Patient Involvement in Education of Nutrition and Dietetics Students: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
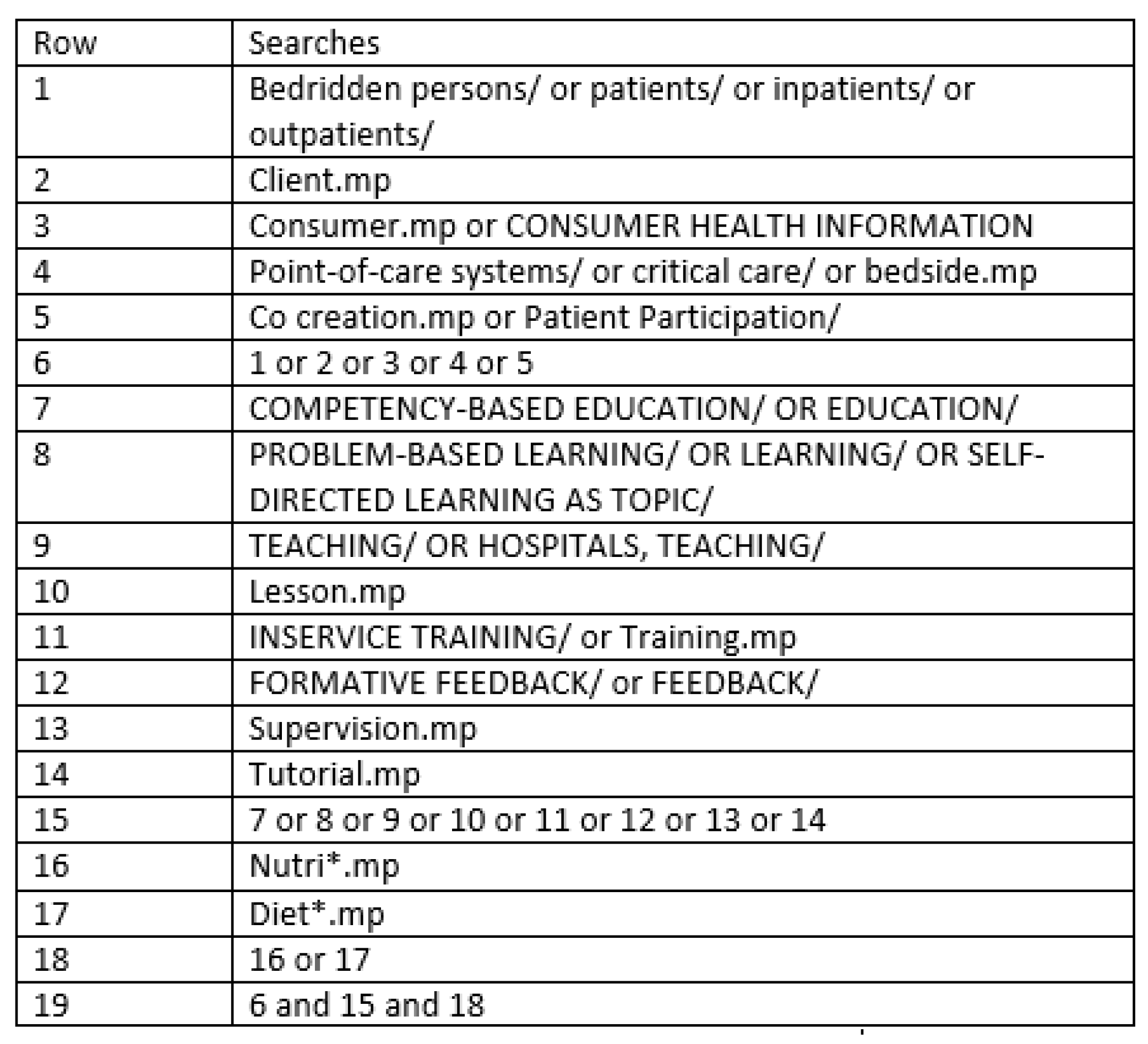
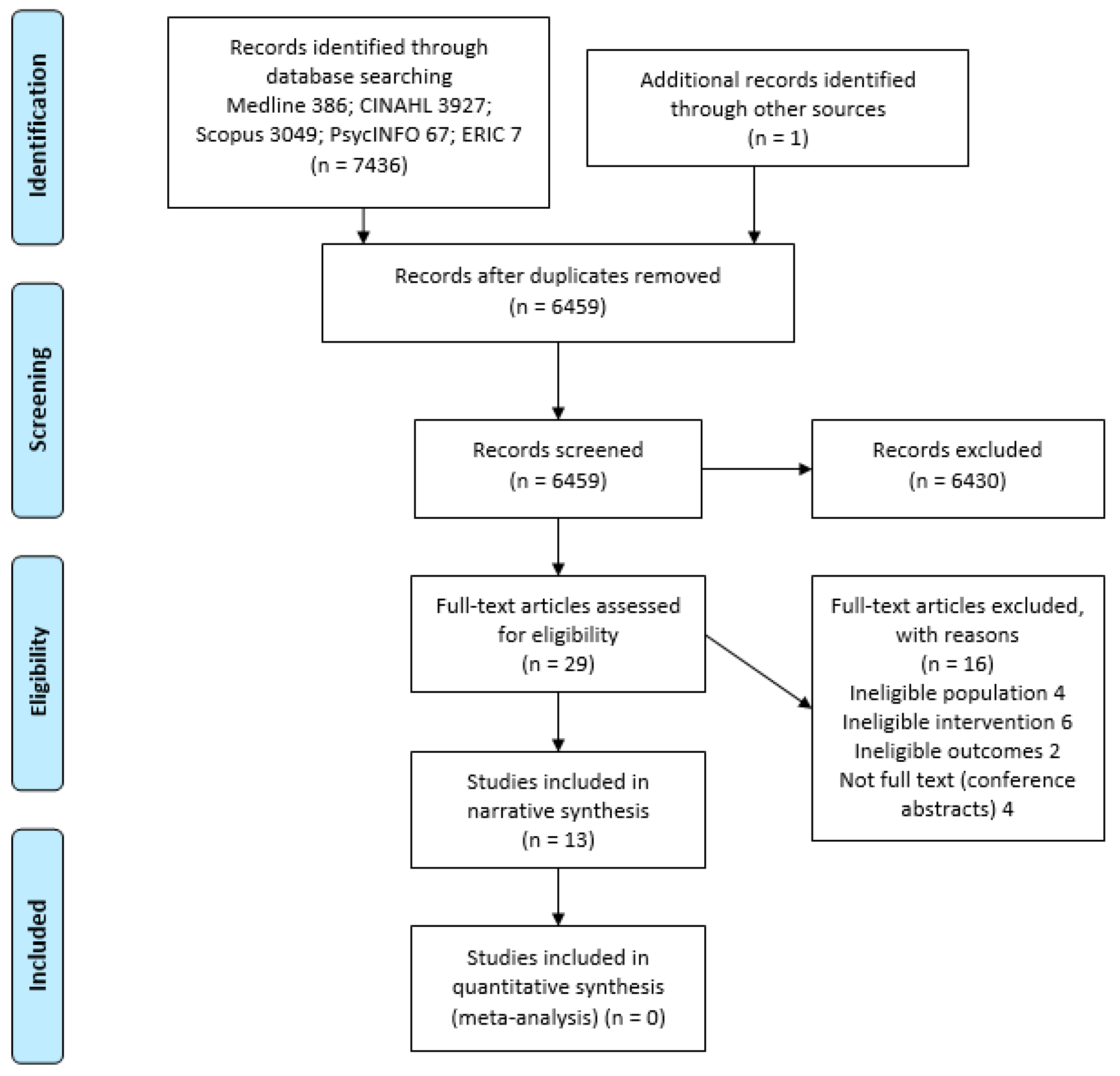
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Congress of Dietetic Association. ICDA Strategic Plan 2017–2020. Available online: https://www.internationaldietetics.org/Downloads/ICDA-STRATEGIC-PLAN-2012-TO-2016.aspx (accessed on 18 March 2019).
