1. Introduction
Childhood stunting is the most prevalent form of undernutrition in the world, with a 22% (151 million) global prevalence in children under five years old. Presently, 66% of stunted children live in low- and middle-income countries (LMICs) [
1]. In Malawi, 37% of children under five years old are stunted [
2]. Stunting reduces a child’s physical, immunological and cognitive capacities throughout his/her lifetime and is estimated to account for 21% of all disability-adjusted life years (DALYs) in children [
3]. Some factors that are associated with stunting include household and family food insecurity, household food allocation, abbreviated breast feeding, complementary feeding with low energy and nutrient density of traditional foods, reduced dietary diversity and frequent infections such as diarrhea, malaria, respiratory infections and environmental enteric dysfunction (EED) [
4,
5,
6,
7].
EED is a gut inflammatory asymptomatic condition that is characterized by T-cell infiltration of the intestinal mucosa, leading to chronic inflammation and blunting of the intestinal villi and thereby increasing intestinal permeability, translocation of gut microbes, micro- and macronutrient malabsorption, insufficient weight gain and stunted physical and cognitive development. While its etiology is poorly understood, poor hygiene and sanitation practices—particularly continuous exposure to fecal contamination—have been linked to the occurrence of EED [
8]. The gold standard for diagnosing EED is an intestinal biopsy; however, this method is invasive and therefore not ideal [
8]. The dual sugar absorption test is the most widely used marker of epithelial integrity. Other fecal and serum biomarkers such as fecal myeloperoxidase, calprotectin and neopterin are being studied for use in EED diagnosis. Like stunting and wasting, EED frequently occurs within the first three years of life, a period when infants transition from breastfeeding to complementary foods [
8].
In traditional sub-Saharan African societies, complementary feeding is dominated by monotonous, low-quality protein and micronutrient-poor starchy foods such as maize, cassava, rice and sorghum. To meet recommended daily dietary intakes, use of such complementary foods require frequent feeding, about five meals per day, but the required resources in terms of cooking fuel and caretaking time are limited, making this option ineffective [
3]. Dietary diversification is touted as an alternative, but in the face of general poverty this may not be an easy option for many rural communities to embrace, hence supplementation using locally available nutrient-dense foods may be considered a better option [
3,
9].
Protein-rich cereal legume blended flours such corn–soy blend (CSB) are the accepted standard dietary supplement in most LMICs where corn is the main staple. CSB is a fortified blended flour that contains selected micronutrients, sugar, maize and soy in different formulations depending on the manufacturer (typically 80:20 for corn and soy, respectively). CSB is used for prevention and treatment of acute malnutrition, wasting and growth retardation [
10]. However, CSB requires central processing, is not readily available and accessible to most poor populations and its efficacy in improving linear growth remains debatable [
11,
12]. Other more readily available nutrient-dense legumes to supplement complementary foods should thus be explored. We supplemented the complementary diets of children aged 6–23 months for 6–12 months with common bean or cowpea flours as alternatives to CSB, and we used CSB flour as a control. In children aged 6–12 months, the cowpea flour added to the weaning food improved linear growth compared to common bean and CSB [
13]; in 12–23-months-old children, the common bean supplement reduced lactulose excretion, a biomarker of gut health, but this did not result in better linear growth outcomes [
14]. In a secondary analysis of these two cohorts, we found higher rates of stunting, wasting and EED, despite adequate macronutrient consumption in Masenjere, a region that had a higher consumption of energy, carbohydrates and fats, better food security and Water, Sanitation and Hygiene (WASH) outcomes than Limera [
15].
