Central But Not General Obesity Is Positively Associated with the Risk of Hyperhomocysteinemia in Middle-Aged Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
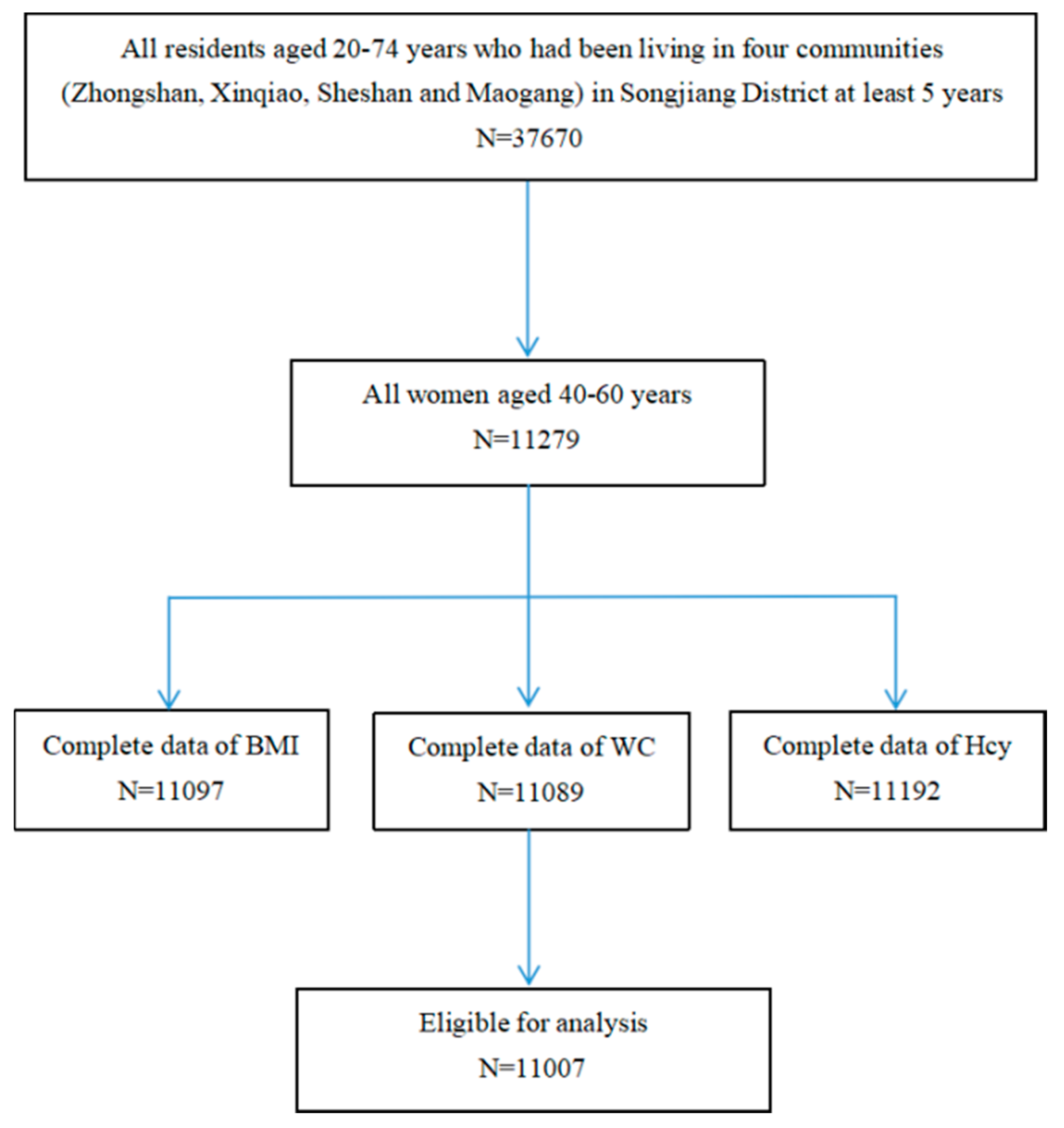
2.1. Study Design and Subjects
2.2. Anthropometric and Other Measurements
2.3. Biological Sample Collection and Determination
2.4. Statistical Analysis
2.5. Ethics Statement
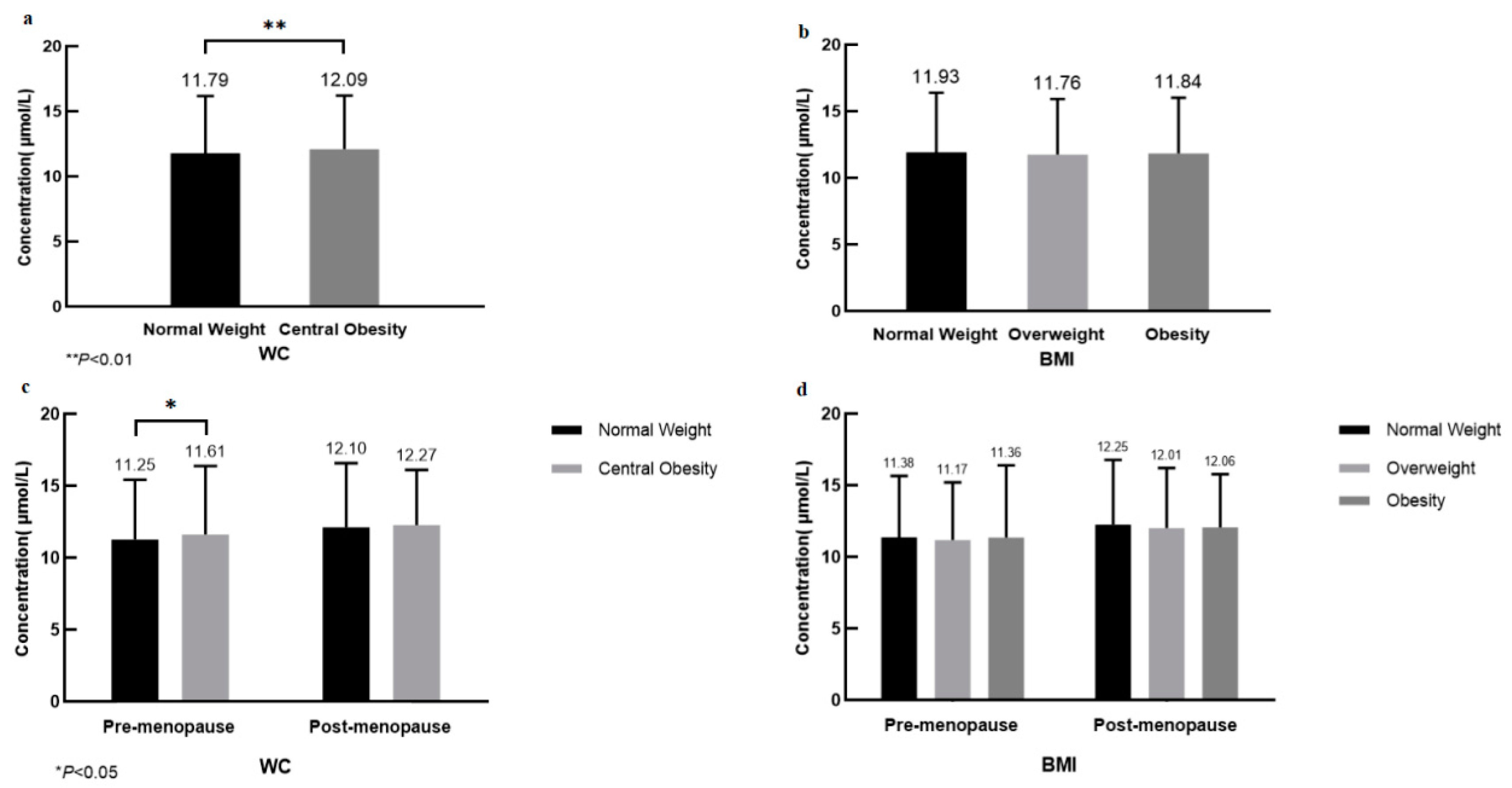
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CVD | cardiovascular disease |
| Hcy | homocysteine |
| HHcy | hyperhomocysteinemia |
| BMI | body mass index |
| WC | waist circumference |
References
- Ganguly, P.; Alam, S.F. Role of homocysteine in the development of cardiovascular disease. Nutr. J. 2015, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Hu, J.; Dong, Y.; Zhan, R.; Li, P.; Su, H.; Peng, Q.; Wu, T.; Lei, L.; Huang, X.; et al. Gender Differences in the Risk Factors for Endothelial Dysfunction in Chinese Hypertensive Patients: Homocysteine is an Independent Risk Factor in Females. PLoS ONE 2015, 10, e0118686. [Google Scholar] [CrossRef] [PubMed]
- McCully, K.S. Homocysteine Metabolism, Atherosclerosis, and Diseases of Aging. Compr. Physiol. 2015, 6, 471–505. [Google Scholar] [PubMed]