- Wright, O.R.L.; Capra, S.M. Entrustable professional activities for nutrition and dietetics practice: Theoretical development. Focus Health Prof. Educ. 2017, 18, 31–43. [Google Scholar] [CrossRef]
- Rees, C.E.; Knight, L.V.; Wilkinson, C.E. “User involvement is a sine qua non, almost, in medical education”: Learning with rather than just about health and social care service users. Adv. Health Sci. Educ. 2007, 12, 359–390. [Google Scholar] [CrossRef]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.L.; Pomey, M.P. Engaging patients to improve quality of care: A systematic review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef]
- Karazivan, P.; Pomey, M.P.; Ghadari, D.P.; Jouet, E. The patient-as-partner approach in healthcare: A conceptual framework for a necessary transition. Acad. Med. 2015, 90, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Entwistle, V.A.; Cribb, A.; Watt, I.S.; Skea, Z.C.; Owens, J.; Morgan, H.M.; Christmas, S. “The more you know, the more you realise it is really challenging to do”: Tensions and uncertainties in person-centred support for people with long-term conditions. Patient Educ. Couns. 2018, 101, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Sladdin, I.; Ball, L.; Bull, C.; Chaboyer, W. Patient-centred care to improve dietetic practice: An integrative review. J. Hum. Nutr. Diet. 2017, 30, 453–470. [Google Scholar] [CrossRef] [PubMed]
- Maclellan, D.L.; Berenbaum, S. Client-centred nutrition counselling: Do we know what this means? Can. J. Diet. Pract. Res. 2003, 64, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, A.; Bligh, J. Students learning from patients: let’s get real in medical education. Adv. Health Sci. Educ. 2008, 13, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.; Blackmore, D.; Heard, S.; McCorie, P.; McHaffie, D.; Scherpbier, A.; Gupta, T.S.; Kuldip, S.; Southgate, L. Patient-oriented learning: A review of the role of the patient in the education of medical students. Med. Educ. 2000, 34, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Costello, J.; Horne, M. Patients as teachers? An evaluative study of patients’ involvement in classroom teaching. Nurse Educ. Pract. 2001, 1, 94–102. [Google Scholar] [CrossRef]
- Stockhausen, L.J. The patient as experience broker in clinical learning. Nurse Educ. Pract. 2009, 9, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Stacy, R.; Spencer, J. Patients as teachers: A qualitative study of patients’ views on their role in a community-based undergraduate project. Med. Educ. 1999, 33, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Suikkala, A.; Koskinen, S.; Leino-Kilpi, H. Patients’ involvement in nursing students’ clinical education: A scoping review. Int. J. Nurs. Stud. 2018, 84, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Rowland, P.; Anderson, M.; Kumagai, A.K.; McMillan, S.; Sandhu, V.; Langlois, S. Patient involvement in health professionals’ education: A meta-narrative review. Adv. Health Sci. Educ. 2018. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 21, e1000097. [Google Scholar] [CrossRef]
- PROSPERO. International Prospective Register of Systematic Reviews. 2019. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42019124085 (accessed on 16 November 2019).
- Endnote X8; Clarivate Analytics: Philadelphia, PA, USA, 2017.
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2011. [Google Scholar]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2018.
- Reed, D.A.; Cook, D.A.; Beckman, T.J.; Levine, R.B.; Kern, D.E.; Wright, S.M. Association between funding and quality of published medical education research. J. Am. Med. Assoc. 2007, 298, 1002–1009. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist.pdf (accessed on 5 May 2018).