More recently, research has indicated that dietary quality, especially protein quality, is important in assessing adequacy of diets to ameliorate the high rates of chronic and acute malnutrition in children consuming otherwise macro- and micronutrient-adequate diets [
16,
17,
18]. Protein quality refers to the availability and digestibility of amino acids after food has been digested, absorbed and met the minimal obligatory rates of oxidation. Protein digestibility corrected amino acid score (PDCAAS) is currently the most used method of protein quality assessment. The PDCAAS method calculates the first limiting amino acid ratio in a gram of the target protein food against a reference protein, which this is then multiplied by the target protein’s digestibility factor, thereby predicting the body’s utilization of that protein. Other methods of protein quality assessment include digestible indispensable amino acid score (DIAAS), protein efficiency ratio (PER), plasma amino acid ratio, nitrogen balance, nitrogen requirements for humans and use of a reference protein [
18]. Despite having a high protein content, plant-based diets have a low quality and low digestibility of proteins, as well as low amounts of bioavailable zinc, iron, calcium and other minerals. Animal-source foods (ASFs), on the other hand, provide better protein quality and bioavailability of vitamin B12, heme iron, vitamin A, zinc, calcium and other minerals [
19]. Some studies and systematic reviews have demonstrated lower rates of stunting in children that consumed animal-source foods (fish, meat, poultry, dairy products, eggs), than children that only consumed plant-based diets [
19,
20,
21,
22,
23,
24,
25,
26].
In this secondary analysis, we hypothesized that the type of food and protein quality of food consumed by children from Masenjere and Limera villages would differ, despite a lack of significant variation in mean macronutrient intake between the two communities, and that this could explain the differences in rates of stunting, acute malnutrition and EED that were observed in the populations.
3. Results
3.1. Baseline Characteristics of the Population
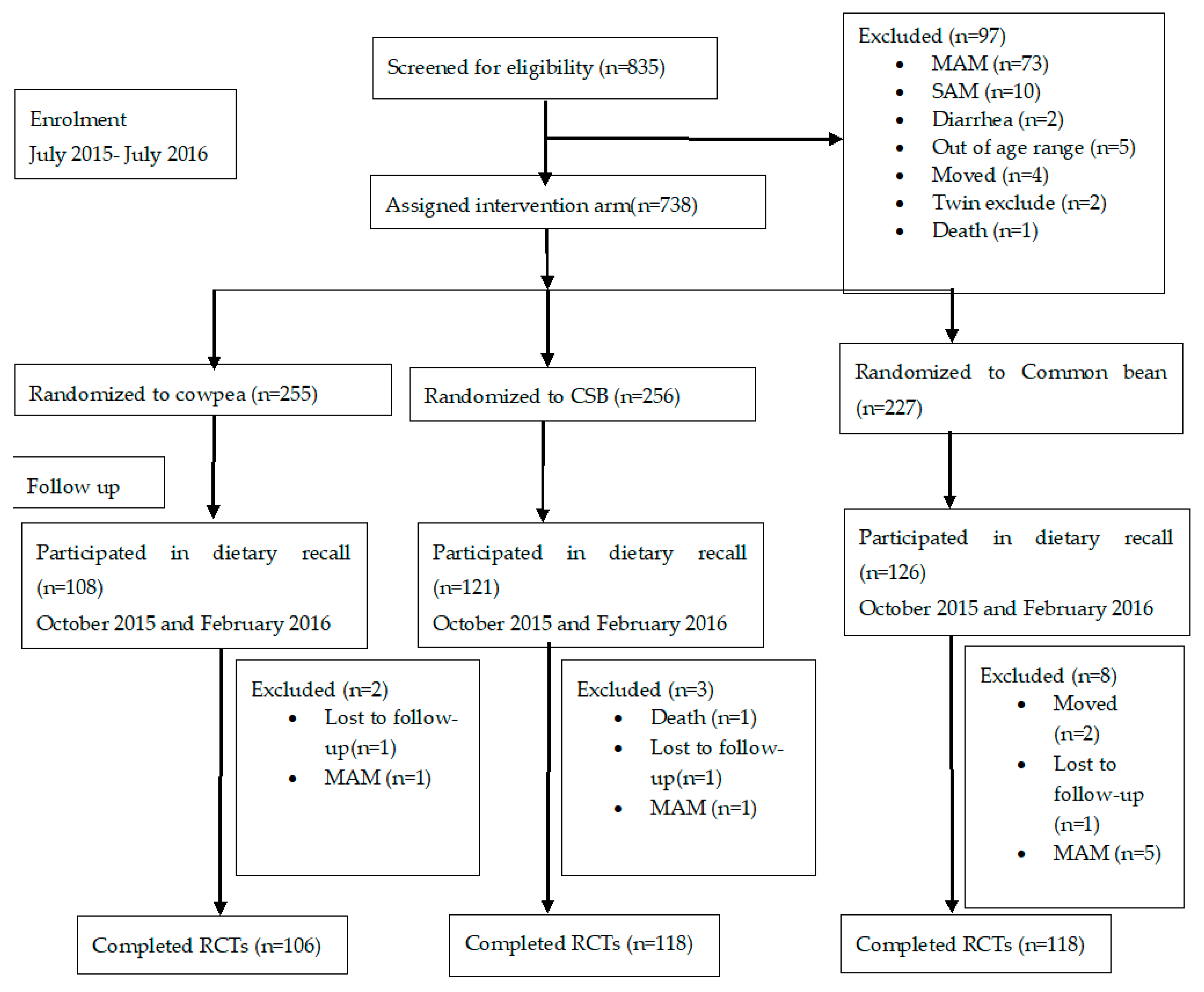
A total of 355 children participated in the dietary recalls—172 from RCT 1, and 183 from RCT 2 (
Figure 1). The characteristics of the study participants at baseline and at completion of the studies are reported in
Table 1. In RCT 1, 100% of the children from Masenjere had access to improved water sources compared to only 34% of children from Limera,
p < 0.001. A higher number of children from Masenjere slept in the same room as domesticated animals (chickens and goats) compared to children from Limera (43% vs. 15%, respectively,
p < 0.001). At the end of the study, children from Limera had better weight-for-length
