Effect of Extra Virgin Olive Oil and Traditional Brazilian Diet on the Bone Health Parameters of Severely Obese Adults: A Randomized Controlled Trial

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
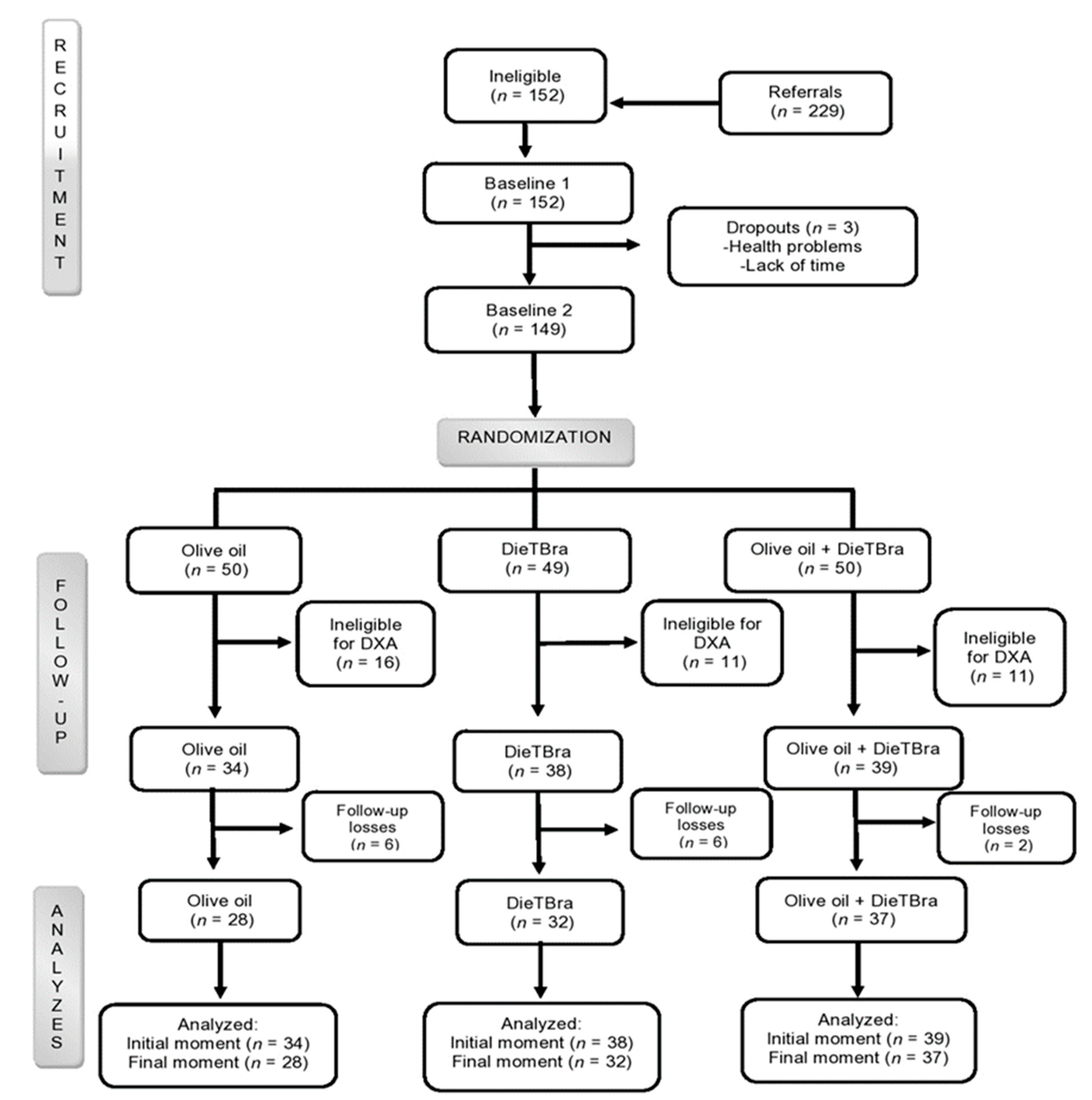
2.1. Design and Recruitment of Participants
2.2. Sample Calculation, Randomization, and Blinding
2.3. Sociodemographic, Lifestyle, and Medical Conditions
2.4. Biochemical Tests, Anthropometry, and Dietary Intake
2.5. Bone Mineral Density and Body Composition
2.6. Statistical Analysis
2.7. Quality Control
2.8. Ethical Aspects and RCT Registration
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Collaboration, N.R.F. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 192 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- World Health Organization. World Health Statistics 2012 [Internet]; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- El Hage, R.; Bachour, F.; Khairallah, W.; Bedran, F.; Maalouf, N.; Zakhem, E.; Issa, M.; Adib, G.; Maalouf, G. The influence of obesity and overweight on hip bone mineral density in Lebanese women. J. Clin. Densitom. 2014, 17, 216–217. [Google Scholar] [CrossRef] [PubMed]
- Cawsey, S.; Padwal, R.; Sharma, A.; Wang, X.; Li, S.; Siminoski, K. Women with severe obesity and relatively low bone mineral density have increased fracture risk. Osteoporos. Int. 2015, 26, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Shapses, S.A.; Pop, L.C.; Wang, Y. Obesity is a concern for bone health with aging. Nutr. Res. 2017, 39, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savvidis, C.; Tournis, S.; Dede, A.D. Obesity and bone metabolism. Hormones 2018, 17, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Ferrari, S.L. IOF Compendium of Osteoporosis. 2017. Available online: https://archive-ouverte.unige.ch/unige:125569 (accessed on 23 December 2019).
- Abdelmagid, S.M.; Barbe, M.F.; Safadi, F.F. Role of inflammation in the aging bones. Life Sci. 2015, 123, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Greco, E.A.; Lenzi, A.; Migliaccio, S. The obesity of bone. Ther. Adv. Endocrinol. Metab. 2015, 6, 273–286. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Huang, H.; Li, B.; Wu, D.; Wang, F.; Zheng, X.H.; Chen, Q.; Wu, B.; Fan, X. Olive oil in the prevention and treatment of osteoporosis after artificial menopause. Clin. Interv. Aging 2014, 9, 2087. [Google Scholar] [CrossRef] [Green Version]
- Tagliaferri, C.; Davicco, M.-J.; Lebecque, P.; Georgé, S.; Amiot, M.-J.; Mercier, S.; Dhaussy, A.; Huertas, A.; Walrand, S.; Wittrant, Y. Olive oil and vitamin D synergistically prevent bone loss in mice. PLoS ONE 2014, 9, e115817. [Google Scholar] [CrossRef] [Green Version]
