Effects of a Gluten-Containing Meal on Gastric Emptying and Gallbladder Contraction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ultrasound Study of Gastric and Gallbladder Dynamics
2.3. Meal Administration
- gluten-free meal—a standard fatty meal consisting of cooked egg albumen (110 g), two slices of toasted gluten-free bread (rice, millet and quinoa flour basis) (50 g), strawberry jam (20 g), water (120 mL). The meal contained 250 kcal, of which 70% from carbohydrates.
- gluten-containing meal—an isocaloric meal differing only as regards the type of bread, which was gluten-containing (wheat flour basis).
2.4. Ultrasonographic Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shewry, P.R.; Halford, N.G.; Belton, P.S.; Tatham, A.S. The structure and properties of gluten: An elastic protein from wheat grain. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2002, 357, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Murray, J.A. Celiac disease. Curr. Opin. Gastroenterol. 2010, 26, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Elli, L.; Tomba, C.; Branchi, F.; Roncoroni, L.; Lombardo, V.; Bardella, M.T.; Ferretti, F.; Conte, D.; Valiante, F.; Fini, L.; et al. Evidence for the Presence of Non-Celiac Gluten Sensitivity in Patients with Functional Gastrointestinal Symptoms: Results from a Multicenter Randomized Double-Blind Placebo-Controlled Gluten Challenge. Nutrients 2016, 8, 84. [Google Scholar] [CrossRef] [PubMed]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Di Sabatino, A.; Volta, U.; Salvatore, C.; Biancheri, P.; Caio, G.; De Giorgio, R.; Di Stefano, M.; Corazza, G.R. Small amounts of gluten in subjects with suspected nonceliac gluten sensitivity: A. randomized, double-blind, placebo-controlled, cross-over trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Rini, G.; Mansueto, P. Non-celiac wheat sensitivity is a more appropriate label than non-celiac gluten sensitivity. Gastroenterology 2014, 146, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; et al. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Verdu, E.F.; Armstrong, D.; Murray, J.A. Between celiac disease and irritable bowel syndrome: The “no man’s land” of gluten sensitivity. Am. J. Gastroenterol. 