Ketoacid Analogues Supplementation in Chronic Kidney Disease and Future Perspectives


1
Department of Nephrology, Hospices Civils de Lyon, Centre Hospitalier Lyon-Sud, F-69495 Pierre-Bénite, France
2
Univ Lyon, CarMeN Laboratory, INSA-Lyon, Inserm U1060, INRA, Université Claude Bernard Lyon 1, F-69621 Villeurbanne, France
3
Department of Medical Clinic, Botucatu Medical School, Universidade Estadual Paulista—UNESP, Botucatu 18618-687, Brazil
*
Author to whom correspondence should be addressed.
Nutrients 2019, 11(9), 2071; https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092071
Submission received: 11 July 2019
/
Revised: 22 August 2019
/
Accepted: 26 August 2019
/
Published: 3 September 2019
(This article belongs to the Special Issue Targeted Nutrition in Chronic Disease)
Abstract
:Diet is a key component of care during chronic kidney disease (CKD). Nutritional interventions, and, specifically, a restricted protein diet has been under debate for decades. In order to reduce the risk of nutritional disorders in very-low protein diets (VLDP), supplementation by nitrogen-free ketoacid analogues (KAs) have been proposed. The aim of this review is to summarize the potential effects of this dietary therapy on renal function, uremic toxins levels, and nutritional and metabolic parameters and propose future directions. The purpose of this paper is also to select all experimental and randomized clinical studies (RCTs) that have compared VLDP + KA to normal diet or/and low protein diet (LPD). We reviewed the SCOPUS, WEB of SCIENCES, CENTRAL, and PUBMED databases from their inception to 1 January, 2019. Following duplicate removal and application of exclusion criteria, 23 RCTs and 12 experimental studies were included. LPD/VLPD + KAs appear nutritionally safe even if how muscle protein metabolism adapts to an LPD/VLPD + KAs is still largely unknown. VLPD + KAs seem to reduce uremic toxins production but the impact on intestinal microbiota remains unexplored. All studies observed a reduction of acidosis, phosphorus, and possibly sodium intake, while still providing adequate calcium intake. The impact of this diet on carbohydrate and bone parameters are only preliminary and need to be confirmed with RCTs. The Modification of Diet in Renal Disease study, the largest RCTs, failed to demonstrate a benefit in the primary outcome of the decline rate for the glomerular filtration rate. However, the design of this study was challenged and data were subsequently reanalyzed. However, when adherent patients were selected, with a rapid rate of progression and a long-term follow up, more recent meta-analysis and RCTs suggest that these diets can reduce the loss of the glomerular filtration rate in addition to the beneficial effects of renin-angiotensin-aldosterone system (RAAS) inhibitors. The current evidence suggests that KAs supplemented LPD diets should be included as part of the clinical recommendations for both the nutritional prevention and metabolic management of CKD. More research is needed to examine the effectiveness of KAs especially on uremic toxins. A reflection about the dose and composition of the KAs supplement, the cost-effective features, and their indication to reduce the frequency of dialysis needs to be completed.
1. Introduction
End-stage kidney disease (ESKD) is a condition associated with a high mortality and poor quality of life combined with extremely high costs. Using interventions for delaying the need to start a kidney replacement treatment is, therefore, a major challenge. Experimentally, Brenner et al. [1] showed that high protein intake induced marked kidney hypertrophy, which is an increase in glomerular pressure and hyperfiltration that negatively impacts kidney function. Chronic kidney disease (CKD) is characterized by the accumulation of a number of organic solutes called uremic toxins. Many of these uremic toxins are produced by the degradation of dietary amino acids by intestinal microbiota and appears to accelerate CKD progression. Based on these observations, a reduction in protein intake can be expected to preserve renal function and reduce uremic toxicity. The main limitation of this diet is the risk of malnutrition and cachexia.
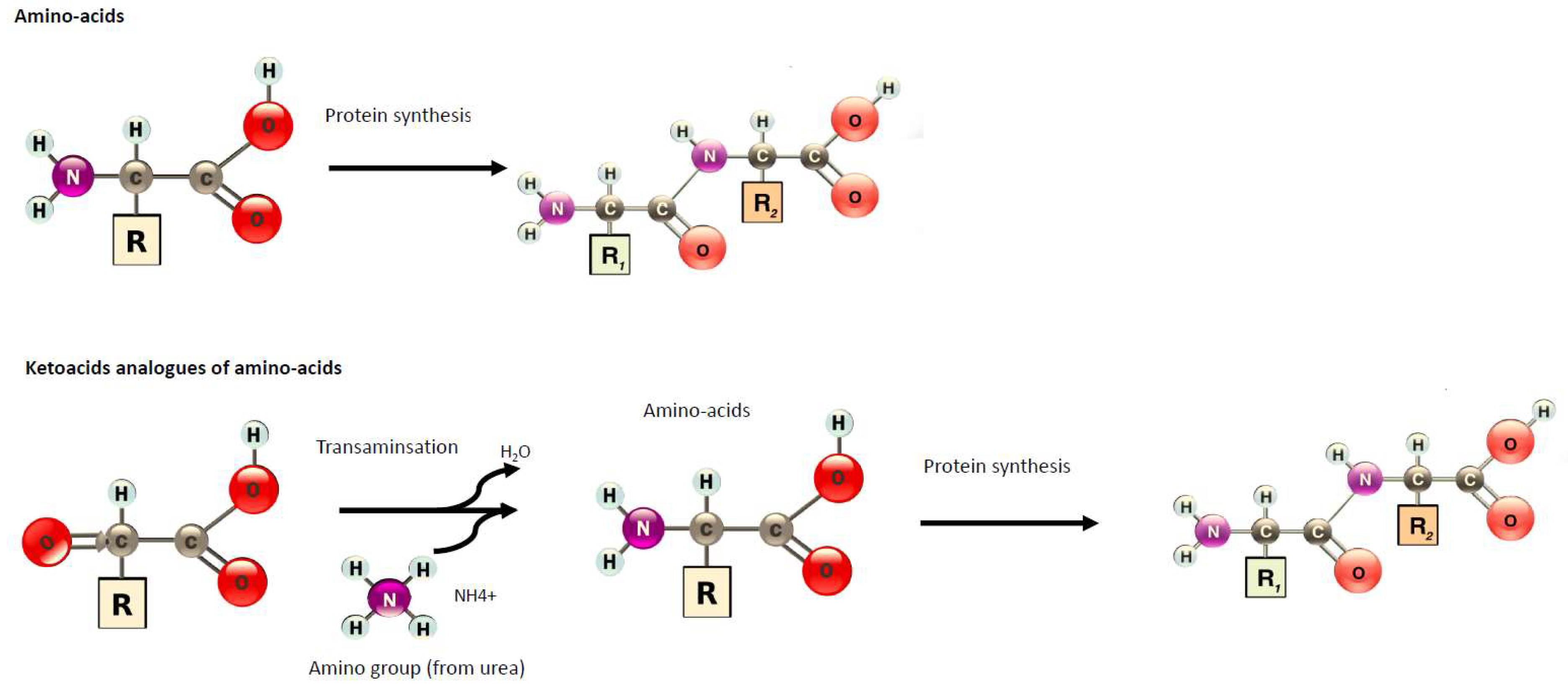
Different dietary protein regimens have been tested: low–protein diets (LPD, 0.6 g protein/kg/day) or very low–protein diets (VLPD: 0.3–0.4 g protein/kg/day) supplemented with essential amino acids (EAAs) or nitrogen-free ketoacid analogues (KAs). KAs are precursors of corresponding amino acids since they can undergo a transamination, e.g., a chemical reaction that transfers an amino group to a ketoacid to form a new amino acid (Figure 1). This pathway is responsible for the deamination of most amino acids. Through this conversion, KAs can be utilized in place of their respective EAAs without providing nitrogen products while re-using available nitrogen already in excess during CKD. If a diet does not provide enough EAAs or calories, then the nitrogen balance can become negative and could partly induce cachexia. Therefore, administration of KAs has been proposed to improve protein status while limiting the nitrogen burden on the body. VLDP + KAs are likely also efficient because the calcium content of KA preparation could allow a better correction of mineral metabolism impairment. Different compositions of KAs and EAAs have been tested, with most of them containing four KAs (of the EAA isoleucine, leucine, phenylalanine, and valine), one hydroxyacid (of the EAA methionine), and four amino acids considered essential in CKD (tryptophan, threonine, histidine, and tyrosine) (Table 1).
Since the publication of the perspective by Shah et al. [2] on the role of KA supplementation in the management of CKD, great effort was undertaken to perform randomized controlled trials (RCTs). This review outlines the potential mechanisms of action and efficacy of KAs in renal function and metabolic parameters with a particular emphasis on potential anabolic effects and reduction of uremic toxins production. Our review mainly focuses on recent experimental data and RCTs. Lastly, we propose new fields of investigation for KAs in future research.
2. Methods
We performed a literature search of trials in SCOPUS, WEB of SCIENCES, CENTRAL, and PUBMED databases from their inception to 1 January, 2019 initially without a language restriction. The search strategy used the terms renal or ESRD or end stage renal disease or kidney or CKD or chronic kidney disease and ketoacids or keto analogs or very low protein diet. Titles and abstracts of publications returned from the search were screened for relevance by three authors (L.K., M.C.d.O., and D.F). Clinical studies were included if (i) full text was available in English, (ii) focused on a randomized controlled trial, and (iii) investigated the effect of KAs in non-dialysis CKD patients of any age. Abstracts, case reports, narrative reviews, editorials, letters, and practice guidelines were excluded. We identified 13,132 potentially relevant references from the search (12,453 records without duplicates, Supplementary Figure S1). After title and abstract screening, 140 full-text articles were considered for inclusion. Twenty-three full-text studies were selected in order to analyze the potential effects of KAs. For experimental studies, we performed a literature search on the PubMed database from inception to 1 January, 2019. We only kept experimental studies, which used a control group.