- Mazzanti, L.; Battino, M.; Nanetti, L.; Raffaelli, F.; Alidori, A.; Sforza, G.; Carle, F.; Quagliarini, V.; Cester, N.; Vignini, A. Effect of 1-year dietary supplementation with vitaminized olive oil on markers of bone turnover and oxidative stress in healthy post-menopausal women. Endocrine 2015, 50, 326–334. [Google Scholar] [CrossRef]
- Chin, K.-Y.; Ima-Nirwana, S. Olives and bone: A green osteoporosis prevention option. Int. J. Environ. Res. Public Health 2016, 13, 755. [Google Scholar] [CrossRef] [PubMed]
- García-Gavilán, J.F.; Bulló, M.; Canudas, S.; Martínez-González, M.A.; Estruch, R.; Giardina, S.; Fito, M.; Corella, D.; Ros, E.; Salas-Salvado, J. Extra virgin olive oil consumption reduces the risk of osteoporotic fractures in the PREDIMED trial. Clin. Nutr. 2018, 37, 329–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncero-Martín, R.; Aliaga Vera, I.; Moreno-Corral, L.; Moran, J.; Lavado-Garcia, J.; Pedrera-Zamorano, J.; Pedrera-Canal, M. Olive oil consumption and bone microarchitecture in Spanish women. Nutrients 2018, 10, 968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Rey, J.; Roncero-Martín, R.; Rico-Martín, S.; Rey-Sánchez, P.; Pedrera-Zamorano, J.D.; Pedrera-Canal, M.; López-Espuela, F.; Lavado García, J.M. Adherence to a Mediterranean Diet and bone mineral density in Spanish premenopausal women. Nutrients 2019, 11, 555. [Google Scholar] [CrossRef] [Green Version]
- Silva, T.D.; Martins, C.; Ferreira, L.; Spritzer, P. Mediterranean diet is associated with bone mineral density and muscle mass in postmenopausal women. Climacteric 2019, 22, 162–168. [Google Scholar] [CrossRef]
- International Council Olive. Health Benefits of Olives and Olive Oil [Internet]; ICO: Madrid, Spain, 2012. [Google Scholar]
- Hagiwara, K.; Goto, T.; Araki, M.; Miyazaki, H.; Hagiwara, H. Olive polyphenol hydroxytyrosol prevents bone loss. Eur. J. Pharmacol. 2011, 662, 78–84. [Google Scholar] [CrossRef]
- Kim, T.-H.; Jung, J.W.; Ha, B.G.; Hong, J.M.; Park, E.K.; Kim, H.-J.; Kim, S.-Y. The effects of luteolin on osteoclast differentiation, function in vitro and ovariectomy-induced bone loss. J. Nutr. Biochem. 2011, 22, 8–15. [Google Scholar] [CrossRef]
- Pérez, A.R.; Velasco, A.R. Adherence to Mediterranean diet and bone health. Nutr. Hosp. 2014, 29, 989–996. [Google Scholar]
- Đudarić, L.; Fužinac-Smojver, A.; Muhvić, D.; Giacometti, J. The role of polyphenols on bone metabolism in osteoporosis. Food Res. Int. 2015, 77, 290–298. [Google Scholar] [CrossRef]
- Ministério da Saúde (Brasil). Guia alimentar para a população brasileira; Ministério da Saúde: Rio de Janeiro, Brazil, 2014.
- Batista Filho, M.; Rissin, A. A transição nutricional no Brasil: Tendências regionais e temporais. Cad. Saude Publica 2003, 19, S181–S191. [Google Scholar] [CrossRef]
