Spatial Association of Food Sales in Supermarkets with the Mean BMI of Young Men: An Ecological Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
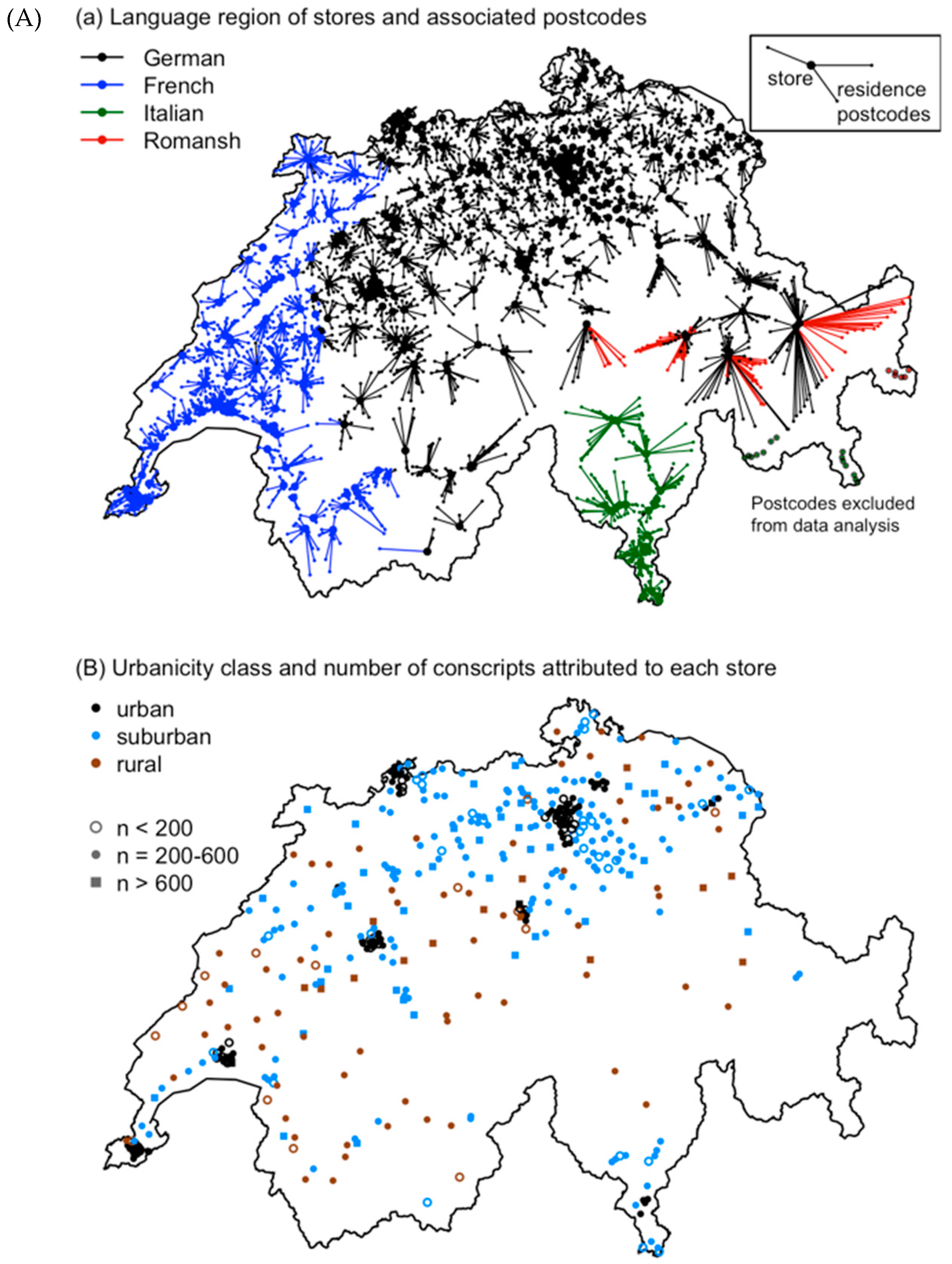
2.1. Food Sales Data
2.2. BMI of Swiss Conscripts
2.3. Combination of Food Sales and BMI Data
2.4. Area-Based Socioeconomic Position (Mean Neighbourhood Swiss-SEP) and Urbanicity
2.5. Data Analysis
2.6. Ethics
2.7. Availability of Data und Material
3. Results
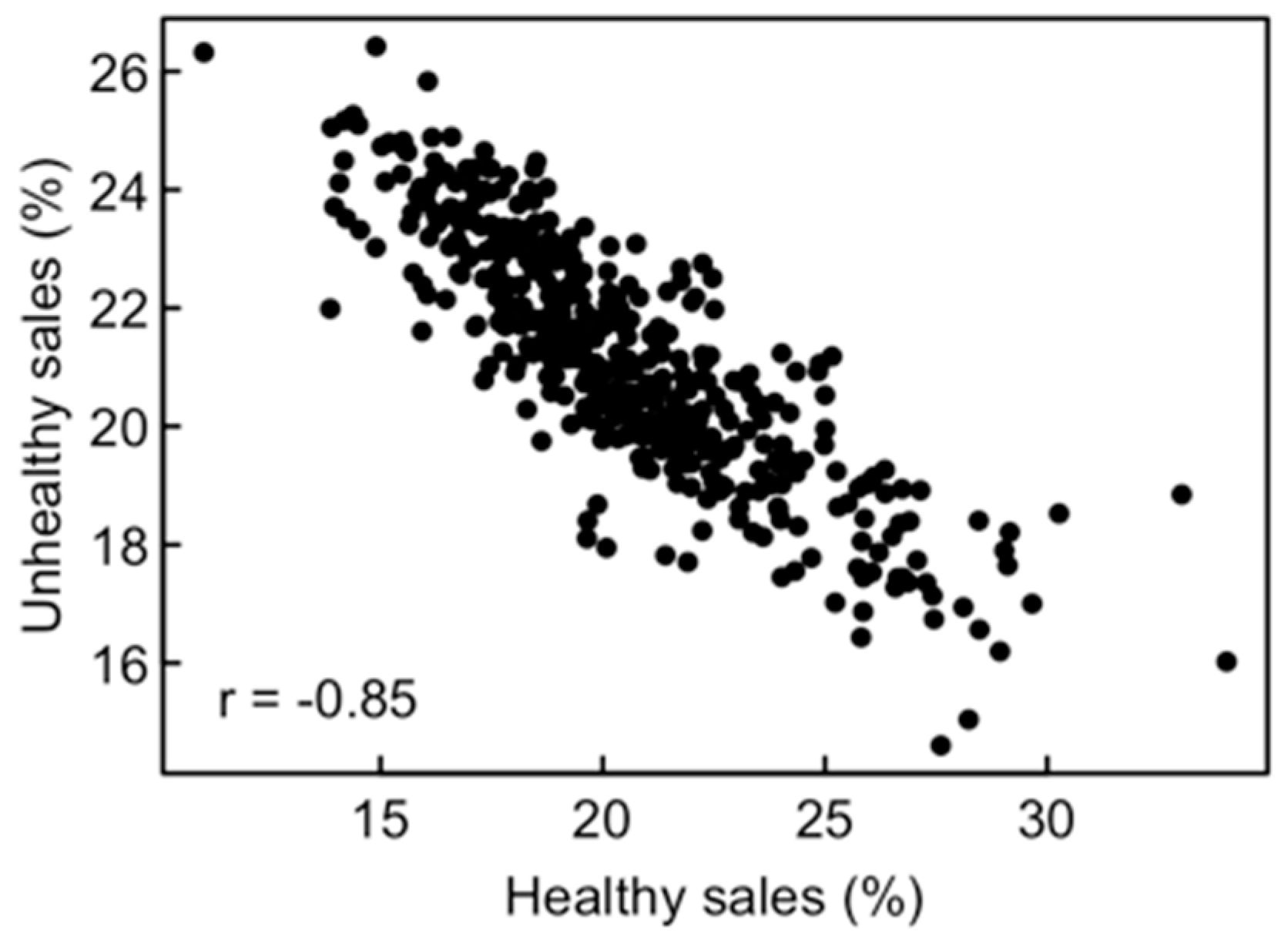
3.1. Patterns in Food Sales
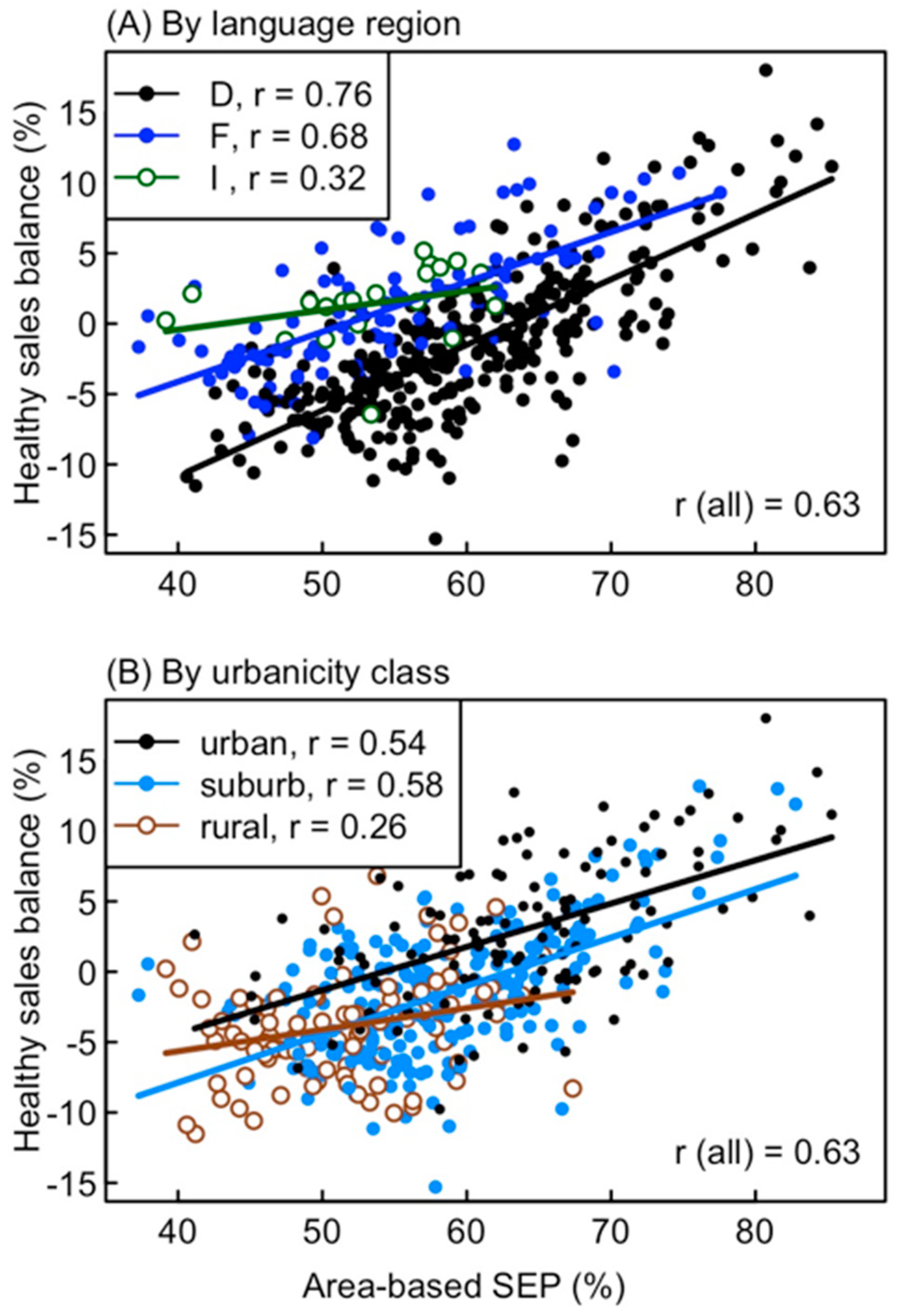
3.2. Factors Influencing Patterns in Food Sales
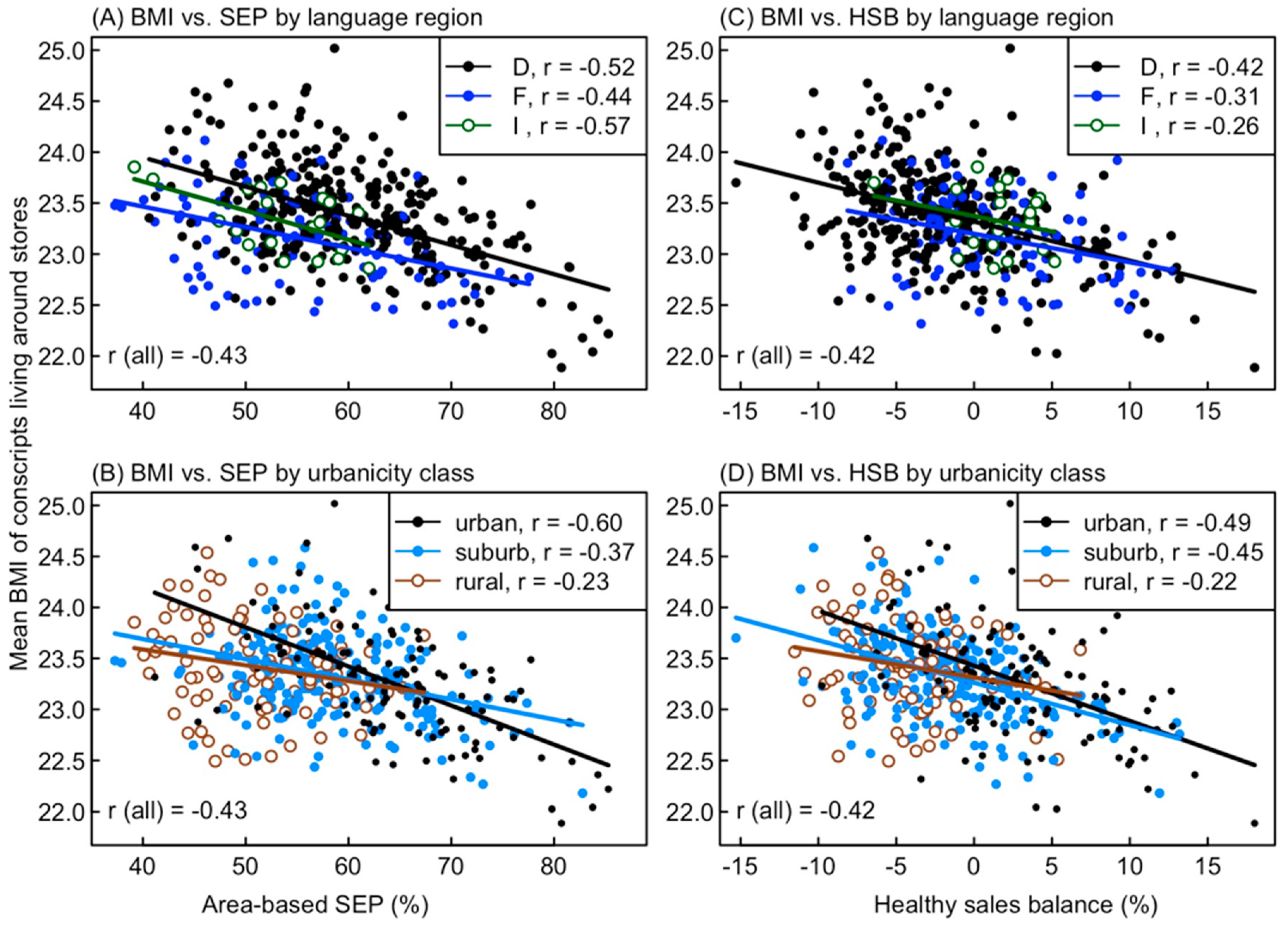
3.3. Factors Influencing the Mean BMI of Conscripts
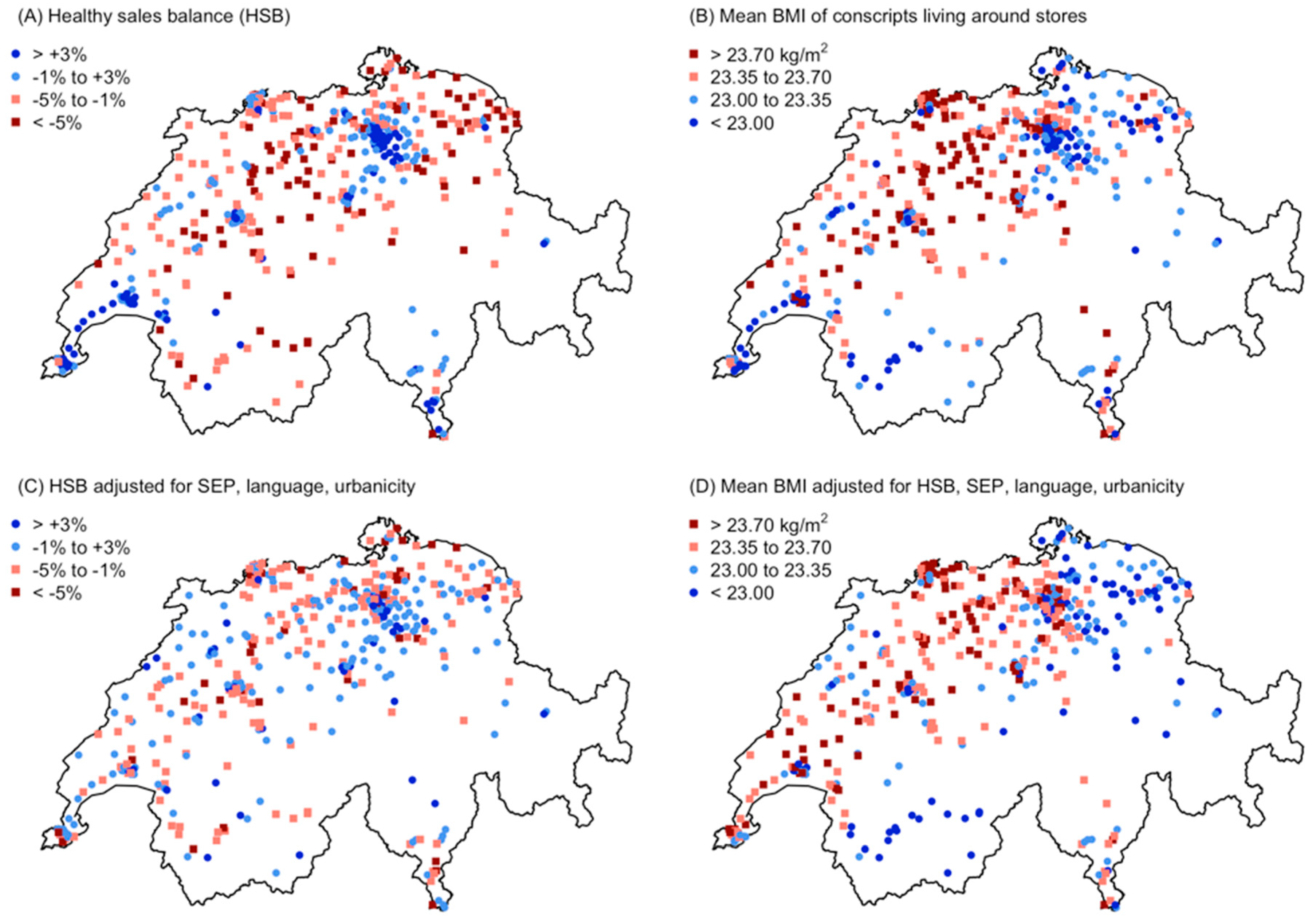
3.4. Spatial Patterns
4. Discussion
4.1. Strong Variation in Sales of Healthy and Unhealthy Food Types
4.2. Environmental Determinants of Food Sales Patterns
4.3. Association of Mean BMI with Food Sales Patterns
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Nesbit, K.C.; Kolobe, T.H.; Sisson, S.B.; Ghement, I.R. A model of environmental correlates of adolescent obesity in the United States. J. Adolesc. Health 2014, 55, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Moudon, A.V.; Jiao, J.; Aggarwal, A.; Charreire, H.; Chaix, B. Food environment and socioeconomic status influence obesity rates in Seattle and in Paris. Int. J. Obes. 2014, 38, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Jilcott Pitts, S.B.; Keyserling, T.C.; Johnston, L.F.; Smith, T.W.; McGuirt, J.T.; Evenson, K.R.; Rafferty, A.P.; Gizlice, Z.; Garcia, B.A.; Ammerman, A.S. Associations between neighborhood-level factors related to a healthful lifestyle and dietary intake, physical activity, and support for obesity prevention polices among rural adults. J. Community Health 2015, 40, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Viola, D.; Arno, P.S.; Maroko, A.R.; Schechter, C.B.; Sohler, N.; Rundle, A.; Neckerman, K.M.; Maantay, J. Overweight and obesity: Can we reconcile evidence about supermarkets and fast food retailers for public health policy? J. Public Health Policy 2013, 34, 424–438. [Google Scholar] [CrossRef] [PubMed]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.M.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major differences in diet across three linguistic regions of Switzerland: Results from the first national nutrition survey menuCH. Nutrients 2017, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A.M. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 2015, 23, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.V.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef]
