The Validity of Children’s Fruit and Vegetable Intake Using Plasma Vitamins A, C, and E: The SAYCARE Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Objective
3. Methods
3.1. Study Design
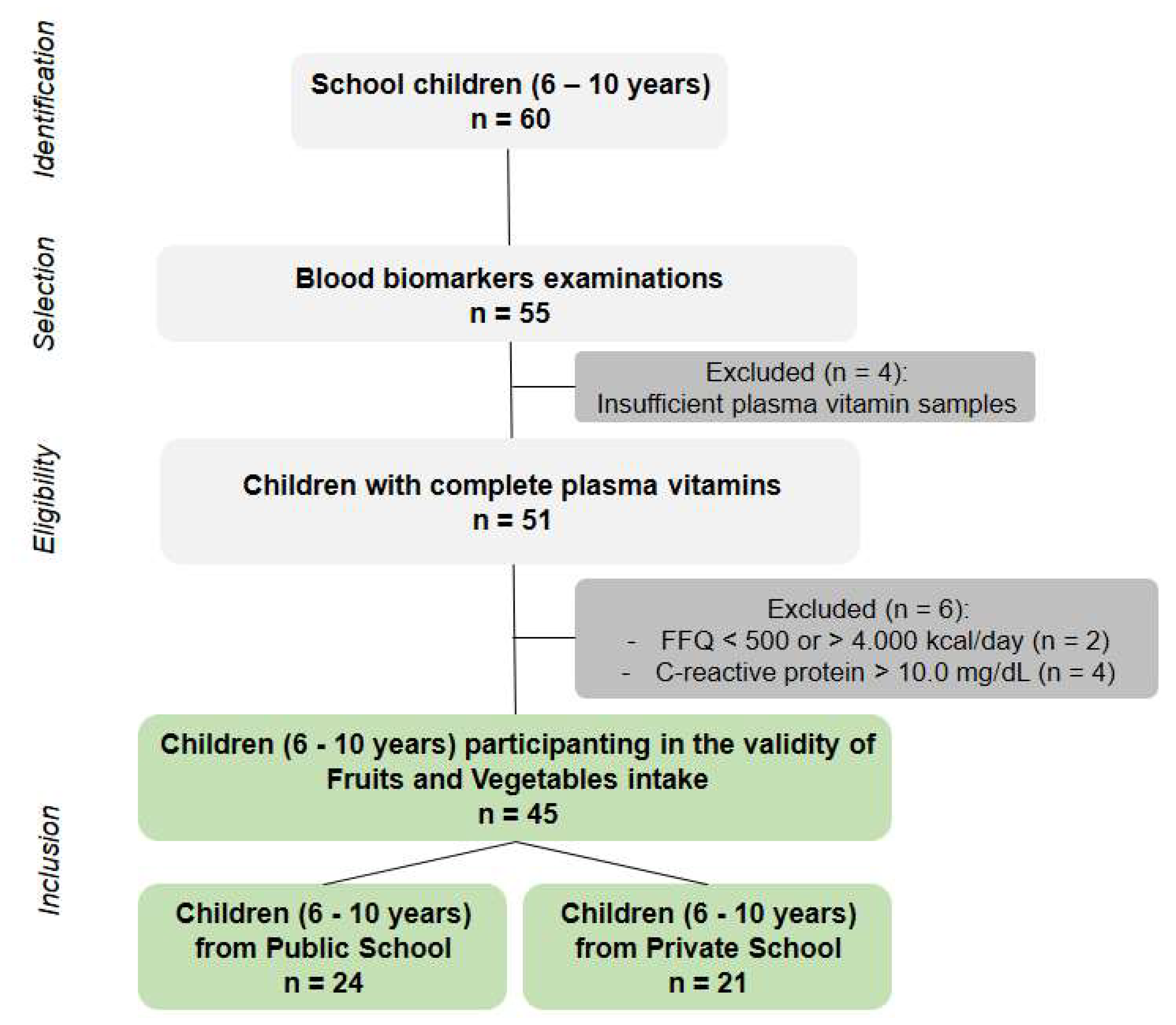
3.2. Study Population
Eligibility Criteria
3.3. Fieldwork
3.4. Anthropometric Measures
- Weight: Measured with an ultra Slim W801 digital scale, with a maximum capacity of 150 kg, and an accuracy of 0.1 kg (Crivitta Diagnostica Ltd., São Paulo, Brazil).