z score (WLZ), length-for-age
z score (LAZ) and weight-for-age
z score (WAZ) compared to children in Limera,
p < 0.001,
p = 0.037 and
p < 0001, respectively. There were 14% and 13% more children from Masenjere that were stunted and underweight compared to children from Limera,
p = 0.048 and 0.003, respectively. No statistically significant results were observed for the other parameters.
In RCT 2, children from Limera had a higher mean weight, HAZ and WAZ, and a lower lactulose excretion than children from Masenjere, p = 0.041, p = 0.023, p = 0.027 and p = 0.034 at baseline, respectively. Children from Limera also had a higher number of siblings compared to those from Masenjere, p = 0.026. A higher number of children from Masenjere had access to an improved water source than children from Limera (99% vs. 45%, p < 0.001). At the end of the study, the change in WAZ was higher in children from Limera than Masenjere, p = 0.024. No statistically significant results were observed for the other parameters.
3.2. Type of Food Consumed
The foods, both composite and individual, consumed by children from both Masenjere and Limera are listed in
Table 2. Chicken, avocado, cabbage, coca cola, egg broth, okra, oranges and tea were only consumed by children from Masenjere, while pawpaw, peas, white beans, sugar plum, guavas and icicles were only consumed by children from Limera; however, these foods were consumed by less than 20% of the children in both RCT 1 and 2. The total number of times a particular food was consumed was higher in Masenjere than Limera (55% vs. 46%,
p < 0.001 in RCT 1 and 55 vs. 45,
p < 0.001 in RCT 2). Fish was the most consumed animal-source food in both regions; a higher number of children from Limera consumed statistically significantly more fish than from Masenjere (54% vs. 35%,
p = 0.009) in RCT 2. Solid meat was not consumed in either regions, only broth from meat stew was consumed, and this was statistically significantly higher in Masenjere than Limera (9% vs. 1%,
p = 0.018) in RCT 1 but not in RCT 2 (1% vs. 0%,
p = 0.313). In RCT 1, children from Limera consumed larger quantities of stiff maize porridge (nsima), red kidney beans and wheat flour fritters (mandasi) than children from Masenjere, leading to a statistically significant higher intake of energy (
p = 0.015,
p = 0.040 and
p < 0.001) and protein (
p = 0.023,
p = 0.040 and
p < 0.001), respectively, from these foods (
Table A1). A higher consumption of protein was observed from maize porridge in children from Masenjere than from Limera,
p = 0.0.001. In RCT 2, children from Masenjere consumed statistically significantly higher amounts of protein from maize porridge and mangoes than children from Limera,
p = 0.042 and
p = 0.022, respectively.