- Rodrigues, A.P.D.S.; Rosa, L.P.S.; Silva, H.D.D.; Silveira-Lacerda, E.D.P.; Silveira, E.A. The single nucleotide polymorphism PPARG2 pro12ALA affects body mass index, fat mass, and blood pressure in severely obese patients. J. Obes. 2018, 2018, 2743081. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.P.S.; Rosa, L.P.S.; Silveira, E.A. PPARG2 Pro12Ala polymorphism influences body composition changes in severely obese patients consuming extra virgin olive oil: A randomized clinical trial. Nutr. Metab. 2018, 15, 52. [Google Scholar] [CrossRef] [PubMed]
- De Siqueira, R.A.; Rodrigues, A.P.D.S.; Miamae, L.M.; Tomimori, E.K.; Silveira, E.A. Thyroid nodules in severely obese patients: Frequency and risk of malignancy on ultrasonography. Endocr. Res. 2019, 45, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.; Rodrigues, A.P.S.; Rosa, L.P.S.; Sarrafzadegan, N.; Silveira, E.A. Cardiometabolic risk factors and Framingham Risk Score in severely obese patients: Baseline data from DieTBra trial. Nutr. Metab. Cardiovasc. Dis. 2019. [Google Scholar] [CrossRef]
- United Nations. Department of Economic and Social Affairs, Population Division. World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; Technical Report, Working Paper No. 241; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Pocock, S.J. Clinical Trials: A Practical Approach; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Satija, A.; Yu, E.; Willett, W.C.; Hu, F.B. Understanding nutritional epidemiology and its role in policy. Adv. Nutr. 2015, 6, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Sichieri, R.; Coitinho, D.C.; Monteiro, J.B.; Coutinho, W.F. Recomendações de alimentação e nutrição saudável para a população brasileira. Arq. Bras. Endocrinol. Metabol. 2000, 44, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Sartorelli, D.S.; Franco, L.J. Tendências do diabetes mellitus no Brasil: O papel da transição nutricional. Cad. Saude Publica 2003, 19, S29–S36. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Sustainable Healthy Diets: Guiding Principles; Food and Agriculture Organization: Rome, Italy, 2019. [Google Scholar]
- Horie, L.M.; Gonzalez, M.C.; Torrinhas, R.S.; Cecconello, I.; Waitzberg, D.L. New specific equation to estimate resting energy expenditure in severely obese patients. Obesity 2011, 19, 1090–1094. [Google Scholar] [CrossRef]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy balance and obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; Academic Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Bouchard, C.; Tremblay, A.; Leblanc, C.; Lortie, G.; Savard, R.; Theriault, G. A method to assess energy expenditure in children and adults. Am. J. Clin. Nutr. 1983, 37, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A. Are defects in energy expenditure involved in the causation of obesity? Obes. Rev. 2007, 8, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Thomazella, M.C.D.; Góes, M.F.; Andrade, C.R.; Debbas, V.; Barbeiro, D.F.; Correia, R.L.; Marie, S.K.; Cardounel, A.J.; Laurindo, F.R. Effects of high adherence to mediterranean or low-fat diets in medicated secondary prevention patients. Am. J. Cardiol. 2011, 108, 1523–1529. [Google Scholar] [CrossRef] [Green Version]