3. Potential Benefit of Ketoacid Analogues
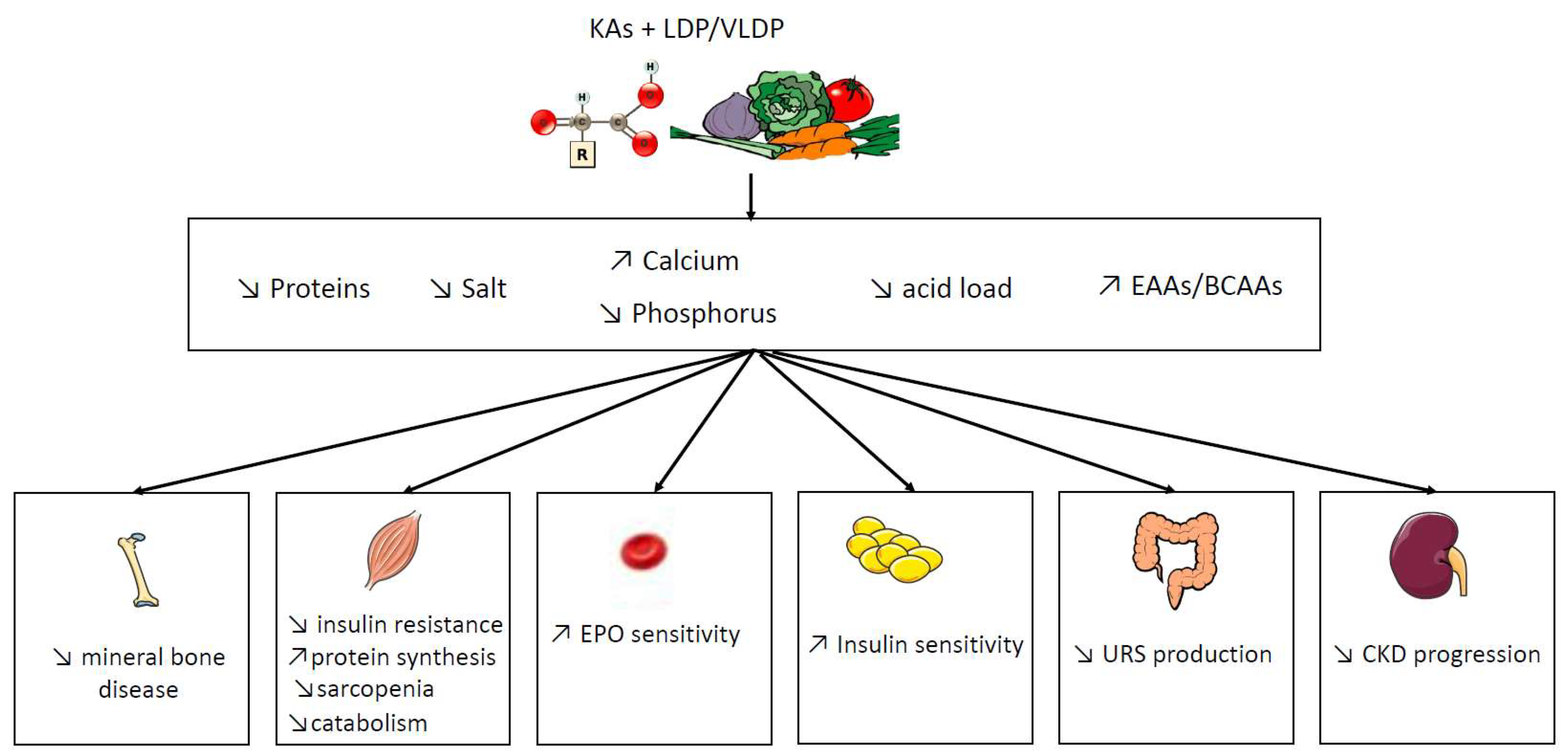
Do we have evidence in CKD of specific KAs actions on the reduction of kidney disease-associated comorbidity? New emerging studies suggest that restricted VLDP + KAs may improve renal function and nutritional status, while preventing hyperparathyroidism, insulin resistance, and accumulation of uremic retention solutes (URS), as summarized in Figure 2. The main concern about the interpretation of the literature is the fact that KAs are not given solely but in association with other EAAs and under LPD/VLPD condition. In particular, we do not know if a supplementation of KA alone without low protein diets has any benefit on metabolic disturbances related to CKD. Few studies [3,4,5,6,7] compared KAs supplementation with the same protein restriction and it is difficult to decipher if “KAs effects” are solely the consequence of a decrease of protein intake or if they act specifically. Another interrogation is the reproducibility of the diet composition in different groups. The composition of fibers, acid load, or sodium is difficult to assess and frequently not specified in dietary surveys, which can influence the results. In order to have a more detailed picture of the effects of KAs during CKD, the main experimental trials and RCTs have been summarized in Table 2 and Table 3.
3.1. Anabolic Action of Ketoacid Analogues
CKD is associated with muscular wasting and there are some concerns about potential catabolic and cachectic effects of LPD/VLPD. Muscle is an adaptive tissue that responds to diet, exercise, and hormones, which may impact protein metabolism. KAs in general and ketoleucine, in particular, have been shown to reduce muscle protein degradation [39]. However, how muscle protein metabolism adapts to a LPD/VLPD + KAs in CKD is still an open question. Leucine kinetics studies have shown that adaptation to dietary protein restriction involves a reduction in leucine flux and oxidation, which leads to a more efficient use of dietary amino acids, and postprandial inhibition of protein degradation with a reduced ureagenesis. These results were similar in CKD patients with an LPD [40] and with a VLPD + KAs [39,41,42]. This reduction in amino acid oxidation during VLPD + KAs persisted during a 16-month follow-up [43].
In addition, in animal models, KAs supplementation may play a protective role on muscle atrophy [8,11,12]. In particular, in 5/6th nephrectomy rats, an LPD + KAs compared to an LPD alone was able to suppress ubiquitin-proteasome system activation and protected skeletal muscle from atrophy and from oxidative damage. KAs can prevent a decrease in the activity of the mitochondrial electron transport chain complex and increase mitochondrial respiration [8,12]. LPD + KAs decreases autophagy markers in muscle, but there was no difference in inflammation in skeletal muscle [11]. It should be noted that the anabolic effect of KAs can be partially explained by the reduction of acid load associated with the reduction in protein intake.
3.2. Role of Ketoacid Analogues in Intestinal Metabolism and Uremic Toxins Production
The uremic syndrome is attributed to the progressive retention of a large number of compounds called uremic retention solutes (URS). Protein bound uremic toxins derived from gut microbiota have emerged as a major class of URS. High levels of indoxyl sulfate (IS) (indol metabolites), p-cresyl sulfate (PCS) (p-cresol metabolite), and trimethylamine-N-oxide (TMAO) have been associated with an increase in cardiovascular risk and renal disease progression [44]. CKD as well as food intake have a deep influence on gut microbiota composition with an increase of pathobionts [45] and recent data have highlighted that modulation of intestinal microbiota appears to be an attractive strategy to reduce URS production [44]. There are some interrogations about the fact that KAs contained a rather large amount of tryptophan/tyrosine, which may have generated more URS. One clinical trial reported that a VLPD + KAs reduced IS serum levels in non-dialyzed CKD patients [23]. The reduction of URS may be explained by the reduction of protein intake and vegetarian diet since Marzocco et al. observed that the higher protein intake (observed during LPD compared to VLPD) was the major determinant of IS levels [23]. In addition, Teplan et al. were able to see a decrease in asymmetric dimethylarginine (another URS) with the same protein intake [4]. Until now, no large RCT has been performed to test the effectiveness of KAs strategy at reducing URS and this is eagerly needed.
The impact of intestinal function and intestinal microbiota with the presence of LPD/VLPD + KAs is unknown. Previous data suggest that the intestinal absorption of KAs is unaffected by CKD [46]. Recently, using modern mass spectrometry in germ-free mice, the serum concentration of BCAAs was shown to be reduced whereas their fecal concentration was increased. This suggests that these amino acids are less absorbed by the colonic mucosa but are intensely metabolized by the colonic microbiota instead. Therefore, the impact of KAs supplementation on gut microbiota in a uremic condition must be considered and explored.
One constant effect of VLPD/LPD + KAs treatment is the reduction of serum urea. Initially, it was thought that an important quantity of urea was hydrolyzed during CKD and the amino-group released from urea could aminate KAs and form new AAs. Studies indicate that the reduction in net urea generation with LPD + KA is due to decreased amino acid degradation [41,42]. The view that urea is simply a marker of renal dysfunction has been challenged by recent publications [47]. The microbial enzyme urease issued from the gut microbiota hydrolyzes urea and locally produces excessive amounts of ammonia [48]. Urea and ammonia in the intestinal gut could influence the gut microbiota composition, URS production, and disrupt the intestinal barrier, which is involved in the pathogenesis of inflammation in CKD [48]. At disease-relevant concentrations, urea induces reactive oxygen species (ROS) production and causes insulin resistance [49] and beta-cell dysfunction [47] by modifying insulin signaling molecules by O-linked β-N-acetylglucosamine. In addition, urea is able to contribute to posttranslational modification of proteins via the breakdown product cyanate through a process called protein carbamylation, which promotes atherosclerosis and mortality during CKD [50]. In good agreement, in a recent RCT including 60 CKD patients, the VLPD + KAs compared to a moderate protein diet (0.7 g/kg/day) significantly decrease serum urea levels and was associated with a reduced protein carbamylation [20].
