1. Introduction
A population’s dietary habits and its access to sources of iodine—such as seafood, milk and dairy products, iodized salt, and iodine containing supplements—are important for securing sufficient iodine intake. The frequency and quantity of consumption of these iodine sources are critical determinants of the individual’s iodine status. Iodine is essential for thyroid hormone production, which plays a crucial role in ensuring optimal growth and brain development of the fetus and child. Insufficient iodine intake in utero and during early childhood may damage the developing brain, leading to the loss of intellectual potential, making it one of the most important preventable causes of brain damage worldwide [
1]. Suboptimal iodine nutrition gives rise to concern since emerging evidence suggests that children of women with an urinary iodine to creatinine ratio (UI/Cr) <150 µg/g in pregnancy are more likely to have lower scores on verbal IQ, reading accuracy, and reading comprehension at eight years of age [
2]. Results from the follow-up of the gestational iodine cohort (9-year and 15-year) in Australia indicate that even mild iodine deficiency during pregnancy may have consequences for the child that are not improved by sufficient iodine intake during childhood [
3,
4]. Adequate maternal iodine status is therefore especially important since the fetus is dependent on maternal transfer of thyroid hormones in early gestation and supply of iodine later in gestation. The recommended intake of iodine during pregnancy is 175 µg/day in the Nordic countries [
5] and 250 µg/day according to World Health Organization (WHO) [
6].
The urinary iodine concentration (UIC) captures the total iodine intake and is regarded as a reliable biomarker for assessing recent iodine intake at a group level [
7]. A median UIC in the range of 150–250 µg/L indicates adequate iodine nutrition in a population of pregnant women [
8]. By using a median cutoff of 150 µg/L, insufficient iodine status has been demonstrated in pregnant women in several European countries during recent years [
2,
9,
10,
11,
12]. The population in Norway has long been considered iodine sufficient due to the contribution of iodine from milk and dairy products. The Norwegian Mother and Child Cohort Study (MoBa), including more than 80 thousand pregnant women, has challenged this assumption as a large proportion of these women was at risk of suboptimal dietary iodine intake [
13]. Studies assessing UIC from pregnant women in Norway confirm the findings of insufficient dietary iodine intake [
13,
14,
15]. Further, the MoBa study has shown that an estimated dietary iodine intake <160 µg/day during pregnancy was associated with symptoms of child language delay, behavior problems, and reduced fine motor skills at age three years [
16].
Both season of the year and time point of urine sampling have been shown to influence the UIC [
17,
18]. Studies also suggest that gestational week is of importance for the interpretation of UIC in pregnancy [
19,
20]. With urine samples and dietary data from approximately one thousand pregnant women, we aim to investigate their iodine status by measuring UIC and assess if maternal characteristics and dietary factors may influence the iodine status. Further, we ask if gestational week, time of urine sampling, season of the year, and creatinine levels may influence the interpretation of iodine nutrition in pregnancy.
2. Materials and Methods
2.1. Study Population and Design
This study used samples and data collected as part of a population-based prospective cohort designed to investigate pre- and postnatal risk factors influencing developmental malleability from pregnancy to 18 months of age. Families were recruited from nine different public health clinics across Norway. The clinics were chosen after considering demographic characteristics and size of the population to include participants from both cities and rural districts with a wide distribution of socioeconomic conditions. At each site, one midwife was trained as a research assistant and invited all the pregnant women at 16–26 weeks gestation to participate, but some women were enrolled before week 16 and some as late as week 30. Between September 2011 and mid-October 2012, 1041 families were enrolled. Five families withdrew their consent, leaving us with 1036 mothers. Three families were excluded due to stillbirth, and 26 were excluded for other reasons before birth of the child (i.e., poor parental health, family moving out of the area, participation felt to be too time consuming). These families let us keep the data we had already collected. We were left with 1007 mothers who gave birth to 1017 children (including 10 twin pairs; multiple pregnancies other than twins have been excluded).
Figure 1 shows participation flowchart.
Data collection phases comprised five points in pregnancy, birth, and four follow-up points up to age 18 months. Data collection up to 18 months was finished by November 2014. In this article urine samples, dietary data, and demographic data from the pregnant women are used. The study was conducted according to the guidelines in the Declaration of Helsinki and was approved by Regional Committees for Medical and Health Research Ethics in Norway (REK 2011/560). Written informed consent was obtained from all subjects.
