Wheat Albumin Increases the Ratio of Fat to Carbohydrate Oxidation during the Night in Healthy Participants: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Consent to Participate
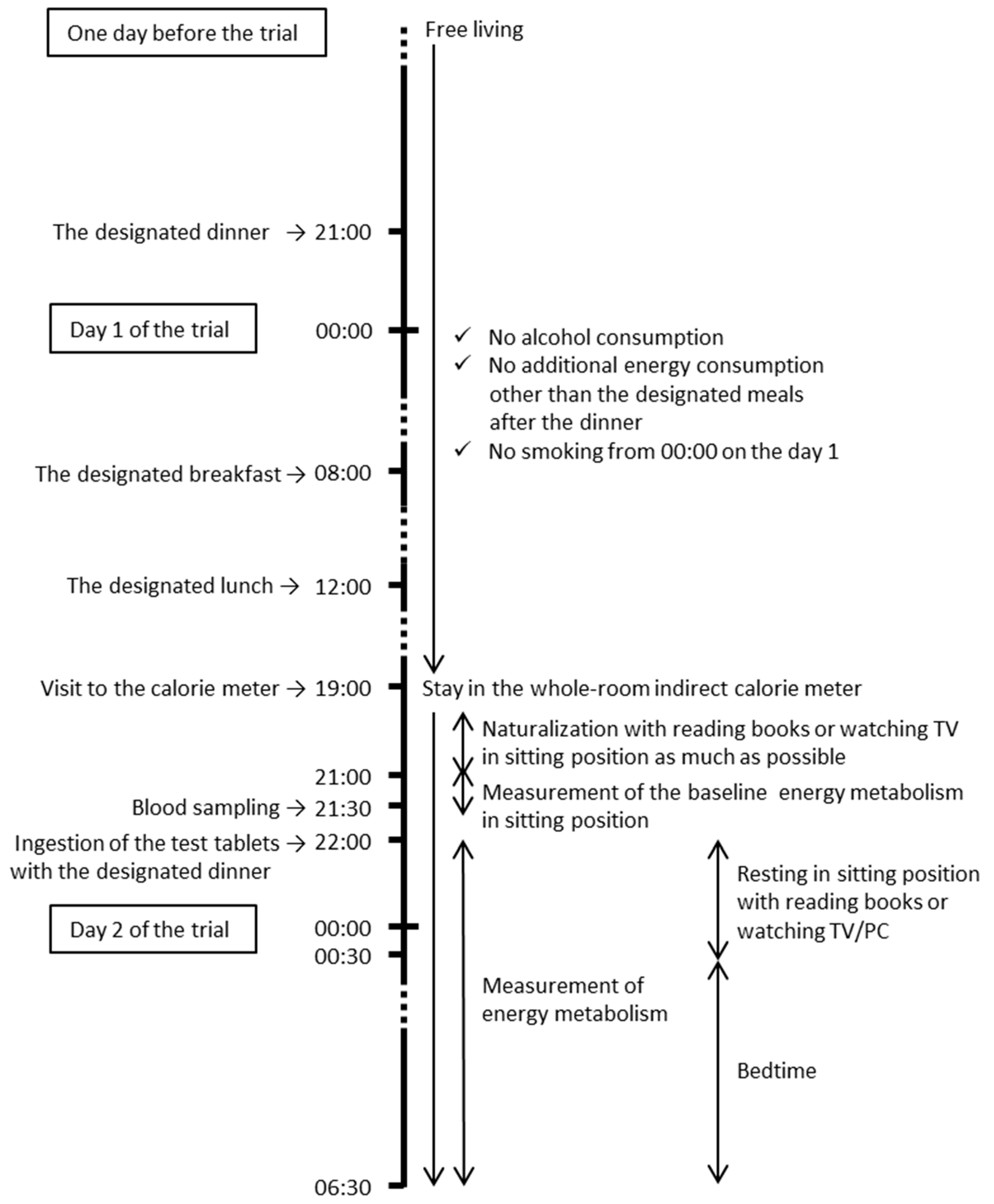
2.2. Study Design
2.3. Participants
2.4. Test Tablets
2.5. Whole-Room Indirect Calorie Meter
2.6. Blood Samples
2.7. Statistics
3. Results
3.1. Characteristics of the Participants
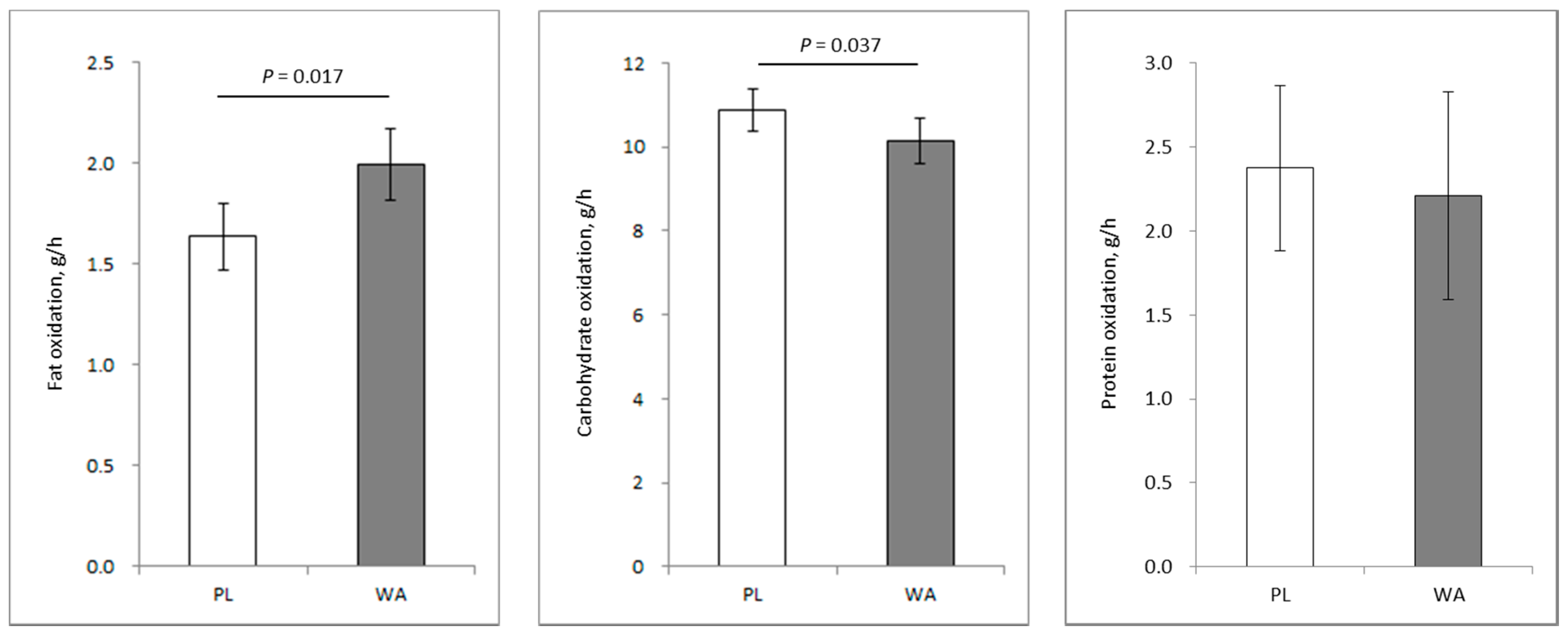
3.2. Substrate Utilization
3.3. EE and RQ
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zurlo, F.; Lillioja, S.; Esposito-Del Puente, A.; Nyomba, B.L.; Raz, I.; Saad, M.F.; Swinburn, B.A.; Knowler, W.C.; Bogardus, C.; Ravussin, E. Low ratio of fat to carbohydrate oxidation as predictor of weight gain: Study of 24-h RQ. Am. J. Physiol. 1990, 259, E650–E657. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.; Scalfi, L.; Contaldo, F.; Pasanisi, F. Fasting respiratory quotient as a predictor of long-term weight changes in non-obese women. Ann. Nutr. Metab. 2004, 48, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T.P.; Marchetti, C.M.; Krishnan, R.K.; Gonzalez, F.; Kirwan, J.P. Effects of aging on basal fat oxidation in obese humans. Metabolism 2008, 57, 1141–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodama, T.; Miyazaki, T.; Kitamura, I.; Suzuki, Y.; Namba, Y.; Sakurai, J.; Torikai, Y.; Inoue, S. Effects of single and long-term administration of wheat albumin on blood glucose control: Randomized controlled clinical trials. Eur. J. Clin. Nutr. 2005, 59, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Schutz, Y. Concept of fat balance in human obesity revisited with particular reference to de novo lipogenesis. Int. J. Obes. Relat. Metab. Disord. 2004, 28, S3–S11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J.; Collins, L.C.; Nannini, L.; Stamford, B.A. Potentiating effects of cigarette smoking and moderate exercise on the thermic effect of a meal. Int. J. Obes. Relat. Metab. Disord. 1992, 16, 341–347. [Google Scholar] [PubMed]