3.3. Other Roles of Ketoacid Analogues
KA supplements have been associated with an improved bone metabolism, insulin sensitivity, and a decrease in blood pressure. Serum bicarbonate also increased. However, the reduction in protein intake and vegetarian diet induce a similar phenotype [51]. Therefore, the specific role of KAs on these parameters is not clear and more studies are needed.
In a large observational study performed by Bellizzi et al. [52], patients who received LDP + KAs had better blood pressure. In fact, there was a correlation between salt intake and blood pressure since salt intake is reduced by the LPD. In a recent RCT, Milovanova et al. reported that LPD + KAs improve blood pressure when compared to the control group with a similar salt and protein intake (0.6 g/kg/day) [3]. These observed hemodynamic effects could be due to the reduction in salt intake and possibly to an additional vasodilating effect of BCAAs-KAs supplementation.
KAs are synthesized as a calcium salt and daily provide an amount of 600 mg of calcium for a person of 60 kg. Therefore, calcium salt may exert a direct alkaline effect and phosphorus binding. This effect is likely amplified by a vegetarian diet. It is well-known that fruits and vegetable are an effective intervention to correct metabolic acidosis [53,54]. However, Gennari et al. reported no effect of diet on serum total CO2 in patients receiving a VLPD + KAs. The increase in serum bicarbonate was related to the decrease in protein intake [27]. However, in a recent RCT with a comparable protein intake, KAs were able to directly increase serum bicarbonate [3]. VLPD + KAs induce a reduction in serum phosphorus only one week after initiation of treatment and this was sufficient to reduce serum FGF23 levels [22]. In a longer six-month study, VLPD + KAs was efficient to improve mineral metabolism [20]. Lineadeau et al. [37] observed an improvement in osteo-fibrotic as well as osteo-malacic changes on bone biopsies after 12 months of treatment with Kas. This fact is independent of calcium intake. Indeed, the control group was supplemented in a comparable amount of calcium than the KAs group. By contrast, Bernhard et al. [6] observed no difference on calcium, phosphorus, and serum bicarbonate in a study where all groups receive calcium and bicarbonate supplementation.
Disorders of glucose homeostasis affect approximately 50% of patients suffering from CKD [55,56], which play a major role in mortality [57]. Pilot clinical studies demonstrated a potential impact of VLPD + KAs compared to an LPD on insulin sensitivity in severe CKD patients [58,59]. However, an LPD is able to improve insulin sensitivity and it is difficult to decipher if KAs have an additive effect [60]. More recently, Teplan et al. have highlighted that, with a similar protein intake, KAs supplementation was able to decrease glycated hemoglobin and visceral body fat, and improve lipid metabolism [4].
Lastly, Di Iorio et al. reported that a VLPD+ KAs diet allowed for a long-lasting reduction of the erythropoietin (EPO) dose required to maintain serum hemoglobin. In this study, the variation of EPO dose directly correlated with the improvement in parathyroid hormone levels. This suggests that the effect of KAs on anemia control was related to the control of phosphorus metabolism [31].
We strongly suggest that such research should be continued to better understand the mechanisms involved during KAs diets. Better knowledge on the interaction between protein intake, gut microbiota, and URS production offers new ways to analyze the mechanisms of action of KAs and increase the motivation of physicians, dietitians, and patients for implementing this diet.
4. Do Ketoacid Analogues Have an Impact on Renal Function and Mortality in CKD?
The beneficial role of KAs supplementation on renal function is well established in experimental models, but the effects are different in human clinical trials. LPD/VLPD + KAs were able to decrease proteinuria, renal fibrosis, and severe glomerular sclerosis in different CKD rodent models, as disclosed in Table 2 [9,10,13,14,15,17,18,19]. However, the majority of these preclinical studies have compared a normal protein diet vs. VLPD/LPD + KAs. It is, therefore, difficult to decipher the specific effect of the KAs supplementation [9,10,15,17,18,19]. Gao et al. highlighted that supplementation of KAs increased the Kruppel-like factor-15, which is a transcription factor shown to reduce fibrosis in 5/6 nephrectomized rats [14]. In this study, rats under LPD + KA had 1% less protein in their diet than rats under LPD but this was likely not sufficient to explain the improvement in renal function. To demonstrate specific effects of KAs, Zhang et al. [10] reported that mesangial cells treated with serum derived from 3/4 nephrectomized rats rapidly expressed higher expression of Angiotensin II and Angiotensin I receptors compared to a serum obtained from sham rats. Serum from CKD rats fed LPD significantly inhibited these abnormalities and this effect was even more pronounced with serum from CKD rats fed with LPD + KAs, which suggests that KAs may be directly involved or respond to the greater decrease in protein intake. This is a fact that limited the deleterious activation of renin-angiotensin system.
The interpretation of literature about the clinical efficacy of KAs seems controversial and depends on the chosen inclusion criteria. A recent meta-analysis (n = 10 RCT, 1010 patients in CKD stage 4) in non-diabetic CKD patients including the large positive study from Garneata et al. [21] and Milovanova et al. [3] showed that VLPD reduced the number of patients reaching ESRD [61]. Another recent meta-analysis with 661 patients, VLDP + KA significantly reversed the decrease of eGFR (mean difference = 2.74, 95% confidence interval = (0.73, 4.75), p = 0.008) in CKD patients [62]. It should be noted that, in the majority of these studies, protein intake was different between groups and the selection of studies is questionable, which makes it difficult to interpret the true role of KAs.
The vast majority of RCTs testing VLPD + KAs reported a decrease in proteinuria. In the large MDRD study, patients with proteinuria >3 g/24 h were more protected against CKD progression with VLPD + KAs [35]. Garneata et al. did not observe a beneficial effect on proteinuria of a VLPD + KAs. However, proteinuria was low in that particular study (<1 g/24 h) [21]. By contrast, in patients with a proteinuria >1 g/24 h, a VLPD + KAs was able to significantly decrease proteinuria [20,52,63,64]. It could be suggested that the anti-proteinuric effect of KAs is more important in patients with a higher proteinuria.
Until now, there is no evidence that LPD/VLPD + KAs have an impact on patients’ survival. A post hoc analysis of the MDRD study demonstrated a slightly increased mortality rate in the VLPD + KAs group after 10 years of study completion (1.95: 95% CI; 1.15–3.20) [25]. However, in this study, the diet adherence was not followed after the termination of the study, and there was no information on the clinical survey and treatments of the patients. The Bellizzi’ historical cohort with approximately 200 patients followed up for more than 10 years did not show adverse effects and suggested possible greater survival [65]. Mortality of patients consuming VLPD + KAs was 8% patients/year, while, in the control group, it was 10% [65]. In another long-term observational study (>10 year), Chauveau et al. did not observe a correlation between the death rate and duration of diet [66]. In recent RCTs, no difference in death or cardiovascular events was observed [3,21]. It should be noted that these studies were not designed to answer this question and larger RCTs are recommended.
5. Is a Keto Acid Analogues Supplementation a Modern Treatment?
There is some evidence about potential benefits of LPD/VLPD + KAs on renal outcomes but the effects seem small and this questions its generalization compared to modern treatments such as renin-angiotensin-aldosterone system (RAAS) inhibitors. In a recent review [67], we reported that there was no clinical evidence for synergistic effects of the RAAS inhibitor and LPD. Experimental and clinical studies evaluating the additive effect of an LPD and RAAS inhibition are few, of low quality and limited duration, and only demonstrate significant beneficial effects on proteinuria. The recent study by Garneata et al. in which 71% of participants were receiving an RAAS inhibitory treatment, showed that the probability of worsening kidney function or need for dialysis was lower in the VLPD + KAs group when adjusted for RAAS inhibitors (hazard ratio, 0.10, 95% CI, 0.05-0.20) [21]. Bellizi et al. studied 45% of patients who were under RAAS inhibition and observed a 35% decrease in proteinuria under an LPD and KA combination compared to a normal diet (vs. −1% in the free diet group) [65]. However, in two recent RCTs, the use of RAAS inhibitors were not detailed or have low incidence [3,20].
The other major concern is a potential risk of malnutrition and kidney cachexia. The majority of studies confirmed the safety of VLPD + KAs. In experimental models, the addition of Kas to the LPD largely prevented the loss of weight and completely normalized serum albumin levels [13,14]. In the MDRD study, patients with protein restriction lost about 2 kg and showed a decrease in other anthropometric parameters during the first four months only, likely because of reduced energy intake. Biochemical and anthropometric indices of nutritional status were generally well within normal limits during follow-up and at the end of the MDRD study [35]. In all RCTs testing VLPD + KAs therapy with dietary management performed by trained dietitians reported no change in serum albumin [5,21,26,29,30,33,68], which is subjective to the global assessment score [21,68] or BMI [33]. In recent meta-analyses, Hahn et al. [61] have reported that, among four studies comparing nutritional measures with VLPD or LPD (n = 291), the mean final body weight was 1.4 kg higher with VLPD when compared to LPD. Therefore, the risk for wasting during VLPD is 0.6%. This is a magnitude that is not different from normal diets (0.4%). However, the specific role of Kas was not tested in this study [61]. Using whole-body DEXA in an observational study, patients with VLPD + KAs showed a significant decrease in lean tissue mass and an increase in total body fat. These different modifications occurred abruptly during the first three months, and then stabilized or slightly improved thereafter [69]. In another cohort, after at least two years, muscle strength increased in CKD diabetic patients under VLPD + KAs [70].
The routine use of VLPD + KAs in clinical practice remains challenging. Their benefits were mainly seen in patients who showed good compliance to an LPD. The study of Garneata et al. was the first study confirming this fact [21]. Only 14% of the screened patients were kept for the study and randomized, which underlines the limitation to propose this therapy to a larger number of patients. Similarly, with a less reduced protein intake, Milovanova et al. included 33% of the screened patients [3]. Overall, only 30% of the pre-selected patients correctly achieved a VLPD + KAs [71]. Zoccali et al. suggested that it is unrealistic to have, at a country level, about one-third of the whole workforce of dietitians entirely dedicated to the follow-up of CKD patients [72].
