Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions of Pre-Pregnancy Body Mass Index and Gestational Weight Gain
2.3. Dietary Assessment
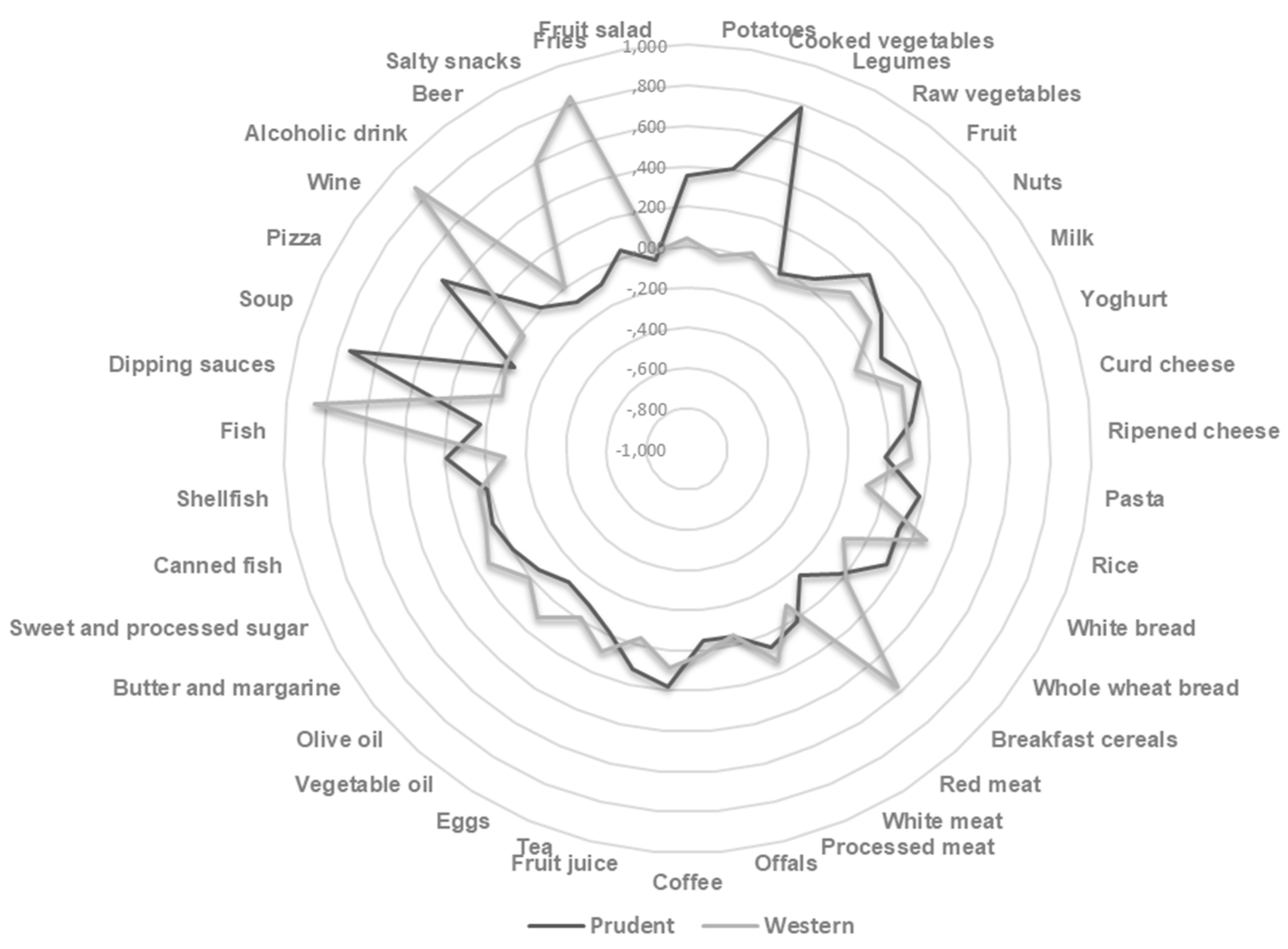
2.4. Principal Component Analysis
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
3.2. Dietary Patterns and Pre-Pregnancy Body Mass Index
3.3. Dietary Patterns and Gestational Weight Gain
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/dietphysicalactivity/media/en/gsfs_obesity.pdf (accessed on 1 April 2019).