2.2. Data Collection and Categorization of Variables
A non-fasting urine sample was obtained from every pregnant woman in specimens collected at each site. Gestational week, time of the day, and date of urine sample were registered. Since women were enrolled in the study at different gestational weeks, the spot urine sample was categorized into first (0–13 weeks of gestation), second (14–27 weeks of gestation), and third (28–40 weeks of gestation) trimester. The time of day for sampling of the urine was categorized into morning (6–9 a.m.), noon (10–13 a.m.), afternoon (14–17 p.m.), evening (18–24 p.m.), and night (0–5 p.m.). The date of sampling was divided into four seasons; spring (March–May), summer (June–August), autumn (September–November), and winter (December–February).
A comprehensive questionnaire package was given to mothers and fathers at the first meeting after inclusion, which could take place from pregnancy week 16 to 34, depending on the specific time of enrollment. All parents were asked to answer these questions, irrespective of exact time of inclusion. Among the many questions, data on maternal (and family) characteristics such as age, weight before pregnancy, height, parity, education, socio-economic status, and use of tobacco were obtained. Age of participating women was divided in four categories; <25 years, 25–29 years, 30–34 years, and ≥35 years. The residence of the women was divided into north, mid, west, and east regions of Norway. The north area included women from one sampling site (Tromsø), mid from three samplings sites (Trondheim), west (Bergen) from two sampling sites, and the east area of Norway included three different sampling sites (Oslo). Parental education was categorized into primary and high school (low), University College or University ≤4 years (middle), or University College or University ≥4 years (high). The income of the mother was categorized as <300,000 NOK, 300,000–449,000 NOK, and ≥450,000 NOK.
Dietary data were collected using a web-based semi–quantitative food frequency questionnaire (FFQ) covering the last three months intake of iodine rich foods, such as seafood, milk, dairy products, and eggs in addition to some questions about the intake of other main food groups, such as fruit and vegetables, bread and cereals, and meat and meat products [
21,
22]. The first question regarding milk and dairy products asked if they consumed milk and dairy products daily or weekly (‘yes’ or ‘no’). A second question concerned portions of milk and dairy products intake per day, which was categorized as 0–1 portions/day, 2–3 portions/day, and 4–9 portions/day. As to the first question, the non-daily users were included in the category 0–1 portions/day. The seafood intake was recoded to estimate the weekly intake for dinner and the daily intake of seafood as bread spread. Follow-up questions regarding type of seafood were asked to differentiate between lean fish, fatty fish, and the frequency of use of processed fish products (i.e., fish cakes, fish fingers, etc.). The weekly intake of seafood for dinner was then dichotomized into <2 portions/week and ≥2 portions/week. Several questions regarding the use of supplements were asked, answers were divided into non-iodine containing supplement and iodine containing supplement based on information given in several questions. Supplement use was then dichotomized as users (≥5 times/week) and non-users (<5 times/week). The level of iodine in supplements on the Norwegian marked varies from 50 to 225 µg. The maximum level to be added is set to 225 µg iodine per daily dose.
2.3. Laboratory Analysis
The spot urine samples were stored at minus 20 °C approximately one month at each sampling site before all samples were shipped to Institute of Marine Research (IMR) and stored at minus 20 °C until analysis of iodine and creatinine concentrations was carried out. Prior to analysis, the urine samples were defrosted in a refrigerator. For the determination of iodine, 500 µL urine was diluted in 4.5 mL 1% tetrametylammonium hydroxide (TMAH) and filtered using a sterile membrane filter with a 0.45 µm pore size and a single use syringe. Samples were analyzed against a urine calibration curve (standard addition curve) to measure the unknown iodine concentration (127I) in the collected urine samples. The accuracy of the results was verified with certified reference material; Seronorm Trace Elements Urine (Nycomed Pharma, Asker, Norway) with certified iodine content of 84 µg/L (range 72–96 µg/L) and 304 µg/L (range 260–348 µg/L). UIC was determined by inductively coupled plasma mass-spectrometry (ICP-MS).
For the urinary creatinine determination, the urine samples were defrosted at room temperature and centrifuged in an Eppendorf (5810R) centrifuge (15 min, 2000× g and 4 °C). An aliquot of 200 µL was transferred to the test tube and placed in the Maxmat carousel. All sample treatment was automatic; samples were diluted 1:20 with distilled water and reagents added. Determination of creatinine was performed by a colorimetric enzymatic principle using a MAXMAT PL II multidisciplinary diagnostic platform using the Creatinine PAP kit, (ERBA Diagnostics, Montpellier, France). The method was calibrated with one standard and further controlled with two independent controls.