Another key question is whether LPD/VLPD + KAs is applicable to the elderly patients who presently dominate the CKD population but are less likely to be recruited into RCTs. Elderly patients have already spontaneous lower dietary protein intakes and are developing sarcopenia. Cognitive deficit may also challenge an effective and safe follow-up of such restricted diets. The RCT Diet or Dialysis in Elderly (DODE) trial, which included 112 patients [73], observed that VLPD + KAs was an efficient strategy to delay the need for dialysis. The interpretation of this study is not consensual and it seems that VLPD + KAs might have increased recurring episodes of fluid overload or hyperkalemia [74]. However, the mortality rate was not different between the two groups and the hospitalization rate was higher in the dialysis group.
If some preliminary data suggest that VLPD + KAs supplementation is interesting and safe in dialysis patients, after renal transplantation or during pregnancy in CKD women, further large studies are necessary [75,76]. Lastly, the best timing, e.g., the kidney disease stage to start a KA supplementation, has not been clearly defined.
A final question is: what are the optimal level and composition of KAs that are needed? One observational study showed that a low dose of KAs had a beneficial effect to slow down renal function deterioration in pre-dialysis patients [77]. Some studies suggest that amino acid like lysine supplementation may improve vascular calcification [78]. By contrast, tryptophan and tyrosine are precursors of URS and, therefore, may be deleterious. As mentioned above, the role of BCAA supplementation must also be clarified.
6. Conclusion
The results of this review support the beneficial effects of VLDP + KAs in CKD patients on renal function and different metabolic parameters in particular acidosis, insulin resistance, and bone metabolism without alteration of the nutritional status. However, evidence is inconclusive regarding the effect of VLDP + KA on mortality and cardiovascular events. The recommendation for the use of KAs has not reached consensus and remains a second-choice alternative. Few international and national societies currently recommend KAs supplementation in the management of CKD (Table 4).
7. Future Directions
The low adherence is a main caveat when prescribing VLPD + KAs. Ethnic and cultural dietary variations between CKD populations raise the question of whether the results of protein restriction trials are applicable on an international basis. Another limitation is the side effects of KAs. They can induce hypercalcemic episodes due to their calcium content and uncomfortable gastrointestinal symptoms. In a developing country without easy access of the medical resource, as compared with the maintenance dialysis expenses, the low cost of KAs may be an attractive alternative strategy. Considering an average yearly cost of about 34,072 € for dialysis and 1440 € for the diet, treating patients with VLDP + KA and delaying dialysis treatment would allow significant financial savings [85]. In Western countries, VLPD + KAs may be proposed as a possible tool to reduce CKD costs and postpone dialysis when waiting for fistula maturation or for a living kidney transplant. The personalized medicine is one of the emerging clinical models in the new millennium. Additionally, multiple choice regarding diet linked to patient characteristics may lead to better adherence [86]. Further studies are needed to identify factors that influence patient adherence. Incremental dialysis, which combines a nutritional-dialysis approach, may be an option for avoiding the abrupt start of thrice weekly hemodialysis and should be one of the possible new treatment options. Additionally, further research will be required to establish the optimal KAs dose and role of this diet on uremic toxin production.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/2072-6643/11/9/2071/s1. Figure S1: Identification process for randomized clinical studies.
Author Contributions
Writing—Review & Editing, L.K., M.C.d.O., and D.F.
Funding
This research was funded by Hospices Civils de Lyon and Université de Lyon and Fresenius Kabi.
Conflicts of Interest
D.F. and L.K. have received honoraria from Fresenius Kabi. Fresenius Kabi had no role in the design, execution, interpretation, or writing of the study. M.C.d.O. has no conflicts of interest to declare.
References
- Brenner, B.M.; Meyer, T.W.; Hostetter, T.H. Dietary protein intake and the progressive nature of kidney disease: The role of hemodynamically mediated glomerular injury in the pathogenesis of progressive glomerular sclerosis in aging, renal ablation, and intrinsic renal disease. N. Engl. J. Med. 1982, 307, 652–659. [Google Scholar] [PubMed]
- Shah, A.P.; Kalantar-Zadeh, K.; Kopple, J.D. Is there a role for ketoacid supplements in the management of CKD? Am. J. Kidney Dis. 2015, 65, 659–673. [Google Scholar] [CrossRef] [PubMed]
- Milovanova, L.; Fomin, V.; Moiseev, S.; Taranova, M.; Milovanov, Y.; Lysenko Kozlovskaya, L.; Kozlov, V.; Kozevnikova, E.; Milovanova, S.; Lebedeva, M.; et al. Effect of essential amino acid кetoanalogues and protein restriction diet on morphogenetic proteins (FGF-23 and Klotho) in 3b-4 stages chronic кidney disease patients: A randomized pilot study. Clin. Exp. Nephrol. 2018, 22, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Teplan, V.; Schück, O.; Racek, J.; Mareckova, O.; Stollova, M.; Hanzal, V.; Malý, J. Reduction of plasma asymmetric dimethylarginine in obese patients with chronic kidney disease after three years of a low-protein diet supplemented with keto-amino acids: A randomized controlled trial. Wien. Klin. Wochenschr. 2008, 120, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Teplan, V.; Schück, O.; Knotek, A.; Hajný, J.; Horácková, M.; Kvapil, M. Czech multicenter study Enhanced metabolic effect of erythropoietin and keto acids in CRF patients on low-protein diet: Czech multicenter study. Am. J. Kidney Dis. 2003, 41, S26–S30. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, J.; Beaufrère, B.; Laville, M.; Fouque, D. Adaptive response to a low-protein diet in predialysis chronic renal failure patients. J. Am. Soc. Nephrol. 2001, 12, 1249–1254. [Google Scholar] [PubMed]
- Hecking, E.; Andrzejewski, L.; Prellwitz, W.; Opferkuch, W.; Müller, D.; Port, F.K. A controlled study of supplementation with essential amino acids and alpha-keto acids in the conservative management of patients with chronic renal failure. Z. Ernahrungswiss. 1982, 21, 299–311. [Google Scholar] [CrossRef]
- Wang, D.; Wei, L.; Yang, Y.; Liu, H. Dietary supplementation with ketoacids protects against CKD-induced oxidative damage and mitochondrial dysfunction in skeletal muscle of 5/6 nephrectomised rats. Skelet Muscle 2018, 8, 18. [Google Scholar] [CrossRef]
- Liu, D.; Wu, M.; Li, L.; Gao, X.; Yang, B.; Mei, S.; Fu, L.; Mei, C. Low-protein diet supplemented with ketoacids delays the progression of diabetic nephropathy by inhibiting oxidative stress in the KKAy mice model. Br. J. Nutr. 2018, 119, 22–29. [Google Scholar] [CrossRef]
- Zhang, J.-Y.; Yin, Y.; Ni, L.; Long, Q.; You, L.; Zhang, Q.; Lin, S.-Y.; Chen, J. Low-protein diet supplemented with ketoacids ameliorates proteinuria in 3/4 nephrectomised rats by directly inhibiting the intrarenal renin-angiotensin system. Br. J. Nutr. 2016, 116, 1491–1501. [Google Scholar] [CrossRef]
- Zhang, Y.; Huang, J.; Yang, M.; Gu, L.; Ji, J.; Wang, L.; Yuan, W. Effect of a low-protein diet supplemented with keto-acids on autophagy and inflammation in 5/6 nephrectomized rats. Biosci. Rep. 2015, 35, e00263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.-T.; Lu, L.; Shi, Y.; Geng, Z.-B.; Yin, Y.; Wang, M.; Wei, L.-B. Supplementation of ketoacids contributes to the up-regulation of the Wnt7a/Akt/p70S6K pathway and the down-regulation of apoptotic and ubiquitin-proteasome systems in the muscle of 5/6 nephrectomised rats. Br. J. Nutr. 2014, 111, 1536–1548. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wu, J.; Dong, Z.; Hua, C.; Hu, H.; Mei, C. A low-protein diet supplemented with ketoacids plays a more protective role against oxidative stress of rat kidney tissue with 5/6 nephrectomy than a low-protein diet alone. Br. J. Nutr. 2010, 103, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Huang, L.; Grosjean, F.; Esposito, V.; Wu, J.; Fu, L.; Hu, H.; Tan, J.; He, C.; Gray, S.; et al. Low-protein diet supplemented with ketoacids reduces the severity of renal disease in 5/6 nephrectomized rats: A role for KLF15. Kidney Int. 2011, 79, 987. [Google Scholar] [CrossRef] [PubMed]
- Maniar, S.; Beaufils, H.; Laouari, D.; Forget, D.; Kleinknecht, C. Supplemented low-protein diets protect the rat kidney without causing undernutrition. J. Lab. Clin. Med. 1992, 120, 851–860. [Google Scholar] [PubMed]
