Prevention of Allergic Sensitization and Treatment of Cow’s Milk Protein Allergy in Early Life: The Middle-East Step-Down Consensus

 ,
,
Abstract
:1. Introduction
2. Allergy Risk in Early Life
3. Clinical Presentation and Diagnosis of CMPA
3.1. IgE-Mediated
3.2. Non-IgE-Mediated
4. Allergy Prevention and CMPA Treatment in the Middle-East
4.1. Allergy Prevention
4.2. CMPA Treatment
5. Methods
6. Consensus Recommendations
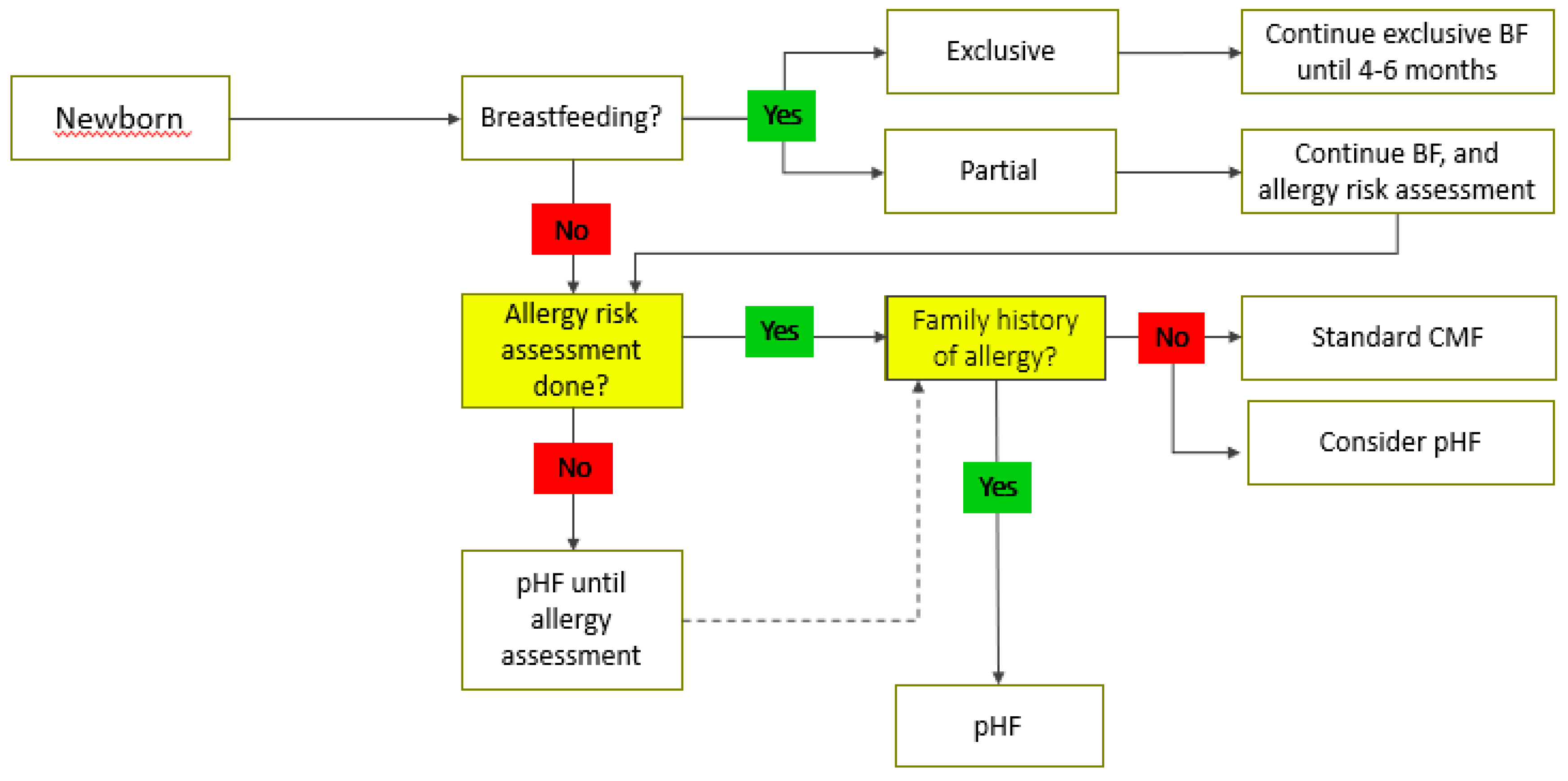
6.1. Prevention
6.2. Treatment
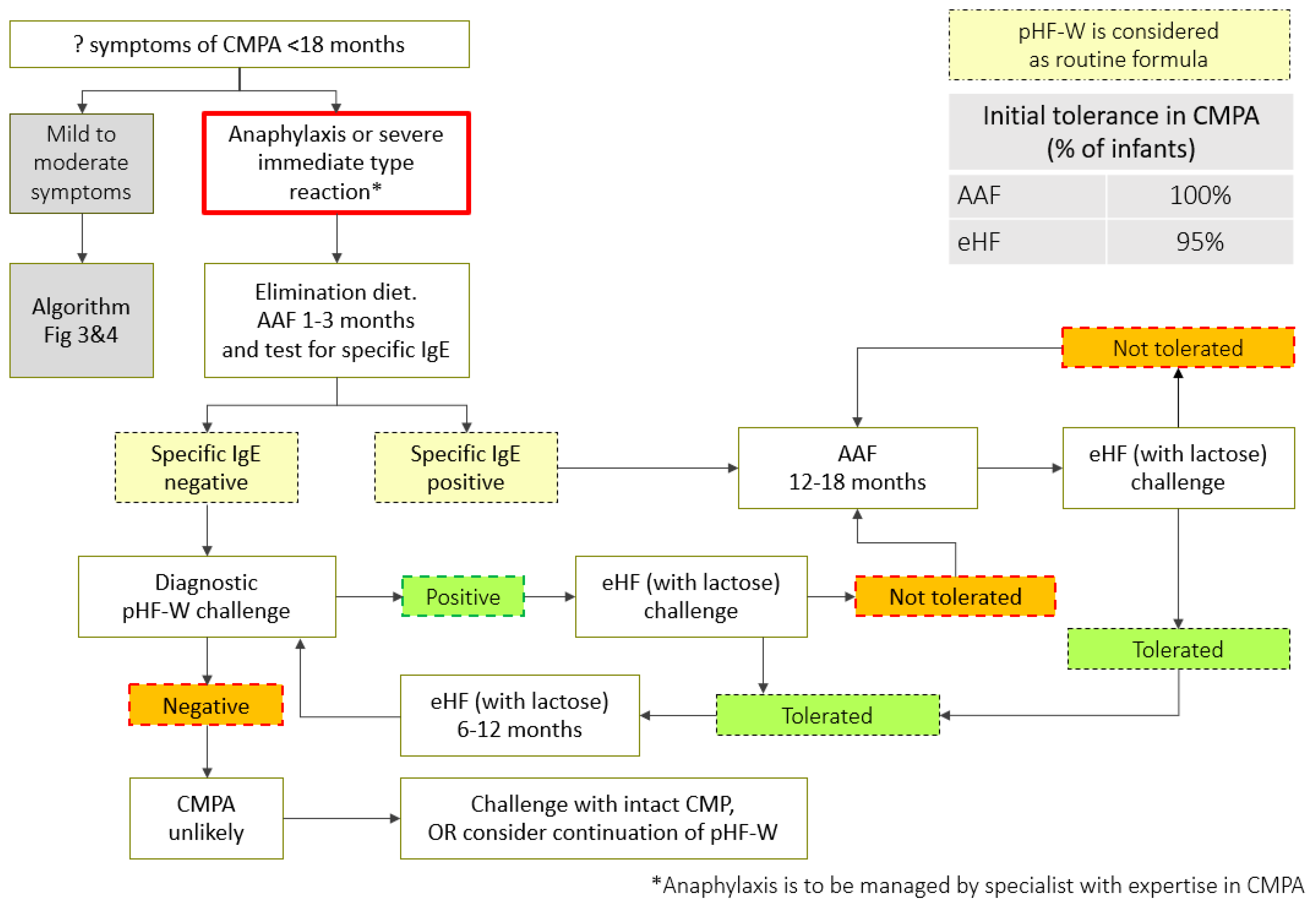
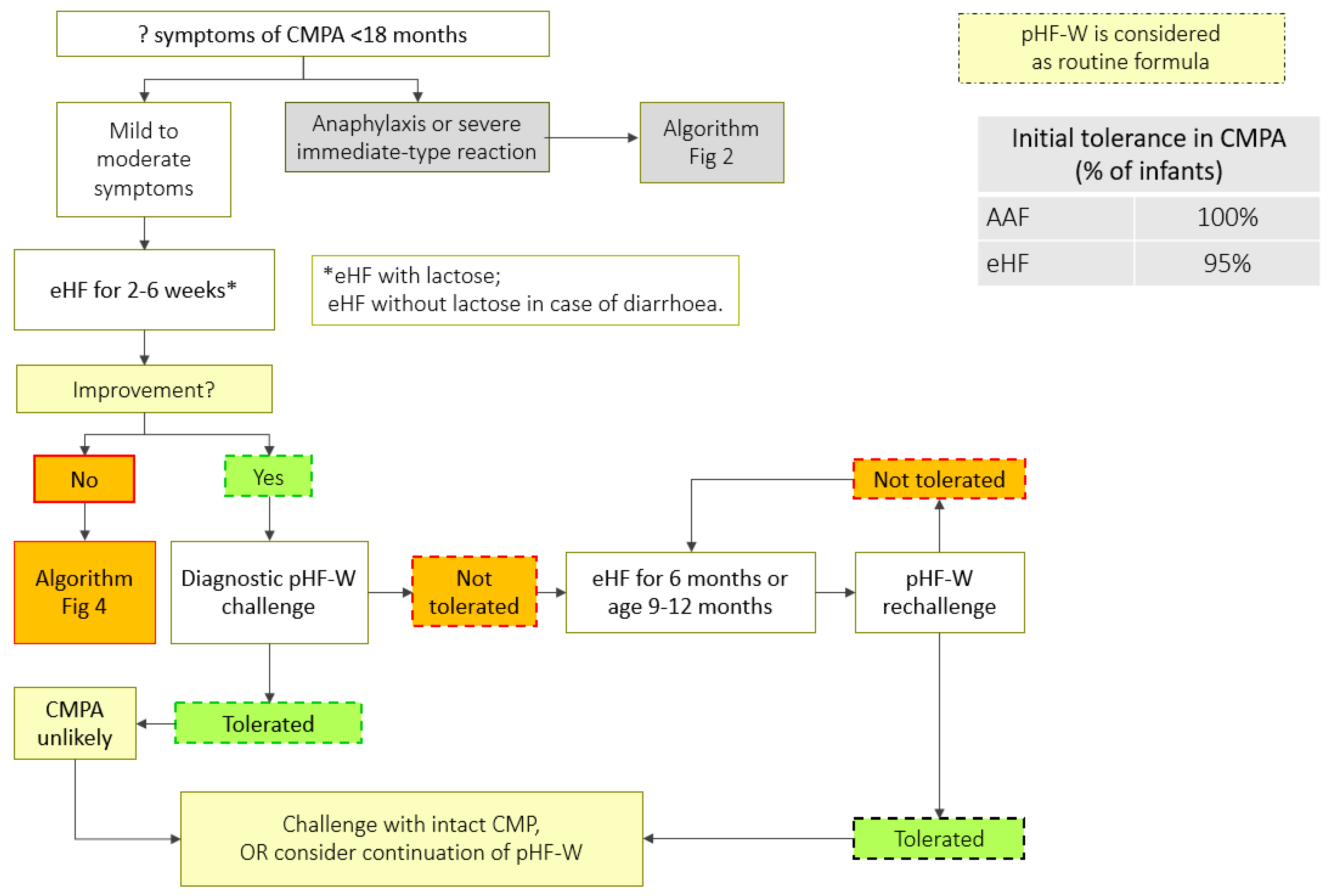
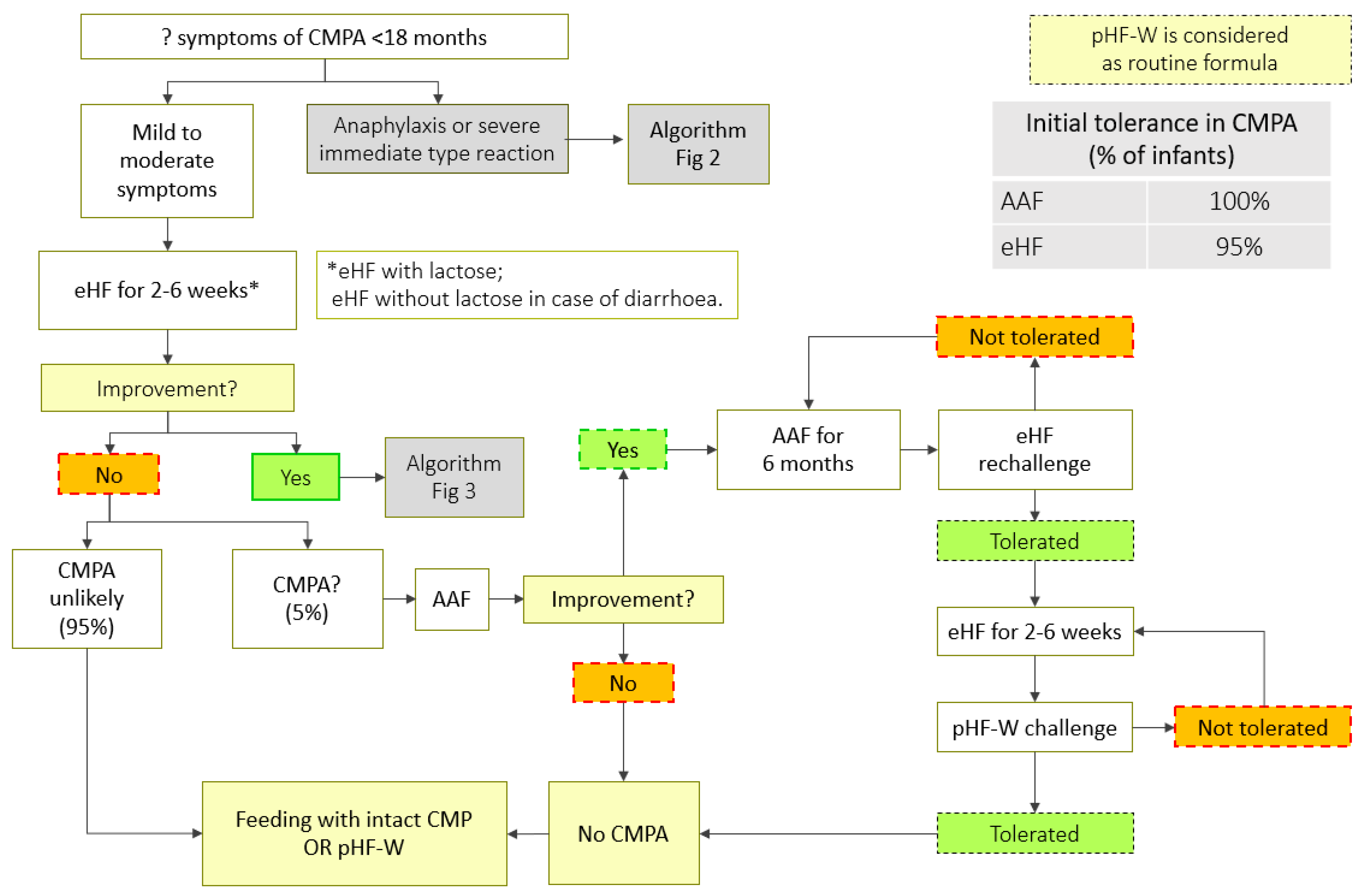