- Kontogianni, M.D.; Vlassopoulos, A.; Gatzieva, A.; Farmaki, A.-E.; Katsiougiannis, S.; Panagiotakos, D.B.; Kalogeropoulos, N.; Skopouli, F.N. Flaxseed oil does not affect inflammatory markers and lipid profile compared to olive oil, in young, healthy, normal weight adults. Metabolism 2013, 62, 686–693. [Google Scholar] [CrossRef]
- Pan American Health Organization. Guias para el control y monitoreo de la epidemia tabaquica; OMS: Geneva, Switzerland, 1995. [Google Scholar]
- Bloomfield, K.; Allamani, A.; Beck, F.; Bergmark, K.H.; Csemy, L.; Eisenbach-Stangl, I.; Elekes, Z.; Gmel, G.; Kerr-Correa, F.; Knibbe, R. Gender, Culture and Alcohol Problems: A Multi-National Study: Project Final Report; Charité Campus Benjamin Franklin: Berlin, Germany, 2005. [Google Scholar]
- World Health Organization. World Health Statistics 2010; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Dillon, C.B.; Fitzgerald, A.P.; Kearney, P.M.; Perry, I.J.; Rennie, K.L.; Kozarski, R.; Phillips, C.M. Number of days required to estimate habitual activity using wrist-worn GENEActiv accelerometer: A cross-sectional study. PLoS ONE 2016, 11, e0109913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazziotti, G.; Canalis, E.; Giustina, A. Drug-induced osteoporosis: Mechanisms and clinical implications. Am. J. Med. 2010, 123, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Panday, K.; Gona, A.; Humphrey, M.B. Medication-induced osteoporosis: Screening and treatment strategies. Ther. Adv. Musculoskelet Dis. 2014, 6, 185–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human kinetics books Champaign: Champaign, IL, USA, 1988. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Steinfeldt, L.; Anand, J.; Murayi, T. Food reporting patterns in the USDA automated multiple-pass method. Procedia Food Sci. 2013, 2, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Barreira, T.V.; Harrington, D.M.; Staiano, A.E.; Heymsfield, S.B.; Gimble, J.M. Relationship between abdominal fat and bone mineral density in white and African American adults. Bone 2012, 50, 576–579. [Google Scholar] [CrossRef] [Green Version]
- Agranonik, M.; Machado, L.R. Análise de covariância: Uma aplicação a dados de função pulmonar, ajustados por idade. Revista. HCPA 2011, 31, 248–253. [Google Scholar]