2009, 104, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Branchi, F.; Pearson, K.; Priest, J.; Sanders, D.S. A study evaluating the bidirectional relationship between inflammatory bowel disease and self-reported non-celiac gluten sensitivity. Inflamm. Bowel Dis. 2015, 21, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Trott, N.; Briggs, R.; North, J.R.; Hadjivassiliou, M.; Sanders, D.S. Efficacy of a gluten-free diet in subjects with irritable bowel syndrome-diarrhea unaware of their HLA-DQ2/8 genotype. Clin. Gastroenterol. Hepatol. 2016, 14, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Barry, R.E. Gluten-induced mucosal changes in subjects without overt small-bowel disease. Lancet 1981, 1, 517–520. [Google Scholar] [CrossRef]
- Junker, Y.; Zeissig, S.; Kim, S.J.; Barisani, D.; Wieser, H.; Leffler, D.A.; Zevallos, V.; Libermann, T.A.; Dillon, S.; Freitag, T.L.; et al. Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J. Exp. Med. 2012, 209, 2395–2408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palová-Jelínková, L.; Rozková, D.; Pecharová, B.; Bártová, J.; Sedivá, A.; Tlaskalová-Hogenová, H.; Spísek, R.; Tucková, L. Gliadin fragments induce phenotypic and functional maturation of human dendritic cells. J. Immunol. 2005, 175, 7038–7045. [Google Scholar] [CrossRef] [PubMed]
- Brottveit, M.; Beitnes, A.C.; Tollefsen, S.; Bratlie, J.E.; Jahnsen, F.L.; Johansen, F.E.; Sollid, L.M.; Lundin, K.E. Mucosal cytokine response after short-term gluten challenge in celiac disease and non-celiac gluten sensitivity. Am. J. Gastroenterol. 2013, 108, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Marciani, L.; Coleman, N.S.; Dunlop, S.P.; Singh, G.; Marsden, C.A.; Holmes, G.K.; Spiller, R.C.; Gowland, P.A. Gallbladder contraction, gastric emptying and antral motility: Single visit assessment of upper GI function in untreated celiac disease using echo-planar MRI. J. Magn. Reson. Imaging 2005, 22, 634–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraquelli, M.; Bardella, M.T.; Peracchi, M.; Cesana, B.M.; Bianchi, P.A.; Conte, D. Gallbladder emptying and somatostatin and cholecystokinin plasma levels in celiac disease. Am. J. Gastroenterol. 1999, 94, 1866–1870. [Google Scholar] [CrossRef] [PubMed]