- Height: Measured with a wall stadiometer with a millimeter scale (Cardiomed, Paraná, Brazil).
- Waist circumference: Measured with a flexible and inextensible tape (in centimeters) positioned between the narrowest point between the last rib and the upper anterior iliac spine.
3.5. Subjective Dietary Assessment Methods
3.5.1. Food Frequency Questionnaire (FFQ)
3.5.2. 24-h Dietary Recall (24 h-DR)
3.6. Blood Processing and Analyzes
3.7. Statistics
3.8. Funding
3.9. Ethics
4. Results
4.1. Participant Characteristics
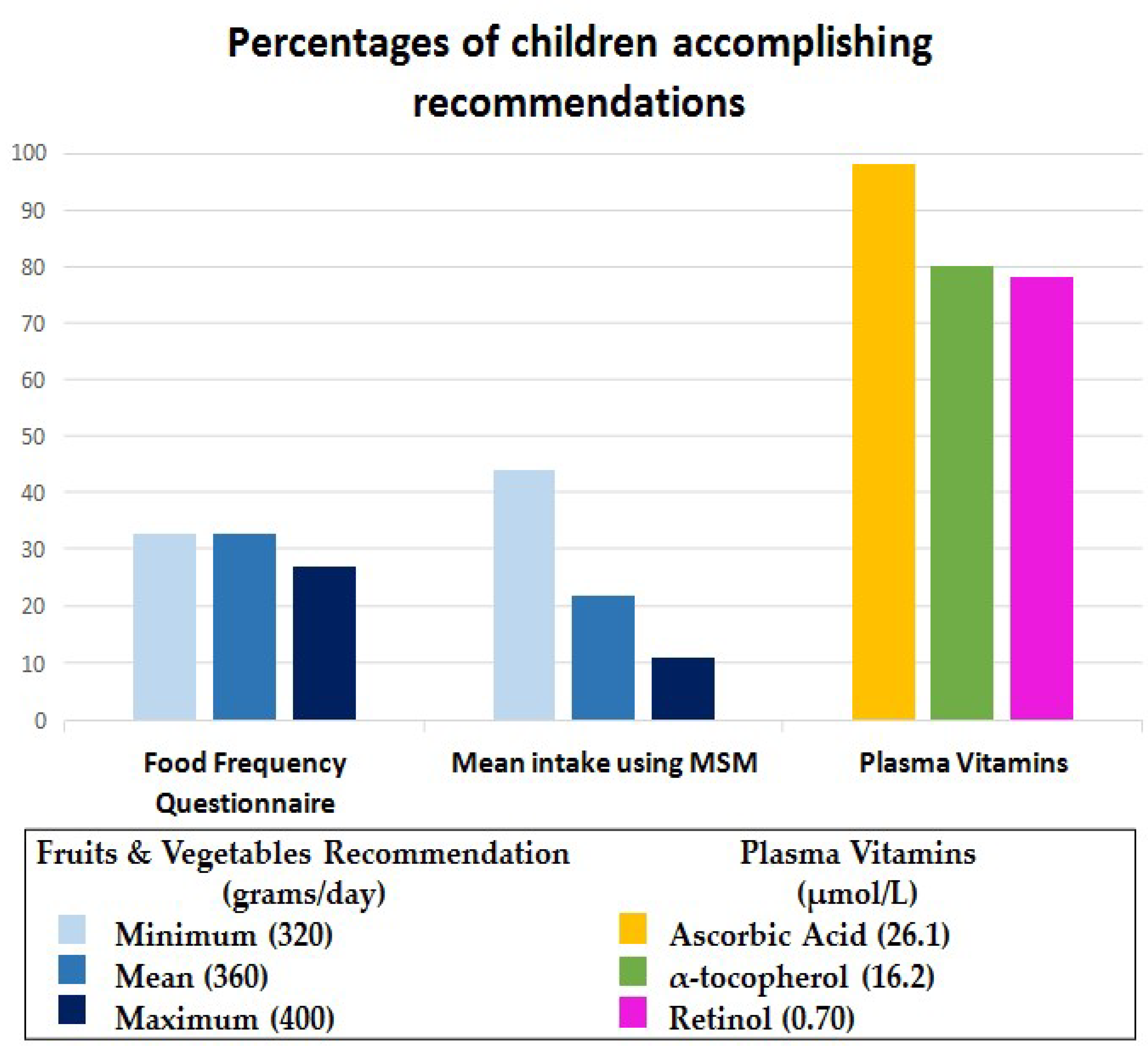
4.2. Fruit and Vegetable Intake
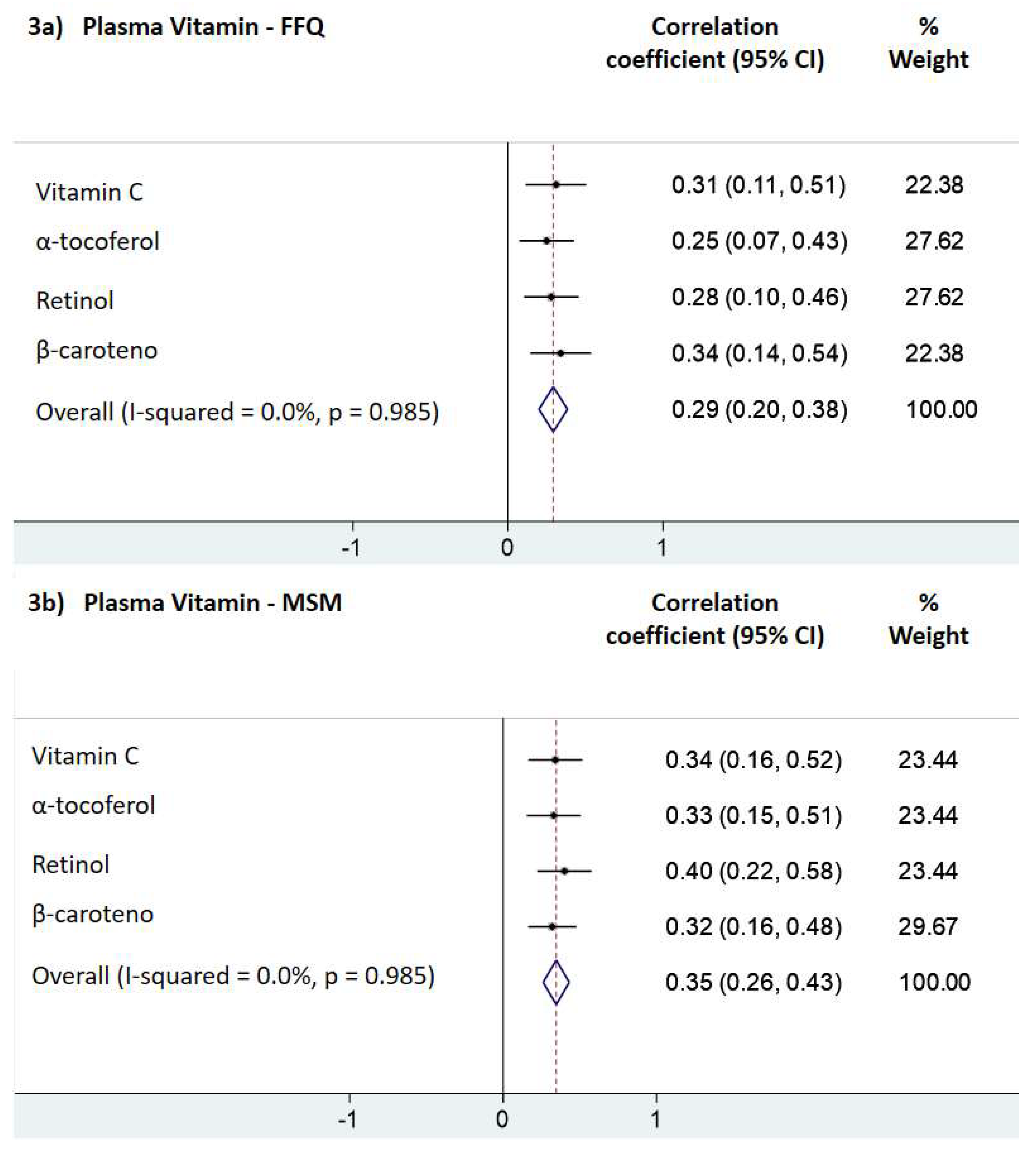
4.3. Correlation Coefficients
4.4. Accuracy of Dietary Assessment Methods
5. Discussion
5.1. Schoolchildren
5.2. Subjective Dietary Assessment Methods
5.3. Combination of Biomarkers
5.4. Accuracy of Dietary Assessment Methods
5.5. Adjustment for Confounders
5.6. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Steinberger, J.; Daniels, S.R.; Hagberg, N.; Isasi, C.R.; Kelly, A.S.; Lloyd-Jones, D.; Pate, R.R.; Pratt, C.; Shay, C.M.; Towbin, J.A.; et al. Cardiovascular Health Promotion in Children: Challenges and Opportunities for 2020 and Beyond: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e236–e255. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Reicks, M. Test-Retest Reliability and Convergent Validity of Two Brief Fruit and Vegetable Intake Questionnaires among School-Aged Children. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Collese, T.S.; Vatavuk-Serrati, G.; Nascimento-Ferreira, M.V.; De Moraes, A.C.F.; Carvalho, H.B. What is the Validity of Questionnaires Assessing Fruit and Vegetable Consumption in Children when Compared with Blood Biomarkers? A Meta-Analysis. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Van de Gaar, V.M.; Jansen, W.; van der Kleij, M.J.; Raat, H. Do children report differently from their parents and from observed data? Cross-sectional data on fruit, water, sugar-sweetened beverages and break-time foods. BMC Public Health 2016, 16, 341. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, A.E.; Tabak, R.G.; Bryant, M.J.; Ward, D.S. Measuring parent food practices: A systematic review of existing measures and examination of instruments. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Stage, V.C.; Downing, C.; Hegde, A.V.; Dev, D.A.; Peterson, A.D.; Goodell, L.S. Comparison of Parent and Child Ratings of Fruit and Vegetable Liking to Assess Parent Accuracy as Proxy Reporters. Ecol. Food Nutr. 2019, 58, 166–186. [Google Scholar] [CrossRef] [Green Version]