- Laouari, D.; Jean, G.; Kleinknecht, C.; Broyer, M. Growth, free plasma and muscle amino-acids in uraemic rats fed various low-protein diets. Pediatr. Nephrol. 1991, 5, 318–322. [Google Scholar] [CrossRef]
- Benjelloun, A.S.; Merville, P.; Cambar, J.; Aparicio, M. Effects of a low-protein diet on urinary glycosaminoglycan excretion in adriamycin-treated rats. Nephron 1993, 64, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Barsotti, G.; Moriconi, L.; Cupisti, A.; Dani, L.; Ciardella, F.; Lupetti, S.; Giovannetti, S. Protection of renal function and of nutritional status in uremic rats by means of a low-protein, low-phosphorus supplemented diet. Nephron 1988, 49, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Meisinger, E.; Gretz, N.; Strauch, M. Hyperfiltration due to amino and keto acid supplements of low-protein diets: Influence on proteinuria. Infus. Klin Ernahr 1987, 14 (Suppl. 5), 26–29. [Google Scholar]
- Di Iorio, B.R.; Marzocco, S.; Bellasi, A.; De Simone, E.; Dal Piaz, F.; Rocchetti, M.T.; Cosola, C.; Di Micco, L.; Gesualdo, L. Nutritional therapy reduces protein carbamylation through urea lowering in chronic kidney disease. Nephrol. Dial. Transplant. 2018, 33, 804–813. [Google Scholar] [CrossRef]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mircescu, G. Ketoanalogue-Supplemented Vegetarian Very Low-Protein Diet and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [PubMed]
- Di Iorio, B.; Di Micco, L.; Torraca, S.; Sirico, M.L.; Russo, L.; Pota, A.; Mirenghi, F.; Russo, D. Acute effects of very-low-protein diet on FGF23 levels: A randomized study. Clin. J. Am. Soc. Nephrol. 2012, 7, 581–587. [Google Scholar] [PubMed]
- Marzocco, S.; Dal Piaz, F.; Di Micco, L.; Torraca, S.; Sirico, M.L.; Tartaglia, D.; Autore, G.; Di Iorio, B. Very low protein diet reduces indoxyl sulfate levels in chronic kidney disease. Blood Purif. 2013, 35, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, B.R.; Cucciniello, E.; Martino, R.; Frallicciardi, A.; Tortoriello, R.; Struzziero, G. Acute and persistent antiproteinuric effect of a low-protein diet in chronic kidney disease. G Ital. Nefrol 2009, 26, 608–615. [Google Scholar] [PubMed]
- Menon, V.; Kopple, J.D.; Wang, X.; Beck, G.J.; Collins, A.J.; Kusek, J.W.; Greene, T.; Levey, A.S.; Sarnak, M.J. Effect of a very low-protein diet on outcomes: Long-term follow-up of the Modification of Diet in Renal Disease (MDRD) Study. Am. J. Kidney Dis. 2009, 53, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Mircescu, G.; Gârneaţă, L.; Stancu, S.H.; Căpuşă, C. Effects of a supplemented hypoproteic diet in chronic kidney disease. J. Ren. Nutr. 2007, 17, 179–188. [Google Scholar] [PubMed]
- Gennari, F.J.; Hood, V.L.; Greene, T.; Wang, X.; Levey, A.S. Effect of dietary protein intake on serum total CO2 concentration in chronic kidney disease: Modification of Diet in Renal Disease study findings. Clin. J. Am. Soc. Nephrol. 2006, 1, 52–57. [Google Scholar] [CrossRef]
- Menon, V.; Wang, X.; Greene, T.; Beck, G.J.; Kusek, J.W.; Selhub, J.; Levey, A.S.; Sarnak, M.J. Homocysteine in chronic kidney disease: Effect of low protein diet and repletion with B vitamins. Kidney Int. 2005, 67, 1539–1546. [Google Scholar] [Green Version]
- Feiten, S.F.; Draibe, S.A.; Watanabe, R.; Duenhas, M.R.; Baxmann, A.C.; Nerbass, F.B.; Cuppari, L. Short-term effects of a very-low-protein diet supplemented with ketoacids in nondialyzed chronic kidney disease patients. Eur. J. Clin. Nutr. 2005, 59, 129–136. [Google Scholar] [PubMed]
- Prakash, S.; Pande, D.P.; Sharma, S.; Sharma, D.; Bal, C.S.; Kulkarni, H. Randomized, double-blind, placebo-controlled trial to evaluate efficacy of ketodiet in predialytic chronic renal failure. J. Ren. Nutr. 2004, 14, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Di Iorio, B.R.; Minutolo, R.; De Nicola, L.; Bellizzi, V.; Catapano, F.; Iodice, C.; Rubino, R.; Conte, G. Supplemented very low protein diet ameliorates responsiveness to erythropoietin in chronic renal failure. Kidney Int. 2003, 64, 1822–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malvy, D.; Maingourd, C.; Pengloan, J.; Bagros, P.; Nivet, H. Effects of severe protein restriction with ketoanalogues in advanced renal failure. J. Am. Coll. Nutr. 1999, 18, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Levey, A.S.; Greene, T.; Chumlea, W.C.; Gassman, J.J.; Hollinger, D.L.; Maroni, B.J.; Merrill, D.; Scherch, L.K.; Schulman, G.; et al. Effect of dietary protein restriction on nutritional status in the Modification of Diet in Renal Disease Study. Kidney Int. 1997, 52, 778–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Adler, S.; Caggiula, A.W.; England, B.K.; Greene, T.; Hunsicker, L.G.; Kusek, J.W.; Rogers, N.L.; Teschan, P.E. Effects of dietary protein restriction on the progression of advanced renal disease in the Modification of Diet in Renal Disease Study. Am. J. Kidney Dis. 1996, 27, 652–663. [Google Scholar] [CrossRef]
- Klahr, S.; Levey, A.S.; Beck, G.J.; Caggiula, A.W.; Hunsicker, L.; Kusek, J.W.; Striker, G. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N. Engl. J. Med. 1994, 330, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Coggins, C.H.; Dwyer, J.T.; Greene, T.; Petot, G.; Snetselaar, L.G.; Van Lente, F. Serum lipid changes associated with modified protein diets: Results from the feasibility phase of the Modification of Diet in Renal Disease Study. Am. J. Kidney Dis. 1994, 23, 514–523. [Google Scholar] [CrossRef]
- Lindenau, K.; Abendroth, K.; Kokot, F.; Vetter, K.; Rehse, C.; Fröhling, P.T. Therapeutic effect of keto acids on renal osteodystrophy. A prospective controlled study. Nephron 1990, 55, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Jungers, P.; Chauveau, P.; Ployard, F.; Lebkiri, B.; Ciancioni, C.; Man, N.K. Comparison of ketoacids and low protein diet on advanced chronic renal failure progression. Kidney Int. Suppl. 1987, 22, S67–S71. [Google Scholar] [PubMed]
- Mitch, W.E.; Walser, M.; Sapir, D.G. Nitrogen sparing induced by leucine compared with that induced by its keto analogue, alpha-ketoisocaproate, in fasting obese man. J. Clin. Investig. 1981, 67, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Goodship, T.H.; Mitch, W.E.; Hoerr, R.A.; Wagner, D.A.; Steinman, T.I.; Young, V.R. Adaptation to low-protein diets in renal failure: Leucine turnover and nitrogen balance. J. Am. Soc. Nephrol. 1990, 1, 66–75. [Google Scholar]
- Garibotto, G.; Sofia, A.; Parodi, E.L.; Ansaldo, F.; Bonanni, A.; Picciotto, D.; Signori, A.; Vettore, M.; Tessari, P.; Verzola, D. Effects of Low-Protein, and Supplemented Very Low–Protein Diets, on Muscle Protein Turnover in Patients With CKD. Kidney Int. Rep. 2018, 3, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Walser, M.; Coulter, A.W.; Dighe, S.; Crantz, F.R. The effect of keto-analogues of essential amino acids in severe chronic uremia. J. Clin. Investig. 1973, 52, 678–690. [Google Scholar] [PubMed]
- Tom, K.; Young, V.R.; Chapman, T.; Masud, T.; Akpele, L.; Maroni, B.J. Long-term adaptive responses to dietary protein restriction in chronic renal failure. Am. J. Physiol. 1995, 268, E668–E677. [Google Scholar] [PubMed]
- Koppe, L.; Mafra, D.; Fouque, D. Probiotics and chronic kidney disease. Kidney Int. 2015, 88, 958–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D.; Wong, J.; Pahl, M.; Piceno, Y.M.; Yuan, J.; Desantis, T.Z.; Ni, Z.; Nguyen, T.-H.; Andersen, G.L. Chronic kidney disease alters intestinal microbial flora. Kidney Int. 2012, 83, 308–315. [Google Scholar]
- Walser, M.; Jarskog, F.L.; Hill, S.B. Branched-chain-ketoacid metabolism in patients with chronic renal failure. Am. J. Clin. Nutr. 1989, 50, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Koppe, L.; Nyam, E.; Vivot, K.; Manning Fox, J.E.; Dai, X.-Q.; Nguyen, B.N.; Trudel, D.; Attané, C.; Moullé, V.S.; MacDonald, P.E.; et al. Urea impairs β cell glycolysis and insulin secretion in chronic kidney disease. J. Clin. Investig. 2016, 126, 3598–3612. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Yuan, J.; Norris, K. Role of urea in intestinal barrier dysfunction and disruption of epithelial tight junction in chronic kidney disease. Am. J. Nephrol. 2013, 37, 1–6. [Google Scholar] [CrossRef]
- D’Apolito, M.; Du, X.; Zong, H.; Catucci, A.; Maiuri, L.; Trivisano, T.; Pettoello-Mantovani, M.; Campanozzi, A.; Raia, V.; Pessin, J.E.; et al. Urea-induced ROS generation causes insulin resistance in mice with chronic renal failure. J. Clin. Investig. 2009, 120, 203–213. [Google Scholar] [CrossRef]
- Koeth, R.A.; Kalantar-Zadeh, K.; Wang, Z.; Fu, X.; Tang, W.H.W.; Hazen, S.L. Protein carbamylation predicts mortality in ESRD. J. Am. Soc. Nephrol. 2013, 24, 853–861. [Google Scholar] [CrossRef]
- Chauveau, P.; Koppe, L.; Combe, C.; Lasseur, C.; Trolonge, S.; Aparicio, M. Vegetarian diets and chronic kidney disease. Nephrol. Dial. Transplant. 2018, 34, 199–207. [Google Scholar]
