The “Fortilat” Randomized Clinical Trial Follow-Up: Neurodevelopmental Outcome at 18 Months of Age

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Trial and Intervention
2.2. The Fortilat Follow-Up Protocol
2.3. Subjects and Statistical Analysis
3. Results
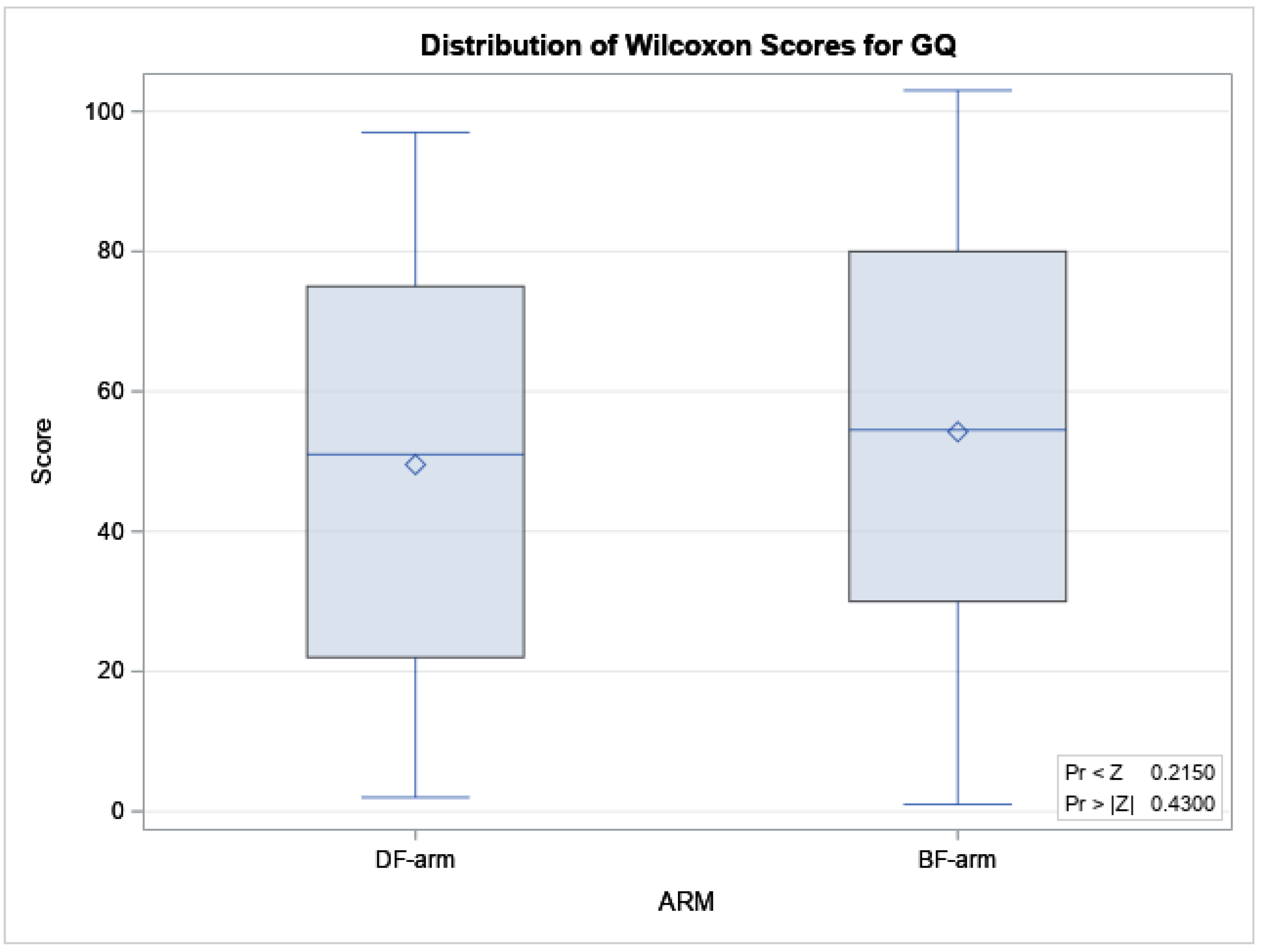
3.1. GQ in Continuous
3.2. GQ in Two Classes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Corchia, C.; Orzalesi, M. Geographic variations in outcome of very low birth weight infants in Italy. Acta Paediatr. 2007, 9, 35–38. [Google Scholar] [CrossRef]
- Vohr, B.R. Neurodevelopmental outcomes of extremely preterm infants. Clin. Perinatol. 2014, 4, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Dinerstein, A.; Nieto, R.M.; Solana, C.L.; Perez, G.P.; Otheguy, L.E.; Larguia, A.M. Early and aggressive nutritional strategy (parenteral and enteral) decreases postnatal growth failure in very low birth weight infants. J. Perinatol. 2006, 2, 436–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, A.Y.; Lee, Y.W.; Chang, M.Y. Modification of nutrition strategy for improvement of postnatal growth in very low birth weight infants. Korean J. Pediatr. 2016, 59, 165–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belfort, M.B.; Ehrenkranz, R.A. Neurodevelopmental outcomes and nutritional strategies in very low birth weight infants. Semin. Fetal Neonatal Med. 2017, 22, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Cormack, B.E.; Harding, J.E.; Miller, S.P.; Bloomfield, F.H. The Influence of Early Nutrition on Brain Growth and Neurodevelopment in Extremely Preterm Babies: A Narrative Review. Nutrients 2019, 11, 2029. [Google Scholar] [CrossRef] [Green Version]
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 22, 7–76. [Google Scholar] [CrossRef]
- Moro, G.E.; Arslanoglu, S.; Bertino, E.; Corvaglia, L.; Montirosso, R.; Picaud, J.C.; Ziegler, E.E. XII. Human Milk in Feeding Premature Infants: Consensus Statement. J. Pediatr. Gastroenterol. Nutr. 2015, 6, S16–S19. [Google Scholar] [CrossRef]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012, 1, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Embleton, N.D. Optimal protein and energy intakes in preterm infants. Early Hum. Dev. 2007, 8, 831–837. [Google Scholar] [CrossRef]
- Dutta, S.; Singh, B.; Chessell, L.; Wilson, J.; Janes, M.; McDonald, K.; Watson, J. Guidelines for feeding very low birth weight infants. Nutrients 2015, 7, 423–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.V.; Embleton, N.D.; Harding, J.E.; McGuire, W. Multi-nutrient fortification of human milk for preterm infants. Cochrane Database Syst. Rev. 2016, 5, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mimouni, F.B.; Nathan, N.; Ziegler, E.E.; Lubetzky, R.; Mandel, D. The Use of Multinutrient Human Milk Fortifiers in Preterm Infants: A Systematic Review of Unanswered Questions. Clin. Perinatol. 2017, 4, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.E. Meeting the nutritional needs of the low-birth-weight infant. Ann. Nutr. Metab. 2011, 5, 8–18. [Google Scholar] [CrossRef]
