Association of Neck Circumference with Anthropometric Indicators and Body Composition Measured by DXA in Young Spanish Adults

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neck Circumference Assessment
2.3. Anthropometric and Body Composition Measurements
2.4. Statistical Analysis
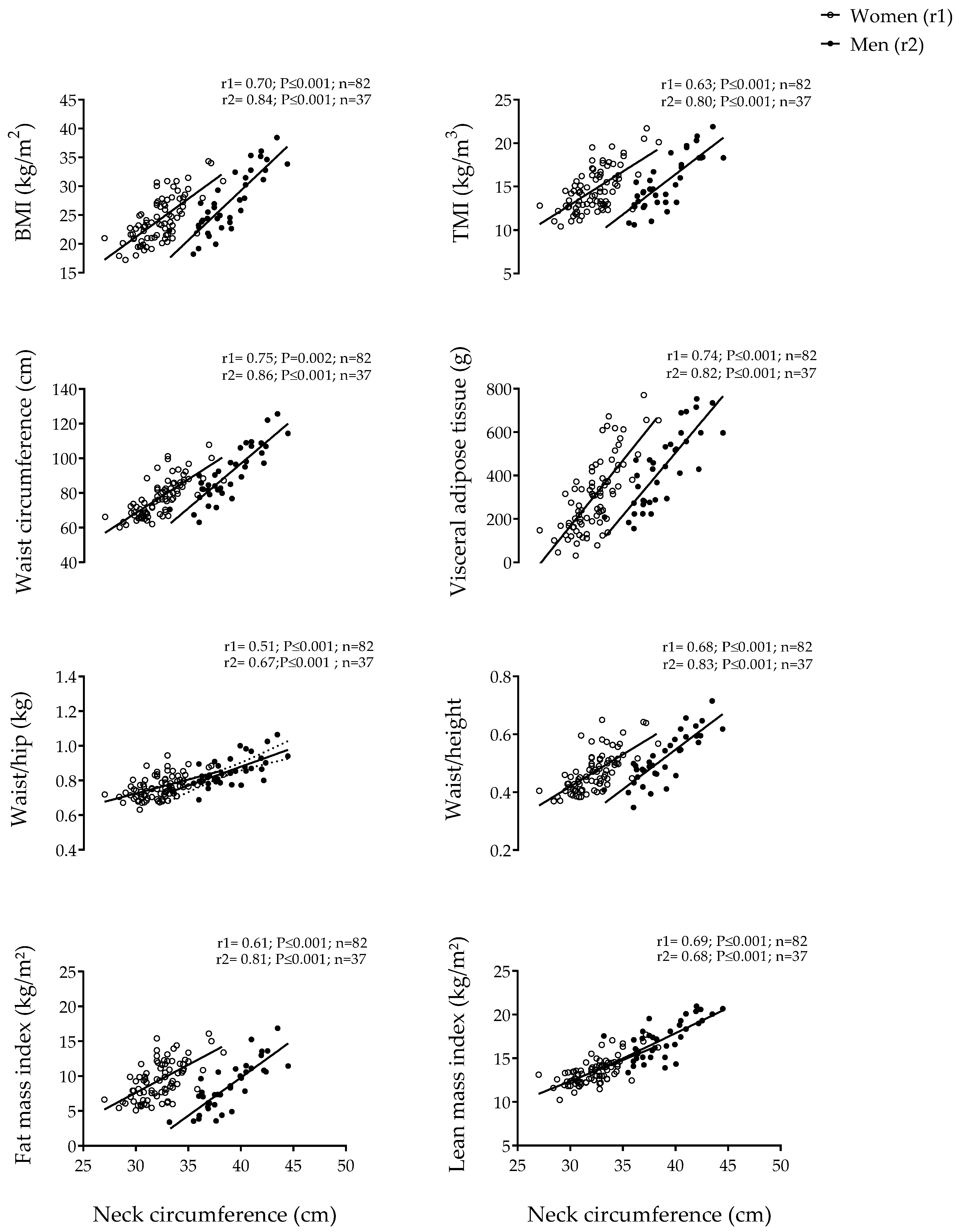
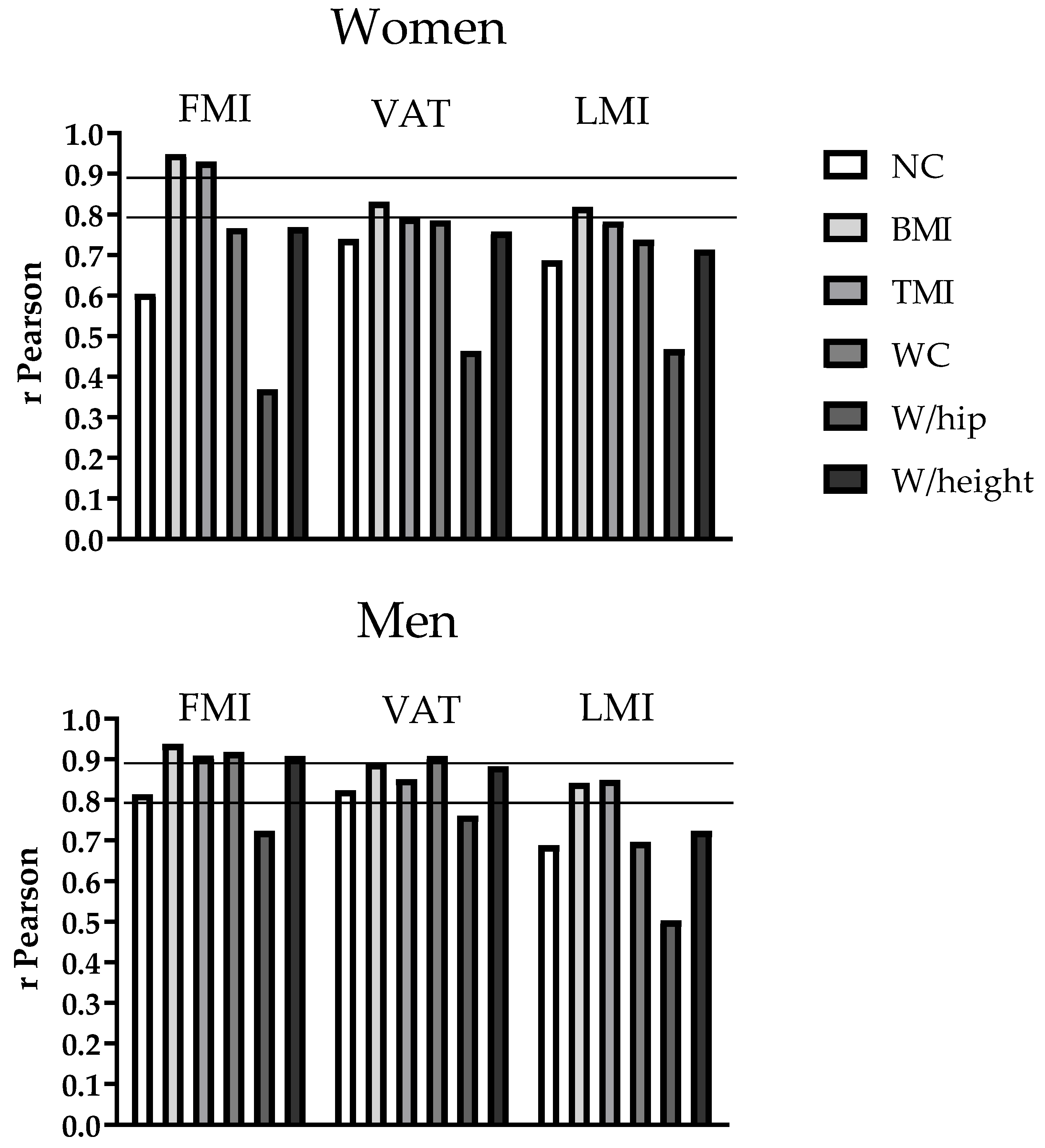
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Eurostat. Eurostat Regional Yearbook 2017. Available online: http://ec.europa.eu/eurostat/documents/3217494/8222062/KS-HA-17-001-EN-N.pdf/eaebe7fa-0c80-45af-ab41-0f806c433763 (accessed on 18 September 2017).
- World Health Organization. Nutrition—Controlling the Global Obesity Epidemic 2009. Available online: http://www.who.int/nutrition/topics/obesity/en/index.html (accessed on 29 September 2017).