Creatinine concentration was also used to determine whether the spot urinary sample was valid. We have excluded urine samples with creatinine concentration outside the WHO guidelines of <0.3 g/L and >3.0 g/L [
23].
2.4. Statistics
We report iodine status in two ways; as the urinary iodine concentration (µg/L) and as the urinary iodine per gram creatinine (µg/g). Both measures were used to explore relations with participants’ characteristics and dietary intake by using independent samples Mann–Whitney U Test. Medians and 25th and 75th percentiles are reported for all these variables (
Table 1). The 24-h excretion of iodine (UIE) was estimated by multiplying the iodine-to creatinine ratio by the expected daily excretion of creatinine 1.23 [
24]. Spearman’s correlations were calculated for UIC, maternal characteristics and intake of iodine rich foods. Variables that showed a relation with the UIC and iodine to creatinine ratio in the unadjusted analysis (
Table 1) were entered in the linear regression model to evaluate associations between maternal characteristics or dietary factors (
Table 2 and
Table 3). The relationship between UIC or IU/Cr ratio was explored by linear regression, and we used a standard multiple regression model. Two-tailed
p-values < 0.05 were considered statistically significant. The statistical software package Statistical Package for the Social Sciences (SPSS
® Statistics Version 24) was used for all data analyses.
4. Discussion
The main finding of this study was that median UIC was 85 µg/L, which is below the recommended cut off value of 150 µg/L set by WHO [
8]. This suggests that many of the pregnant women in this study had an insufficient iodine intake. In fact, almost 80% of the women had a UIC <150 µg/L. Dietary factors such as use of iodine supplements and intake of dairy products, as well as residence of the mother and season of urine sampling, were all significantly associated with both UIC and UI/Cr. The agreement of correct assignments between UIC and UI/Cr was 84% when the UIC was dichotomized (<150 µg/L and >150 µg/L); 111 women (11.5%) had both UIC and UI/Cr <50 µg/L. To our best knowledge, this is the first survey using UIC and UI/Cr in such a large sample of pregnant women living in several areas in Norway.
Insufficient iodine nutrition in pregnant women has been demonstrated in several European countries. In studies from Austria [
11], Belgium [
25], Denmark [
9], Latvia [
26], Poland [
12], Portugal [
27], Spain [
28], Sweden [
10], and the UK [
19], the median UIC was in the range from 57 µg/L in UK to 140 µg/L in Spain. In contrast, only a few studies have reported sufficient iodine intake in pregnant women. In Iceland, the median UIC was 200 µg/L [
29] and in the Netherlands UIC was 230 µg/L in pregnant women [
30]. In studies from Norway, median UIC was 92 µg/L (
n = 777) in pregnant women living in the Oslo area from 2016 [
15], 84 µg/L (
n = 197) in the Northern Mother-and-Child contaminant cohort (MISA) from 2007–2009 [
14], and 69 µg/L in the MoBa cohort (
n = 119) from 2003–2004 [
13]. In the MISA study and in the MoBa cohort, 80% and 89%, respectively, of the pregnant women had UIC <150 µg/L. The UIC levels in the Oslo area, MISA, MoBa, and our study are in line with results from the estimated dietary iodine intake in more than 60 thousand mothers in the MoBa cohort study [
13]. In the MoBa study, 54.3% had an estimated iodine intake below the Nordic recommendation of 175 µg/day and only 21.7% of the women reached the WHO recommendation of 250 µg iodine/day. In the Oslo area study, 55% had a calculated iodine intake below estimated average requirement (EAR) of 160 µg/day [
15]. Our study, as was also the case for the estimated iodine intake in the MoBa study [
13] and the study in the Oslo area [
15], comprised many participants and therefore suggest that pregnant women in Norway are at risk of having insufficient iodine intake.