- Tai, V.; Leung, W.; Grey, A.; Reid, I.R.; Bolland, M.J. Calcium intake and bone mineral density: Systematic review and meta-analysis. BMJ 2015, 351, h4183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivas, A.; Romero, A.; Mariscal-Arcas, M.; Monteagudo, C.; Feriche, B.; Lorenzo, M.L.; Olea, F. Mediterranean diet and bone mineral density in two age groups of women. Int. J. Food Sci. Nutr. 2013, 64, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Denova-Gutiérrez, E.; Clark, P.; Tucker, K.; Muñoz-Aguirre, P.; Salmerón, J. Dietary patterns are associated with bone mineral density in an urban Mexican adult population. Osteoporos Int. 2016, 27, 3033–3040. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Prince, R.L. Calcium and bone. Clin. Biochem. 2012, 45, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Hassoon, A.; Michos, E.; Miller, E.; Crisp, Z.; Appel, L. Effects of different dietary interventions on calcitriol, parathyroid hormone, calcium, and phosphorus: Results from the DASH Trial. Nutrients 2018, 10, 367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Real, J.M.; Bulló, M.; Moreno-Navarrete, J.M.; Ricart, W.; Ros, E.; Estruch, R.; Salas-Salvado, J. A Mediterranean diet enriched with olive oil is associated with higher serum total osteocalcin levels in elderly men at high cardiovascular risk. J. Clin. Endocrinol. Metab. 2012, 97, 3792–3798. [Google Scholar] [CrossRef]
- Wolf, R.L.; Cauley, J.A.; Baker, C.E.; Ferrell, R.E.; Charron, M.; Caggiula, A.W.; Salamone, L.M.; Heaney, R.P.; Kuller, L.H. Factors associated with calcium absorption efficiency in pre-and perimenopausal women. Am. J. Clin. Nutr. 2000, 72, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Johns, D.J.; Lindroos, A.K.; Jebb, S.A.; Sjöström, L.; Carlsson, L.M.; Ambrosini, G.L. Dietary patterns, cardiometabolic risk factors, and the incidence of cardiovascular disease in severe obesity. Obesity 2015, 23, 1063–1070. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [CrossRef]
- Waterman, E.; Lockwood, B. Active components and clinical applications of olive oil. Altern. Med. Rev. 2007, 12, 331–342. [Google Scholar]
- Bueno, J.M.; Leal, F.S.; Saquy, L.P.L.; Santos, C.B.D.; Ribeiro, R.P.P. Educação alimentar na obesidade: Adesão e resultados antropométricos. Rev. Nutrição 2011, 24, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Cashman, K.D. Diet, nutrition, and bone health. J. Nutr. 2007, 137, 2507S–2512S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, C.M.; Miller, J.W. Challenges in conducting clinical nutrition research. Nutr. Rev. 2017, 75, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxoford, UK, 2012. [Google Scholar]
- Aued-Pimentel, S. Olive Oil in Brazil: Economic and Regulatory Control Aspects. Products from Olive Tree; Intech Open Science: London, UK, 2016. [Google Scholar] [CrossRef] [Green Version]