- Radmacher, P.G.; Adamkin, D.H. Fortification of human milk for preterm infants. Semin. Fetal Neonatal Med. 2017, 2, 30–35. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. The Wapm Working Group on Nutrition. Optimization of human milk fortification for preterm infants: New concepts and recommendations. J. Perinat. Med. 2010, 3, 233–238. [Google Scholar]
- Polberger, S. III. Individualized Fortification of Human Milk: Targeted Fortification. J. Pediatr. Gastroenterol. Nutr. 2015, 5, S1–S4. [Google Scholar] [CrossRef]
- Arslanoglu, S. IV. Individualized Fortification of Human Milk: Adjustable Fortification. J. Pediatr. Gastroenterol. Nutr. 2015, 6, S1–S4. [Google Scholar] [CrossRef]
- Bertino, E.; Cavallarin, L.; Cresi, F.; Tonetto, P.; Peila, C.; Ansaldi, G.; Raia, M.; Varalda, A.; Giribaldi, M.; Conti, A.; et al. A Novel Donkey Milk-derived Human Milk Fortifier in Feeding Preterm Infants: A Randomized Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2019, 6, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Coscia, A.; Bertino, E.; Tonetto, P.; Peila, C.; Cresi, F.; Arslanoglu, S.; Moro, G.E.; Spada, E.; Milani, S.; Giribaldi, M.; et al. Nutritional adequacy of a novel human milk fortifier from donkey milk in feeding preterm infants: Study protocol of a randomized controlled clinical trial. Nutr. J. 2018, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Bertino, E.; Gastaldi, D.; Monti, G.; Baro, C.; Fortunato, D.; Garoffo, L.P.; Coscia, A.; Fabris, C.; Mussap, M.; Conti, A. Detailed proteomic analysis on DM: Insight into its hypoallergenicity. Front. Biosci. 2010, 2, 526–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastaldi, D.; Bertino, E.; Monti, G.; Baro, C.; Fabris, C.; Lezo, A.; Medana, C.; Baiocchi, C.; Mussa, M.; Galvano, F.; et al. Donkey’s milk detailed lipid composition. Front. Biosci. 2010, 2, 537–546. [Google Scholar]
- Trinchese, G.; Cavaliere, G.; Canani, R.B.; Matamoros, S.; Bergamo, P.; De Filippo, C.; Greco, L. Human, donkey and cow milk differently affects energy efficiency and inflammatory state by modulating mitochondrial function and gut microbiota. J. Nutr. Biochem. 2015, 2, 1136–1146. [Google Scholar] [CrossRef] [Green Version]