- Gustafson, A.; Hankins, S.; Jilcott, S. Measures of the consumer food store environment: A systematic review of the evidence 2000–2011. J. Community Health 2012, 37, 897–911. [Google Scholar] [CrossRef]
- Giskes, K.; van Lenthe, F.; Avendano-Pabon, M.; Brug, J. A systematic review of environmental factors and obesogenic dietary intakes among adults: Are we getting closer to understanding obesogenic environments? Obes. Rev. 2011, 12, e95–e106. [Google Scholar] [CrossRef]
- Burgoine, T.; Mackenbach, J.D.; Lakerveld, J.; Forouhi, N.G.; Griffin, S.J.; Brage, S.; Wareham, N.J.; Monsivais, P. Interplay of socioeconomic status and supermarket distance is associated with excess obesity risk: A UK cross-sectional study. Int. J. Environ. Res. Public Health 2017, 14, 1290. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, M.; Griffiths, C.; Green, M.A.; Jordan, H.; Saunders, J.; McKenna, J. Neighbourhood typologies and associations with body mass index and obesity: A cross-sectional study. Prev. Med. 2018, 111, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A. Neighbourhood food environments: food choice, foodscapes and planning for health. Proc. Nutr. Soc. 2018, 77, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Timperio, A.; Crawford, D.; Leech, R.M.; Lamb, K.E.; Ball, K. Patterning of neighbourhood food outlets and longitudinal associations with children’s eating behaviours. Prev. Med. 2018, 111, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Vogel, C.; Lewis, D.; Ntani, G.; Cummins, S.; Cooper, C.; Moon, G.; Baird, J. The relationship between dietary quality and the local food environment differs according to level of educational attainment: A cross-sectional study. PLoS ONE 2017, 12, e0183700. [Google Scholar] [CrossRef]
- Black, C.; Ntani, G.; Inskip, H.; Cooper, C.; Cummins, S.; Moon, G.; Baird, J. Measuring the healthfulness of food retail stores: Variations by store type and neighbourhood deprivation. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Thiele, S.; Peltner, J.; Richter, A.; Mensink, G.B.M. Food purchase patterns: Empirical identification and analysis of their association with diet quality, socio-economic factors, and attitudes. Nutr. J. 2017, 16, 69. [Google Scholar] [CrossRef]
- Howard Wilsher, S.; Harrison, F.; Yamoah, F.; Fearne, A.; Jones, A. The relationship between unhealthy food sales, socio-economic deprivation and childhood weight status: Results of a cross-sectional study in England. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 21. [Google Scholar] [CrossRef]