- Kirkpatrick, D.L. Evaluation of training. In Training and Development Handbook; Craig, R., Bittel, L., Eds.; McGraw-Hill: New York, NY, USA, 1967; pp. 87–112. [Google Scholar]
- Yardley, S.; Dornan, T. Kirkpatrick’s levels and education “evidence”. Med. Educ. 2012, 46, 97–106. [Google Scholar] [CrossRef]
- Beshgetoor, D.; Wade, D. Use of actors as simulated patients in nutritional counseling. J. Nutr. Educ. Behav. 2007, 39, 101–102. [Google Scholar] [CrossRef]
- Brightwell, D.R.; Sloan, C.L. Graduate students and faculty learn behavior therapy of obesity. J. Nutr. Educ. Behav. 1976, 8, 71–72. [Google Scholar] [CrossRef]
- Dobson, R.; Taylor, J.; Cassidy, J.; Walker, D.; Proctor, P.; Perepelkin, J. Interprofessional and intraprofessional teams in a standardized patient assessment lab. Pharm. Educ. 2007, 7, 159–166. [Google Scholar] [CrossRef]
- Gibson, S.J.; Golder, J.; Cant, R.P.; Davidson, Z.E. An Australian mixed methods pilot study exploring students performing patient risk screening. Nurs. Health Sci. 2016, 18, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Horacek, T.M.; Salomón, J.E.; Nelsen, E.K. Evaluation of dietetic students’ and interns’ application of a lifestyle-oriented nutrition-counseling model. Patient Educ. Couns. 2007, 68, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Clasen, C.; Canfield, A. Effectiveness of service learning and learning through service in dietetics education. J. Allied Health 2003, 32, 275–278. [Google Scholar] [PubMed]
- Schwartz, V.S.; Rothpletz-Puglia, P.; Denmark, R.; Byham-Gray, L. Comparison of standardized patients and real patients as an experiential teaching strategy in a nutrition counseling course for dietetic students. Patient Educ. Couns. 2015, 98, 168–173. [Google Scholar] [CrossRef]
- Simper, T.N.; Breckon, J.D.; Kilner, K. Effectiveness of training final-year undergraduate nutritionists in motivational interviewing. Patient Educ. Couns. 2017, 100, 1898–1902. [Google Scholar] [CrossRef]
- Tada, T.; Moritoshi, P.; Sato, K.; Kawakami, T.; Kawakami, Y. Effect of simulated patient practice on the self-efficacy of Japanese undergraduate dietitians in nutrition care process skills. J. Nutr. Educ. Behav. 2018, 50, 610–619. [Google Scholar] [CrossRef]
- Gibson, S.J.; Davidson, Z.E. An observational study investigating the impact of simulated patients in teaching communication skills in preclinical dietetic students. J. Hum. Nutr. Diet. 2016, 29, 529–536. [Google Scholar] [CrossRef]
- Hampl, J.S.; Herbold, N.H.; Schneider, M.A.; Sheeley, A.E. Using standardized patients to train and evaluate dietetics students. J. Am. Diet. Assoc. 1999, 99, 1094–1097. [Google Scholar] [CrossRef]
- Henry, B.W.; Duellman, M.C.; Smith, T.J. Nutrition-based standardized patient sessions increased counseling awareness and confidence among dietetic interns. Top. Clin. Nutr. 2009, 24, 25–34. [Google Scholar] [CrossRef]
- Swanepoel, E.; Tweedie, J.; Maher, J. Building dietetic student confidence and professional identity through participation in a university health clinic. Nutr. Diet. 2016, 73, 229–234. [Google Scholar] [CrossRef]
- Wykurz, G.; Kelly, D. Developing the role of patients as teachers: Literature review. Br. Med. J. 2002, 325, 818–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauphinee, W.D. Educators must consider patient outcomes when assessing the impact of clinical training. Med. Educ. 2012, 46, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Kent, F.; Molloy, E. Patient feedback in physiotherapy clinical education: A mixed methods study. Focus Health Prof. Educ. 2013, 14, 21–34. [Google Scholar]
- Nestel, D.; Clark, S.; Tabak, D.; Ashwell, V.; Muir, E.; Paraskevas, P.; Higham, J. Defining responsibilities of simulated patients in medical education. Simul. Healthc. 2010, 5, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Vail, R.; Mahon-Salazar, C.; Morrison, A.; Kalet, A. Patients as teachers: An integrated approach to teaching medical students about the ambulatory care of HIV-infected patients. Patient Educ. Couns. 1996, 27, 95–101. [Google Scholar] [CrossRef]