3.3. Comparison of Dietary Diversity of the Children
The mean ± SD dietary diversity score (DDS) of the children’s diets was higher in Masenjere compared to Limera (2.8 ± 1.0 vs. 2.5 ± 1.1,
p = 0.024), for RCT 2 but not RCT 1 (2.4 ± 1.2 vs. 2.3 ± 1.0,
p = 0.442) (
Table 3); this difference remained after adjusting for potential confounders (asset score, number of siblings, sex, age and season) in multivariate analysis (
p = 0.018). Grains, roots, and tubers were the most consumed food group by the children (77–79% in RCT 1 and 83–89% in RCT 2), while dairy products were rarely consumed by this population (1% in RCT 1 and 0–3% in RCT 2) with differences between the two regions (
p > 0.05). Children from Masenjere consumed more plant food groups, particularly legumes and nuts (32% vs. 12%,
p = 0.001) and vitamin A-rich fruits and vegetables, than children from Limera (85% vs. 59%,
p < 0.001) in RCT 2, and more vitamin A-rich fruits and vegetables (70% vs. 48%,
p = 0.003) in RCT 1. Flesh foods, defined as intake of solid meat (excluding broth), were more consumed by children from Limera than Masenjere in both RCT 1 (62% vs. 38%,
p = 0.001) and RCT 2 (59% vs. 43%,
p = 0.032). Eggs were consumed more by children from Masenjere than children from Limera in both RCT 1 (12% vs. 4%,
p = 0.048) and RCT 2 (17% vs. 5%,
p = 0.017). More than one-third of the children in RCT 1 (37% in Masenjere and 42% in Limera) and more than half of the children in RCT 2 (78% in Masenjere and 83% in Limera) did not meet the recommended MDD; there was no difference between the two regions (
p > 0.05).
3.4. Comparison of Protein Quality in the Diets of Children
The mean PDCAAS values for children from Masenjere and Limera were 77.7% and 73.8%, respectively, in RCT 1, and 70.9% and 71.8%, respectively, in RCT 2, with Lysine as the limiting amino acid in both studies, reflecting a high consumption of grain staples. The food items consumed only in Masenjere had an average PDCAAS of 70% and 72% in RCT 1 and 2, respectively, contributing 12.9 g (2.0 g in RCT 1 and 6.9 g in RCT 2) of bioavailable protein. The food items consumed only in Limera had an average PDCAAS of 75% and 71% in RCT 1 and 2, respectively, contributing 12.0 g (6.2 g in RCT 1 and 5.8 g in RCT 2) of bioavailable protein, while the PDCAAS values between the two regions were similar (p = 0.773). The food consumed in Limera contributed 3.1 g more bioavailable protein than from Masenjere (p = 0.035). Animal-source protein consumption (defined as consuming chicken, fish or eggs at least once) was associated with a higher PDCAAS value compared to plant protein consumption, 63.7 ± 15.9 vs. 46.5 ± 6.0 (p < 0.001), respectively, in both regions.
A higher percentage of children in Limera consumed animal-source food (defined as the intake of solid meat excluding broth) than in Masenjere, 4.9 ± 8.1 g/day vs 2.1 ± 4.2 g/day (
p < 0.001), respectively, and mean quantities of animal-source food were higher in Limera compared to Masenjere (99(56%) vs. 79(44%), respectively,
p = 0.030). Considering breastmilk consumption, children from Limera consumed 2.1 g/day more bioavailable protein from their total intake than children from Masenjere (
p = 0.013) (
Table 4). In children 12–36 months, no difference was observed for total protein consumption; however, children from Limera consumed higher amounts of bioavailable protein (
p = 0.018). More than 80% of the children met their recommended daily protein intake, but the difference between the two regions tended toward significance in the 6–12-months-old group (
p = 0.051) but not the 12–36-months-old group (
p = 0.231) (
Table 4). When ages were pooled, 87.6% and 93.2% of the children from Masenjere and Limera met their recommended levels of protein consumption, respectively; this was higher in Limera than Masenjere (
p = 0.037).