- Närhinen, M.; Berg, M.-A.; Nissinen, A.; Puska, P. Supermarket sales data: A tool for measuring regional differences in dietary habits. Public Health Nutr. 1999, 2, 277–282. [Google Scholar] [CrossRef]
- Ransley, J.K.; Donnelly, J.K.; Khara, T.N.; Botham, H.; Arnot, H.; Greenwood, D.C.; Cade, J.E. The use of supermarket till receipts to determine the fat and energy intake in a UK population. Public Health Nutr. 2001, 4, 1279–1286. [Google Scholar] [CrossRef]
- OECD. OECD: Income Inequality Remains High in the Face of Weak Recovery; OECD Publishing: Paris, France, 2016. [Google Scholar]
- Panczak, R.; Held, L.; Moser, A.; Jones, P.A.; Rühli, F.J.; Staub, K. Finding big shots: Small-area mapping and spatial modelling of obesity among Swiss male conscripts. BMC Obes. 2016, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Panczak, R.; Zwahlen, M.; Woitek, U.; Rühli, F.J.; Staub, K. Socioeconomic, temporal and regional variation in body mass index among 188,537 Swiss male conscripts born between 1986 and 1992. PLoS ONE 2014, 9, e96721. [Google Scholar] [CrossRef]
- Joost, S.; Duruz, S.; Marques-Vidal, P.; Bochud, M.; Stringhini, S.; Paccaud, F.; Gaspoz, J.-M.; Theler, J.-M.; Chetelat, J.; Waeber, G.; et al. Persistent spatial clusters of high body mass index in a Swiss urban population as revealed by the 5-year GeoCoLaus longitudinal study. BMJ Open 2016, 6, e010145. [Google Scholar] [CrossRef] [PubMed]
- Guessous, I.; Joost, S.; Jeannot, E.; Theler, J.-M.; Mahler, P.; Gaspoz, J.-M. A comparison of the spatial dependence of body mass index among adults and children in a Swiss general population. Nutr. Diabetes 2014, 4, e111. [Google Scholar] [CrossRef]
- Vormund, K.; Braun, J.; Rohrmann, S.; Bopp, M.; Ballmer, P.; Faeh, D. Mediterranean diet and mortality in Switzerland: An alpine paradox? Eur. J. Nutr. 2015, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Brombach, C.; Jacob, S.; Schmid, I.; Sieber, R.; Siegrist, M. Ernährungssituation in der Schweiz. In Sechster Schweizerischer Ernährungsbericht; Keller, U., Battaglia, R., Beer, M., Darioli, R., Meyer, K., Renggli, A., Römer-Lüthi, C., Stoffel-Kurt, N., Eds.; Bundesamt für Gesundheit: Bern, Switzerland, 2012. [Google Scholar]