- Jha, V.; Quinton, N.D.; Bekker, H.L.; Roberts, T.E. Strategies and interventions for the involvement of real patients in medical education: A systematic review. Med. Educ. 2009, 43, 10–20. [Google Scholar] [CrossRef]
- Davidson, R.; Duerson, M.; Rathe, R.; Pauly, R.; Watson, R.T. Using standardized patients as teachers: A concurrent controlled trial. Acad. Med. 2001, 76, 840–843. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author Date, Country | Setting | Student Characteristics | Patient Characteristics | Study Design | Outcome Measures |
|---|---|---|---|---|---|
| Beshgetoor [25] 2007, USA | Simulated settings including clinics, hospital | Dietetic students (number unspecified) enrolled in a senior level community nutrition course | SP as patients of various cultural and nutritional backgrounds. | Post-test survey completed by students | Student perceived effectiveness and value |
| Brightwell [26] 1976, USA | Not specified | n = 10 undergraduate dietetic students | 11 female and 1 male patients underwent weight reduction counselling by students. 9 patients (75% retention) completed the program | Mixed methods – patient anthropometry measurements and qualitative interviews of students | Post-programme patient weight change and student perceptions of counselling patients |
| Dobson [27] 2007, Canada | Osteoporosis assessment laboratory | pharmacy, nutrition and physical therapy n = 25 3rd year nutrition students | 6 female SP role-played a patient with a newly diagnosed vertebral compression fracture | Pre- and post-test of researcher developed survey (6 statements, 7-point Likert scale) administered to students | Attitudes and experiences of working in inter professional team |
| Gibson [28] 2015, Australia | University | n = 215 3rd year undergraduate dietetic students | SP role-played a simple nutritional condition congruent with the concurrently taught academic content including communication skill development | Observational study using researcher-developed survey measuring communication skills by dietetic educators | Communication skill development |
| Gibson [34] 2016, Australia | Hospital | n = 58 pre-clinical 3rd year dietetic students | Hospital patients in medical, rehabilitation, surgical, and coronary care wards | Mixed method case-control study, using a survey developed by other authors and 6 focus groups at placement completion. Intervention group completed patient malnutrition screening activity; control group had usual orientation activities. | Student feelings of preparedness for placement; student perceptions of participating in screening activity |
| Hampl [35] 1999, USA | University | n = 14 undergraduate student dietitians | SP in role of 17-year-old pregnant woman | Qualitative evaluation of student-SP interviews using a questionnaire, primarily composed of open-ended questions | Student perceptions of participating in activity |
| Henry [36] 2009, USA | Family counselling centre | n = 11 dietetic interns (mean age 25 years) near midpoint of supervised practice experience. | 4 SPs (mean age 25 years) recruited from the first-year graduate students in the marriage and family therapy programme. | Qualitative study using focus groups (n = 10 dietetic interns) | Student perceptions of effectiveness of SP sessions on counselling competence |
| Horacek [25] 2007, USA | Unspecified private location | n = 121 dietetic students and interns | Patients were identified through campus recreation services or a wellness programme. | Mixed methods: Students and supervising dietitians used a modified version of the Dietitian’s Interviewing Rating Scale to evaluate session. Clients evaluated the counselling experience and skills in a post-interview survey. | Student, supervising dietitian, and client perceptions of counselling sessions; outcomes were compared between groups. |