- Hibi, M.; Masumoto, A.; Naito, Y.; Kiuchi, K.; Yoshimoto, Y.; Matsumoto, M.; Katashima, M.; Oka, J.; Ikemoto, S. Nighttime snacking reduces whole body fat oxidation and increases LDL cholesterol in healthy young women. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R94–R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henning, B.; Lofgren, R.; Sjostrom, L. Chamber for indirect calorimetry with improved transient response. Med. Biol. Eng. Comput. 1996, 34, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, E. On simple formulae for calculating the heat expenditure and the quantities of carbohydrate and fat oxidized in metabolism of men and animals, from gaseous exchange (Oxygen intake and carbonic acid output) and urine-N. Acta Physiol. Pharmacol. Neerl. 1957, 6, 795–802. [Google Scholar] [PubMed]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frisancho, A.R. Reduced rate of fat oxidation: A metabolic pathway to obesity in the developing nations. Am. J. Hum. Biol. 2003, 15, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Piaggi, P.; Thearle, M.S.; Bogardus, C.; Krakoff, J. Lower energy expenditure predicts long-term increases in weight and fat mass. J. Clin. Endocrinol. Metab. 2013, 98, E703–E707. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Yamada, Y.; Tsukiyama, K.; Miyawaki, K.; Hosokawa, M.; Nagashima, K.; Toyoda, K.; Naitoh, R.; Mizunoya, W.; Fushiki, T.; et al. Gastric inhibitory polypeptide modulates adiposity and fat oxidation under diminished insulin action. Biochem. Biophys. Res. Commun. 2005, 335, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Seino, Y.; Fukushima, M.; Yabe, D. GIP and GLP-1, the two incretin hormones: Similarities and differences. J. Diabetes Investig. 2010, 1, 8–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimotoyodome, A.; Suzuki, J.; Fukuoka, D.; Tokimitsu, I.; Hase, T. RS4-type resistant starch prevents high-fat diet-induced obesity via increased hepatic fatty acid oxidation and decreased postprandial GIP in C57BL/6J mice. Am. J. Physiol. Endocrinol. Metab. 2010, 298, E652–E662. [Google Scholar] [CrossRef] [PubMed]