Even though several factors determine the level of iodine in urine, the UIC captures the total iodine intake from all dietary sources [
7]. In our study, we found a strong relationship between UIC or UI/Cr and iodine supplement intakes and the intake of milk and dairy products. In studies from Denmark [
9], Poland [
12], and the UK [
19] it was also reported a higher UIC or UI/Cr in pregnant women using iodine supplements and/or consumed ≥2 portions of milk and dairy products per day. The MoBa study has also shown that the estimated dietary iodine intake was strongly associated with the intake of iodine supplement, milk and dairy products, and seafood [
13]. Since fortification of cow fodder started around 1950 in Norway, milk and dairy products have, been the most important dietary iodine source for Norwegians [
31]. This was confirmed in a study using dietary data from a representative sample of Norwegians [
32], and by the MoBa study using dietary data of pregnant women [
13]. However, the total iodine intake is still not in accordance with the recommendation. Analysis of the iodine content in milk and dairy products in Norway in 2000 [
33] showed a seasonal variation, but more recent analyses show that this variation has been less pronounced in recent years [
34,
35]. The urine samples in the present study were collected in 2011–12. Although we found a seasonal effect of UIC, meaning that UIC in samples collected in the winter (December–February) was significantly higher than in autumn (September–November), this difference was not related to a higher intake of milk and dairy products or supplement intake among these women. Therefore, it is reasonable to speculate that the iodine level in the milk and dairy products was higher during the winter season at the time of the data collection in the present study (i.e., 2011–12). As to residence, the women living in the eastern part of Norway with significantly higher UIC, did not have a higher milk and dairy or supplement intake than women living in the three other parts of Norway (mid, north, or west). Even if we found these higher UIC related to season and residence, all UIC levels were below the cut off value of ≤150 µg/L.
Although, seafood intake contributes to the iodine intake, the study among pregnant women in Iceland is the only one showing that fish intake of ≥2 times/week results in UIC above 150 µg/L [