- Richard, A.; Faeh, D.; Bopp, M.; Rohrmann, S. Diet and other lifestyle factors associated with prostate cancer differ between the German and Italian region of Switzerland. Int. J. Vitam. Nutr. Res. 2016, 86, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Joost, S.; De Ridder, D.; Marques-Vidal, P.; Bacchilega, B.; Theler, J.-M.; Gaspoz, J.-M.; Guessous, I. Detecting overlapping spatial clusters of high sugar-sweetened beverage intake and high body mass index in a general population: A cross-sectional study. bioRxiv 2018, 399584. [Google Scholar] [CrossRef]
- GfK Switzerland AG. Detailhandel Schweiz 2012; GfK Switzerland: Hergiswil, Switzerland, 2012. [Google Scholar]
- Panczak, R.; Woitek, U.; Rühli, F.; Staub, K. Regionale und sozio-ökonomische Unterschiede im Body Mass Index (BMI) von Schweizer Stellungspflichtigen 2004–2012; Projektschlussbericht zuhanden des Bundesamtes für Gesundheit (BAG): Zürich, Switzerland, 2013. [Google Scholar]
- Panczak, R.; Moser, A.; Held, L.; Jones, P.A.; Rühli, F.J.; Staub, K. A tall order: Small area mapping and modelling of adult height among Swiss male conscripts. Econ. Hum. Biol. 2017, 26, 61–69. [Google Scholar] [CrossRef]
- Staub, K.; Bender, N.; Floris, J.; Pfister, C.; Rühli, F.J. From undernutrition to overnutrition: The evolution of overweight and obesity among young men in Switzerland since the 19th century. Obes. Facts 2016, 9, 259–272. [Google Scholar] [CrossRef]
- Panczak, R.; Galobardes, B.; Voorpostel, M.; Spoerri, A.; Zwahlen, M.; Egger, M. A Swiss neighbourhood index of socioeconomic position: Development and association with mortality. J. Epidemiol. Community Health 2012, 66, 1129–1136. [Google Scholar] [CrossRef]
- Eurostat Degree of Urbanisation (DEGURBA). Local Administrative Units; Eurostat Degree of Urbanisation: Bydgoszcz, Poland, 2011. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Chrisinger, B.W.; DiSantis, K.I.; Hillier, A.E.; Kumanyika, S.K. Family food purchases of high- and low-calorie foods in full-service supermarkets and other food retailers by Black women in an urban US setting. Prev. Med. Rep. 2018, 10, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Chrisinger, B.W.; Kallan, M.J.; Whiteman, E.D.; Hillier, A. Where do U.S. households purchase healthy foods? An analysis of food-at-home purchases across different types of retailers in a nationally representative dataset. Prev. Med. 2018, 112, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Mackenzie, T.; Mhurchu, C.N. Indicators of the relative availability of healthy versus unhealthy foods in supermarkets: A validation study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Hümberlin, O. Ungleichheit, Umverteilung und der Wohlfahrtsstaat in der