| Kim [30] 2003, USA | Senior Citizens Centre | n = 49 dietetic students enrolled in Nutrition for the Ageing unit | 150 elderly people attending the Senior Citizens Centre for meals | Pre and post evaluation questionnaires | Student attitudes towards community service before and after service learning experiences |
| Schwartz [31] 2014,USA | University | n = 75 dietetic students | Real patients who were recruited from community for healthy eating or weight loss advice; SPs were actors with abdominal obesity | Retrospective evaluation of student-patient consultation video recordings (n = 138) by recent nutrition course graduates trained to use rating tool | Rating of student communication and promoting behaviour change skills |
| Simper [32] 2017, UK | Not specified | n = 52 students from a final year undergraduate nutrition cohort | Actor familiar with motivational interviewing approach | Repeated measures design where students were videoed and videos were coded for motivational interviewing behaviours | Student behaviour and global ratings related to motivational interviewing |
| Swanepoel [37] 2016, Australia | University weight management clinic | n = 13 third-year dietetic students (43% of total enrolment) | Clients were university staff attending the university weight management clinic | Qualitative study design: student focus groups used to explore the impact of participation | Student perceived confidence and skills |
| Tada [33] 2018, Japan | Private Japanese university | n = 90 third-year dietetics undergraduates aged 20–38 years | SPs as elderly patients in hospital and home setting | Pre- and post- survey using researcher-developed questionnaire | Student self-efficacy across 7 nutrition professional practice competencies |
| First Author | Educational Role of the Patient | Student Related Outcomes (e.g., Learning, Perceptions) | Kirkpatrick’s Levels | Patient Related Outcomes |
|---|---|---|---|---|
| Beshgetoor [25] | SPs played patients with body weight issues, health-related risks, and resources for food procurement. Scenarios represented patients of diverse ages and ethnic backgrounds | Students perceived learning to be effective and the SP encounter useful for learning. | 2a | None |
| Brightwell [26] | Overweight/ obese patients received weight reduction counselling by students | Learned new techniques; chance to work with real patients (and see them be successful); improved relationships with patients. | 4b | All patients lost weight (2.0–18.2kg) |
| Dobson [27] | SP were interviewed for data collection | Students perceived they performed better than expected with regard to their ability to contribute to the interview, the patient care plan, and communication skills. | 2a | None |
| Gibson [28] | SP provided feedback on student communication skills | No significant improvement in communication skills from formative to summative evaluation, but significant improvement made for failing and borderline students. | 3 | None |
| Gibson [34] | Hospital patients were screened for malnutrition | Improved student-perceived communication skills and mean of all skills (background knowledge, professional attributes, professionalism, communication skills, overall placement preparedness) in patient screening group compared with control group. | 2a | Malnutrition screening performed satisfactorily |
| Hampl [35] | SP was interviewed and counselled by students and provided them with feedback | Students perceived the learning experience as valuable learning experience; range of perceptions regarding authenticity of setting, immediate feedback from SP, and instructor enhanced learning, SP feedback was helpful, informative, and encouraging. | 2a | None |
| Henry [36] | SP provided feedback to students, however, it was unclear if this was in their patient capacity | Students reported varying levels of confidence, with videoing of session adding to anxiety; students perceived improved confidence and competence; valued opportunity to practise a second time. | 2a | None |