- Flatt, J.P.; Ravussin, E.; Acheson, K.J.; Jequier, E. Effects of dietary fat on postprandial substrate oxidation and on carbohydrate and fat balances. J. Clin. Investig. 1985, 76, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered eating and obesity: Associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Number of participants (male/female) | 20 (14/6) |
| Age, years | 38 ± 10 |
| Body weight, kg | 62.4 ± 9.8 (M, 67.7 ± 7.7; F, 51.9 ± 4.0) |
| Body mass index, kg/m2 | 21.8 ± 1.9 |
| Fat mass, kg | 12.5 ± 2.9 |
| Fat free mass, kg | 49.8 ± 8.2 |
| Systolic blood pressure, mmHg | 124 ± 18 |
| Diastolic blood pressure, mmHg | 73 ± 14 |
| Glucose, mmol/L | 5.36 ± 0.31 |
| Insulin, pmol/L | 19.2 ± 7.2 |
| Triglyceride, mg/dL | 0.894 ± 0.485 |
| Parameter | PL | WA |
|---|---|---|
| Energy, kJ/day | 8299 ± 1616 | 8464 ± 1610 |
| Protein, g/day | 72.1 ± 18.0 | 69.5 ± 17.6 |
| Fat, g/day | 64.2 ± 19.4 | 68.7 ± 22.7 |
| Carbohydrate, g/day | 249.2 ± 54.5 | 250.5 ± 46.1 |
| Parameter | PL | WA |
|---|---|---|
| EE, kJ/h | 1148 ± 139 | 1142 ± 122 |
| RQ, L/L/h | 0.904 ± 0.027 | 0.890 ± 0.032 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, S.; Sakuda, T.; Shudo, A.; Sugiura, Y.; Osaki, N. Wheat Albumin Increases the Ratio of Fat to Carbohydrate Oxidation during the Night in Healthy Participants: A Randomized Controlled Trial. Nutrients 2019, 11, 197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010197
Saito S, Sakuda T, Shudo A, Sugiura Y, Osaki N. Wheat Albumin Increases the Ratio of Fat to Carbohydrate Oxidation during the Night in Healthy Participants: A Randomized Controlled Trial. Nutrients. 2019; 11(1):197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010197
Chicago/Turabian StyleSaito, Shinichiro, Toshitaka Sakuda, Aiko Shudo, Yoko Sugiura, and Noriko Osaki. 2019. "Wheat Albumin Increases the Ratio of Fat to Carbohydrate Oxidation during the Night in Healthy Participants: A Randomized Controlled Trial" Nutrients 11, no. 1: 197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010197