Schweiz; Universitätsbibliothek Bern: Bern, Switzerland, 2016. [Google Scholar]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Positive attitude toward healthy eating predicts higher diet quality at all cost levels of supermarkets. J. Acad. Nutr. Diet. 2014, 114, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Jensen, J.D. What is the effectiveness of obesity related interventions at retail grocery stores and supermarkets?—A systematic review. BMC Public Health 2016, 16, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Pliner, P.; Mann, N. Influence of social norms and palatability on amount consumed and food choice. Appetite 2004, 42, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Higgs, S. Food choices in the presence of ‘healthy’ and ‘unhealthy’ eating partners. Br. J. Nutr. 2013, 109, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Fleming, A.; Higgs, S. Prompting healthier eating: Testing the use of health and social norm based messages. Heal. Psychol. 2014, 33, 1057–1064. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Burgoine, T.; Sarkar, C.; Webster, C.J.; Monsivais, P. Examining the interaction of fast-food outlet exposure and income on diet and obesity: Evidence from 51,361 UK Biobank participants. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 71. [Google Scholar] [CrossRef]
- Robinson, S.M.; Crozier, S.R.; Borland, S.E.; Hammond, J.; Barker, D.J.P.; Inskip, H.M. Impact of educational attainment on the quality of young women’s diets. Eur. J. Clin. Nutr. 2004, 58, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Huybrechts, I.; Lioret, S.; Mouratidou, T.; Gunter, M.J.; Manios, Y.; Kersting, M.; Gottrand, F.; Kafatos, A.; De Henauw, S.; Cuenca-García, M.; et al. Using reduced rank regression methods to identify dietary patterns associated with obesity: A cross-country study among European and Australian adolescents. Br. J. Nutr. 2017, 117, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Pinho, M.G.M.; Mackenbach, J.D.; Charreire, H.; Oppert, J.-M.; Bárdos, H.; Glonti, K.; Rutter, H.; Compernolle, S.; De Bourdeaudhuij, I.; Beulens, J.W.J.; et al. Exploring the relationship between perceived barriers to healthy eating and dietary behaviours in European adults. Eur. J. Nutr. 2018, 57, 1761–1770. [Google Scholar] [CrossRef] [PubMed]