- Halade, G.V.; Kain, V. Obesity and Cardiometabolic Defects in Heart Failure Pathology. Compr. Physiol. 2017, 7, 1463–1477. [Google Scholar] [PubMed]
- Pi-Sunyer, F.X.; Becker, D.M.; Bouchard, C.; Carleton, R.A.; Colditz, G.A.; Dietz, W.H.; Foreyt, J.P.; Garrison, R.J.; Grundy, S.M.; Hansen, B.C.; et al. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: Executive summary. Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Am. J. Clin. Nutr. 1998, 68, 899–917. [Google Scholar]
- Despres, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Despres, J.P. Body fat distribution and risk of cardiovascular disease: An update. Circulation 2012, 126, 1301–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Waist Circumference and Waist-hip Ratio: Report of a WHO Expert Consultation; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Parker, E.D.; Pereira, M.A.; Stevens, J.; Folsom, A.R. Association of hip circumference with incident diabetes and coronary heart disease: The Atherosclerosis Risk in Communities study. Am. J. Epidemiol. 2009, 169, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caan, B.; Armstrong, M.A.; Selby, J.V.; Sadler, M.; Folsom, A.R.; Jacobs, D.; Slattery, M.L.; Hilner, J.E.; Roseman, J. Changes in measurements of body fat distribution accompanying weight change. Int. J. Obes. Relat. Metab. Disord. 1994, 18, 397–404. [Google Scholar] [PubMed]
- Pandzic Jaksic, V.; Grizelj, D.; Livun, A.; Boscic, D.; Ajduk, M.; Kusec, R.; Jaksic, O. Neck adipose tissue-tying ties in metabolic disorders. Horm. Mol. Biol. Clin. Investig. 2018, 33. [Google Scholar] [CrossRef]
- Torriani, M.; Gill, C.M.; Daley, S.; Oliveira, A.L.; Azevedo, D.C.; Bredella, M.A. Compartmental neck fat accumulation and its relation to cardiovascular risk and metabolic syndrome. Am. J. Clin. Nutr. 2014, 100, 1244–1251. [Google Scholar] [CrossRef] [Green Version]
- Preis, S.R.; Massaro, J.M.; Hoffmann, U.; D’Agostino, R.B., Sr.; Levy, D.; Robins, S.J.; Meigs, J.B.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Neck circumference as a novel measure of cardiometabolic risk: The Framingham Heart study. J. Clin. Endocrinol. Metab. 2010, 95, 3701–3710. [Google Scholar] [CrossRef] [Green Version]
- Hingorjo, M.R.; Qureshi, M.A.; Mehdi, A. Neck circumference as a useful marker of obesity: A comparison with body mass index and waist circumference. J. Pak. Med. Assoc. 2012, 62, 36–40. [Google Scholar]
- Arias Tellez, M.J.; Martinez-Tellez, B.; Soto, J.; Sanchez-Delgado, G. Validity of neck circumference as a marker of adiposity in children and adolescents, and in adults: A systematic review. Nutr. Hosp. 2018, 35, 707–721. [Google Scholar] [PubMed]
- Kroll, C.; Mastroeni, S. The accuracy of neck circumference for assessing overweight and obesity: A systematic review and meta-analysis. Ann. Hum. Biol. 2017, 44, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Ben-Noun, L.L.; Laor, A. Relationship between changes in neck circumference and cardiovascular risk factors. Exp. Clin. Cardiol. 2006, 11, 14–20. [Google Scholar] [PubMed]