- Kouli, G.-M.; Panagiotakos, D.B.; Kyrou, I.; Magriplis, E.; Georgousopoulou, E.N.; Chrysohoou, C.; Tsigos, C.; Tousoulis, D.; Pitsavos, C. Olive oil consumption and 10-year (2002–2012) cardiovascular disease incidence: The ATTICA study. Eur. J. Nutr. 2019, 58, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Total n (%) | Olive Oil (n = 34) n (%) | DieTBra (n = 38) n (%) | Olive Oil + DieTBra (n = 39) n (%) |
|---|---|---|---|---|
| Sex * | ||||
| Women | 104 (93.7) | 32 (94.1) | 36 (94.7) | 36 (92.3) |
| Men | 7 (6.3) | 2 (5.9) | 2 (5.3) | 3 (7.7) |
| Age (years) ** | ||||
| 18–40 | 57 (51.4) | 19 (55.9) | 21 (55.3) | 17 (43.6) |
| ≥41 | 54 (48.6) | 15 (44.1) | 17 (44.7) | 22 (56.4) |
| Skin color ** | ||||
| White/dark | 94 (84.7) | 29 (85.3) | 33 (86.8) | 32 (82.0) |
| Black | 17 (15.3) | 5 (14.7) | 5 (13.2) | 7 (18.0) |
| Formal education (years of study) ** | ||||
| ≤4 | 10 (9.0) | 1 (2.9) | 2 (5.3) | 7 (17.9) |
| 5–11 | 83 (74.8) | 27 (79.4) | 30(78.9) | 26 (66.7) |
| ≥12 | 18 (16.2) | 6 (17.7) | 6(15.8) | 6 (15.4) |
| Economic class ** | ||||
| A-B | 28 (25.2) | 12 (35.3) | 7 (18.4) | 9 (23.1) |
| C | 65 (58.6) | 15 (44.1) | 24 (63.2) | 26 (66.7) |
| D-E | 18 (16.2) | 7 (20.6) | 7 (18.4) | 4(10.2) |
| Smoking** | ||||
| Never smoked | 76 (68.5) | 25 (73.5) | 27 (71.0) | 24 (61.5) |
| Smoker/ex-smoker | 35 (31.5) | 9 (26.5) | 11 (29.0) | 15 (38.5) |
| Binge drinking (n = 62) ** | ||||
| Yes | 32 (51.6) | 9 (50.0) | 10 (47.6) | 13 (56.5) |
| No | 30 (48.4) | 9 (50.0) | 11 (52.4) | 10 (43.5) |
| Menopause (n = 104) * | ||||
| Yes | 18 (16.2) | 6 (18.7) | 3 (8.3) | 9 (25.0) |
| No | 86 (77.5) | 26 (81.3) | 33 (91.7) | 27 (75.0) |
| Drugs↓BMD ** | ||||
| Yes | 28 (25.2) | 6 (17.6) | 8 (21.1) | 14 (35.9) |
| No | 83 (74.8) | 28 (82.4) | 30 (78.9) | 25 (64.1) |
| PA ≥150 min/week (n = 104) * | ||||
| Yes | 99 (95.2) | 30 (93.8) | 35 (97.2) | 34 (94.5) |
| No | 4 (4.8) | 2 (6.2) | 1 (2.8) | 2 (5.6) |
| BMI (kg/m2) * | ||||
| 35–39.99 | 22 (19.8) | 7 (20.6) | 8 (21.1) | 7 (18.0) |
| 40–49.99 | 78 (70.3) | 25 (73.5) | 23 (60.5) | 30 (76.9) |
| >50 | 11(9.9) | 2 (5.9) | 7 (18.4) | 2 (5.1) |
| Weight (mean kg ± SD) *** | 110.211.6 | 108.0 ± 10.9 | 111.7 ± 12.1 | 110.7 ± 11.8 |
| Fat mass (mean kg ± SD) *** | 51.6 ± 5.2 | 50.5 ± 5.1 | 51.5 ± 4.7 | 52.6 ± 5.6 |
| Lean mass (mean kg ± SD) | 50.7 ± 9.1 | 47.9 ± 11.1 | 51.9 ± 7.6 | 50.4 ± 8.5 |
| Outcomes | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD |
| BMD spine (g/cm2) *** | 1.069 ± 0.165 | 1.053 ± 0.136 | 1.119 ± 0.166 | 1.035 ± 0.180 |
| BMD hip (g/cm2) *** | 1.201 ± 0.143 | 1.182 ± 0.139 | 1.236 ± 0.120 | 1.183 ± 0.162 |
| Serum calcium (mg/dL) *** | 9.5 ± 0.5 | 9.4 ± 0.5 | 9.6 ± 0.6 | 9.4 ± 0.41 |
| Serum vitamin D (ng/mL) *** | 30.5 ± 9.6 | 30.8 ± 9.5 | 29.16 ± 9.2 | 31.5 ± 10.1 |
| PTH (pg/mL) *** | 53.7 ± 26.0 | 55.0 ± 20.7 | 57.9 ± 35.9 | 48.5 ± 16.5 |
| Dietary calcium (mg/day) *** | 417.2 ± 222.6 | 375.5 ± 213.0 | 445.0 ± 210.9 | 426.5 ± 241.5 |