- Marciani, L.; Pritchard, S.E.; Hellier-Woods, C.; Costigan, C.; Hoad, C.L.; Gowland, P.A.; Spiller, R.C. Delayed gastric emptying and reduced postprandial small bowel water content of equicaloric whole meal bread versus rice meals in healthy subjects: Novel MRI insights. Eur. J. Clin. Nutr. 2013, 67, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Coletta, M.; Gates, F.K.; Marciani, L.; Shiwani, H.; Major, G.; Hoad, C.L.; Chaddock, G.; Gowland, P.A.; Spiller, R.C. Effect of bread gluten content on gastrointestinal function: A crossover MRI study on healthy humans. Br. J. Nutr. 2016, 115, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Bortolotti, M.; Santi, V.; Calletti, T.; Gaiani, S.; Labò, G. Measurement of gastric emptying time by real-time ultrasonography. Gastroenterology 1985, 89, 752–759. [Google Scholar] [CrossRef]
- Di Stefano, M.; Carnevale Maffè, G.; Bergonzi, M.; Mengoli, C.; Formagnana, P.; Di Sabatino, A.; Corazza, G.R. The effect of gluten on intestinal fermentation, gastric and gallbladder emptying in healthy volunteers. Dig. Liver Dis. 2015, 47, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Dodds, W.J.; Groh, W.J.; Darweesh, R.M.; Lawson, T.L.; Kishk, S.M.; Kern, M.K. Sonographic measurement of gallbladder volume. Am. J. Roentgenol. 1985, 145, 1009–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapone, A.; Lammers, K.M.; Casolaro, V.; Cammarota, M.; Giuliano, M.T.; De Rosa, M.; Stefanile, R.; Mazzarella, G.; Tolone, C.; Russo, M.I.; et al. Divergence of gut permeability and mucosal immune gene expression in two gluten-associated conditions: Celiac disease and gluten sensitivity. BMC Med. 2011, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Sapone, A.; Lammers, K.M.; Mazzarella, G.; Mikhailenko, I.; Cartenì, M.; Casolaro, V.; Fasano, A. Differential mucosal IL-17 expression in two gliadin-induced disorders: Gluten sensitivity and the autoimmune enteropathy celiac disease. Int. Arch. Allergy Immunol. 2010, 152, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.; Dall, M.; Antvorskov, J.C.; Weile, C.; Engkilde, K.; Josefsen, K.; Buschard, K. Dietary gluten increases natural killer cell cytotoxicity and cytokine secretion. Eur. J. Immunol. 2014, 44, 3056–3067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardella, M.T.; Fraquelli, M.; Peracchi, M.; Cesana, B.M.; Bianchi, P.A.; Conte, D. Gastric emptying and plasma neurotensin levels in untreated celiac patients. Scand. J. Gastroenterol. 