29]. The intake of haddock (lean fish) was reported by 83% of Icelandic women. The iodine content within and between fish species varies, and in general, lean fish has higher levels of iodine than fatty fish [
32,
35]. The lack of associations between UIC or UI/Cr and intake of seafood in the present study is most likely due to the fact that approximately 30% of the women reported to consume seafood in accordance to the recommendation of 300–450 g/week. However, since the urine reflects only the last day of iodine intake, it would be more difficult to find a correlation with seafood intake which is eaten 2–3 times per week than milk and dairy products which are consumed more on a daily basis.
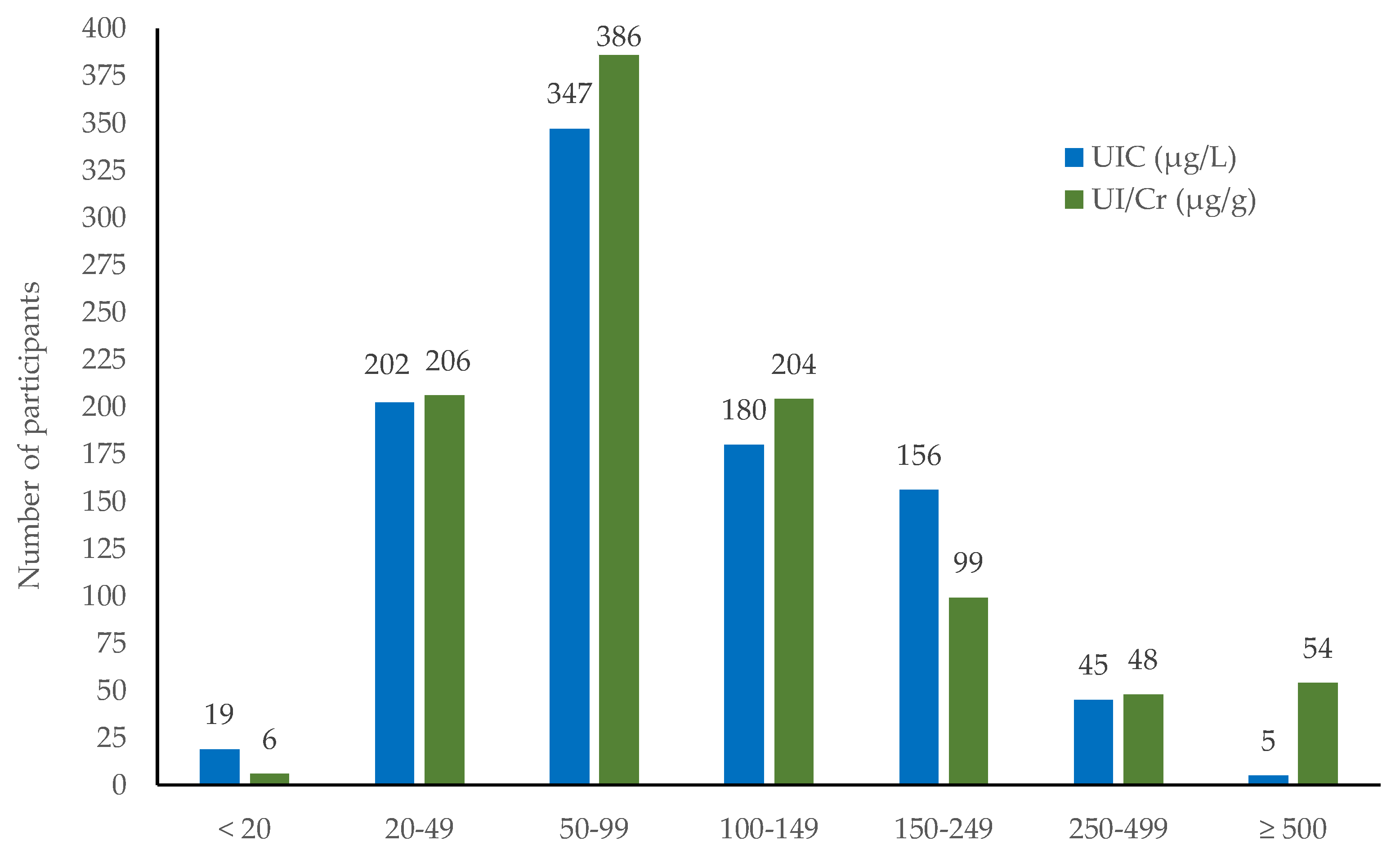
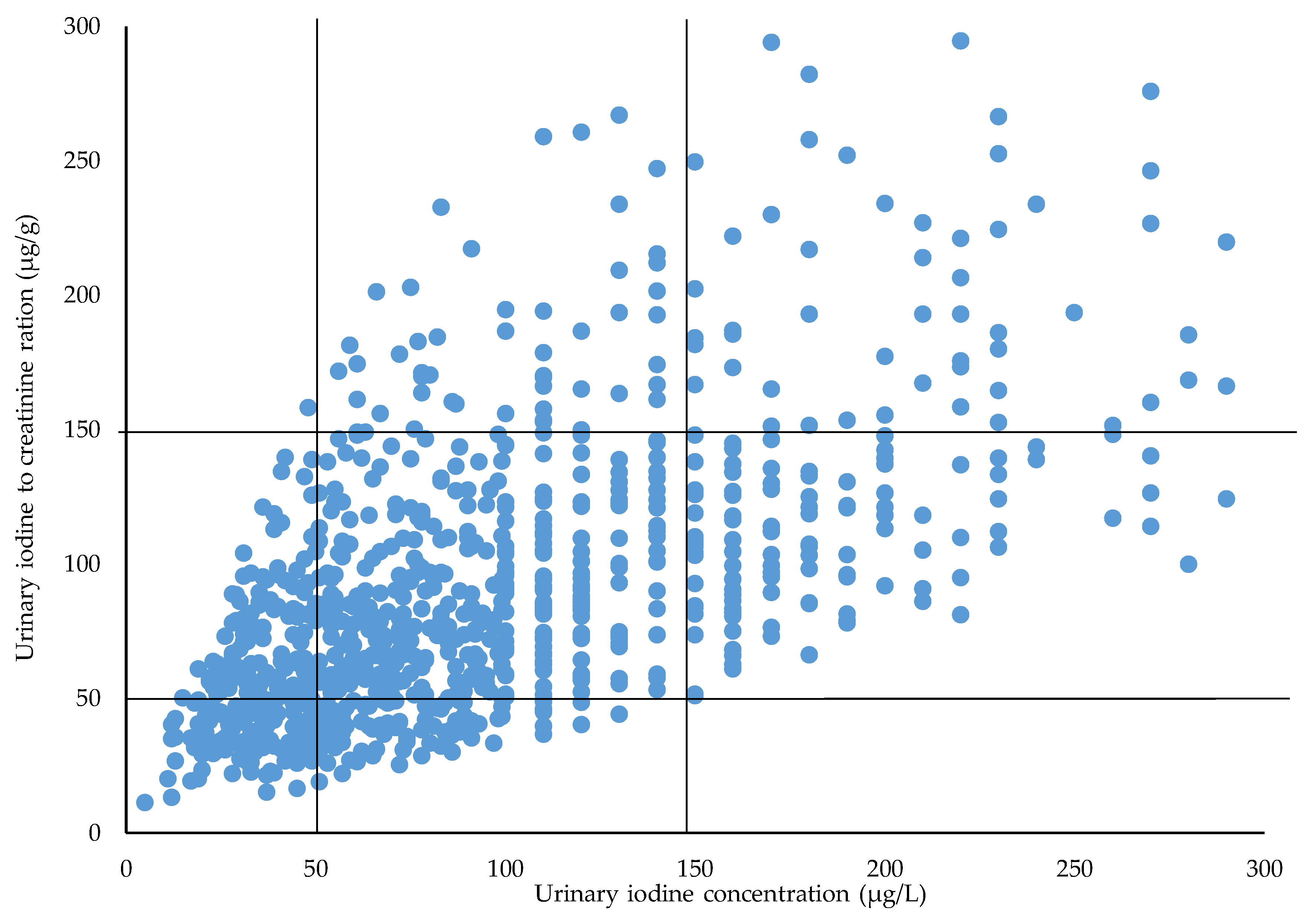
UIC is not recommended to be applied at an individual level. By using UIC and UI/Cr, respectively, for the classification of iodine deficiency, one may inadvertently come to classify women into different groups. By using UIC, our results showed that 221 (23.2%) of the women were classified with an UIC below 50 µg/L. By using the UI/Cr, 212 (22.2%) were so classified. Although the number of women is quite similar by both methods, only 111 individuals were assigned to the same group, i.e., had both UIC and UI/Cr <50 µg/L. This is a caveat to the effect that one should be careful when selecting the classification criterion. The inter- and intra-individual variation in UIC is caused by variation in fluid intake as well as differences in iodine intake. Since the creatinine excretion is relatively constant, the use of creatinine adjustments can minimize the variation in UIC caused by variation in the urine volume [
36]. In the study by Henjum et al. 2018 [
15] a sub-study group of 49 pregnant women had a median urine volume of 1.4 L. Considering this, we have overestimated the proportion of pregnant women having an UIC <150 µg/L when using the WHO criteria [
8].
The relationship of UIC or UI/Cr to maternal characteristics shows conflicting results. We found that trimester, time of the day of urine sampling, smoking, parity, education, and income were significantly associated with the UI/Cr (
p < 0.01) but not with the UIC. Studies using UIC have reported a reduction of UIC throughout pregnancy [
17,
20,
37,
38] or an increase of UIC [
19,
28]. UIC in our study increased with trimester, however not significantly. Studies using UI/Cr also report increasing level of UI/Cr by increasing gestational week [
19,
25,
26] and others have reported decreasing level of UI/Cr throughout pregnancy [