- Willet, W. Chap 6—Reproducibility and Validity of Food Frequency Questionnaires. In Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Gleason, P.M.; Harris, J.; Sheean, P.M.; Boushey, C.J.; Bruemmer, B. Publishing nutrition research: Validity, reliability, and diagnostic test assessment in nutrition-related research. J. Am. Diet. Assoc. 2010, 110, 409–419. [Google Scholar] [CrossRef]
- Satija, A.; Stampfer, M.J.; Rimm, E.B.; Willett, W.; Hu, F.B. Perspective: Are Large, Simple Trials the Solution for Nutrition Research? Adv. Nutr. 2018, 9, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Corella, D.; Ordovas, J.M. Biomarkers: Background, classification and guidelines for applications in nutritional epidemiology. Nutr. Hosp. 2015, 31 (Suppl. 3), 177–188. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A.; Russell, R.M.; Stephensen, C.B.; Gannon, B.M.; Craft, N.E.; Haskell, M.J.; Lietz, G.; Schulze, K.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)-Vitamin A Review. J. Nutr. 2016, 146, 1816S–1848S. [Google Scholar] [CrossRef]
- Chun, J.; Lee, J.; Ye, L.; Exler, J.; Ronald, R.E. Tocopherol and tocotrienol contents of raw and processed fruits and vegetables in the United States diet. J. Food Compos. Anal. 2006, 19, 196–204. [Google Scholar] [CrossRef]
- Wilett, W. Chapter 8—Biochemical Indicators of Dietary Intake. In Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Dehghan, M.; Akhtar-Danesh, N.; McMillan, C.R.; Thabane, L. Is plasma vitamin C an appropriate biomarker of vitamin C intake? A systematic review and meta-analysis. Nutr. J. 2007, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Alimentos Regionais Brasileiros/Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica, 2nd ed.; Básica, A., Ed.; Ministério da Saúde: Brasília, Brasil, 2015.