| Horacek [29] | Real patients received dietetic counselling from students and rated the experience and students’ counselling skills | Improved skills in knowledge, preparedness, communication skills, confidence, flexibility, and professionalism. | 3 | High satisfaction of counselling experience |
| Kim [30] | Senior citizens received meal-related services and nutrition education by students | Improved knowledge of community; improved understanding of resources, health care needs, barriers to receiving health care, impact of SES on health, importance of community programmes. Developed communication and “people” skills, improved writing and presentation skills, better understanding of older people. | 2a | None |
| Schwartz [31] | Real patients and SPs were counselled for weight reduction where the session was videoed | Quality of communication and behaviour change counselling skills were assessed as good to excellent, however change in student learning as a result of the intervention was not measured. | 3 | None |
| Simper [32] | SP received motivational interviewing from students | Improved motivational interviewing skills including reduced closed questions, increased reflections and affirmations, and reduced student: client speaking time ratio. | 3 | None |
| Swanepoel [37] | University staff attending a university-based weight management clinic were interviewed by students | Increased professional confidence; increased confidence in clinical skills; improved students’ perceived ability to identify skills required for practice; developed sense of professional identity; feedback from supervisor. | 2a | None |
| Tada [33] | SP played role of an elderly person in hospital and home settings | Improved self-efficacy in ethics, interpersonal skills, nutrition assessment, diagnosis, and care planning skills. Students reported enhanced learning and understanding, self-reflection, and confidence. | 2a | None |
| Author(s) | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Qualitative Studies Assessed Using the Critical Appraisal Skills Programme1 | |||||||||||
| Gibson [28] | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N/A |
| Hampyl [35] | N | Y | N | Y | N | N | N | N | N | N | N/A |
| Henry [36] | Y | Y | Y | N | Y | N | N | Y | Y | Y | N/A |
| Swanepoel [37] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N/A |
| Quantitative and mixed method studies assessed using the Medical Education Research Study Quality Instrument2 | |||||||||||
| Beshgetoor et al. [25] | 3 | 0.5 | 0.5 | 1 | 0 | 0 | 0 | 1 | 2 | 1 | 9 |
| Brightwell [26] | 1.5 | 0.5 | 1.5 | 3 | 0 | 0 | 0 | 1 | 1 | 3 | 11.5 |
| Dobson et al. [27] | 3 | 0.5 | 1.5 | 3 | 0 | 0 | 0 | 1 | 2 | 2 | 13 |
| Gibson & Davidson [34] | 1.5 | 0.5 | 1.5 | 3 | 0 | 0 | 0 | 1 | 2 | 2 | 11.5 |
| Horacek et al. [29] | 1.5 | 0.5 | 1.5 | 3 | 0 | 0 | 0 | 1 | 2 | 1.5 | 11 |
| Kim et al. [30] | 1.5 | 0.5 | 1.5 | 1 | 0 | 0 | 0 | 1 | 2 | 1.5 | 9 |
| Schwartz et al. [31] | 1 | 0.5 | 1.5 | 3 | 0 | 0 | 0 | 1 | 2 | 1.5 | 10.5 |
| Simper [32] | 1.5 | 0.5 | 1 | 3 | 0 | 0 | 0 | 1 | 2 | 2 | 11 |
| Tada [33] | 1.5 | 0.5 | 1.5 | 1 | 0 | 0 | 0 | 1 | 2 | 1.5 | 9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porter, J.; Kellow, N.; Anderson, A.; Bryce, A.; Dart, J.; Palermo, C.; Volders, E.; Gibson, S. Patient Involvement in Education of Nutrition and Dietetics Students: A Systematic Review. Nutrients 2019, 11, 2798. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112798
Porter J, Kellow N, Anderson A, Bryce A, Dart J, Palermo C, Volders E, Gibson S. Patient Involvement in Education of Nutrition and Dietetics Students: A Systematic Review. Nutrients. 2019; 11(11):2798. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112798
Chicago/Turabian StylePorter, Judi, Nicole Kellow, Amanda Anderson, Andrea Bryce, Janeane Dart, Claire Palermo, Evelyn Volders, and Simone Gibson. 2019. "Patient Involvement in Education of Nutrition and Dietetics Students: A Systematic Review" Nutrients 11, no. 11: 2798. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112798