- Heijer, M.D.; Rosendaal, F.R.; Blom, H.J.; Gerrits, W.B.J.; Bos, G.M.J. Hyperhomocysteinemia and Venous Thrombosis: A Meta-analysis. Thromb. Haemost. 1998, 80, 874–877. [Google Scholar] [CrossRef]
- Haslam, D.W.; James, W.P.T. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef]
- Nakazato, M.; Maeda, T.; Takamura, N.; Wada, M.; Yamasaki, H.; Johnston, K.E.; Tamura, T. Relation of body mass index to blood folate and total homocysteine concentrations in Japanese adults. Eur. J. Nutr. 2011, 50, 581–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elshorbagy, A.K.; Nurk, E.; Gjesdal, C.G.; Tell, G.S.; Ueland, P.M.; Nygård, O.; Tverdal, A.; E Vollset, S.; Refsum, H. Homocysteine, cysteine, and body composition in the Hordaland Homocysteine Study: Does cysteine link amino acid and lipid metabolism? Am. J. Clin. Nutr. 2008, 88, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Bostom, A.G.; Wilson, P.W.; Rich, S.; Rosenberg, I.H.; Selhub, J. Determinants of plasma total homocysteine concentration in the Framingham Offspring cohort. Am. J. Clin. Nutr. 2001, 73, 613–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Bayyari, N.; Hamadneh, J.; Hailat, R.; Hamadneh, S. Total homocysteine is positively correlated with body mass index, waist-to-hip ratio, and fat mass among overweight reproductive women: A cross-sectional study. Nutr. Res. 2017, 48, 9–15. [Google Scholar] [CrossRef]
- Van Driel, L.M.J.W.; Eijkemans, M.J.C.; De Jonge, R.; De Vries, J.H.M.; Van Meurs, J.B.J.; Steegers, E.A.P.; Steegers-Theunissen, R.P.M. Body Mass Index Is an Important Determinant of Methylation Biomarkers in Women of Reproductive Ages. J. Nutr. 2009, 139, 2315–2321. [Google Scholar] [CrossRef]
- Astrup, A. Physical activity and weight gain and fat distribution changes with menopause: Current evidence and research issues. Med. Sci. Sports Exerc. 1999, 31, S564. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, A.A.; Lee, A.R. Estrogen and the cardiovascular system. Pharmacol. Ther. 2012, 135, 54–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Family Planning Commission of the People’s Republic of China. Health Standard of the People’s Republic of China. No. WS/T 428-2013: Criteria of Weight for Adults. 2013. Available online: http://g.wanfangdata.com.cn/details/detail.do?_type=standards&id=WS/T 428-2013 (accessed on 21 June 2019).