3.5. The Association of Food Type and Food Quality with Stunting, Acute Malnutrition and EED
In bivariate analysis, children aged 6–12 months that consumed fish protein had a 0.3 increase in HAZ per month compared to children that did not consume any fish (
p = 0.019). However, this association did not remain significant after adjusting for confounders in a multivariate analysis (
p = 0.161). Meanwhile, data collection in October remained statistically significantly associated with a 0.3 increase in HAZ per month accounting for fish consumption, water quality, sex, age at recall, number of siblings, asset score, food security, stooling place and presence of animals in the child’s room (
p = 0.048). The female gender and data collection in February were negatively associated with change in HAZ, −0.3 ± 0.1 (
p = 0.046) and −0.4 ± 0.2 (
p = 0.027), respectively, after adjusting for animal protein and other confounders (
Table 5). Being female was associated with 0.1 increase in lactulose % excreted (
p = 0.026). Consumption of animal-source food was not statistically significantly associated with lactulose % excreted (
p = 0.437) or rate of acute malnutrition (
p = 0.095) in both bivariate and multivariate analysis (
Table 5).
In children aged 12–36 months, a 1 g increase in consumption of animal-source protein was associated with a 0.02 increase in HAZ per month in bivariate (
p = 0.021) and multivariate analyses (
p = 0.047) (
Table 5). In bivariate analysis, a 1 g higher intake of bioavailable protein was associated with a 0.02 increase in HAZ (
p = 0.048). This association did not remain significant after adjusting for confounders; however, age remained statistically significantly associated with a 0.05 increase in HAZ per month after accounting for bioavailable protein, water quality, sex, season, number of siblings, asset score, food security, stooling place and presence of animals in the child’s room (
p = 0.001). Age was significantly associated with a 0.1 increase in HAZ (
p < 0.001) and a 0.01 increase in lactulose % excreted, after adjusting for animal protein (
p = 0.003). Animal-source protein consumption was not associated with rates of acute malnutrition (
p = 0.341) or lactulose % excretion (
p = 0.437) (
Table 5).
4. Discussion
In this secondary analysis, we assessed whether the diets of children from Masenjere and Limera differed, and if this difference was associated with different rates of stunting, acute malnutrition and EED observed in 6–36-months-old children within these communities. We have shown that children from Limera consumed a higher amount of protein from animal sources, and this was associated with improved linear growth in children aged 12–36 months.
We have demonstrated that a region with lower rates of stunting, acute malnutrition and EED had a higher consumption of animal-source proteins than a region with lower consumption, despite equivalent or better nutrient intakes and sanitation practices. In our analysis, children from the Masenjere region consumed 2.1 g less mean bioavailable protein from animal sources, and consumption of animal-source protein was associated with improved linear growth in 12–36-months-old children. This agrees with findings from other studies. Krebs et al. [
20] demonstrated a lower risk of stunting and wasting in children aged 5–24 months from the Democratic Republic of Congo, Zambia, Guatemala and Pakistan who consumed meat compared with those who did not. In Cambodia, consumption of animal-source foods was associated with lower rates of stunting (adjusted odds ratio of 0.69,
p < 0.01) in children aged 12–59 months [
21]. A study in Peru that assessed the breastfeeding and nutrient intakes of 12–15-months-old children demonstrated a 0.4 cm greater gain in child length over a 3-month period in weaned children that consumed food from animal products [
51]. We speculate that a higher consumption of animal-source food in Limera was protective against worsening anthropometric outcomes in 12–36-months-old children but not 6–12-months-olds because older infants have lower ad lib breastmilk consumption and therefore consume more complementary food than children 6–12 months who consume more breastmilk than complementary food.