The Step-Down Approach for CMPA Treatment
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savage, J.; Johns, C.B. Food allergy: Epidemiology and natural history. Immunol. Allergy Clin. North Am. 2015, 35, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Oranje, A.P.; Wolkerstorfer, A.; de Waard-van der Spek, F.B. Natural course of cow’s milk allergy in childhood atopic eczema/dermatitis syndrome. Ann. Allergy Asthma Immunol. 2002, 89, 52–55. [Google Scholar] [CrossRef]
- Tikkanen, S.; Kokkonen, J.; Juntti, H.; Niinimäki, A. Status of children with cow’s milk allergy in infancy by 10 years of age. Acta Paediatr. 2000, 89, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Sardecka, I.; Łoś-Rycharska, E.; Ludwig, H.; Gawryjołek, J.; Krogulska, A. Early risk factors for cow’s milk allergy in children in the first year of life. Allergy Asthma Proc. 2018, 39, e44–e54. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, E.; Standl, M.; von Berg, A.; Lehmann, I.; Hoffmann, B.; Bauer, C.-P.; Koletzko, S.; Berdel, D.; Heinrich, J. Parental allergic disease before and after child birth poses similar risk for childhood allergies. Allergy 2015, 70, 873–876. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence. Food Allergy in Children and Young People; National Institute for Health and Clinical Excellence: London, UK, 2011. [Google Scholar]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.; Brown, T.; Meyer, R.; Walsh, J.; Shah, N.; Nowak-Węgrzyn, A.; Chen, T.-X.; Fleischer, D.M.; Heine, R.G.; Levin, M.; et al. Better recognition, diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy: iMAP—An international interpretation of the MAP (Milk Allergy in Primary Care) guideline. Clin. Transl. Allergy 2017, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.J.F.; Sarinho, E.S.C.; Motta, M.E.F.A.; Gomes, P.N.; de Oliveira de Melo, S.M.; da Silva, G.A.P. Allergy to cow’s milk proteins: What contribution does hypersensitivity in skin tests have to this diagnosis? Pediatr. Allergy Immunol. 2011, 22, e133–e138. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Dupont, C.; Eigenmann, P.; Host, A.; Kuitunen, M.; Ribes-Koninckx, C.; Shah, N.; Shamir, R.; Staiano, A.; Szajewska, H.; et al. A workshop report on the development of the Cow’s Milk-related Symptom Score awareness tool for young children. Acta Paediatr. 2015, 104, 334–339. [Google Scholar] [CrossRef]
- Breastfeeding. Available online: https://www.who.int/topics/breastfeeding/en/ (accessed on 13 March 2019).