- Bellizzi, V.; Di Iorio, B.R.; De Nicola, L.; Minutolo, R.; Zamboli, P.; Trucillo, P.; Catapano, F.; Cristofano, C.; Scalfi, L.; Conte, G.; et al. Very low protein diet supplemented with ketoanalogs improves blood pressure control in chronic kidney disease. Kidney Int. 2007, 71, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Brito-Ashurst, I.; Varagunam, M.; Raftery, M.J.; Yaqoob, M.M. Bicarbonate supplementation slows progression of CKD and improves nutritional status. J. Am. Soc. Nephrol. 2009, 20, 2075–2084. [Google Scholar] [PubMed]
- Menon, V.; Tighiouart, H.; Vaughn, N.S.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Greene, T.; Sarnak, M.J. Serum bicarbonate and long-term outcomes in CKD. Am. J. Kidney Dis. 2010, 56, 907–914. [Google Scholar] [PubMed]
- Lorenzo, C.; Nath, S.D.; Hanley, A.J.G.; Abboud, H.E.; Haffner, S.M. Relation of Low Glomerular Filtration Rate to Metabolic Disorders in Individuals without Diabetes and with Normoalbuminuria. Clin. J. Am. Soc. Nephrol. 2008, 3, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, R.H. Insulin and its role in chronic kidney disease. Pediatr. Nephrol. 2008, 23, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Greene, T.; Pereira, A.A.; Wang, X.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. Glycosylated Hemoglobin and Mortality in Patients with Nondiabetic Chronic Kidney Disease. JASN 2005, 16, 3411–3417. [Google Scholar] [CrossRef] [Green Version]
- Rigalleau, V.; Blanchetier, V.; Combe, C.; Guillot, C.; Deleris, G.; Aubertin, J.; Aparicio, M.; Gin, H. A low-protein diet improves insulin sensitivity of endogenous glucose production in predialytic uremic patients. Am. J. Clin. Nutr. 1997, 65, 1512–1516. [Google Scholar] [CrossRef] [Green Version]
- Rigalleau, V.; Combe, C.; Blanchetier, V.; Aubertin, J.; Aparicio, M.; Gin, H. Low protein diet in uremia: Effects on glucose metabolism and energy production rate. Kidney Int. 1997, 51, 1222–1227. [Google Scholar] [Green Version]
- Fontana, L.; Cummings, N.E.; Arriola Apelo, S.I.; Neuman, J.C.; Kasza, I.; Schmidt, B.A.; Cava, E.; Spelta, F.; Tosti, V.; Syed, F.A.; et al. Decreased Consumption of Branched-Chain Amino Acids Improves Metabolic Health. Cell Rep. 2016, 16, 520–530. [Google Scholar] [CrossRef] [Green Version]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 10, CD001892. [Google Scholar] [PubMed]
- Li, A.; Lee, H.Y.; Lin, Y.C. The Effect of Ketoanalogues on Chronic Kidney Disease Deterioration: A Meta-Analysis. Nutrients 2019, 26, 957. [Google Scholar]
- Chauveau, P.; Combe, C.; Rigalleau, V.; Vendrely, B.; Aparicio, M. Restricted protein diet is associated with decrease in proteinuria: Consequences on the progression of renal failure. J. Ren. Nutr. 2007, 17, 250–257. [Google Scholar] [PubMed]
- Di Iorio, B.R.; Bellizzi, V.; Bellasi, A.; Torraca, S.; D’Arrigo, G.; Tripepi, G.; Zoccali, C. Phosphate attenuates the anti-proteinuric effect of very low-protein diet in CKD patients. Nephrol. Dial. Transplant. 2013, 28, 632–640. [Google Scholar] [PubMed]
- Bellizzi, V.; Chiodini, P.; Cupisti, A.; Viola, B.F.; Pezzotta, M.; De Nicola, L.; Minutolo, R.; Barsotti, G.; Piccoli, G.B.; Di Iorio, B. Very low-protein diet plus ketoacids in chronic kidney disease and risk of death during end-stage renal disease: A historical cohort controlled study. Nephrol. Dial. Transplant. 2015, 30, 71–77. [Google Scholar] [PubMed]
- Chauveau, P.; Couzi, L.; Vendrely, B.; de Précigout, V.; Combe, C.; Fouque, D.; Aparicio, M. Long-term outcome on renal replacement therapy in patients who previously received a keto acid-supplemented very-low-protein diet. Am. J. Clin. Nutr. 2009, 90, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Koppe, L.; Fouque, D. The Role for Protein Restriction in Addition to Renin-Angiotensin-Aldosterone System Inhibitors in the Management of CKD. Am. J. Kidney Dis. 2018, 73, 248–257. [Google Scholar] [PubMed]
- Jiang, Z.; Zhang, X.; Yang, L.; Li, Z.; Qin, W. Effect of restricted protein diet supplemented with keto analogues in chronic kidney disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2016, 48, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Chauveau, P.; Barthe, N.; Rigalleau, V.; Ozenne, S.; Castaing, F.; Delclaux, C.; de Précigout, V.; Combe, C.; Aparicio, M. Outcome of nutritional status and body composition of uremic patients on a very low protein diet. Am. J. Kidney Dis. 1999, 34, 500–507. [Google Scholar] [CrossRef]
- Bellizzi, V.; Calella, P.; Hernández, J.N.; González, V.F.; Lira, S.M.; Torraca, S.; Arronte, R.U.; Cirillo, P.; Minutolo, R.; Montúfar Cárdenas, R.A. Safety and effectiveness of low-protein diet supplemented with ketoacids in diabetic patients with chronic kidney disease. BMC Nephrol. 2018, 19, 110. [Google Scholar]
- Aparicio, M.; Chauveau, P.; Combe, C. Low protein diets and outcome of renal patients. J. Nephrol. 2001, 14, 433–439. [Google Scholar] [PubMed]
- Zoccali, C.; Mallamaci, F. Moderator’s view: Low-protein diet in chronic kidney disease: Effectiveness, efficacy and precision nutritional treatments in nephrology. Nephrol. Dial. Transplant. 2018, 33, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Brunori, G.; Viola, B.F.; Parrinello, G.; De Biase, V.; Como, G.; Franco, V.; Garibotto, G.; Zubani, R.; Cancarini, G.C. Efficacy and safety of a very-low-protein diet when postponing dialysis in the elderly: A prospective randomized multicenter controlled study. Am. J. Kidney Dis. 2007, 49, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Nolph, K. Efficacy and safety of a very-low-protein diet in the elderly: What are the options? Am. J. Kidney Dis. 2008, 51, 530–531. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Leone, F.; Attini, R.; Parisi, S.; Fassio, F.; Deagostini, M.C.; Ferraresi, M.; Clari, R.; Ghiotto, S.; Biolcati, M.; et al. Association of low-protein supplemented diets with fetal growth in pregnant women with CKD. Clin. J. Am. Soc. Nephrol. 2014, 9, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Qian, J.; Sun, W.; Lin, A.; Cao, L.; Wang, Q.; Ni, Z.; Wan, Y.; Linholm, B.; Axelsson, J.; et al. Better preservation of residual renal function in peritoneal dialysis patients treated with a low-protein diet supplemented with keto acids: A prospective, randomized trial. Nephrol. Dial. Transplant. 2009, 24, 2551–2558. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-B.; Cheng, B.-C.; Kao, T.-W. A comparison of progression of chronic renal failure: low dose vs. standard dose ketoacids. Kidney Res. Clin. Pract. 2012, 31, A24. [Google Scholar] [CrossRef]
- Shimomura, A.; Matsui, I.; Hamano, T.; Ishimoto, T.; Katou, Y.; Takehana, K.; Inoue, K.; Kusunoki, Y.; Mori, D.; Nakano, C.; et al. Dietary l-Lysine Prevents Arterial Calcification in Adenine-Induced Uremic Rats. JASN 2014, 25, 1954–1965. [Google Scholar] [CrossRef] [PubMed]
- Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am. J. Kidney Dis. 2000, 35, S1–S140. [Google Scholar]
- Cano, N.; Fiaccadori, E.; Tesinsky, P.; Toigo, G.; Druml, W.; DGEM (German Society for Nutritional Medicine); Kuhlmann, M.; Mann, H.; Hörl, W.H.; ESPEN (European Society for Parenteral and Enteral Nutrition). ESPEN Guidelines on Enteral Nutrition: Adult renal failure. Clin. Nutr. 2006, 25, 295–310. [Google Scholar] [CrossRef]
- Campbell, K.L.; Rangan, G.K.; Lopez-Vargas, P.; Tong, A. KHA-CARI Autosomal Dominant Polycystic Kidney Disease Guideline: Diet and Lifestyle Management. Semin. Nephrol. 2015, 35, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Stevens, P.E. Summary of KDIGO 2012 CKD Guideline: Behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014, 85, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizler, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.M.; et al. Etiology of the protein-energy wasting syndrome in chronic kidney disease: A consensus statement from the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. 2013, 23, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional Management of Chronic Kidney Disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Mennini, F.S.; Russo, S.; Marcellusi, A.; Quintaliani, G.; Fouque, D. Economic effects of treatment of chronic kidney disease with low-protein diet. J. Ren. Nutr. 2014, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Nazha, M.; Capizzi, I.; Vigotti, F.N.; Scognamiglio, S.; Consiglio, V.; Mongilardi, E.; Bilocati, M.; Avagnina, P.; Versino, E. Diet as a system: An observational study investigating a multi-choice system of moderately restricted low-protein diets. BMC Nephrol. 2016, 17, 197. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Amino-acid and transamination of ketoacid analogues of amino acids in order to synthesize protein.
Figure 1.
Amino-acid and transamination of ketoacid analogues of amino acids in order to synthesize protein.

Figure 2.