| Dietary vitamin D (µcg/day) *** | 2.1 ± 1.8 | 1.8 ± 1.6 | 2.4 ± 1.6 | 2.1 ± 2.2 |
| Energy intake (kcal/day) **** | 1685.1 ± 762.1 | 1674.8 ± 610.8 | 1678.1 ± 568.2 | 1701.1 ± 1021.1 |
| Protein intake (% TEV) *** | 18.0 ± 4.8 | 18.1 ± 4.3 | 17.3 ± 5.1 | 18.7 ± 4.7 |
| Olive Oil | DieTBra | Olive Oil + DieTBra | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||||||
| Outcomes | Before (n = 34) | After (n = 28) | p * | Before (n = 38) | After (n = 32) | p * | Before (n = 39) | After (n = 37) | p * |
| BMD spine total (g/cm2) | 1.053 ± 0.136 | 1.092 ± 0.139 | 0.269 | 1.119 ± 0.166 | 1.145 ± 0.157 | 0.512 | 1.035 ± 0.179 | 1.044 ± 0.177 | 0.806 |
| BMD hip total (g/cm2) | 1.183 ± 0.139 | 1.214 ± 0.125 | 0.364 | 1.236 ± 0.119 | 1.244 ± 0.151 | 0.792 | 1.183 ± 0.162 | 1.164 ± 0.149 | 0.588 |
| Serum calcium (mg/dL) | 9.5 ± 0.5 | 9.8 ± 0.5 | 0.007 | 9.5 ± 0.5 | 9.6 ± 0.6 | 0.622 | 9.4 ± 0.4 | 9.5 ± 0.5 | 0.330 |
| Vit. D serum (ng/mL) | 30.8 ± 9.5 | 31.3 ± 9.8 | 0.823 | 29.2 ± 9.2 | 31.7 ± 9.7 | 0.255 | 31.5 ± 10.1 | 31.5 ± 9.9 | 0.998 |
| PTH (pg/ml) | 55.0 ± 20.7 | 45.9 ± 16.4 | 0.065 | 57.9 ± 35.9 | 44.6 ± 13.6 | 0.047 | 48.5 ± 16.5 | 47.5 ± 15.2 | 0.791 |
| Dietary calcium (mg/day) | 375.5 ± 213.0 | 362.4 ± 257.4 | 0.819 | 445.0 ± 210.9 | 341.1 ± 263.6 | 0.061 | 426.5 ± 241.5 | 358.0 ± 238.2 | 0.211 |
| Dietary vitamin D (µcg/day) | 1.8 ± 1.4 | 1.9 ± 2.1 | 0.710 | 2.6 ± 1.9 | 3.3 ± 3.6 | 0.214 | 2.1 ± 2.0 | 1.9 ± 1.9 | 0.773 |
| Energy intake (kcal/day) | 1674.8 ± 610.8 | 1529.9 ± 885.0 | 0.434 | 1678.1 ± 568.2 | 1104.1 ± 609.7 | 0.000 | 1701.1 ± 1021.1 | 1397.3 ± 567.0 | 0.108 |
| Protein intake (%TEV) | 18.1 ± 4.3 | 13.2 ± 7.1 | 0.001 | 17.3 ± 5.1 | 15.9 ± 8.6 | 0.374 | 18.7 ± 4.7 | 14.9 ± 7.2 | 0.007 |
| Olive Oil (n = 28) | DieTBra (n = 32) | Olive Oil + DieTBra (n = 37) | All | Olive Oil × DieTBra | Olive Oil × Olive Oil + DieTBra | DieTBra × Olive Oil + DieTBra | |
|---|---|---|---|---|---|---|---|
| Outcomes | Mean ± SD | Mean ± SD | Mean ± SD | p | p | p | p |
| BMD spine total (g/cm2) | 1.092 ± 0.139 | 1.145 ± 0.157 a | 1.044 ± 0.177 a | 0.040 * | 0.178 *** | 0.246 *** | 0.016 *** |
| BMD hip total (g/cm2) | 1.214 ± 0.125 | 1.244 ± 0.151 | 1.164 ± 0.149 | 0.066 * | 0.397 *** | 0.157 *** | 0.029 *** |
| Serum calcium (mg/dL) | 9.8 ± 0.5 | 9.6 ± 0.6 | 9.5 ± 0.5 | 0.092 * | 0.137 *** | 0.026 *** | 0.535 *** |
| Vit. D serum (ng/mL) | 31.3 ± 9.8 | 31.7 ± 9.7 | 31.5 ± 9.9 | 0.988 * | 0.879 *** | 0.947 *** | 0.926 *** |
| PTH (pg/mL) | 45.9 ± 16.4 | 44.6 ± 13.6 | 47.5 ± 15.2 | 0.721 * | 0.710 *** | 0.688 *** | 0.404 *** |
| Dietary calcium (mg/day) | 362.4 ± 257.4 | 341.1 ± 263.6 | 358.0 ± 238.2 | 0.930 * | 0.731 *** | 0.940 *** | 0.768 *** |
| Dietary vitamin D (µcg/day) | 1.9 ± 2.1 | 3.3 ± 3.6 | 1.9 ± 1.9 | 0.257 ** | 0.220 **** | 0.712 **** | 0.124 **** |