- Alfaleh, K.; Alluwaimi, E.; Aljefri, S.; Alosaimi, A.; Behaisi, M. Infant formula in saudi arabia: A cross sectional survey. Kuwait Med. J. 2014, 46, 328–332. [Google Scholar]
- Al-Nuaimi, N.; Katende, G.; Arulappan, J. Breastfeeding Trends and Determinants: Implications and recommendations for Gulf Cooperation Council countries. Sultan Qaboos Univ. Med. J. 2017, 17, e155–e161. [Google Scholar] [CrossRef] [PubMed]
- Alzaheb, R.A. A review of the factors associated with the timely initiation of breastfeeding and exclusive breastfeeding in the Middle East. Clin. Med. Insights Pediatr. 2017, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gardner, H.; Green, K.; Gardner, A. Infant feeding practices of emirati women in the rapidly developing city of Abu Dhabi, United Arab Emirates. Int. J. Environ. Res. Public Health 2015, 12, 10923–10940. [Google Scholar] [CrossRef]
- Sheehan, W.J.; Gardynski, A.; Phipatanakul, W. Skin testing with water buffalo’s milk in children with cow’s milk allergy. Pediatr. Asthma. Allergy Immunol. 2009, 22, 121–125. [Google Scholar] [CrossRef]
- Restani, P.; Beretta, B.; Fiocchi, A.; Ballabio, C.; Galli, C.L. Cross-reactivity between mammalian proteins. Ann. Allergy Asthma Immunol. 2002, 89, 11–15. [Google Scholar] [CrossRef]
- Bellioni-Businco, B.; Paganelli, R.; Lucenti, P.; Giampietro, P.G.; Perborn, H.; Businco, L. Allergenicity of goat’s milk in children with cow’s milk allergy. J. Allergy Clin. Immunol. 1999, 103, 1191–1194. [Google Scholar] [CrossRef]
- Ehlayel, M.; Bener, A.; Abu Hazeima, K.; Al-Mesaifri, F. Camel milk is a safer choice than goat milk for feeding children with cow milk allergy. ISRN Allergy 2011, 2011, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ehlayel, M.; Bener, A. Camel’s milk allergy. Allergy Asthma Proc. 2018, 39, 384–388. [Google Scholar] [CrossRef]
- Al-Hammadi, S.; El-Hassan, T.; Al-Reyami, L. Anaphylaxis to camel milk in an atopic child. Allergy 2010, 65, 1623–1625. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Abuabat, A.; Al-Hammadi, S.; Aly, G.S.; Miqdady, M.S.; Shaaban, S.Y.; Torbey, P.-H. Middle east consensus statement on the prevention, diagnosis, and management of cow’s milk protein allergy. Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 61–73. [Google Scholar] [CrossRef]
- Inuo, C.; Tanaka, K.; Suzuki, S.; Nakajima, Y.; Yamawaki, K.; Tsuge, I.; Urisu, A.; Kondo, Y. Oral immunotherapy using partially hydrolyzed formula for cow’s milk protein allergy: A randomized, controlled trial. Int. Arch. Allergy Immunol. 2018, 177, 259–268. [Google Scholar] [CrossRef] [PubMed]
- CDC Evaluation Research Team. Gaining Consensus among Stakeholders Through the Nominal Group Technique. Available online: https://www.cdc.gov/healthyyouth/evaluation/pdf/brief7.pdf (accessed on 13 March 2019).
- Nielsen, S.D.; Beverly, R.L.; Dallas, D.C. Milk proteins are predigested within the human mammary gland. J. Mammary Gland Biol. Neoplasia 2017, 22, 251–261. [Google Scholar] [CrossRef] [PubMed]
- von Berg, A.; Filipiak-Pittroff, B.; Krämer, U.; Hoffmann, B.; Link, E.; Beckmann, C.; Hoffmann, U.; Reinhardt, D.; Grübl, A.; Heinrich, J.; et al. Allergies in high-risk schoolchildren after early intervention with cow’s milk protein hydrolysates: 10-year results from the German Infant Nutritional Intervention (GINI) study. J. Allergy Clin. Immunol. 2013, 131, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- von Berg, A.; Koletzko, S.; Grübl, A.; Filipiak-Pittroff, B.; Wichmann, H.-E.; Bauer, C.P.; Reinhardt, D.; Berdel, D.; German Infant Nutritional Intervention Study Group. The effect of hydrolyzed cow’s milk formula for allergy prevention in the first year of life: the German Infant Nutritional Intervention Study, a randomized double-blind trial. J. Allergy Clin. Immunol. 2003, 111, 533–540. [Google Scholar] [CrossRef] [PubMed]