- Jin, M.; Wang, F.; Uthup, M.; Szydlowska, M. Analytical performance of an enzymatic cycling method for total homocysteine measurement. Clin. Chim. Acta 2009, 399, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-L.; Chen, S.-C. Microchip capillary electrophoresis with electrochemical detector for precolumn enzymatic analysis of glucose, creatinine, uric acid and ascorbic acid in urine and serum. Talanta 2004, 64, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Vayá, A.; Rivera, L.; Hernández-Mijares, A.; De La Fuente, M.; Solá, E.; Romagnoli, M.; Alis, R.; Laiz, B. Homocysteine levels in morbidly obese patients: Its association with waist circumference and insulin resistance. Clin. Hemorheol. Microcirc. 2012, 52, 49–56. [Google Scholar] [PubMed]
- Rhee, E.-J.; Hwang, S.-T.; Lee, W.-Y.; Yoon, J.-H.; Kim, B.-J.; Kim, B.-S.; Kang, J.-H.; Lee, M.-H.; Park, J.-R.; Sung, K.-C. Relationship between Metabolic Syndrome Categorized by Newly Recommended by International Diabetes Federation Criteria with Plasma Homocysteine Concentration. Endocr. J. 2007, 54, 995–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, G.A.; Bressan, J.; Oliveira, F.L.P.; Sant’Ana, H.M.P.; Pimenta, A.M.; Lopes, L.L.; Hermsdorff, H.H.M. Dietary Folate Intake Is Negatively Associated with Excess Body Weight in Brazilian Graduates and Postgraduates (CUME Project). Nutrients 2019, 11, 518. [Google Scholar] [CrossRef]
- Tamura, T.; Picciano, M.F. Folate and human reproduction. Am. J. Clin. Nutr. 2006, 83, 993–1016. [Google Scholar] [CrossRef]
- Schneede, J.; Refsum, H.; Ueland, P.M. Biological and Environmental Determinants of Plasma Homocysteine. Semin. Thromb. Hemost. 2000, 26, 263–280. [Google Scholar] [CrossRef]
- McNeil, C.J.; Hay, S.M.; Rucklidge, G.J.; Reid, M.; Duncan, G.; Maloney, C.A.; Rees, W.D. Disruption of lipid metabolism in the liver of the pregnant rat fed folate-deficient and methyl donor-deficient diets. Br. J. Nutr. 2008, 99, 262–271. [Google Scholar] [CrossRef] [Green Version]
- Björck, J.; Hellgren, M.; Råstam, L.; Lindblad, U. Associations between serum insulin and homocysteine in a Swedish population—A potential link between the metabolic syndrome and hyperhomocysteinemia: The Skaraborg project. Metabolism 2006, 55, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B.; Jacques, P.F.; Selhub, J.; Singer, D.E.; Nathan, D.M.; Rifai, N.; D’Agostino, R.B.; Wilson, P.W. Fasting Plasma Homocysteine Levels in the Insulin Resistance Syndrome: The Framingham Offspring Study. Diabetes Care 2001, 24, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Després, J.P. Abdominal obesity as important component of insulin-resistance syndrome. Nutrition 1993, 9, 452–459. [Google Scholar] [PubMed]
- Antonopoulos, A.S.; Oikonomou, E.; Antoniades, C.; Tousoulis, D. From the BMI paradox to the obesity paradox: The obesity-mortality association in coronary heart disease. Obes. Rev. 2016, 17, 989–1000. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Georgiades, A. Changes in Body Composition Predict Homocysteine Changes and Hyperhomocysteinemia in Korea. J. Korean Med Sci. 2013, 28, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Nair, K.S. Aging muscle. Am. J. Clin. Nutr. 2005, 81, 953–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, H.; Li, X.; Zheng, L.; Chen, X.; Lan, Q.; Wu, H.; Ding, X.; Qian, D.; Shen, Y.; Yu, Z.; et al. Abdominal obesity is strongly associated with Cardiovascular Disease and its Risk Factors in Elderly and very Elderly Community-dwelling Chinese. Sci. Rep. 2016, 6, 21521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pischon, T. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2010, 362, 2105–2120. [Google Scholar]