| Energy intake (kcal/day) | 1529.9 ± 885.0 a | 1104.1 ± 609.7 a,b | 1397.3 ± 567.0 b | 0.002 ** | 0.019 *** | 0.443 *** | 0.031 *** |
| Protein intake (%TEV) | 13.2 ± 7.1 | 15.9 ± 8.6 | 14.9 ± 7.2 | 0.336 * | 0.157 *** | 0.315 *** | 0.593 *** |
| Olive Oil (n = 28) | DieTBra (n = 32) | Olive Oil + DieTBra (n = 37) | All * | Olive Oil × DieTBra ** | Olive Oil × Olive Oil + DieTBra ** | DieTBra × Olive Oil + DieTBra ** | |
|---|---|---|---|---|---|---|---|
| Outcomes (Final-Initial) | Mean ± SD | Mean ± SD | Mean ± SD | p | p | p | p |
| ▲BMD spine (g/cm2) | 0.034 ± 0.116 | 0.043 ± 0.092 | 0.009 ± 0.111 | 0.399 * | 0.754 | 0.380 | 0.180 |
| ▲BMD hip (g/cm2) | 0.026 ± 0.111 | 0.009 ± 0.100 | −0.003 ± 0.109 | 0.556 * | 0.531 | 0.296 | 0.641 |
| ▲Serum calcium (mg/dL) | 0.4 ± 0.7 | −0.0 ± 0.8 | 0.1 ± 0.7 | 0.116 * | 0.051 | 0.122 | 0.536 |
| ▲ Serum Vit. D (ng/mL) | 0.1 ± 6.5 | 2.7 ± 8.4 | 0.7 ± 5.4 | 0.675 ** | 0.218 | 0.697 | 0.273 |
| ▲PTH (pg/mL) | −7.3 ± 20.7 | −12.6 ± 29.9 a | −1.2 ± 13.2 a | 0.10 ** | 0.431 | 0.158 | 0.042 |
| ▲Dietary calcium (mg/day) | −13.1 ± 294.8 | −103.8 ± 268.3 | −68.4 ± 218.4 | 0.337 * | 0.176 *** | 0.362 *** | 0.526 *** |
| ▲Dietary vitamin D (µcg/day) | 0.2 ± 2.9 | 0.9 ± 3.9 | −0.2 ± 2.4 | 0.831 ** | 0.458 *** | 0.448 *** | 0.129 *** |
| ▲Energy intake (kcal/day) | −144.8 ± 918.3 a | −573.9 ± 719.8 a | −303.7 ± 882.1 | 0.016 ** | 0.005 **** | 0.325 **** | 0.055 **** |
| ▲Protein intake (%TEV) | −4.9 ± 7.1 | −1.4 ± 10.2 | −3.8 ± 8.3 | 0.227 * | 0.105 *** | 0.560 *** | 0.265 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, C.K.d.S.; Santos, A.S.e.A.d.C.; Rosa, L.P.d.S.; Mendonça, C.R.; Vitorino, P.V.d.O.; Peixoto, M.d.R.G.; Silveira, É.A. Effect of Extra Virgin Olive Oil and Traditional Brazilian Diet on the Bone Health Parameters of Severely Obese Adults: A Randomized Controlled Trial. Nutrients 2020, 12, 403. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020403
Cardoso CKdS, Santos ASeAdC, Rosa LPdS, Mendonça CR, Vitorino PVdO, Peixoto MdRG, Silveira ÉA. Effect of Extra Virgin Olive Oil and Traditional Brazilian Diet on the Bone Health Parameters of Severely Obese Adults: A Randomized Controlled Trial. Nutrients. 2020; 12(2):403. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020403
Chicago/Turabian StyleCardoso, Camila Kellen de Souza, Annelisa Silva e Alves de Carvalho Santos, Lorena Pereira de Souza Rosa, Carolina Rodrigues Mendonça, Priscila Valverde de Oliveira Vitorino, Maria do Rosário Gondim Peixoto, and Érika Aparecida Silveira. 2020. "Effect of Extra Virgin Olive Oil and Traditional Brazilian Diet on the Bone Health Parameters of Severely Obese Adults: A Randomized Controlled Trial" Nutrients 12, no. 2: 403. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020403