- Baena, C.P.; Lotufo, P.A.; Fonseca, M.G.; Santos, I.S.; Goulart, A.C.; Bensenor, I.M. Neck Circumference Is Independently Associated with Cardiometabolic Risk Factors: Cross-Sectional Analysis from ELSA-Brasil. Metab. Syndr. Relat. Disord. 2016, 14, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.R.; Yuan, S.Y.; Fu, H.J.; Wan, G.; Zhu, L.X.; Bu, X.L.; Zhang, J.D.; Du, X.P.; Li, Y.L.; Ji, Y.; et al. Neck circumference positively related with central obesity, overweight, and metabolic syndrome in Chinese subjects with type 2 diabetes: Beijing Community Diabetes Study 4. Diabetes Care 2010, 33, 2465–2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laakso, M.; Matilainen, V.; Keinanen-Kiukaanniemi, S. Association of neck circumference with insulin resistance-related factors. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 873–875. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Guo, Q.; Peng, L.; Li, J.; Gao, Y.; Yan, B.; Fang, B.; Wang, G. The association of neck circumference with incident congestive heart failure and coronary heart disease mortality in a community-based population with or without sleep-disordered breathing. BMC Cardiovasc. Disord. 2018, 18, 108. [Google Scholar] [CrossRef] [Green Version]
- Kurtoglu, S.; Hatipoglu, N.; Mazicioglu, M.M.; Kondolot, M. Neck circumference as a novel parameter to determine metabolic risk factors in obese children. Eur. J. Clin. Investig. 2012, 42, 623–630. [Google Scholar] [CrossRef]
- Ben-Noun, L.; Sohar, E.; Laor, A. Neck circumference as a simple screening measure for identifying overweight and obese patients. Obes. Res. 2001, 9, 470–477. [Google Scholar] [CrossRef]
- Rosenquist, K.J.; Therkelsen, K.E.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Development and reproducibility of a computed tomography-based measurement for upper body subcutaneous neck fat. J. Am. Heart Assoc. 2014, 3, e000979. [Google Scholar] [CrossRef] [Green Version]
- Cizza, G.; de Jonge, L.; Piaggi, P.; Mattingly, M.; Zhao, X.; Lucassen, E.; Rother, K.I.; Sumner, A.E.; Csako, G. NIDDK Sleep Extension Study. Neck circumference is a predictor of metabolic syndrome and obstructive sleep apnea in short-sleeping obese men and women. Metab. Syndr. Relat. Disord. 2014, 12, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Ravensbergen, H.R.; Lear, S.A.; Claydon, V.E. Waist circumference is the best index for obesity-related cardiovascular disease risk in individuals with spinal cord injury. J. Neurotrauma 2014, 31, 292–300. [Google Scholar] [CrossRef]
- Li, H.X.; Zhang, F.; Zhao, D.; Xin, Z.; Guo, S.Q.; Wang, S.M.; Zhang, J.J.; Wang, J.; Li, Y.; Yang, G.R.; et al. Neck circumference as a measure of neck fat and abdominal visceral fat in Chinese adults. BMC Public Health 2014, 14, 311. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Samarasinghe, Y.P.; Kane, P.; Amiel, S.A.; Aylwin, S.J.B. Visceral adiposity is closely correlated with neck circumference and represents a significant indicator of insulin resistance in WHO grade III obesity. Clin. Endocrinol. 2010, 73, 197–200. [Google Scholar] [CrossRef]
- Sanchez-Delgado, G.; Martinez-Tellez, B.; Olza, J.; Aguilera, C.M.; Labayen, I.; Ortega, F.B.; Chillon, P.; Fernandez-Reguera, C.; Alcantara, J.M.; Martinez-Avila, W.D.; et al. Activating brown adipose tissue through exercise (ACTIBATE) in young adults: Rationale, design and methodology. Contemp. Clin. Trials 2015, 45 (Pt B), 416–425. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.D.; de Ridder, J.H. International Standards for Anthropometric Assessment; Stewart, A., Marfell-Jones, M., Olds, T., Ridder, D.H., Eds.; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Ramirez-Velez, R.; Correa-Bautista, J.E.; Carrillo, H.A.; Gonzalez-Jimenez, E. Tri-Ponderal Mass Index vs. Fat Mass/Height(3) as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People. Nutrients 2018, 10, 412. [Google Scholar] [CrossRef] [Green Version]