- Satija, A.; Yu, E.; Willett, W.C.; Hu, F.B. Understanding nutritional epidemiology and its role in policy. Adv. Nutr. 2015, 6, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, H.B.; Moreno, L.A.; Silva, A.M.; Berg, G.; Estrada-Restrepo, A.; Gonzalez-Zapata, L.I.; De Miguel-Etayo, P.; Delgado, C.A.; Bove, M.I.; de Sousa, M.; et al. Design and Objectives of the South American Youth/Child Cardiovascular and Environmental (SAYCARE) Study. Obesity 2018, 26 (Suppl. 1), S5–S13. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Population Based Approaches to Childhood Obesity Prevention; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Saravia, L.; Gonzalez-Zapata, L.I.; Rendo-Urteaga, T.; Ramos, J.; Collese, T.S.; Bove, I.; Delgado, C.; Tello, F.; Iglesia, I.; Goncalves Sousa, E.D.; et al. Development of a Food Frequency Questionnaire for Assessing Dietary Intake in Children and Adolescents in South America. Obesity 2018, 26 (Suppl. 1), S31–S40. [Google Scholar] [CrossRef]
- Rendo-Urteaga, T.; Saravia, L.; Collese, T.S.; Tello, F.; Monsalve-Alvarez, J.; González-Zapata, L.; Martínez-Oliván, B.; Torres-Leal, F.; Moreno, L.; De Moraes, A.; et al. Reliability and validity of a food frequency questionnaire for South American children and adolescents from the SAYCARE study. Public Health Nutr. 2019, 206, 8. [Google Scholar] [CrossRef]
- Benzecry, E.H.; Pinheiro, A.B.V.; Lacerda, E.M.D.A.; Gomes, M.C.D.S.; Costa, V.M.D. Tabela Para Avaliação de Consumo Alimentar em Medidas Caseiras, 5th ed.; Atheneu: Rio de Janeiro, Brazil, 2005; p. 152. [Google Scholar]
- Núcleo de Estudos e Pesquisa em Alimentação. Tabela Brasileira de Composição de Alimentos (TACO), 4th ed.; Núcleo de Estudos e Pesquisa em Alimentação: Campinas, Brazil, 2011. [Google Scholar]
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S87–S91. [Google Scholar] [CrossRef]
- World Health Organization. Laboratory Quality Management System: Handbook; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Simundic, A.M.; Cornes, M.; Grankvist, K.; Lippi, G.; Nybo, M.; Kovalevskaya, S.; Sprongl, L.; Sumarac, Z.; Church, S. Survey of national guidelines, education and training on phlebotomy in 28 European countries: An original report by the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) working group for the preanalytical phase (WG-PA). Clin. Chem. Lab. Med. 2013, 51, 1585–1593. [Google Scholar] [CrossRef]