- von Berg, A.; Filipiak-Pittroff, B.; Schulz, H.; Hoffmann, U.; Link, E.; Sußmann, M.; Schnappinger, M.; Brüske, I.; Standl, M.; Krämer, U.; et al. Allergic manifestation 15 years after early intervention with hydrolyzed formulas--the GINI Study. Allergy 2016, 71, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Horvath, A. A partially hydrolyzed 100% whey formula and the risk of eczema and any allergy: an updated meta-analysis. World Allergy Organ. J. 2017, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Pecquet, S.; Bovetto, L.; Maynard, F.; Fritsché, R. Peptides obtained by tryptic hydrolysis of bovine β-lactoglobulin induce specific oral tolerance in mice. J. Allergy Clin. Immunol. 2000, 105, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Fritsché, R.; Pahud, J.J.; Pecquet, S.; Pfeifer, A. Induction of systemic immunologic tolerance to beta-lactoglobulin by oral administration of a whey protein hydrolysate. J. Allergy Clin. Immunol. 1997, 100, 266–273. [Google Scholar] [CrossRef]
- Billeaud, C.; Guillet, J.; Sandler, B. Gastric emptying in infants with or without gastro-oesophageal reflux according to the type of milk. Eur. J. Clin. Nutr. 1990, 44, 577–583. [Google Scholar]
- Exl, B.M.; Deland, U.; Secretin, M.C.; Preysch, U.; Wall, M.; Shmerling, D.H. Improved general health status in an unselected infant population following an allergen-reduced dietary intervention programme: the ZUFF-STUDY-PROGRAMME. Part II: Infant growth and health status to age 6 months. ZUg-FrauenFeld. Eur. J. Nutr. 2000, 39, 145–156. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ierodiakonou, D.; Khan, T.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Afxentiou, T.; Reeves, T.; Cunha, S.; et al. Hydrolysed formula and risk of allergic or autoimmune disease: Systematic review and meta-analysis. BMJ 2016, 352, i974. [Google Scholar] [CrossRef] [PubMed]
- Giampietro, P.G.; Kjellman, N.I.; Oldaeus, G.; Wouters-Wesseling, W.; Businco, L. Hypoallergenicity of an extensively hydrolyzed whey formula. Pediatr. Allergy Immunol. 2001, 12, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, J.; Greer, F.; American Academy of Pediatrics Committee on Nutrition. Use of soy protein-based formulas in infant feeding. Pediatrics 2008, 121, 1062–1068. [Google Scholar] [CrossRef] [PubMed]
- Dennis, S.; Fitzpatrick, S.; Egan, K.; Flannery, B.; Kanwal, R.; Smegal, D.; Spungen, J.; Tao, S. Arsenic in Rice and Rice Products Risk Assessment Report; Center for Food Safety and Applied Nutrition, Food and Drug Administration, U.S. Department of Health and Human Services: Washington, DC, USA, 2016.
- Hojsak, I.; Braegger, C.; Bronsky, J.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Mis, N.F.; Mihatsch, W.; et al. Arsenic in rice: A cause for concern. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R.; Carey, M.P.; Turner, P.J.; Meharg, A.A. Low inorganic arsenic in hydrolyzed rice formula used for cow’s milk protein allergy. Pediatr. Allergy Immunol. 2018, 29, 561–563. [Google Scholar] [CrossRef]
- Werkstetter, K.; Chmielewska, A.; Dolinšek, J.; Burk, F.E.; Korponay-Szabó, I.; Kurppa, K.; Mišak, Z.; Papadopoulou, A.; Popp, A.; Ribes-Konickx, C.; et al. Diagnosis and management of cow’s milk protein allergy—How big is the gap between ideal and reality? A quality-of-care survey in Europe. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 399–400. [Google Scholar]
- Salvatore, S.; Abkari, A.; Cai, W.; Catto-Smith, A.; Cruchet, S.; Gottrand, F.; Hegar, B.; Lifschitz, C.; Ludwig, T.; Shah, N.; et al. Review shows that parental reassurance and nutritional advice help to optimise the management of functional gastrointestinal disorders in infants. Acta Paediatr. 2018, 107, 1512–1520. [Google Scholar] [CrossRef]