- Hinton, B.J.; Fan, B.; Ng, B.K.; Shepherd, J.A. Dual energy X-ray absorptiometry body composition reference values of limbs and trunk from NHANES 1999-2004 with additional visualization methods. PLoS ONE 2017, 12, e0174180. [Google Scholar] [CrossRef]
- Castro-Pinero, J.; Delgado-Alfonso, A.; Gracia-Marco, L.; Gomez-Martinez, S.; Esteban-Cornejo, I.; Veiga, O.L.; Marcos, A.; Segura-Jiménez, V. Neck circumference and clustered cardiovascular risk factors in children and adolescents: Cross-sectional study. BMJ Open 2017, 7, e016048. [Google Scholar] [CrossRef]
- Onat, A.; Hergenc, G.; Yuksel, H.; Can, G.; Ayhan, E.; Kaya, Z.; Dursunoğlu, D. Neck circumference as a measure of central obesity: Associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin. Nutr. (Edinb. Scotl.) 2009, 28, 46–51. [Google Scholar] [CrossRef]
- Yan, Q.; Sun, D.; Li, X.; Zheng, Q.; Li, L.; Gu, C.; Feng, B. Neck circumference is a valuable tool for identifying metabolic syndrome and obesity in Chinese elder subjects: A community-based study. Diabetes/Metab. Res. Rev. 2014, 30, 69–76. [Google Scholar] [CrossRef]
- Assyov, Y.; Gateva, A.; Tsakova, A.; Kamenov, Z. A comparison of the clinical usefulness of neck circumference and waist circumference in individuals with severe obesity. Endocr. Res. 2017, 42, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.; Munoz-Torres, F.; Vergara, J.; Palacios, C.; Pérez, C.M. Neck Circumference May Be a Better Alternative to Standard Anthropometric Measures. J. Diabetes Res. 2016, 2016, 6058916. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| All (n = 119) | Women (n = 82) | Men (n = 37) | p | |
|---|---|---|---|---|
| Age (years) | 21.9 (2.3) | 21.8 (2.2) | 22.1 (2.4) | 0.488 |
| Weight (kg) | 71.7 (16.4) | 66.0 (11.6) | 84.9 (18.0) | <0.001 |
| Height (m) | 1.69 (8.5) | 1.65 (6.5) | 1.77 (6.3) | <0.001 |
| Neck circumference (cm) | 34.3 (3.8) | 32.3 (2.1) | 38.8 (2.6) | <0.001 |
| BMI (kg/m2) | 25.1 (4.6) | 24.1 (4.0) | 27.2 (5.3) | 0.003 |
| TMI (kg/m3) | 14.9 (2.7) | 14.7 (2.5) | 15.4 (3.0) | 0.193 |
| WC (cm) | 81.6 (13.8) | 77.4 (11) | 90.1 (15.3) | <0.001 |
| Waist/hip | 0.85 (0.1) | 0.80 (0.1) | 0.85 (0.1) | <0.001 |
| Waist/height | 0.48 (0.08) | 0.47 (0.07) | 0.52 (0.09) | 0.006 |
| Fat mass (kg) | 26.0 (8.8) | 26.0 (7.5) | 27.0 (11.3) | 0.594 |
| FMI (kg/m2) | 9.1 (3.0) | 9.4 (2.7) | 8.5 (3.5) | 0.124 |
| VAT (g) | 348.5 (181.8) | 307.4 (168.0) | 439.4 (181.0) | <0.001 |
| Lean mass (kg) | 42.0 (9.9) | 37.0 (5.0) | 53.7 (7.6) | <0.001 |
| LMI (kg/m2) | 14.6 (2.4) | 13.5 (1.5) | 17.2 (2.2) | <0.001 |
| WOMEN | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FMI | VAT | LMI | ||||||||||
| β | 95% CI | R2 | sr | β | 95% CI | R2 | sr | β | 95% CI | R2 | sr | |
| Univariable model | ||||||||||||
| - NC | 3.765 (0.554) *** | 2.662 to 4.867 | 0.358 | 282.857 (28.706) *** | 225.731 to 339.983 | 0.543 | 2.277 (0.270) *** | 1.741 to 2.813 | 0.465 | |||
| - BMI | 3.025 (0.112) *** | 2.801 to 3.248 | 0.899 | 162.546 (12.172) *** | 138.323 to 186.769 | 0.686 | 1.391 (0.109) *** | 1.175 to 1.608 | 0.667 | |||