- Sociedade Brasileira de Análises Clínicas (SBAC). Consenso Brasileiro Para a Normatização da Determinação Laboratorial do Perfil Lipídico; SBAC: Rio de Janeiro, Brazil, 2016. [Google Scholar]
- Brasil, A.R.; Norton, R.C.; Rossetti, M.B.; Leão, E.; Mendes, R.P. Proteína C reativa como indicador de inflamação de baixa intensidade em crianças e adolescentes com e sem obesidade. J. Pediatr. 2007, 83, 477–480. [Google Scholar] [CrossRef]
- Woodside, J.V.; Draper, J.; Lloyd, A.; McKinley, M.C. Use of biomarkers to assess fruit and vegetable intake. Proc. Nutr. Soc. 2017, 76, 308–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnaud, J.; Fortis, I.; Blachier, S.; Kia, D.; Favier, A. Simultaneous determination of retinol, alpha-tocopherol and beta-carotene in serum by isocratic high-performance liquid chromatography. J. Chromatogr. 1991, 572, 103–116. [Google Scholar] [CrossRef]
- Robitaille, L.; Hoffer, L.J. A simple method for plasma total vitamin C analysis suitable for routine clinical laboratory use. Nutr. J. 2016, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Indicators for Assessing Vitamin a Deficiency and Their Application in Monitoring and Evaluating Intervention Programmes; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- Sauberlich, H.E. Laboratory Tests for the Assessment of Nutritional Status, 2nd ed.; CRC Press: Boca Raton, FL, USA, 1999. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Dou, P.; Ju, H.; Shang, J.; Li, X.; Xue, Q.; Xu, Y.; Guo, X. Application of receiver operating characteristic curve in the assessment of the value of body mass index, waist circumference and percentage of body fat in the Diagnosis of Polycystic Ovary Syndrome in childbearing women. J. Ovarian Res. 2016, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Prasad, M.; Takkinen, H.M.; Uusitalo, L.; Tapanainen, H.; Ovaskainen, M.L.; Alfthan, G.; Erlund, I.; Ahonen, S.; Akerlund, M.; Toppari, J.; et al. Carotenoid Intake and Serum Concentration in Young Finnish Children and Their Relation with Fruit and Vegetable Consumption. Nutrients 2018, 10. [Google Scholar] [CrossRef]
- Vandevijvere, S.; Geelen, A.; Gonzalez-Gross, M.; van’t Veer, P.; Dallongeville, J.; Mouratidou, T.; Dekkers, A.; Bornhorst, C.; Breidenassel, C.; Crispim, S.P.; et al. Evaluation of food and nutrient intake assessment using concentration biomarkers in European adolescents from the Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2013, 109, 736–747. [Google Scholar] [CrossRef]