Fish was the main source of animal food in this population, followed by some consumption of eggs. Chicken, soup from beef and milk were consumed by very few children. While we have reported that 21–54% of the children consumed fish, the quantities of the fish consumed were small, providing mean energy intakes between 42–57 kcal/day and protein intakes of 3.9–5.5 g/day. Both Masenjere and Limera villages are located close to water bodies (Shire river and Lake Chilwa, respectively), hence there is an abundance of both small and big fish in the areas and it is cheaper than red meat or chicken. Because they are consumed with bones, organs and other viscera, small fish have a higher micronutrient content (especially of iron, zinc, calcium and vitamin A) compared to larger fish from which only the flesh is consumed [
52]. Small fish are cheaper and more available on the market than large fish in Malawi, and it is therefore important to educate and encourage mothers to add more fish into the weaning diets of children. The use of dried fish and fish powder in complementary feeding programs is well established. A study in Ghana that assessed growth and micronutrient intake in children supplemented with a modified cereal–legume complimentary food called Weanimix found no differences in child growth for groups that received either Weanimix, fortified Weanimix, Weanimix plus fish powder or koko (a fermented corn meal or millet flour) plus fish powder. What is interesting about this finding is that the addition of fish seemed to have a protective effect on growth of children just as fortified Weanimix did, for consumption of koko alone has been linked to poor growth outcomes [
53].
As expected, the diet of the children from both regions was predominantly plant based with maize staples as the most consumed food. This was also reflected in the low PDCAAS values with lysine as the limiting amino acid. While more than 80% of the children met their recommended daily protein intake, the quality of this protein was poor with low bioavailability, for it was mainly plant based. We have demonstrated a higher plant food consumption in Masenjere than Limera, and it is therefore not surprising that the region has poor growth outcomes since the overall quality of the diet is poor in quality bioavailable protein. The importance of consuming quality protein in infancy cannot be understated, as it impacts cognitive development. A Kenyan study that assessed the cognitive performance of school children found that children who received better nourishment (adequate diets with high energy, fat, carbohydrate and animal protein intake) had higher cognitive scores, played more and were more verbal compared to children with inadequate diets. Consumption of animal protein was more strongly associated with better cognitive outcomes than the intake of other nutrients. The study also established that intakes of animal protein between 18 and 30 months of age predicted higher cognitive scores at 5 years old [
54]. Similarly, a Ghanaian study of healthy 6–9-years-old school children demonstrated higher cognitive scores in children that received 8.8 g milk protein per day compared with children that received 4.4 g milk protein per day or 4.4 g milk plus 4.4 g rice protein per day [
55].
We have demonstrated that the quality of the nutrients consumed is more reflective of the observed nutrition status of children than meeting the minimum recommended dietary diversity. Children from Masenjere had a higher dietary diversity score, and more of them met the minimum required dietary diversity, which are indicators dietary adequacy; this did not, however, reflect in the anthropometric status of the children. In this study, a higher dietary diversity was not associated with improved growth outcomes and nutritional status. The positive association of higher dietary diversity with improved anthropometric outcomes has been reported by many and is an accepted indicator of dietary adequacy [
44,
56,
57,
58,
59]. However, our findings suggest that assessing the source of the nutrients may be equally important in assessing the anthropometric outcomes of children.
Some non-governmental organizations working within the regions of Masenjere and Limera recommend the addition of fish bones to maize for porridge flour preparation, but the uptake of this program is poor. Further studies investigating the feasibility and acceptability of adding dried fish to the complementary food of children in these regions are needed.
A limitation of this study, as with all interactive 24-h dietary recalls, is that the number of recalls needed per individual to reduce uncertainty is about 10. Since this was not done in this work, our data can only be used to describe the collective populations of Masenjere and Limera. Modification of a child’s diet by the guardians is a potential source of bias in interactive 24-h recalls. In most cases, the guardians modified the diet of the child on the recall day to impress the researchers by adding foods that are not normally consumed. This could have led to over-reporting intake, which could have produced results that do not represent the usual intake amount. In this analysis, only 9 out of 70 (13%) children that developed acute malnutrition in the main RCTs 1 and 2 [
15] participated in dietary recalls, so the association of food type and quality consumption with acute malnutrition may have been affected. More reflective results on this association would have been attained if we assessed the diet of all the children that developed acute malnutrition.

 ,
, 
{kind=link}