- Feunekes, G.I.J.; de Graaf, C.; Meyboom, S.; van Staveren, W.A. Food choice and fat intake of adolescents and adults: Associations of intakes within social networks. Prev. Med. 1998, 27, 645–656. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Brombach, C.; Jacob, S.; Schmid, I.; Sieber, R.; Siegrist, M. Ernährungssituation in der Schweiz. In Sechster Schweizerischer Ernährungsbericht; Federal Office of Public Health (BAG), Ed.; Merkur Druck AG: Bern, Switzerland, 2012; pp. 50–126. [Google Scholar]
- Finger, J.D.; Varnaccia, G.; Tylleskär, T.; Lampert, T.; Mensink, G.B.M. Dietary behaviour and parental socioeconomic position among adolescents: The German Health Interview and Examination Survey for Children and Adolescents 2003–2006 (KiGGS). BMC Public Health 2015, 15, 498. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, M.K.; Arvola, A.; Hursti, U.-K.K.; Åberg, L.; Sjödén, P.-O. Choice of organic foods is related to perceived consequences for human health and to environmentally friendly behaviour. Appetite 2003, 40, 109–117. [Google Scholar] [CrossRef]
- Kit, B.K.; Ogden, C.L.; Flegal, K.M. Epidemiology of Obesity. In Handbook of Epidemiology; Ahrens, W., Pigeot, I., Eds.; Springer Science+Business Media: New York, NY, USA, 2014; pp. 2229–2262. ISBN 9780387098340. [Google Scholar]
- Staub, K.; Floris, J.; Koepke, N.; Trapp, A.; Nacht, A.; Schärli Maurer, S.; Rühli, F.J.; Bender, N. Associations between anthropometric indices, blood pressure and physical fitness performance in young Swiss men: A cross-sectional study. BMJ Open 2018, 8, e018664. [Google Scholar] [CrossRef] [PubMed]
- Cannuscio, C.C.; Hillier, A.; Karpyn, A.; Glanz, K. The social dynamics of healthy food shopping and store choice in an urban environment. Soc. Sci. Med. 2014, 122, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Plachta-Danielzik, S.; Kehden, B.; Landsberg, B.; Schaffrath Rosario, A.; Kurth, B.-M.; Arnold, C.; Graf, C.; Hense, S.; Ahrens, W.; Müller, M.J. Attributable risks for childhood overweight: Evidence for limited effectiveness of prevention. Pediatrics 2012, 130, e865–e871. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Emmett, P.M.; Northstone, K.; Howe, L.D.; Tilling, K.; Jebb, S.A. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int. J. Obes. 2012, 36, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Peeters, A.; Gearon, E.; Backholer, K. Contribution of discretionary food and drink consumption to socio-economic inequalities in children’s weight: Prospective study of Australian children. Int. J. Epidemiol. 2018, 47, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Dovey, T.M.; Torab, T.; Yen, D.; Boyland, E.J.; Halford, J.C.G. Responsiveness to healthy advertisements in adults: An experiment assessing beyond brand snack selection and the impact of restrained eating. Appetite 2017, 112, 102–106. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Category | n | Means ± SD among Stores | |