- Brouwer-Brolsma, E.M.; Brennan, L.; Drevon, C.A.; van Kranen, H.; Manach, C.; Dragsted, L.O.; Roche, H.M.; Andres-Lacueva, C.; Bakker, S.J.L.; Bouwman, J.; et al. Combining traditional dietary assessment methods with novel metabolomics techniques: Present efforts by the Food Biomarker Alliance. Proc. Nutr. Soc. 2017, 76, 619–627. [Google Scholar] [CrossRef]
- Fisberg, R.M.; Sales, C.H.; Fontanelli, M.M.; Pereira, J.L.; Alves, M.; Escuder, M.M.L.; Cesar, C.L.G.; Goldbaum, M. 2015 Health Survey of Sao Paulo with Focus in Nutrition: Rationale, Design, and Procedures. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Inhulsen, M.M.; Merelle, S.Y.; Renders, C.M. Parental feeding styles, young children’s fruit, vegetable, water and sugar-sweetened beverage consumption, and the moderating role of maternal education and ethnic background. Public Health Nutr. 2017, 20, 2124–2133. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E. Nutritional epidemiology: Forest, trees and leaves. Eur. J. Epidemiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Fisberg, R.M.; Marchioni, D.M.; Colucci, A.C. Assessment of food consumption and nutrient intake in clinical practice. Arq. Bras. Endocrinol. Metabol. 2009, 53, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Midthune, D.; Arab, L.; Prentice, R.L.; Subar, A.F.; Willett, W.; Neuhouser, M.L.; Tinker, L.F.; Kipnis, V. Combining a Food Frequency Questionnaire with 24-Hour Recalls to Increase the Precision of Estimation of Usual Dietary Intakes-Evidence From the Validation Studies Pooling Project. Am. J. Epidemiol. 2018, 187, 2227–2232. [Google Scholar] [CrossRef]
- McGrath, A.J.; Hamill, L.L.; Cardwell, C.R.; Draffin, C.R.; Neville, C.E.; Appleton, K.M.; McEneny, J.; McKinley, M.C.; Young, I.S.; Woodside, J.V. Combining vitamin C and carotenoid biomarkers better predicts fruit and vegetable intake than individual biomarkers in dietary intervention studies. Eur. J. Nutr. 2016, 55, 1377–1388. [Google Scholar] [CrossRef]
- Burrows, T.L.; Warren, J.M.; Colyvas, K.; Garg, M.L.; Collins, C.E. Validation of overweight children’s fruit and vegetable intake using plasma carotenoids. Obesity 2009, 17, 162–168. [Google Scholar] [CrossRef]