Proven and controversial mechanism of VLDP/LPD + KAs supplementation in CKD Abbreviations: URS: uremic retention solutes, EAAs: essential amino acids, BCAAs: branched-chain amino acids, LPD: low protein diet, VLDP: very low protein diet, GFR: glomerular filtration rate, and KAs: ketoacid analogues.
Figure 2.
Proven and controversial mechanism of VLDP/LPD + KAs supplementation in CKD Abbreviations: URS: uremic retention solutes, EAAs: essential amino acids, BCAAs: branched-chain amino acids, LPD: low protein diet, VLDP: very low protein diet, GFR: glomerular filtration rate, and KAs: ketoacid analogues.


{kind=link}
{kind=link}
Table 1.
Ketoacid analogues composition.
| Component Name | mg/pill |
|---|---|
| Ca-Keto-dl-isoleucine | 67 |
| Ca-Ketoeucine | 101 |
| Ca-Ketophénylalanine | 68 |
| Ca-Ketovaline | 86 |
| Ca-Hydroxy-dl-methionine | 59 |
| l-Lysine monoacetate | 105 |
| l-Threonine | 53 |
| l-Tryptophan | 23 |
| l-Histidine | 38 |
| l-Tyrosine | 30 |
Ca: calcium.
Table 2.
Animal studies that examined the effects of VLPD/LPD supplemented with ketoacid analogues on various endpoints.
Table 2.
Animal studies that examined the effects of VLPD/LPD supplemented with ketoacid analogues on various endpoints.
| Study | Models | Diet Intervention | Follow-Up | Results (LPD vs. VLDP/LPD + KAs) |
|---|---|---|---|---|
| Wang et al., 2018 [8] | 5/6 nephrectomy rats | NPD: 22% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 24 weeks | ↓ muscle atrophy ↑ activities of mitochondrial electron transport chain complexes and mitochondrial respiration, ↓ muscle oxidative damage ↑body weight |
| Liu et al., 2018 [9] | KKAy mice, an early type 2 DN model | NPD: 22% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 12 weeks | ↓ proteinuria ↓ mesangial proliferation and oxidative stress ↑ serum albumin and body weight No difference in creatinine and GFR |
| Zhang et al., 2016 [10] | 3/4 nephrectomy rats | NPD: 18% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 12 weeks | ↓ proteinuria ↓ intrarenal RAS activation. ↓ transforming growth factor-β1 in the mesangial cells |
| Zhang et al., 2015 [11] | 5/6 nephrectomy rats | NPD: 11 g/kg/day protein vs. LPD: 3 g/kg/day protein vs. LPD + KAs: 3 g/kg/day protein which including 5% protein plus 1% KA | 24 weeks | ↑ body weight, gastrocnemius muscle mass ↓ autophagy marker in muscle No difference of inflammation markers |
| Wang et al., 2014 [12] | 5/6 nephrectomy rats | NPD: 22% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 24 weeks | ↑improved protein synthesis and increased related mediators such as phosphorylated Akt in the muscle ↓ protein degradation and proteasome activity in the muscle |
| Gao et al., 2010 [13] | 5/6 Nephrectomy rats | NPD: 22% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 24 weeks | ↓ proteinuria, glomerular sclerosis, and tubulointerstitial fibrosis ↑renal function ↑ body weight and albumin ↓ lipid and protein oxidative products |
| Gao et al., 2011 [14] | 5/6 Nephrectomy rats | NPD: 22% protein vs. LPD: 6% protein vs. LPD + KAs: 5% protein plus 1% KA | 6 months | ↑ body weight and albumin ↑ Kruppel-like factor-15, a transcription factor shown to reduce fibrosis |
| Maniar et al., 1992 [15] | 5/6 Nephrectomy rats | NPD: 16% casein vs. LPD + EAA: 6% casein + EAA vs. LPD + KAs: 6% casein + KA | 3 months | No difference on body weight No difference on proteinuria vs. LDP + EAA but reduction vs. NPD ↓ creatinemia, proteinuria, glomerular sclerosis, and tubulointerstitial fibrosis vs. NPD but no difference vs. LPD + EAA ↑survival vs. NPD but no difference vs. LPD + EAA |
| Laouari et al., 1991 [16] | 5/6 Nephrectomy rats | NPD: 12% casein vs. LPD + EAAs: 5% casein + EAA vs. LPD + KAs: 5% casein + KA | ↓Appetite and growth No increase in BCAAs | |
| Benjelloun et al., 1993 [17] | Rats with after a single 5 mg/kg intravenous injection of Adriamycin: a model of induces glomerular damage in glomerulonephritis. | NPD: 21% protein vs. LPD + KAs: 6% protein plus KA | 15 days | ↓ proteinuria ↓ glycosaminoglycan excretion and glomerular glycosaminoglycan contents |
| Barsotti et al; 1988 [18] | 5/6 Nephrectomy rats | NPD: 20.5% protein vs. LPD + KAs: 3.3% protein plus 7.5% KA | 3 months | ↑survival ↑ GFR ↓ proteinuria and histological damage of kidney No difference in body weight and albuminuria |
| Meisinger et al., 1987 [19] | 5/6 Nephrectomy rats | LPD: 8% protein vs. LPD + KAs: 8% protein plus KA | 3 months | ↓ proteinuria |
NPD: normal protein diet. HPD: high protein diet. GFR: estimated Glomerular Filtration Rate. LPD: Low protein diet. KAs: ketoacid analogues. EAAs: essential amino acids. BCAAs: branched-chain amino acids; RAS: renin angiotensin system; NPD: normal protein diet.
Table 3.
Main RCTs that examined the effects of LPD or VLDP/LPD supplemented with ketoacid analogues on various endpoints in non-dialysis patients with eDFG under 60 mL/min/1.73 m2.
Table 3.
Main RCTs that examined the effects of LPD or VLDP/LPD supplemented with ketoacid analogues on various endpoints in non-dialysis patients with eDFG under 60 mL/min/1.73 m2.
| Study | Design of Study | Diet | Follow-Up | Results | Comments |
|---|---|---|---|---|---|
| Milovanova et al., 2018 [3] | RCT n = 42 in LPD + KA vs. LPD n = 37 Non-diabetic CKD 3B–4 | LPD (0.6 g/kg of body weight/day, comprising 0.3 g of vegetable protein and 0.3 g of animal protein, phosphorus content ≤ 800 mg/day and calories: 34–35 kcal/kg/day) vs. LPD + KA: 0.6 g/kg of body weight/day | 14 months | ↑ eGFR (29.1 L/min/1.73 m2 vs. 26.6) ↓SBP ↑BMI and muscle body mass NO change in albumin levels No change in lipids parameters ↓ phosphate, FGF23, and PTH levels ↑Klotho levels and phosphate binder uses ↑bicarbonates levels | Similar protein intake in both group Long follow up |
| Di Iorio et al., 2018 [20] | RCT, crossover trial CKD stages 3B–4 Group A1: 3 months of FD, 6 months of VLPD + KA, 3 months of FD and 6 months of MD Group B: 3 months of FD, 6 months of MD, 3 months of FD and 6 months of VLPD + KA. n = 30 in each group | FD: proteins 1 g/kg body weight (bw)/day (animal proteins 50–70 g/day, vegetal proteins 15–20 g/day), energy 30–35 kcal/bw/day, calcium (Ca) 1.1–1.3 g/day, phosphorus (P) 1.2–1.5 g/day, sodium (Na) 6 g/day and potassium (K) 2–4 g/day. MD: proteins 0.7–0.8 g/kg bw/day (animal proteins 30–40 g/day, vegetal proteins 40–50 g/day), energy 30–35 kcal/bw/day, Ca 1.1–1.3 g/day, P 1.2–1.5 g/day, Na 2.5–3 g/day and K 2–4 g/day. VLPD + KA: proteins 0.3–0.5 g/kg bw/day (animal proteins 0 g/day, vegetal proteins 30–40 g/day), energy 30–35 kcal/bw/day, Ca 1.1–1.3 g/day, P 0.6–0.8 g/day, Na 6 g/day, K 2–4 g/day plus a mixture of KA | 6 months | ↓ SBP No change in creatinuria ↓proteinuria ↓ phosphate, FGF23, and PTH levels ↑bicarbonates levels ↑Hg levels ↓protein carbamylation | Sodium intake and phosphore intake was reduce in VLDP + KA group |
| Garneata et al., 2016 [21] | RCT CKD stage 4–5, proteinuria < 1 g/24 h n = 207 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = vegetarian diet, 0.3 g protein/kg per day + KA | 15 months | ↓ RRT initiation or a >50% reduction in the initial GFR (13% in KA+LDP vs. 42% in LPD reached the primary composite efficacy point i.e., RRT initiation or a >50% reduction in the initial GFR) ↓CRP ↑bicarbonates levels ↓uric acid ↓ phosphate, FGF23 and PTH levels and phosphate binder uses No difference in proteinuria No difference of death and CV events No difference of albumin, BMI No change in lipids parameters | Long follow up Large effective Only 14% of patients screened was included |
| Di Iorio et al., 2012 [22] | RCT, crossover trial eGFR < 55 and > 20 mL/min/1.73 m2 Group A: VLDP + KA during the first week and LPD during the second week Group B: LPD during the first week and a VLPD + KA during the second week. n = 16 in each group | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 1 week | ↓ phosphate (−12%), FGF23 (−33.5) No change on calcium a post hoc of this study, ↓ indoxyl sulfate [23] ↑bicarbonates levels | Short exposition |
| Di Iorio et al., 2009 [24] | RCT, crossover trial eGFR < 55 and > 20 mL/min Group A: VLDP + KA during 6 month and a LPD during 6 month Group B: LPD during 6 month and a VLDP + KA during 6 month. n = 16 in each group 32 patients | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 6 months | ↓proteinuria and AGE | Open label Phosphor intake was different and lower in VLDP+ KA |