| - TMI | 2.708 (0.120) *** | 2.470 to 2.946 | 0.863 | 141.522 (12.208) *** | 117.227 to 165.817 | 0.622 | 1.215 (0.108) *** | 1.000 to 1.429 | 0.608 | |||
| - WC | 2.696 (0.253) *** | 2.193 to 3.199 | 0.582 | 169.522 (814.961) *** | 139.749 to 199.295 | 0.611 | 1.384 (0.141) *** | 1.103 to 1.665 | 0.539 | |||
| - W/hip | 1.281 (0.360) *** | 0.565 to 1.997 | 0.126 | 98.527 (21.049) *** | 56.638 to 140.416 | 0.205 | 0.864 (0.182) *** | 0.502 to 1.227 | 0.210 | |||
| - W/height | 2.360 (0.220) *** | 1.923 to 2.797 | 0.586 | 142.782 (13.746) *** | 115.427 to 170.137 | 0.569 | 1.168 (0.128) *** | 0.913 to 1.422 | 0.504 | |||
| Multivariable model | ||||||||||||
| - BMI - NC | 3.269 (0.153) *** −0.684 (0.298) * | 2.965 to 3.573 −1.277 to −0.090 | 0.904 | 0.735 −0.079 | 119.758 (15.622) *** 119.875 (30.504) *** | 88.664 to 150.853 59.159 to 180.592 | 0.734 | 0.439 0.225 | 1.125 (0.147) *** 0.746 (0.286) * | 0.833 to 1.417 0.176 to 1.316 | 0.690 | 0.475 0.161 |
| MEN | ||||||||||||
| Univariable model | ||||||||||||
| - NC | 5.115 (0.616) *** | 3.864 to 6.367 | 0.653 | 270.139 (31.414) *** | 206.366 to 333.912 | 0.670 | 2.717 (0.490) *** | 1.723 to 3.710 | 0.453 | |||
| - BMI | 2.800 (0.175) *** | 2.444 to 3.156 | 0.876 | 138.745 (12.002) *** | 114.380 to 163.109 | 0.787 | 1.590 (0.172) *** | 1.241 to 1.939 | 0.701 | |||
| - TMI | 2.775 (0.214) *** | 2.340 to 3.211 | 0.822 | 135.489 (14.154) *** | 106.754 to 164.224 | 0.716 | 1.640 (0.172) *** | 1.292 to 1.988 | 0.715 | |||
| - WC | 2.839 (0.207) *** | 2.420 to 3.259 | 0.839 | 146.521 (11.426) *** | 123.325 to 169.717 | 0.820 | 1.360 (0.237) *** | 0.879 to 1.842 | 0.470 | |||
| - W/hip | 2.475 (0.398) *** | 1.667 to 3.284 | 0.511 | 135.740 (19.555) *** | 96.040 to 175.439 | 0.567 | 1.086 (0.316) ** | 0.445 to 1.727 | 0.231 | |||
| - W/height | 2.777 (0.217) *** | 2.337 to 3.217 | 0.819 | 140.969 (12.658) *** | 115.273 to 166.666 | 0.774 | 1.399 (0.226) *** | 0.941 to 1.857 | 0.510 | |||
| Multivariable model | ||||||||||||
| - BMI - WC - TMI | 1.788 (0.400) *** 1.144 (0.414) ** | 0.975 to 2.601 0.303 to 1.986 | 0.896 | 0.241 0.149 | 56.675 (26.110) * 92.791 (27.033) ** | 3.612 to 109.738 37.855 to 147.728 | 0.837 | 0.146 0.231 | 1.640 (0.172) *** | 1.292 to 1.988 | 0.715 | 0.850 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Téllez, M.J.A.; Acosta, F.M.; Sanchez-Delgado, G.; Martinez-Tellez, B.; Muñoz-Hernández, V.; Martinez-Avila, W.D.; Henriksson, P.; Ruiz, J.R. Association of Neck Circumference with Anthropometric Indicators and Body Composition Measured by DXA in Young Spanish Adults. Nutrients 2020, 12, 514. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020514
Téllez MJA, Acosta FM, Sanchez-Delgado G, Martinez-Tellez B, Muñoz-Hernández V, Martinez-Avila WD, Henriksson P, Ruiz JR. Association of Neck Circumference with Anthropometric Indicators and Body Composition Measured by DXA in Young Spanish Adults. Nutrients. 2020; 12(2):514. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020514
Chicago/Turabian StyleTéllez, María José Arias, Francisco M. Acosta, Guillermo Sanchez-Delgado, Borja Martinez-Tellez, Victoria Muñoz-Hernández, Wendy D. Martinez-Avila, Pontus Henriksson, and Jonatan R. Ruiz. 2020. "Association of Neck Circumference with Anthropometric Indicators and Body Composition Measured by DXA in Young Spanish Adults" Nutrients 12, no. 2: 514. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020514