- Royo-Bordonada, M.A.; Gorgojo, L.; Ortega, H.; Martin-Moreno, J.M.; Lasuncion, M.A.; Garces, C.; Gil, A.; Rodriguez-Artalejo, F.; de Oya, M. Greater dietary variety is associated with better biochemical nutritional status in Spanish children: The Four Provinces Study. Nutr. Metab. Cardiovasc. Dis. 2003, 13, 357–364. [Google Scholar] [CrossRef]
- USDA; Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. Chapter 2. Shifts Needed to Align with Healthy Eating Patterns. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 4 July 2019).
- Giovannucci, E. Nutrient biomarkers are not always simple markers of nutrient intake. Am. J. Clin. Nutr. 2013, 97, 657–659. [Google Scholar] [CrossRef]
- Russell, R.; Chung, M.; Balk, E.M.; Atkinson, S.; Giovannucci, E.L.; Ip, S.; Lichtenstein, A.H.; Mayne, S.T.; Raman, G.; Ross, A.C.; et al. Opportunities and challenges in conducting systematic reviews to support the development of nutrient reference values: Vitamin A as an example. Am. J. Clin. Nutr. 2009, 89, 728–733. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | % or Mean | (95% CI) | |
|---|---|---|---|
| Sex (n = 45) | |||
| Female | 24 | 53.3 | (38.3–67.8) |
| Male | 21 | 46.7 | (32.2–61.7) |
| Age in years (n = 45) | 8.3 | (7.9–8.6) | |
| Body Mass Index (kg/m2) * (n = 45) | |||
| Underweight | 1 | 2.2 | (0.3–15.1) |
| Healthy weight | 29 | 64.4 | (49.0–77.4) |
| Overweight | 10 | 22.2 | (12.1–37.2) |
| Obesity | 5 | 11.1 | (4.5–24.7) |
| Waist Circumference (cm) (n = 45) | 62.1 | (59.0–65.3) | |
| Total Cholesterol (n = 45) ** | |||
| Healthy (<170 mg/dL) | 34 | 75.6 | (60.4–86.2) |
| High (>170 mg/dL) | 11 | 24.4 | (13.8–39.6) |
| C-reactive protein (mg/dL) (n = 45) | 0.8 | (0.4–1.2) | |
| School (n = 45) | |||
| Public | 24 | 46.7 | (32.2–61.7) |
| Private | 21 | 53.3 | (38.3–7.8) |
| Maternal Education Level (n = 32) ! | |||
| Incomplete high school | 3 | 9.4 | (2.9–26.7) |
| High school | 12 | 37.5 | (22.0–56.1) |
| Technical | 1 | 3.1 | (0.4–20.9) |
| University degree | 16 | 50.0 | (32.5–67.5) |
| Total | Public School | Private School | ||||
|---|---|---|---|---|---|---|
| n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | |
| Fruit and Vegetable Intake (grams/day) | ||||||