- Trinchese, G.; Cavaliere, G.; De Filippo, C.; Aceto, S.; Prisco, M.; Chun, J.T.; Penna, E.; Negri, R.; Muredda, L.; Demurtas, A.; et al. Human Milk and Donkey Milk, Compared to Cow Milk, Reduce Inflammatory Mediators and Modulate Glucose and Lipid Metabolism, Acting on Mitochondrial Function and Oleylethanolamide Levels in Rat Skeletal Muscle. Front. Physiol. 2018, 30, 9–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheikh Ismail, L.; Knight, H.; Bhutta, Z. Anthropometric protocols for the construction of new international fetal and newborn growth standards: The INTERGROWTH-21st Project. BJOG Int. J. Obstetr. Gynecol. 2013, 120, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Onis, M.; Onyango, A.W.; Van den Broeck, J.; Chumlea, W.C.; Martorell, R. Measurement and standardization protocols for anthropometry used in the construction of a new international growth reference. Food Nutr. Bull. 2004, 25, S27–S36. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Helps, S.K.; Hart, D.; Zatorska, A.; Gupta, N.; Cianfaglione, R.; Vollmer, B. Minor neurological signs and behavioural function at age 2 years in neonatal hypoxic ischaemic encephalopathy (HIE). Eur. J. Paediatr. Neurol. 2020, 27, 78–85. [Google Scholar] [CrossRef]
- Bax, M.C.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Dan, B. Executive Committee for the Definition of Cerebral Palsy. Proposed definition and classification of cerebral palsy. Dev. Med. Child. Neurol. 2005, 47, 571–576. [Google Scholar] [CrossRef]
- Intergowth 21st. Available online: https://intergrowth21.tghn.org/standards-tools/ (accessed on 1 November 2020).
- INES Chart. Available online: http://www.inescharts.com/ (accessed on 1 November 2020).
- Mariani, E.; Biasini, A.; Marvulli, L.; Martini, S.; Aceti, A.; Faldella, G.; Corvaglia, L.; Sansavini, A.; Savini, S.; Agostini, F.; et al. Strategies of Increased Protein Intake in ELBW Infants Fed by Human Milk Lead to Long Term Benefits. Front. Public Health 2018, 27, 272. [Google Scholar] [CrossRef]
- Ohnishi, S.; Ichiba, H.; Tanaka, Y.; Harada, S.; Matsumura, H.; Kan, A.; Asada, Y.; Shintaku, H. Early and intensive nutritional strategy combining parenteral and enteral feeding promotes neurodevelopment and growth at 18months of corrected age and 3years of age in extremely low birth weight infants. Early Hum. Dev. 2016, 1, 35–41. [Google Scholar] [CrossRef]
- Ruys, C.A.; Bröring, T.; van Schie, P.E.M.; van de Lagemaat, M.; Rotteveel, J.; Finken, M.J.J.; Oostrom, K.J.; Lafeber, H.N. Neurodevelopment of children born very preterm and/or with a very low birth weight: 8-Year follow-up of a nutritional RCT. Clin. Nutr. ESPEN 2019, 3, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Kashaki, M.; Samghabadi, F.M.; Bordbar, A. Effect of Fortification of Breast Milk in Conjugation with Protein Supplement on Neurodevelopment of Preterm Low Birth Weight Infants at 3 Years. Med. Arch. 2019, 7, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Pfister, K.M.; Zhang, L.; Miller, N.C.; Ingolfsland, E.C.; Demerath, E.W.; Ramel, S.E. Early body composition changes are associated with