Social Stratification, Diet Diversity and Malnutrition among Preschoolers: A Survey of Addis Ababa, Ethiopia

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
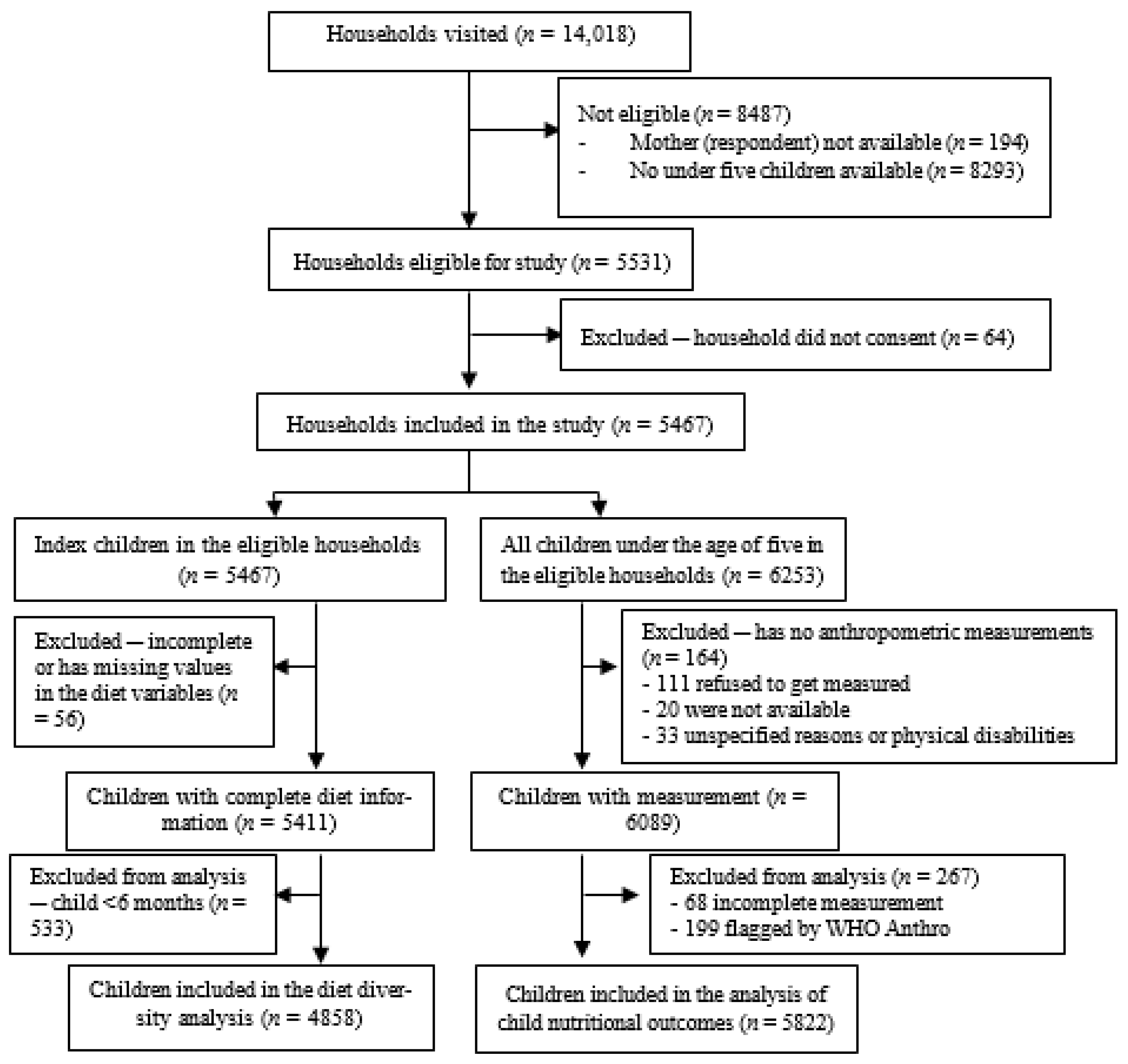
2.2. Sampling
2.3. Data Collection
2.4. Measurement
2.5. Outcome Variables
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Child Nutritional Status and Associations with Socioeconomic Resources
3.2. Child Diet Diversity and Associations with Socioeconomic Resources
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tzioumis, E.; Adair, L.S. Childhood dual burden of under- and over-nutrition in low- and middle-income countries: A critical review. Food Nutr. Bull. 2014, 35, 230–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Double burden of malnutrition. Available online: https://www.who.int/nutrition/double-burden-malnutrition/en/ (accessed on 25 February 2020).