| FFQ | 45 | 261.2 (195.1–327.3) | 21 | 225.9 (139.4–312.4) | 24 | 292.1 (189.5–394.7) |
| Mean intake using MSM | 45 | 301.7 (277.2–326.2) | 21 | 309.0 (278.1–340.0) | 24 | 295.3 (256.2–334.4) |
| Plasma Vitamins (μmol/L) | ||||||
| Ascorbic Acid | 45 | 80.9 (66.5–95.4) | 21 | 78.8 (64.9–92.8) | 24 | 82.8 (57.5–108.1) |
| α-tocopherol | 45 | 21.8 (20.2–23.3) | 21 | 21.1 (18.3–23.9) | 24 | 22.3 (20.5–24.1) |
| Retinol | 45 | 0.94 (0.84–1.03) | 21 | 0.88 (0.76–1.0) | 24 | 0.98 (0.84–1.12) |
| β-carotene | 45 | 0.32 (0.26–0.39) | 21 | 0.31 (0.24–0.39) | 24 | 0.33 (0.23–0.44) |
| Fruits and Vegetables Daily Intake | Plasma Vitamins | |||
|---|---|---|---|---|
| Ascorbic Acid | α-Tocopherol | Retinol | Sum of Vitamins (≥2 Points) | |
| FFQ, accuracy (%) | ||||
| Continuous | 47.7 | 51.5 | 64.2 | - |
| Minimum (320 g/day) | 67.1 | 50.0 | 62.7 | 67.9 |
| Mean (360 g/day) | 67.1 | 50.0 | 62.7 | 67.9 |
| Maximum (400 g/day) | 63.6 | 52.8 | 58.6 | 64.3 |
| Mean intake using MSM, accuracy (%) | ||||
| Continuous | 65.9 | 71.3 | 30.1 | - |
| Minimum (320 g/day) | 72.7 | 56.9 | 31.4 | 56.0 |
| Mean (360 g/day) | 61.4 | 63.9 | 33.1 | 61.9 |
| Maximum (400 g/day) | 55.7 | 56.9 | 34.0 | 56.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collese, T.S.; De Moraes, A.C.F.; Rendo-Urteaga, T.; Luzia, L.A.; Rondó, P.H.d.C.; Marchioni, D.M.L.; Carvalho, H.B. The Validity of Children’s Fruit and Vegetable Intake Using Plasma Vitamins A, C, and E: The SAYCARE Study. Nutrients 2019, 11, 1815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081815
Collese TS, De Moraes ACF, Rendo-Urteaga T, Luzia LA, Rondó PHdC, Marchioni DML, Carvalho HB. The Validity of Children’s Fruit and Vegetable Intake Using Plasma Vitamins A, C, and E: The SAYCARE Study. Nutrients. 2019; 11(8):1815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081815
Chicago/Turabian StyleCollese, Tatiana Sadalla, Augusto César Ferreira De Moraes, Tara Rendo-Urteaga, Liania Alves Luzia, Patrícia Helen de Carvalho Rondó, Dirce Maria Lobo Marchioni, and Heráclito Barbosa Carvalho. 2019. "The Validity of Children’s Fruit and Vegetable Intake Using Plasma Vitamins A, C, and E: The SAYCARE Study" Nutrients 11, no. 8: 1815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081815