39].
This study has several strengths. Since the women were recruited year-round, the seasonal bias noted in other studies was reduced. The women were recruited from several regions in Norway and this is the first study using spot urine samples in a large sample of pregnant women. UIC is the recommended marker of assessments of iodine nutrition in population studies by WHO, and with almost 1000 samples we were able to estimate the iodine level within a precision range of ±5% [
36]. Further, analysis of iodine was performed with ICP-MS, which is a highly accurate method. The high retention rate is a strength to this study. This was possibly due to the participants being followed up by health care nurses serving as research assistants. One limitation is that most of the samples were collected in the second, and not in first trimester. It should be noted that the project is not a study of a truly representative population in terms of socioeconomic background. However, the study population is sufficiently large to conclude that the median UIC or UI/Cr indicate insufficient iodine intake in the population [
40].
Insufficient iodine intake among pregnant women is widespread in Europe. The lack of knowledge about the importance of iodine and about dietary sources of iodine among women can be regarded as a risk factor for iodine deficiency [
41]. More attention by health care providers, including obstetricians and midwives, may be important in solving this problem, along with the identification of new strategies capable to increase the knowledge of and awareness in the general population [
42]. Today, there is no national monitoring of iodine status of the Norwegian population, but according to a national plan of action for a better diet, public authorities should follow-up initiatives to improve and secure the iodine intake [
43]. Iodized salt is the most important source worldwide and is the agreed strategy for achieving iodine sufficiency [
8]. In Norway, iodized salt is available as table salt, however the level of iodine is only 5 µg/g, and the food industry is not permitted to use iodized salt. To improve the situation in Norway, the health authorities have recently initiated a risk–benefit analysis of increased iodization of table salt and iodization of bread products. Another action is to recommend iodine supplementation to pregnant women and other vulnerable groups with low consumption of milk.

 ,
, 



{kind=link}
{kind=link}
{kind=link}