- Yu, Z.; Han, S.; Zhu, J.; Sun, X.; Ji, C.; Guo, X. Pre-pregnancy body mass index in relation to infant birth weight and offspring overweight/obesity: A systematic review and meta-analysis. PLoS ONE 2013, 8, e61627. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Blanco, I.; Agodi, A. Effects of Vitamin D Supplementation during Pregnancy on Birth Size: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2019, 11, 442. [Google Scholar] [CrossRef] [PubMed]
- Labayen, I.; Ruiz, J.R.; Vicente-Rodríguez, G.; Turck, D.; Rodríguez, G.; Meirhaeghe, A.; Molnár, D.; Sjöström, M.; Castillo, M.J.; Gottrand, F.; et al. Early life programming of abdominal adiposity in adolescents: The HELENA Study. Diabetes Care 2009, 32, 2120–2122. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, L.; Flick, A.A.; Istwan, N.; Rhea, D.; Cordova, Y.; Dieguez, C.; Desch, C.; González-Quintero, V.H. The effect of new antepartum weight gain guidelines and prepregnancy body mass index on the development of pregnancy-related hypertension. Am. J. Perinatol. 2011, 28, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Mamun, A.A.; Kinarivala, M.; O’Callaghan, M.J.; Williams, G.M.; Najman, J.M.; Callaway, L.K. Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up. Am. J. Clin. Nutr. 2010, 91, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Crane, J.M.; White, J.; Murphy, P.; Burrage, L.; Hutchens, D. The effect of gestational weight gain by body mass index on maternal and neonatal outcomes. J. Obstet. Gynaecol. Can. 2009, 31, 28–35. [Google Scholar] [CrossRef]
- Mannan, M.; Doi, S.A.; Mamun, A.A. Association between weight gain during pregnancy and postpartum weight retention and obesity: A bias-adjusted meta-analysis. Nutr. Rev. 2013, 71, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.L.; Schauberger, C.W.; Mathiason, M.A. Impact of perinatal weight change on long-term obesity and obesity-related illnesses. Obstet. Gynecol. 2005, 106, 1349–1356. [Google Scholar] [CrossRef]
- Shapiro, S.; McCormick, M.C.; Starfield, B.H.; Krischer, J.P.; Bross, D. Relevance of correlates of infant deaths for significant morbidity at 1 year of age. Am. J. Obstet. Gynecol. 1980, 136, 363–373. [Google Scholar] [CrossRef]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009.
- Cedergren, M. Effects of gestational weight gain and body mass index on obstetric outcome in Sweden. Int. J. Gynaecol. Obstet. 2006, 93, 269–274. [Google Scholar] [CrossRef]
- Gillman, M.W. Gestational weight gain: Now and the future. Circulation 2012, 125, 1339–1340. [Google Scholar] [CrossRef] [PubMed]
- Lucia Bergmann, R.; Bergmann, K.E.; Haschke-Becher, E.; Richter, R.; Dudenhausen, J.W.; Barclay, D.; Haschke, F. Does maternal docosahexaenoic acid supplementation during pregnancy and lactation lower BMI in late infancy? J. Perinat. Med. 2007, 35, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.C.; McNeil, D.A.; Best, M.; MacLeod, C. A growth status measurement pilot in four Calgary area schools: Perceptions of grade 5 students and their parents. J. Sch. Nurs. 2011, 27, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Nohr, E.A.; Vaeth, M.; Baker, J.L.; Sørensen, T.I.; Olsen, J.; Rasmussen, K.M. Pregnancy outcomes related to gestational weight gain in women defined by their body mass index, parity, height, and smoking status. Am. J. Clin. Nutr. 2009, 90, 1288–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorsdottir, I.; Gunnarsdottir, I.; Kvaran, M.A.; Gretarsson, S.J. Maternal body mass index, duration of exclusive breastfeeding and children’s developmental status at the age of 6 years. Eur. J. Clin. Nutr. 2005, 59, 426–431. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Uusitalo, U.; Arkkola, T.; Ovaskainen, M.L.; Kronberg-Kippilä, C.; Kenward, M.G.; Veijola, R.; Simell, O.; Knip, M.; Virtanen, S.M. Unhealthy dietary patterns are associated with weight gain during pregnancy among Finnish women. Public Health Nutr. 2009, 12, 2392–2399. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.; Lee, K.W.; Song, W.O. Pre-Pregnancy Weight Status Is Associated with Diet Quality and Nutritional Biomarkers during Pregnancy. Nutrients 2016, 8, 162. [Google Scholar] [CrossRef]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef]
- Hillesund, E.R.; Bere, E.; Haugen, M.; Øverby, N.C. Development of a New Nordic Diet score and its association with gestational weight gain and fetal growth—A study performed in the Norwegian Mother and Child Cohort Study (MoBa). Public Health Nutr. 2014, 17, 1909–1918. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Agrifoglio, O.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Panella, M.; Cianci, A.; Agodi, A. The impact of social determinants and lifestyles on dietary patterns during pregnancy: Evidence from the “Mamma & Bambino” study. Annali di Igiene Medicina Preventiva e di Comunita 2019, 31, 81–89. [Google Scholar] [PubMed]
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; Magnano San Lio, R.; Favara, G.; Panella, M.; Cianci, A.; Agodi, A. Single Nucleotide Polymorphisms in Vitamin D Receptor Gene Affect Birth Weight and the Risk of Preterm Birth: Results from the “Mamma & Bambino” Cohort and A Meta-Analysis. Nutrients 2018, 10, 1172. [Google Scholar] [CrossRef]
- Eveleth, P.B.; Andres, R.; Chumlea, W.C.; Eiben, O.; Ge, K.; Harris, T.; Heymsfield, S.B.; Launer, L.J.; Rosenberg, I.H.; Solomons, N.W.; et al. Uses and interpretation of anthropometry in the elderly for the assessment of physical status. Report to the Nutrition Unit of the World Health Organization: The Expert Subcommittee on the Use and Interpretation of Anthropometry in the Elderly. J. Nutr. Health Aging 1998, 2, 5–17. [Google Scholar] [PubMed]
- Agodi, A.; Barchitta, M.; Valenti, G.; Marzagalli, R.; Frontini, V.; Marchese, A.E. Increase in the prevalence of the MTHFR 677 TT polymorphism in women born since 1959: Potential implications for folate requirements. Eur. J. Clin. Nutr. 2011, 65, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Agrifoglio, O.; Scalisi, A.; Agodi, A. The Association of Dietary Patterns with High-Risk Human Papillomavirus Infection and Cervical Cancer: A Cross-Sectional Study in Italy. Nutrients 2018, 10, 469. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Barchitta, M.; Quattrocchi, A.; Maugeri, A.; Canto, C.; Marchese, A.E.; Vinciguerra, M. Low fruit consumption and folate deficiency are associated with LINE-1 hypomethylation in women of a cancer-free population. Genes Nutr. 2015, 10, 480. [Google Scholar] [CrossRef] [PubMed]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Barone, G.; Mazzoleni, P.; Catalfo, A.; De Guidi, G.; Iemmolo, M.G.; Crimi, N.; Agodi, A. Mediterranean Diet and Particulate Matter Exposure Are Associated with LINE-1 Methylation: Results from a Cross-Sectional Study in Women. Front. Genet. 2018, 9, 514. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Maugeri, A.; Kunzova, S.; Sochor, O.; Bauerova, H.; Kiacova, N.; Barchitta, M.; Vinciguerra, M. Association of Dietary Patterns with Metabolic Syndrome: Results from the Kardiovize Brno 2030 Study. Nutrients 2018, 10, 898. [Google Scholar] [CrossRef]