| Menon et al., 2009 [25] | Post hoc study of MDRD study B CKD stage 4 nondiabetic n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 10.2 years | No delay progression to kidney failure ↑the risk of death. | Long follow up without intervention -Observance and protein intake was not monitored during the follow up |
| Teplan et al., 2008 [4] | RCT, double-blind placebo CKD stage 4 n = 111 | LDP: 0.6 g protein/kg per day vs. LPD + KA: 0.6 g protein/kg per day + KA | 36 months | ↓ADMA ↓ BMI and visceral body fat in obese patients ↓proteinuria ↓ glycated hemoglobin ↓LDL-cholesterol | Mean BMI was > 30 kg/m2 at the inclusion Long follow up No difference of protein intake Using a placebo |
| Mircescu et al., 2007 [26] | RCT eGFR <30 mL/min/1.73 m2, nondiabetic n = 53 | VLPD + KA =0.3 g/kg vegetable proteins + KA vs. LPD =0.6 g/kg/d) | 48 weeks | ↑bicarbonates levels ↑calcium levels and ↓ phosphate lower percentages of patients in group I required renal replacement therapy initiation (4% vs. 27%). No change of rate of eGFR and proteinuria No change in SBP | Open label |
| Gennari et al., 2006 [27] | Post hoc study of MDRD study RCT CKD stage 4–5 n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 2,2 years | No significant effect of diet on serum total CO2 was seen | |
| Menon et al., 2005 [28] | Post oc study of MDRD study RCT CKD stage 4–5 n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 2.2 years | ↓ homocysteinemia by 24% at 1 year | |
| Feiten et al., 2005 [29] | RCT n = 24 eGFR <25 mL/min | VLPD + KA = 0.3 g/kg vegetable proteins + KA vs. LPD = 0.6 g/kg/d | 4 months | ↑bicarbonates levels No change on calcium levels ↓ phosphate and PTH Decrease the progression of renal decline function of rate of eGFR No change in lipid parameters No change in nutritional status (BMI, albumin) | Open label Short time of follow up Significant reduction in dietary phosphorus (529 ± 109 to 373 ± 125 mg/day, p < 0.05) |
| Prakash et al., 2004 [30] | RCT, double-blind placebo eGFR:28 mL/min/1.73 m2 n = 34 | LPD = 0.6 g protein/kg per day + placebo vs. VLPD = 0.3 g protein/kg per day + KA | 9 months | preserve mGFR (−2% in LDP + KA vs. −21% in LPD) No effect on proteinuria No effect of BMI and albumin | Measure of GFR with 99mTc-DTPA The placebo is problematic because protein intake was different between both groups. |
| Teplan et al., 2003 [5] | RCT eGFR: 22–36 mL/min/1.73 m2 n = 186 | LPD 0.6 g protein/kg per day + rhuEPO + KA vs. LPD: 0.6 g protein/kg per day + rhuEPO vs. LPD: 0.6 g protein/kg per day | 3 years | Slower progression of CKD ↓proteinuria ↓LDL-cholesterol No change in SBP ↑albumin ↑ plasmatic leucine levels | Role of rhuEPO unclear Insulin clearance |
| Di Iorio et al., 2003 [31] | RCT eGFR: < or =25 mL/min/1.73 m2 n = 10 in each group | LPD = 0.6 g protein/kg per day vs. VLPD = 0.3 g protein/kg per day + KA | 2 years | No difference on hemoglobin ↓ EPO dose ↓ phosphate and PTH No change in BMI and albumin No difference in the rate of RRT initiation (8 vs. 7) Slower rate of GFR decline (creatinine clearance) ↓SBP and 24 h NA excretion ↓LDL-cholesterol | Very few populations |
| Bernhard et al., 2001 [6] | RCT CKD stage 4–5 n = 6 in each group | LPD = 0.6 g protein/kg per day vs. LPD + KA = 0.6 g protein/kg per day + KA | 3 months | No difference could be attributed to the ketoanalogs total body flux and leucine oxidation No difference on phosphorus, calcium levels No difference on BMI and albumin No difference in renal function and proteinuria No difference on bicarbonatemia | KA is metabolically safe Short follow-up Small effective |
| Malvy et al., 1999 [32] | RCT eGFR<20 mL/min/1.73 m2 n = 50 | LPD:LPD = 0.65 g protein/kg per day + Ca+ vs. VLPD + KA = 0.3 g protein/kg per day + KA | 3 months or time to eGFR < 5 mL/min/1.73 m2 or RRT | No difference on GFR progression ↑calcium levels ↓ phosphate and PTH No difference on lipid parameters | |
| Kopple et al., 1997 [33] | Post hoc study of MDRD study RCT CKD stage 4–5 n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 2,2 years | No difference of death and first hospitalization ↑ albumin ↓ transferrin, body wt, percent body fat, arm muscle area, and urine creatinine excretion No correlation between nutritional parameters and death or hospitalization ↓ energy intake | |
| Levey et al., 1996 [34] | Post hoc study of MDRD study RCT CKD stage 4–5 n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 2.2 years | A 0.2 g/kg/d lower achieved total protein intake was associated with a 1.15 mL/min/yr slower mean decline in GFR (p = 0.011), which is equivalent to 29% of the mean GFR decline | Reanalyze of MDRD study by using correlations of protein intake with a rate of decline in GFR and time to renal failure |
| Klahr et al., 1994 Study 2 [35] | RCT CKD stage 4–5 n = 255 | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 27 months | Marginally slower eGFR decline (−19% in LPD vs. 12% in VLDP + KA, p 0.067) No significant interactions between blood-pressure interventions and the rate of decline in eGFR No difference on albumin No difference in proteinuria | -Large RCT study -Good adherence of diet -Measured GFR with iothalamate |
| Coggins et al. 1994 [36] | Feasibility phase of the MDRD Study eGFR: 8 to 56 mL/min/1.73 m2 n = 96 25 participants were excluded | LPD = 0.6 g protein/kg per day vs. VLPD + KA = 0.3 g protein/kg per day + KA | 6 months | No difference on lipid parameters | Pilot study |
| Lindenau et al. 1990 [37] | RCT eGFR<15 mL/min/1.73 m2 n = 40 | LPD = 0.6 g protein/kg per day + Ca+ vs. VLPD + KA = 0.4 g protein/kg per day + KA | 12 months | Improvement in osteo-fibrotic as well as in osteo-malacic changes | A calcium supplementation was given in LPD diet as a control for KA |
| Jungers et al. 1987 [38] | RCT CKD stage 5 n = 19 | LPD = 0.6 g protein/kg per day + Ca+ vs. VLPD + KA = 0.4 g protein/kg per day + KA | 12 months | No difference on biochemical or morphometric sign of de-nutrition ↑mean renal survival duration until dialysis | Small and effective |
| Hecking et al., 1982 [7] | RCT Mean eGFR: 10.8 mL/min/1.73 m2 n = 15 | LPD = 0.6 g protein/kg per day + Ca+ vs. LPD + KA = 0.6 g protein/kg per day + KA or EAA or placebo | 3 weeks per periods | ↓ phosphate No difference on GFR and proteinuria No difference on lipids parameters No difference on albumin | Small and effective versus the placebo |
FD: Free diet. P: phosphorus. MDRD: Modification of Diet in the Renal Disease Study. eGFR: estimated Glomerular Filtration Rate. RRT: renal replacement therapy. FGF23: Fibroblast Growth Factor 23. LPD: Low protein diet. VLDP: Very low protein diet. KA: Keto-analogues. RCT: randomized controlled trial. EAA: essential amino acids; PTH: parathyroid hormone.
Table 4.
VLDP/LDP and KA in non-dialyzed patients with chronic kidney disease.
| CKD Stage | NKF/KDOQI Clinical Practice Guidelines for Nutrition in Chronic Renal Failure, 2000 [79] | ESPEN Guidelines on Enteral Nutrition: Adult Renal Failure, 2006 [80] | Australian KHA-CARI Guidelines [81] | KDIGO, 2012 [82] | International Society of Renal Nutrition and Metabolism, 2013 [83] | Review, 2017, NEJM [84] |
|---|---|---|---|---|---|---|
| 3 | 0.60–0.75 g/kg/day of protein | 0.55–0.6 g/kg/day of protein | 0.75–1.0 g/kg/day of protein | <1.3 g/kg/day protein | 0.6 and 0.8 g/kg/day protein, ≥50% of protein of HBV | <1.0 g/kg/day protein (consider 0.6–0.8 if eGFR <45 mL/min/1.73 m2 or rapid progression) |
| 4–5 | 0.60–0.75 g/kg/day of protein | 0.55–0.6 g/kg/day of protein (2/3 HBV) or ~0.3 g/kg/day of protein supplemented with KAs/EAAs (0.1 g/kg/day) | 0.75–1.0 g/kg/day | 0.8 g/kg/day protein | 0.6 and 0.8 g/kg/day protein, ≥50% of protein of HBV | 0.6–0.8 g/kg/day protein, including 50% HBV protein, or <0.6 with addition of EAAs or KAs (0.1 g/kg/day) |
HBV: high biological value. KAs: ketoacids analogues. EAAs: essential amino acids.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Koppe, L.; Cassani de Oliveira, M.; Fouque, D. Ketoacid Analogues Supplementation in Chronic Kidney Disease and Future Perspectives. Nutrients 2019, 11, 2071. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092071
AMA Style
Koppe L, Cassani de Oliveira M, Fouque D. Ketoacid Analogues Supplementation in Chronic Kidney Disease and Future Perspectives. Nutrients. 2019; 11(9):2071. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092071
Chicago/Turabian StyleKoppe, Laetitia, Mariana Cassani de Oliveira, and Denis Fouque. 2019. "Ketoacid Analogues Supplementation in Chronic Kidney Disease and Future Perspectives" Nutrients 11, no. 9: 2071. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092071
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.