neurodevelopmental and metabolic outcomes at 4 years of age in very preterm infants. Pediatr. Res. 2018, 84, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.K.; Kennedy, K.; Castaneda-Gutierrez, E.; Forsyth, S.; Godfrey, K.M.; Koletzko, B.; Latulippe, M.E.; Ozanne, S.E.; Rueda, R.; Schoemaker, M.H.; et al. Postnatal growth in preterm infants and later health outcomes:a systematic review. Acta Pediatrica 2015, 104, 974–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cresi, F.; Maggiora, E.; Pirra, A.; Tonetto, P.; Rubino, C.; Cavallarin, L.; Giribaldi, M.; Moro, G.E.; Peila, C.; Coscia, A. Effects on Gastroesophageal Reflux of Donkey Milk-Derived Human Milk Fortifier Versus Standard Fortifier in Preterm Newborns: Additional Data from the FortiLat Study. Nutrients 2020, 12, 2142. [Google Scholar] [CrossRef]
- Giribaldi, M.; Peila, C.; Coscia, A.; Cavallarin, L.; Antoniazzi, S.; Corbu, S.; Maiocco, G.; Sottemano, S.; Cresi, F.; Moro, G.E.; et al. Urinary Metabolomic Profile of Preterm Infants Receiving Human Milk with Either Bovine or Donkey Milk-Based Fortifiers. Nutrients 2020, 12, 2247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| BF-arm N = 54 | DF-arm N = 49 | ||
|---|---|---|---|
| Boys | n (%) | 25 (46.3) | 24 (49.0) |
| GA < 32 weeks | n (%) | 44 (81.5) | 33 (67.4) |
| GA (days) | median (IQR) | 209 (193–218) | 221 (210–226) |
| Minor Neurological Sequelae | n (%) | 7 (13.0) | 9 (18.4) |
| Major Neurological Sequelae | n (%) | 0 (0.0) | 1 (2.0) |
| Broncho Pulmonary Dysplasia | n (%) | 9 (16.7) | 3 (6.1) |
| RDS | n (%) | 47 (87.0) | 40 (81.6) |
| Intraventricular hemorrhage | n (%) | 6 (11.1) | 3 (6.1) |
| Periventricular leukomalacia | n (%) | 0 (0.0) | 0 (0.0) |
| Patent Ductus Arteriosus | n (%) | 17 (31.5) | 7 (14.3) |
| Fetal Growth Restriction | n (%) | 17 (32.1) | 25 (51.0) |
| Retinopathy of prematurity | n (%) | 9 (16.7) | 4 (8.2) |
| Necrotizing Enterocolitis | n (%) | 0 (0.0) | 0 (0.0) |
| Length of stay | median (IQR) | 44.5 (32–70) | 35 (29–51) |
| Birth head circumference * | |||
| cm | mean (SD) | 26.3 (2.29) | 27.0 (2.12) |
| z-score Int21s | mean (SD) | −0.54 (1.00) | −1.07 (1.04) |
| <10th centile Int21st | n (%) | 16 (30.2) | 21 (42.9) |
| >90th centile Int21st | n (%) | 1 (1.9) | 0 (0.0) |
| z−score INeS | mean (SD) | −0.32 (1.07) | −0.97 (1.13) |
| <10th centile INeS | n (%) | 12 (22.2) | 20 (40.8) |
| >90th centile INeS | n (%) | 4 (7.4) | 2 (3.9) |
| Birth length ** | |||
| cm | 36.6 (3.03) | 37.5 (2.73) | |
| z-score Int21s | mean (SD) | −1.00 (0.87) | −1.59 (1.23) |
| <10th centile Int21st | n (%) | 15 (35.7) | 23 (59.0) |
| >90th centile Int21st | n (%) | 0 (0.0) | 0 (0.0) |
| z-score INeS | mean (SD) | −0.58 (1.00) | −1.26 (1.28) |
| <10th centile INeS | n (%) | 11 (25.6) | 20 (51.3) |