- Zhang, X.; Shu, X.-O.; Yang, G.; Li, H.; Cai, H.; Gao, Y.-T.; Zheng, W. Abdominal Adiposity and Mortality in Chinese Women. Arch. Intern. Med. 2007, 167, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Sponholtz, T.R.; Heuvel, E.R.V.D.; Xanthakis, V.; Vasan, R.S. Association of Variability in Body Mass Index and Metabolic Health with Cardiometabolic Disease Risk. J. Am. Hear. Assoc. 2019, 8, e010793. [Google Scholar] [CrossRef]
- Hou, X.H.; Lu, J.M.; Weng, J.P.; Ji, L.N.; Shan, Z.Y.; Liu, J.; Tian, H.M.; Ji, Q.H.; Zhu, D.L.; Ge, J.P.; et al. Impact of waist circumference and body mass index on risk of cardiometabolic disorder and cardiovascular disease in Chinese adults: A national diabetes and metabolic disorders survey. PLoS ONE 2013, 8, e57319. [Google Scholar] [CrossRef] [PubMed]
- Duval, K.; Prud’Homme, D.; Rabasa-Lhoret, R.; Strychar, I.; Brochu, M.; Lavoie, J.-M.; Doucet, E.; Karine, D.; Denis, P.; Rémi, R.-L.; et al. Effects of the menopausal transition on energy expenditure: A MONET Group Study. Eur. J. Clin. Nutr. 2013, 67, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Karvonen-Gutierrez, C.; Kim, C. Association of Mid-Life Changes in Body Size, Body Composition and Obesity Status with the Menopausal Transition. Health 2016, 4, 42. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, E.K.; Hofvind, S.; Byberg, L.; Eskild, A. The relation of age at menarche with age at natural menopause: A population study of 336 788 women in Norway. Hum. Reprod. 2018, 33, 1149–1157. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Subjects (n = 11,007) | Non-Hhcy (n = 9498) | Hhcy (n = 1509) | p Value | |
|---|---|---|---|---|
| Age (years) | <0.001 | |||
| 40–45 | 1211 (11.00) | 1097 (11.55) | 114 (7.55) | |
| 46–50 | 2225 (20.21) | 1997 (21.03) | 228 (15.11) | |
| 51–55 | 4057 (36.86) | 3504 (36.89) | 553 (36.65) | |
| 56–60 | 3514 (31.93) | 2900 (30.53) | 614 (40.69) | |
| Menopausal status | <0.001 | |||
| Pre-menopause | 3717 (33.77) | 3324 (35.00) | 393 (26.04) | |
| Post-menopause | 7290 (66.23) | 6174 (65.00) | 1116 (73.96) | |
| Body mass index (kg/m2) | 0.590 | |||
| <24.0 (normal weight) | 5807 (52.76) | 4993 (52.57) | 814 (53.94) | |
| 24.0–27.9 (overweight) | 3971 (36.08) | 3443 (36.25) | 528 (34.99) | |
| ≥28.0 (obesity) | 1229 (11.17) | 1062 (11.18) | 167 (11.07) | |
| Waist circumference (cm) | 0.002 | |||
| <85.00 (normal weight) | 8489 (77.12) | 7372 (77.62) | 1117 (74.02) | |
| ≥85.00 (central obesity) | 2518 (22.88) | 2126 (22.38) | 392 (25.98) | |
| Cardiovascular-related comorbidities | <0.001 | |||
| No | 7398 (67.21) | 6451 (67.92) | 947 (62.76) | |
| Yes | 3609 (32.79) | 3047 (32.08) | 562 (37.24) | |
| Education | 0.028 | |||
| Middle school or below | 3889 (35.33) | 3318 (34.93) | 571 (37.84) | |
| High school or above | 7118 (64.67) | 6180 (65.07) | 938 (62.16) | |
| Retired | <0.001 | |||
| No | 5162 (46.90) | 4543 (47.83) | 619 (41.02) | |
| Yes | 5845 (53.10) | 4955 (52.17) | 890 (58.98) | |
| Exercising | 0.013 | |||
| No | 7442 (67.61) | 6380 (67.17) | 1062 (70.38) | |