- Olson, C.M.; Strawderman, M.S. Modifiable behavioral factors in a biopsychosocial model predict inadequate and excessive gestational weight gain. J. Am. Diet. Assoc. 2003, 103, 48–54. [Google Scholar] [CrossRef]
- Shin, D.; Bianchi, L.; Chung, H.; Weatherspoon, L.; Song, W.O. Is gestational weight gain associated with diet quality during pregnancy? Matern. Child Health J. 2014, 18, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Lampe, J.W. Health effects of vegetables and fruit: Assessing mechanisms of action in human experimental studies. Am. J. Clin. Nutr. 1999, 70, 475S–490S. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; He, J.R.; Lin, Y.; Lu, M.; Zhou, Q.; Li, S.; Lu, J.; Yuan, M.; Chen, N.; Zhang, L.; et al. The influence of maternal dietary patterns on gestational weight gain: A large prospective cohort study in China. Nutrition 2019, 59, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Freisling, H.; van Bakel, M.M.; Biessy, C.; May, A.M.; Byrnes, G.; Norat, T.; Rinaldi, S.; Santucci de Magistris, M.; Grioni, S.; Bueno-de-Mesquita, H.B.; et al. Dietary reporting errors on 24 h recalls and dietary questionnaires are associated with BMI across six European countries as evaluated with recovery biomarkers for protein and potassium intake. Br. J. Nutr. 2012, 107, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Ellis, K.J.; Wong, W.W.; Hopkinson, J.M.; Smith, E.O. Composition of gestational weight gain impacts maternal fat retention and infant birth weight. Am. J. Obstet. Gynecol. 2003, 189, 1423–1432. [Google Scholar] [CrossRef]
- Leddy, M.A.; Power, M.L.; Schulkin, J. The impact of maternal obesity on maternal and fetal health. Rev. Obstet. Gynecol. 2008, 1, 170–178. [Google Scholar] [PubMed]
- Randall, E.; Marshall, J.R.; Graham, S.; Brasure, J. High-risk health behaviors associated with various dietary patterns. Nutr. Cancer 1991, 16, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Kerver, J.M.; Yang, E.J.; Bianchi, L.; Song, W.O. Dietary patterns associated with risk factors for cardiovascular disease in healthy US adults. Am. J. Clin. Nutr. 2003, 78, 1103–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tielemans, M.J.; Erler, N.S.; Leermakers, E.T.; van den Broek, M.; Jaddoe, V.W.; Steegers, E.A.; Kiefte-de Jong, J.C.; Franco, O.H. A Priori and a Posteriori Dietary Patterns during Pregnancy and Gestational Weight Gain: The Generation R Study. Nutrients 2015, 7, 9383–9399. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Pisa, P.T.; Norris, S.A. The Influence of Maternal Dietary Patterns on Body Mass Index and Gestational Weight Gain in Urban Black South African Women. Nutrients 2017, 9, 732. [Google Scholar] [CrossRef]
- Tielemans, M.J.; Garcia, A.H.; Peralta Santos, A.; Bramer, W.M.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; de Jonge, E.A.; Visser, T.L.; et al. Macronutrient composition and gestational weight gain: A systematic review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.E.; Ellison, G.T. Practical approaches for estimating prepregnant body weight. J. Nurse Midwifery 1998, 43, 97–101. [Google Scholar] [CrossRef]