- Francavilla, R.; Calasso, M.; Calace, L.; Siragusa, S.; Ndagijimana, M.; Vernocchi, P.; Brunetti, L.; Mancino, G.; Tedeschi, G.; Guerzoni, E.; et al. Effect of lactose on gut microbiota and metabolome of infants with cow’s milk allergy. Pediatr. Allergy Immunol. 2012, 23, 420–427. [Google Scholar] [CrossRef]
- Vandenplas, Y. Lactose intolerance. Asia Pac. J. Clin. Nutr. 2015, 24 (Suppl. 1), S9–S13. [Google Scholar]
- Heine, R.G.; AlRefaee, F.; Bachina, P.; De Leon, J.C.; Geng, L.; Gong, S.; Madrazo, J.A.; Ngamphaiboon, J.; Ong, C.; Rogacion, J.M. Lactose intolerance and gastrointestinal cow’s milk allergy in infants and children—Common misconceptions revisited. World Allergy Organ. J. 2017, 10, 41. [Google Scholar] [CrossRef]
- Järvinen, K.M.; Chatchatee, P. Mammalian milk allergy: Clinical suspicion, cross-reactivities and diagnosis. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 251–258. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
| Sr. No. | Statement | Agreement |
|---|---|---|
| 1 | Exclusive breastfeeding up to 6 months is the best feeding for every infant to achieve optimal growth, development, and health (WHO statement). | 100% (rating 9) |
| 2 | When breastfeeding is not possible or when breast milk is not available, partially hydrolyzed whey formula (pHF-W) with documented safety and efficacy should be recommended for infants at risk of allergy. | 100% (rating 9) |
| 3 | Not all pHFs are the same, as different formulations have different peptide compositions and production methods and have demonstrated different outcomes. | 100% (rating 9) |
| 4 | When breastfeeding is not possible or when breast milk is not available, pHF-W with documented safety and efficacy could be considered for all infants. | 100% (rating 9) |
| Sr. No. | Statement | Agreement |
|---|---|---|
| 1 | Management of cow milk protein allergy involves avoidance of cow milk protein, through extensively hydrolyzed formula (eHF) in most of the infants, or if it is not tolerated, amino acid formula (AAF). | 100% (rating 9) |
| 2 | In case of anaphylaxis, start with AA-based formula | 100% (rating 9) |
| 3 | pHF-W can be used in the transition from eHF or AAF to intact CMP, if the initial pHF-W challenge is tolerated by the child. | 100% (rating 9) |
| 4 | pHF formulas should not be interchanged, as the formulas differ in their clinical outcomes. | 100% (rating 9) |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vandenplas, Y.; Al-Hussaini, B.; Al-Mannaei, K.; Al-Sunaid, A.; Helmi Ayesh, W.; El-Degeir, M.; El-Kabbany, N.; Haddad, J.; Hashmi, A.; Kreishan, F.; et al. Prevention of Allergic Sensitization and Treatment of Cow’s Milk Protein Allergy in Early Life: The Middle-East Step-Down Consensus. Nutrients 2019, 11, 1444. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071444
Vandenplas Y, Al-Hussaini B, Al-Mannaei K, Al-Sunaid A, Helmi Ayesh W, El-Degeir M, El-Kabbany N, Haddad J, Hashmi A, Kreishan F, et al. Prevention of Allergic Sensitization and Treatment of Cow’s Milk Protein Allergy in Early Life: The Middle-East Step-Down Consensus. Nutrients. 2019; 11(7):1444. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071444
Chicago/Turabian StyleVandenplas, Yvan, Bakr Al-Hussaini, Khaled Al-Mannaei, Areej Al-Sunaid, Wafaa Helmi Ayesh, Manal El-Degeir, Nevine El-Kabbany, Joseph Haddad, Aziza Hashmi, Furat Kreishan, and et al. 2019. "Prevention of Allergic Sensitization and Treatment of Cow’s Milk Protein Allergy in Early Life: The Middle-East Step-Down Consensus" Nutrients 11, no. 7: 1444. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071444