| >90th centile INeS | n (%) | 1 (2.3) | 2 (5.1) |
| Birth weight | |||
| g | mean (SD) | 1116 (310.0) | 1192 (290.5) |
| z-score Int21s | mean (SD) | −0.78 (1.13) | −1.37 (1.12) |
| <10th centile Int21st (SGA) | n (%) | 21 (39.6) | 27 (55.1) |
| >90th centile Int21st (LGA) | n (%) | 1 (1.9) | 0 (0.0) |
| z-score INeS | mean (SD) | −0.41 (1.10) | −1.03 (1.06) |
| <10th centile INeS (SGA) | n (%) | 14 (25.9) | 21 (42.9) |
| >90th centile INeS (LGA) | n (%) | 3 (5.6) | 0 (0.0) |
| Parameter | Intergrowth 21st | INeS | ||
|---|---|---|---|---|
| Estimate ± SE | p | Estimate ± SE | p | |
| Intercept | 302.5 ± 94.5 | 0.0019 | 291.7 ± 91.9 | <0.0001 |
| Arm: DF vs. BF | −11.9 ± 8.9 | 0.1853 | −11.9 ± 8.9 | 0.1857 |
| Birth head (z−score) | 1.77 ± 4.84 | 0.7160 | 1.78 ± 4.38 | 0.6857 |
| BPD: yes vs. no | −4.30 ± 16.19 | 0.7911 | −5.17 ± 15.94 | 0.7466 |
| Minor neurological sequelae: yes vs. no | −35.0 ± 12.2 | 0.0051 | −34.2 ± 12.0 | 0.0053 |
| GA (weeks) | 2.84 ± 2.90 | 0.3310 | 3.15 ± 2.83 | 0.2680 |
| Population: GA < 32 wks vs. GA ≥ 32 wks | −4.29 ± 14.8 | 0.7733 | −3.22 ± 14.4 | 0.8236 |
| <Q1 | ≥Q1 | |
|---|---|---|
| BF-arm | 13 | 41 |
| DF-arm | 16 | 33 |
| Intergrowth21st | INeS | |||
|---|---|---|---|---|
| OR [CI (95%)] | p | OR [CI (95%)] | p | |
| Arm: DF vs. BF | 1.887 (0.665; 5.352) | 0.2325 | 1.941 (0.680; 5.540) | 0.2152 |
| Birth head (z-score) | 0.832 (0.476; 1.452) | 0.5171 | 0.898 (0.545; 1.480) | 0.6743 |
| BPD: yes vs. no | 2.007 (0.371; 10.863) | 0.4190 | 2.312 (0.437; 12.223) | 0.2824 |
| Minor neurological sequelae: yes vs. no | 4.319 (1.267; 14.726) | 0.0194 | 3.930 (1.174;13.159) | 0.0264 |
| GA (weeks) | 0.872 (0.625; 1.215) | 0.4173 | 0.839 (0.609; 1.156) | 0.3239 |
| Population: GA < 32 wks vs. GA ≥ 32 wks | 0.655 (0.121; 3.546) | 0.6232 | 0.520 (0.102;2.660) | 0.4327 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peila, C.; Spada, E.; Deantoni, S.; Iuliano, E.; Moro, G.E.; Giribaldi, M.; Cavallarin, L.; Cresi, F.; Coscia, A. The “Fortilat” Randomized Clinical Trial Follow-Up: Neurodevelopmental Outcome at 18 Months of Age. Nutrients 2020, 12, 3807. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123807
Peila C, Spada E, Deantoni S, Iuliano E, Moro GE, Giribaldi M, Cavallarin L, Cresi F, Coscia A. The “Fortilat” Randomized Clinical Trial Follow-Up: Neurodevelopmental Outcome at 18 Months of Age. Nutrients. 2020; 12(12):3807. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123807
Chicago/Turabian StylePeila, Chiara, Elena Spada, Sonia Deantoni, Ester Iuliano, Guido E. Moro, Marzia Giribaldi, Laura Cavallarin, Francesco Cresi, and Alessandra Coscia. 2020. "The “Fortilat” Randomized Clinical Trial Follow-Up: Neurodevelopmental Outcome at 18 Months of Age" Nutrients 12, no. 12: 3807. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123807