- Oken, E.; Taveras, E.M.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Gestational weight gain and child adiposity at age 3 years. Am. J. Obstet. Gynecol. 2007, 196, 322.e1–322.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C.; Steyerberg, E.W. The number of subjects per variable required in linear regression analyses. J. Clin. Epidemiol. 2015, 68, 627–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talai Rad, N.; Ritterath, C.; Siegmund, T.; Wascher, C.; Siebert, G.; Henrich, W.; Buhling, K.J. Longitudinal analysis of changes in energy intake and macronutrient composition during pregnancy and 6 weeks post-partum. Arch. Gynecol. Obstet. 2011, 283, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Inskip, H.M.; Crozier, S.R.; Godfrey, K.M.; Borland, S.E.; Cooper, C.; Robinson, S.M. Women’s compliance with nutrition and lifestyle recommendations before pregnancy: General population cohort study. BMJ 2009, 338, b481. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Reduced GWG (n = 73) | Adequate GWG (n = 95) | Excessive GWG (n = 64) | p-Value a |
|---|---|---|---|---|
| Age b | 37.0 (4.0) | 38.0 (5.0) | 37.0 (4.0) | 0.546 |
| Educational level (low-medium %) c | 15.1% | 13.4% | 17.2% | 0.804 |
| Working (%) | 58.9% | 63.9% | 54.7% | 0.495 |
| Smoking (%) | 15.1% | 17.7% | 22.2% | 0.553 |
| Pre-pregnancy weight b | 61.0 (13.3) | 59.0 (13.0) | 64.0 (17.8) | <0.001 |
| Pre-pregnancy BMI b | 23.1 (4.4) | 21.6 (3.8) | 24.2 (6.5) | 0.002 |
| Pre-pregnancy BMI categories | ||||
| Underweight | 6.8% | 8.2% | 9.4% | 0.001 |
| Normal weight | 68.5% | 77.3% | 46.9% | |
| Overweight | 15.1% | 7.2% | 32.8% | |
| Obese | 9.6% | 7.2% | 10.9% | |
| Weight at delivery b | 68.0 (10.0) | 72.0 (14.0) | 82.0 (16.7) | <0.001 |
| Length of gestation b | 39.0 (2.0) | 39.0 (2.0) | 39.2 (2.0) | 0.701 |
| Birth weight b | 3.2 (0.6) | 3.2 (0.6) | 3.3 (0.6) | 0.039 |
| Birth length b | 50.0 (2.0) | 50.0 (2.0) | 50.0 (2.0) | 0.286 |
| Characteristics | 1st Tertile | 2nd Tertile | 3rd Tertile | p-Value a |
|---|---|---|---|---|
| Age b | 38.0 (5.0) | 38.0 (4.0) | 36.0 (3.0) | <0.001 |
| Gestational age b | 16.0 (3.0) | 16.0 (4.0) | 16.0 (2.0) | 0.777 |
| Educational level (low-medium %) c | 20.0% | 11.7% | 26.4% | 0.022 |
| Working (%) | 59.1% | 63.1% | 52.7% | 0.291 |
| Smoking (%) | 17.4% | 16.2% | 27.5% | 0.074 |
| Use of folic acid supplements (%) | 95.1% | 94.7% | 94.7% | 0.949 |
| Use of other multivitamin supplements (%) | 44.4% | 33.3% | 42.1% | 0.334 |
| Pre-pregnancy weight b | 60.0 (14.2) | 62.5 (15.0) | 60.0 (15.0) | 0.923 |
| Pre-pregnancy BMI b | 22.3 (4.4) | 22.7 (5.0) | 22.8 (5.5) | 0.704 |
| Pre-pregnancy BMI categories | ||||
| Underweight | 7.3% | 7.2% | 6.4% | 0.687 |
| Normal weight | 63.6% | 69.4% | 66.1% | |
| Overweight | 17.3% | 13.5% | 21.1% | |
| Obese | 11.8% | 9.9% | 6.4% | |
| Weight at delivery b | 71.5 (16.5) | 74.0 (16.0) | 74.0 (14.0) | 0.636 |
| Length of gestation b | 39.0 (2.0) | 39.0 (2.0) | 39.0 (2.0) | 0.976 |
| Birth weight b | 3.2 (0.6) | 3.2 (0.7) | 3.3 (0.5) | 0.800 |
| Length b | 50.0 (2.0) | 50.0 (1.0) | 50.0 (2.0) | 0.391 |
| GWG b | 11.5 (7.2) | 13.0 (7.0) | 13.0 (9.0) | 0.056 |