|---|---|---|---|---|
| Area-Based SEP | Mean BMI (kg/m2) | |||
| Overall | all | 445 | 58.45 ± 8.90 | 23.33 ± 0.46 |
| Language region (2013) | German (D) | 324 | 59.93 ± 8.60 | 23.38 ± 0.48 |
| French (F) | 101 | 54.71 ± 8.89 | 23.17 ± 0.41 | |
| Italian (I) | 20 | 53.40 ± 6.12 | 23.33 ± 0.31 | |
| Urbanicity class (DEGURBA, Eurostat 2011) | urban | 120 | 64.12 ± 8.86 | 23.26 ± 0.56 |
| suburban | 232 | 58.43 ± 7.59 | 23.33 ± 0.41 | |
| rural | 93 | 51.20 ± 6.39 | 23.41 ± 0.44 | |
| Food Type | Category and Rationale H = Healthy, U = Unhealthy, B = Both H&U or Basic Food | Mean ± SD (% of Total) | Range (% of Total) |
|---|---|---|---|
| Fruit | H: vitamins and minerals | 6.77 ± 0.95 | 3.8–10.0 |
| Vegetables, fresh and preserved | H: low energy, fiber, vitamins and minerals | 7.72 ± 0.98 | 3.9–10.8 |
| Legumes | H: proteins, fiber, minerals | 0.12 ± 0.05 | 0.0–0.3 |
| Fish | H: protein, relatively low fat | 1.87 ± 0.79 | 0.8–5.1 |
| Food supplements 1 | H: “healthy lifestyle” product | 0.24 ± 0.07 | 0.0–0.5 |
| Organically produced food 2 | H: “healthy lifestyle” product | 3.65 ± 1.53 | 1.2–11.5 |
| Crisps | U: high fat and salt content | 0.63 ± 0.13 | 0.4–1.2 |
| Sausages and cold meat | U: high fat and salt content | 10.12 ± 1.31 | 6.2–13.6 |
| Sweet drinks | U: high sugar content | 1.81 ± 0.52 | 0.8–4.3 |
| Ice-cream | U: high sugar and fat content | 1.38 ± 0.25 | 0.6–2.2 |
| Chocolate and cookies 3 | U: high sugar and fat content | 3.61 ± 0.71 | 2.2–8.7 |
| Cakes | U: high sugar and fat content | 3.66 ± 0.64 | 1.5–6.1 |
| Fruit juice | B: both: vitamins/high sugar | 1.02 ± 0.16 | 0.6–1.6 |
| Breakfast cereals | B: both: “healthy lifestyle” but partly high sugar 4 | 1.17 ± 0.19 | 0.7–2.4 |
| Bread | B: basic food | 5.27 ± 0.95 | 3.2–8.8 |
| Pasta | B: basic food | 1.22 ± 0.18 | 0.8–2.8 |
| Meat (beef, pork, lamb) | B: basic food for non-vegetarians, partly high fat | 5.78 ± 1.08 | 2.6–9.0 |
| Poultry | B: basic food for non-vegetarians | 3.44 ± 0.63 | 1.9–5.2 |
| Eggs | B: basic food | 1.43 ± 0.19 | 0.8–2.1 |
| Milk and dairy products | B: basic food, partly high sugar/fat 4 | 16.16 ± 1.23 | 11.9–19.4 |
| Total | All classes above without organic food | 73.41 ± 2.15 | 63.8–78.0 |
| Variation Represented | Axis 1 | Axis 2 | Axis 3 |
|---|---|---|---|
| 25.4% | 16.7% | 12.3% | |
| Fruit | −0.35 | −0.16 | −0.04 |
