Maltodextrin) | ||||
|---|---|---|---|---|---|---|
| N | 30 | 17 (56.6%) | 13 (63.4%) | |||
| Gender (G–girls, B–boys) | G = 18 (60%) | G = 10 (58.8%) | G = 8 (61.5%) | |||
| B = 12 (40%) | B = 7 (41.2%) | B = 5 (38.5%) | ||||
| Age (years) | 4–18 | 4–18 | 4–16 | |||
| Average = 10 | Average = 10 | Average = 10 | ||||
| T0 a | T1 b | T0 | T1 | T0 | T1 | |
| Weight (kg) | 15.0–78.0 | 15.7–77.5 | 15.0–78.0 | 15.7–77.5 | 16.3–66.8 | 17.0–71.5 |
| Av = 35.8 | Av = 37.6 | Av = 35.8 | Av = 37.6 | Av = 33.7 | Av = 36.2 | |
| Height (cm) | 103.0–183.0 | 104.5–184.5 | 104.5–183.0 | 108.0–184.5 | 103.0–172.0 | 104.5–172.6 |
| Av = 139.6 | Av = 141.4 | Av = 141.5 | Av = 142.4 | Av = 137.1 | Av = 139.7 | |
| BMI (kg/m2) | 12.5–28.4 | 12.7–29.0 | 12.5–23.5 | 12.7–23.6 | 13.7–28.4 | 13.4–29.0 |
| Av = 17.1 | Av = 17.3 | Av = 17.1 | Av = 17.3 | Av = 17.0 | Av = 17.3 | |
| Morphology Parameters | Synergy 1 Group | Placebo Group | Synergy 1: T0 vs. T1 1 (p Value) | Placebo: T0 vs. T1 1 (p Value) | T1: Synergy 1 vs. Placebo (p Value) | ||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||||
| Red Blood Cell (106/mm3) | 4.63 ± 0.37 | 4.69 ± 0.34 | 4.58 ± 0.37 | 4.57 ± 0.34 | 0.274 | 0.851 | 0.359 |
| Hemoglobin (g/dL) | 13.22 ± 0.99 | 13.13 ± 1.09 | 13.12 ± 0.99 | 12.89 ± 1.09 | 0.912 | 0.297 | 0.565 |
| Hematocrit (%) | 39.11 ± 2.95 | 39.65 ± 3.22 | 38.94 ± 2.95 | 38.93 ± 3.22 | 0.314 | 0.838 | 0.559 |
| Mean Cell Volume (µm3) | 84.50 ± 4.18 | 84.63 ± 4.33 | 85.19 ± 4.18 | 84.92 ± 4.33 | 1.000 | 0.779 | 0.283 |
| Mean Cell Hemoglobin (pg) | 28.48 ± 1.53 | 27.65 ± 1.17 | 28.65 ± 1.53 | 28.13 ± 1.17 | 0.139 | 0.052 | 0.102 |
| Red Blood Cell Distribution Width (%) | 12.64 ± 0.71 | 12.91 ± 0.92 | 12.99 ± 0.71 | 13.22 ± 0.92 | 0.247 | 0.308 | 0.695 |
| Platelets (103/mm3) | 290.28 ± 64.15 | 314.63 ± 55.51 | 301.38 ± 64.15 | 315.77 ± 55.51 | 0.299 | 0.197 | 0.957 |
| White Blood Cell (103/mm3) | 6.29 ± 1.64 | 6.57 ± 1.78 | 6.59 ± 1.64 | 6.65 ± 1.78 | 0.721 | 0.844 | 0.283 |
| Biochemical parameters | |||||||
| C-reactive protein (CRP) (mg/dL) | 0.14 ± 0.08 | 0.11 ± 0.07 | 0.10 ± 0.08 | 0.12 ± 0.07 | 0.582 | 0.100 | 0.660 |
| Ferritin (ng/mL) | 25.78 ± 14.48 | 22.94 ± 13.94 | 27.62 ± 14.48 | 23.08 ± 13.94 | 0.507 | 0.107 | 0.742 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feruś, K.; Drabińska, N.; Krupa-Kozak, U.; Jarocka-Cyrta, E. A Randomized, Placebo-Controlled, Pilot Clinical Trial to Evaluate the Effect of Supplementation with Prebiotic Synergy 1 on Iron Homeostasis in Children and Adolescents with Celiac Disease Treated with a Gluten-Free Diet. Nutrients 2018, 10, 1818. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111818
Feruś K, Drabińska N, Krupa-Kozak U, Jarocka-Cyrta E. A Randomized, Placebo-Controlled, Pilot Clinical Trial to Evaluate the Effect of Supplementation with Prebiotic Synergy 1 on Iron Homeostasis in Children and Adolescents with Celiac Disease Treated with a Gluten-Free Diet. Nutrients. 2018; 10(11):1818. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111818
Chicago/Turabian StyleFeruś, Klaudia, Natalia Drabińska, Urszula Krupa-Kozak, and Elżbieta Jarocka-Cyrta. 2018. "A Randomized, Placebo-Controlled, Pilot Clinical Trial to Evaluate the Effect of Supplementation with Prebiotic Synergy 1 on Iron Homeostasis in Children and Adolescents with Celiac Disease Treated with a Gluten-Free Diet" Nutrients 10, no. 11: 1818. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111818