| GWG classification | ||||
| Reduced | 36.6% | 28.0% | 28.9% | 0.162 |
| Adequate | 41.5% | 48.0% | 34.2% | |
| Excessive | 22% | 24% | 36.8% | |
| Characteristics | 1st Tertile | 2nd Tertile | 3rd Tertile | p-Value a |
|---|---|---|---|---|
| Age b | 38.0 (5.0) | 37.0 (4.0) | 37.0 (4.0) | 0.675 |
| Gestational age b | 16.0 (1.0) | 16.0 (3.0) | 15.0 (5.0) | 0.001 |
| Educational level (low-medium %) c | 22.7% | 19.8% | 15.5% | 0.389 |
| Working (%) | 57.3% | 60.4% | 57.3% | 0.865 |
| Smoking (%) | 20.9% | 18.0% | 22.2% | 0.731 |
| Use of folic acid supplements (%) | 91.7% | 93.8% | 98.7% | 0.210 |
| Use of other multivitamin supplements (%) | 59.7% | 61.0% | 59.0% | 0.966 |
| Pre-pregnancy weight b | 63.0 (12.0) | 60.5 (14.2) | 58.5 (14.0) | 0.043 |
| Pre-pregnancy BMI b | 23.2 (4.7) | 22.7 (4.7) | 21.8 (5.1) | 0.019 |
| Pre-pregnancy BMI categories | ||||
| Underweight | 5.5% | 8.1% | 7.3% | 0.007 |
| Normal weight | 64.5% | 65.8% | 70.8% | |
| Overweight | 20.9% | 17.4% | 14.5% | |
| Obese | 9.1% | 8.7% | 7.4% | |
| Weight at delivery b | 74.0 (17.0) | 73.5 (14.2) | 72.0 (15.0) | 0.551 |
| Length of gestation b | 39.0 (2.0) | 39.0 (2.0) | 39.0 (2.0) | 0.562 |
| Birth weight b | 3.2 (0.6) | 3.2 (0.6) | 3.3 (0.7) | 0.522 |
| Length b | 50.0 (2.0) | 50.0 (2.0) | 50.0 (2.0) | 0.935 |
| GWG b | 12.0 (8.0) | 12.0 (6.2) | 13.0 (7.5) | 0.830 |
| GWG classification | ||||
| Reduced | 31.9% | 34.1% | 27.8% | 0.823 |
| Adequate | 37.5% | 40.2% | 45.6% | |
| Excessive | 30.6% | 25.6% | 26.6% | |
| Dietary Patterns | Total | Underweight | Normal Weight | Overweight | Obese | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | |
| Western | |||||||||||||||
| 1st tertile | Ref | Ref | Ref | Ref | Ref | ||||||||||
| 2nd tertile | 1.369 | 0.971 | 0.161 | 1.198 | 5.516 | 0.848 | 1.218 | 0.992 | 0.223 | 5.003 | 4.152 | 0.250 | 2.549 | 3.967 | 0.636 |
| 3rd tertile | 1.542 | 1.072 | 0.152 | 2.308 | 10.321 | 0.860 | 0.961 | 1.116 | 0.392 | 1.917 | 3.637 | 0.605 | 13.701 | 0.887 | 0.041 |
| Trend | 1.217 | 0.487 | 0.013 | −0.425 | 1.651 | 0.804 | 0.372 | 0.542 | 0.493 | 2.695 | 1.828 | 0.152 | 7.363 | 1.808 | 0.005 |
| Prudent | |||||||||||||||
| 1st tertile | Ref | Ref | Ref | Ref | Ref | ||||||||||
| 2nd tertile | −0.353 | 1.019 | 0.730 | −5.149 | 1.351 | 0.163 | 0.895 | 1.098 | 0.417 | −7.975 | 2.672 | 0.010 | −5.730 | 2.156 | 0.131 |
| 3rd tertile | 0.184 | 1.067 | 0.863 | 5.382 | 1.678 | 0.274 | −0.003 | 1.142 | 0.998 | −9.736 | 4.302 | 0.037 | −10.730 | 4.156 | 0.061 |
| Trend | 0.118 | 0.513 | 0.818 | 4.127 | 1.722 | 0.048 | 0.046 | 0.538 | 0.932 | −4.209 | 1.635 | 0.016 | −7.356 | 2.304 | 0.031 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Magnano San Lio, R.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients 2019, 11, 1308. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061308
Maugeri A, Barchitta M, Favara G, La Rosa MC, La Mastra C, Magnano San Lio R, Agodi A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients. 2019; 11(6):1308. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061308
Chicago/Turabian StyleMaugeri, Andrea, Martina Barchitta, Giuliana Favara, Maria Clara La Rosa, Claudia La Mastra, Roberta Magnano San Lio, and Antonella Agodi. 2019. "Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort" Nutrients 11, no. 6: 1308. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061308