| Vegetables | −0.34 | −0.14 | −0.24 |
| Legumes | −0.25 | 0.34 | 0.19 |
| Fish | −0.31 | 0.32 | 0.10 |
| Food supplements | −0.14 | −0.10 | −0.17 |
| Organic food | −0.26 | −0.33 | −0.06 |
| Crisps | 0.31 | 0.06 | −0.08 |
| Sausages and cold meat | 0.33 | 0.18 | −0.28 |
| Sweet drinks | 0.24 | −0.28 | 0.12 |
| Ice-cream | 0.23 | −0.08 | −0.20 |
| Chocolate and cookies | 0.08 | 0.12 | 0.43 |
| Cakes | 0.18 | −0.07 | 0.36 |
| Fruit juices | −0.18 | 0.01 | 0.12 |
| Breakfast cereals | −0.10 | −0.09 | −0.14 |
| Bread | 0.07 | −0.31 | 0.34 |
| Pasta | 0.17 | 0.08 | 0.18 |
| Meat | 0.08 | 0.36 | −0.24 |
| Poultry | −0.15 | 0.37 | −0.09 |
| Eggs | −0.11 | −0.32 | −0.11 |
| Milk and dairy products | 0.21 | −0.09 | −0.38 |
| Predictor Regression | Simple Regression | Multiple | ||
|---|---|---|---|---|
| Area-based SEP quartiles | ||||
| low | 0.0 | - | 0.0 | - |
| low-mid | 0.9 | (−0.2 to 2.0) | 1.3 | (0.3 to 2.3) |
| mid-high | 3.0 | (1.9 to 4.2) | 3.1 | (2.1 to 4.2) |
| high | 7.6 | (6.5 to 8.7) | 7.5 | (6.4 to 8.6) |
| Language | ||||
| German | 0.0 | - | 0.0 | - |
| French | 2.6 | (1.5 to 3.8) | 4.0 | (3.2 to 4.9) |
| Italian | 3.0 | (0.7 to 5.2) | 5.2 | (3.5 to 6.8) |
| Urbanicity | ||||
| rural | 0.0 | - | 0.0 | - |
| suburban | 2.4 | (1.3 to 3.5) | 1.1 | (0.2 to 2.1) |
| urban | 7.0 | (5.7 to 8.2) | 3.6 | (2.4 to 4.7) |
| Predictor Regression | Simple Regression | Multiple | ||
|---|---|---|---|---|
| low | 0.0 | - | 0.0 | - |
| low-mid | −0.14 | (−0.25 to −0.03) | −0.07 | (−0.18 to 0.05) |
| mid-high | −0.38 | (−0.40 to −0.17) | −0.13 | (−0.25 to 0.00) |
| high | −0.47 | (−0.58 to −0.35) | −0.19 | (−0.34 to −0.04) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Güsewell, S.; Floris, J.; Berlin, C.; Zwahlen, M.; Rühli, F.; Bender, N.; Staub, K. Spatial Association of Food Sales in Supermarkets with the Mean BMI of Young Men: An Ecological Study. Nutrients 2019, 11, 579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030579
Güsewell S, Floris J, Berlin C, Zwahlen M, Rühli F, Bender N, Staub K. Spatial Association of Food Sales in Supermarkets with the Mean BMI of Young Men: An Ecological Study. Nutrients. 2019; 11(3):579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030579
Chicago/Turabian StyleGüsewell, Sabine, Joël Floris, Claudia Berlin, Marcel Zwahlen, Frank Rühli, Nicole Bender, and Kaspar Staub. 2019. "Spatial Association of Food Sales in Supermarkets with the Mean BMI of Young Men: An Ecological Study" Nutrients 11, no. 3: 579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030579