| Yes | 3565 (32.39) | 3118 (32.83) | 447 (29.62) | |
| Smoking | 0.359 | |||
| No | 10,967 (99.64) | 9467 (99.67) | 1500 (99.40) | |
| Yes | 31 (0.28) | 25 (0.26) | 6 (0.40) | |
| Alcohol drinking | 0.105 | |||
| No | 10,927 (99.27) | 9424 (99.22) | 1503 (99.60) | |
| Yes | 80 (0.73) | 74 (0.78) | 6 (0.40) | |
| Tea drinking | 0.004 | |||
| No | 9781 (88.86) | 8407 (88.51) | 1374 (91.05) | |
| Yes | 1226 (11.14) | 1091 (11.49) | 135 (8.95) |
| Total | Normal Weight | Central Obesity | |||
|---|---|---|---|---|---|
| Cases/n | OR (ref) | Cases/n | OR (95% CI) | ||
| All subjects a | 11,007 | 1117/8491 | 392/2518 | ||
| Model 1 | 1.00 | 1.13 (1.00–1.29) | |||
| Model 2 | 1.00 | 1.10 (0.97–1.26) | |||
| Model 3 | 1.00 | 1.30 (1.11–1.52) ** | |||
| Age (years) b | 1.00 | ||||
| 40–50 | 3436 | 279/2906 | 1.00 | 63/530 | 1.51 (1.04–2.20) * |
| 51–60 | 7571 | 838/5583 | 1.00 | 329/1988 | 1.27 (1.06–1.51) ** |
| Menopausal status b | |||||
| Pre-menopause | 3717 | 305/3050 | 1.00 | 88/667 | 1.44 (1.03–2.01) * |
| Post-menopause | 7290 | 812/5439 | 1.00 | 304/1851 | 1.26 (1.05–1.51) * |
| CVD-related comorbidities b | |||||
| No | 7398 | 755/6074 | 1.00 | 191/1324 | 1.17 (0.94–1.44) |
| Yes | 3610 | 361/2416 | 1.00 | 201/1194 | 1.52 (1.20–1.94) ** |
| Total | Normal Weight | Overweight | Obesity | ||||
|---|---|---|---|---|---|---|---|
| Cases/n | OR (ref) | Cases/n | OR (95%CI) | Cases/n | OR (95%CI) | ||
| All subjects a | 11,007 | 814/5807 | 528/3971 | 167/1229 | |||
| Model 1 | 1.00 | 0.89 (0.79–1.00) | 0.91 (0.76–1.09) | ||||
| Model 2 | 1.00 | 0.88 (0.78–0.99) * | 0.87 (0.73–1.05) | ||||
| Model 3 | 1.00 | 0.82 (0.72–0.93) ** | 0.71 (0.57–0.89) ** | ||||
| Age (years) b | |||||||
| 40–50 | 3436 | 213/2090 | 1.00 | 99/1038 | 0.86 (0.65–1.13) | 30/308 | 0.74 (0.45–1.23) |
| 51–60 | 7571 | 601/3717 | 1.00 | 429/2933 | 0.81 (0.70–0.94) ** | 137/921 | 0.70 (0.54–0.90) ** |
| Menopausal status b | |||||||
| Pre-menopause | 3717 | 231/2162 | 1.00 | 117/1167 | 0.80 (0.61–1.03) | 45/388 | 0.74 (0.47–1.15) |
| Post-menopause | 7290 | 583/3645 | 1.00 | 411/2804 | 0.82 (0.71–0.96) * | 122/841 | 0.70 (0.54–0.90) ** |
| CVD-related comorbidities b | |||||||
| No | 7398 | 559/4360 | 1.00 | 308/2434 | 0.90 (0.77–1.06) | 80/604 | 0.89 (0.66–1.20) |
| Yes | 3609 | 255/1447 | 1.00 | 220/1537 | 0.67 (0.54–0.84) ** | 87/625 | 0.52 (0.37–0.73) ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Jiang, Y.; Wang, N.; Zhu, M.; Liu, X.; Wang, R.; Jiang, F.; Chen, Y.; Zhao, Q.; Zhao, G. Central But Not General Obesity Is Positively Associated with the Risk of Hyperhomocysteinemia in Middle-Aged Women. Nutrients 2019, 11, 1614. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071614
Wang Y, Jiang Y, Wang N, Zhu M, Liu X, Wang R, Jiang F, Chen Y, Zhao Q, Zhao G. Central But Not General Obesity Is Positively Associated with the Risk of Hyperhomocysteinemia in Middle-Aged Women. Nutrients. 2019; 11(7):1614. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071614
Chicago/Turabian StyleWang, Yingying, Yonggen Jiang, Na Wang, Meiying Zhu, Xing Liu, Ruiping Wang, Feng Jiang, Yue Chen, Qi Zhao, and Genming Zhao. 2019. "Central But Not General Obesity Is Positively Associated with the Risk of Hyperhomocysteinemia in Middle-Aged Women" Nutrients 11, no. 7: 1614. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071614