2000, 35, 269–273. [Google Scholar] [PubMed]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology 2013, 145, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Mansueto, P.; Seidita, A.; D’Alcamo, A.; Carroccio, A. Role of FODMAPs in patients with irritable bowel syndrome. Nutr. Clin. Pract. 2015, 30, 665–682. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A.; Hasler, W.L. Rome IV-functional GI disorders: Disorders of gut-brain interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | Gluten-Containing Meal | Gluten-Free Meal | p |
|---|---|---|---|
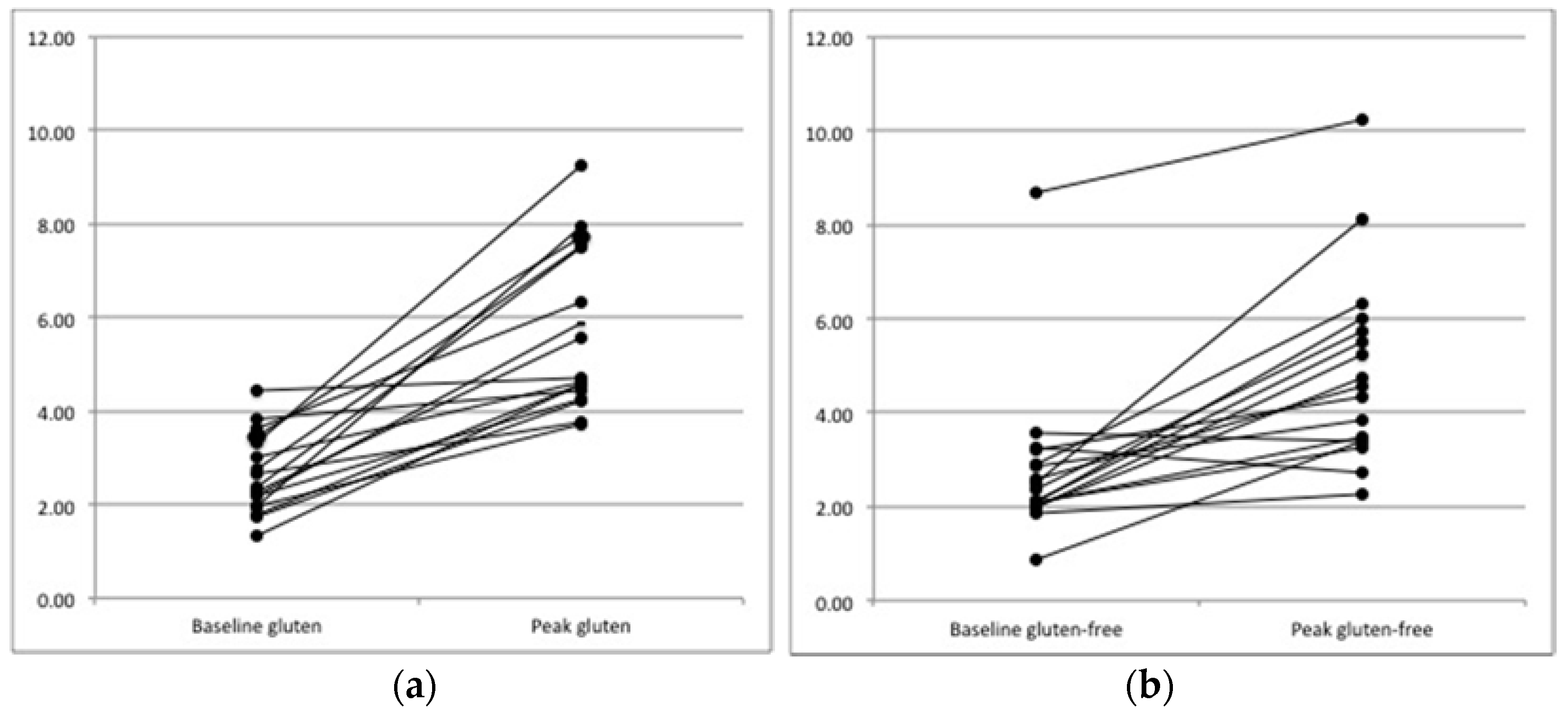
| Gastric filling peak area in cm2, median (range) | 4.70 (3.71–9.27) | 4.57 (2.27–10.22) | 0.023 |
| Difference peak-basal area in cm2, median (range) | 3.02 ± 1.74 | 1.89 ± 1.68 | 0.01 |
| Time to peak mins, mean (SD) | 45.9 ± 30.2 | 52.9 ± 34.4 | 0.47 |
| Gastric emptying time mins, mean (SD) | 222.4 (81.5) | 202 (65.0) | 0.37 |
| Parameters | Gluten-Containing Meal | Gluten-Free Meal | p |
|---|---|---|---|
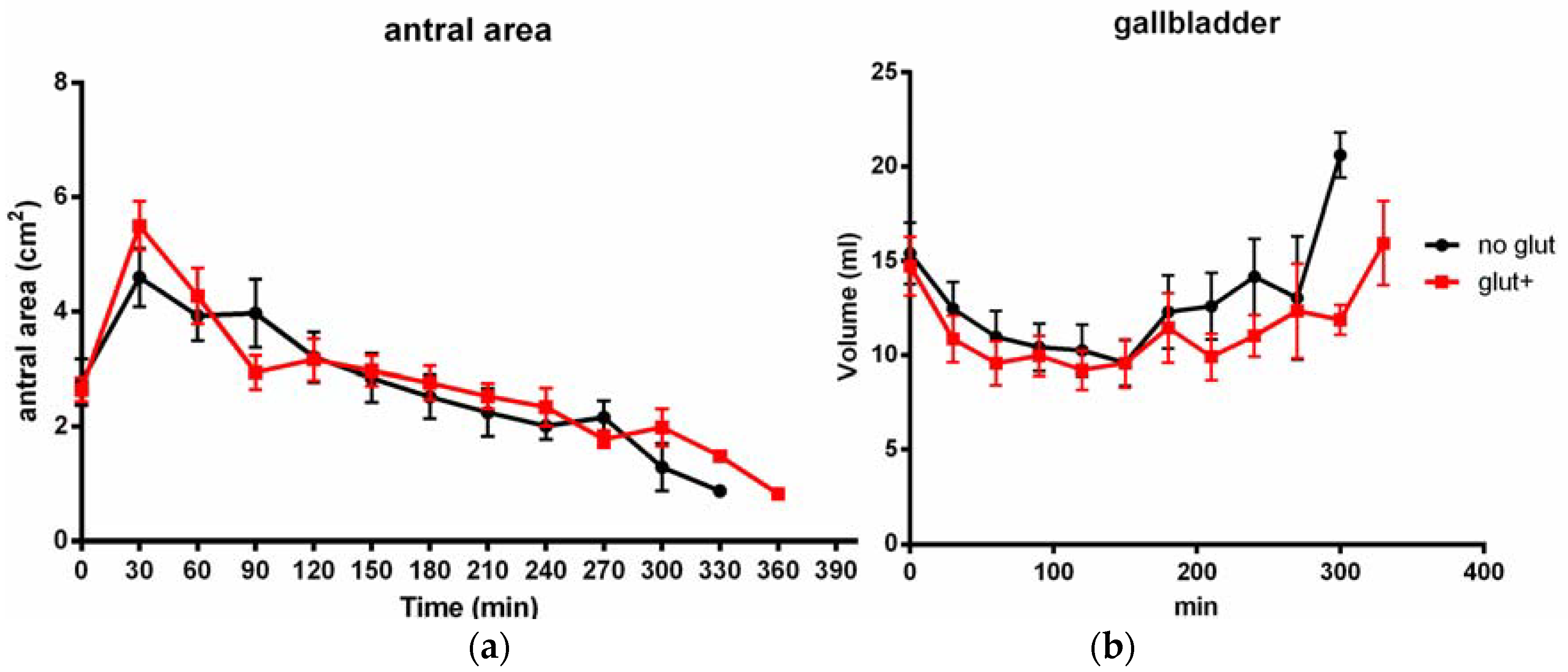
| GB basal volume mL, mean (SD) | 14.7 (6.5) | 15.4 (6.8) | 0.76 |
| Gallbladder ejection fraction %, mean (SD) | 44.4 (28.1) | 44.2 (28.1) | 0.9 |
| GB volume at 240 min mL, median (range) | 10.8 (5.2–13.4) | 14.3 (12.1–21.2) | 0.039 |
| Pattern of GB contraction mL*min, AUC | 3711 | 3630 | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massironi, S.; Branchi, F.; Fraquelli, M.; Baccarin, A.; Somalvico, F.; Ferretti, F.; Conte, D.; Elli, L. Effects of a Gluten-Containing Meal on Gastric Emptying and Gallbladder Contraction. Nutrients 2018, 10, 910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070910
Massironi S, Branchi F, Fraquelli M, Baccarin A, Somalvico F, Ferretti F, Conte D, Elli L. Effects of a Gluten-Containing Meal on Gastric Emptying and Gallbladder Contraction. Nutrients. 2018; 10(7):910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070910
Chicago/Turabian StyleMassironi, Sara, Federica Branchi, Mirella Fraquelli, Alessandra Baccarin, Francesco Somalvico, Francesca Ferretti, Dario Conte, and Luca Elli. 2018. "Effects of a Gluten-Containing Meal on Gastric Emptying and Gallbladder Contraction" Nutrients 10, no. 7: 910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070910