- Crush, J.; Frayne, B.; McLachlan, M. Rapid Urbanization and the Nutrition Transition in Southern African. Kingston and Cape Town: Queen’s University and AFSUN. 2011. Available online: https://fsnnetwork.org/sites/default/files/rapid_urbanization_and_the_nutrition.pdf (accessed on 25 February 2020).
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Popkin, B.M. Nutrition Transition and the Global Diabetes Epidemic. Curr. Diabet. Rep. 2015, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. NOW AND THEN: The Global Nutrition Transition: The Pandemic of Obesity in Developing Countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Escamilla, R.; Bermudez, O.; Buccini, G.S.; Kumanyika, S.; Lutter, C.K.; Monsivais, P.; Victora, C. Nutrition disparities and the global burden of malnutrition. BMJ 2018, 361. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.; Ruel, M.T.; Salm, L.; Sinclair, B.; Branca, F. Double-duty actions: Seizing programme and policy opportunities to address malnutrition in all its forms. Lancet 2020, 395, 142–155. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Muthuri, S.K.; Oti, S.O.; Mutua, M.K.; van de Vijver, S.; Kyobutungi, C. Evidence of a Double Burden of Malnutrition in Urban Poor Settings in Nairobi, Kenya. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.W. Urban Food Systems and the Poor in Developing Countries. Trans. Inst. Br. Geogr. 1998, 23, 207–219. [Google Scholar] [CrossRef]
- Ziraba, A.K.; Fotso, J.C.; Ochako, R. Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health 2009, 9, 465. [Google Scholar] [CrossRef] [Green Version]
- Van de Poel, E.; Hosseinpoor, A.R.; Jehu-Appiah, C.; Vega, J.; Speybroeck, N. Malnutrition and the disproportional burden on the poor: The case of Ghana. Int. J. Equity Health 2007, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, R.; Eagle, T.F.; Sheetz, A.; Woodward, A.; Leibowitz, R.; Song, M.; Sylvester, R.; Corriveau, N.; Kline-Rogers, E.; Jiang, Q.; et al. The Relationship between Childhood Obesity, Low Socioeconomic Status, and Race/Ethnicity: Lessons from Massachusetts. Child Obes. 2015, 11, 691. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Moudon, A.V.; Jiao, J.; Aggarwal, A.; Charreire, H.; Chaix, B. Food environment and socioeconomic status influence obesity rates in Seattle and in Paris. Int. J. Obes. 2014, 38, 306–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villanueva, R.; Albaladejo, R.; Astasio, P.; Ortega, P.; Santos, J.; Regidor, E. Socio-economic environment, area facilities and obesity and physical inactivity among children. Eur. J. Public Health 2016, 26, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Herforth, A.; Ahmed, S. The food environment, its effects on dietary consumption, and potential for measurement within agriculture-nutrition interventions. Food Secur. 2015, 7, 505–520. [Google Scholar] [CrossRef] [Green Version]
- Demilew, Y.M.; Tafere, T.E.; Abitew, D.B. Infant and young child feeding practice among mothers with 0–24 months old children in Slum areas of Bahir Dar City, Ethiopia. Int. Breastfeed J. 2017, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Akombi, B.J.; Agho, K.E.; Renzaho, A.M.; Hall, J.J.; Merom, D.R. Trends in socioeconomic inequalities in child undernutrition: Evidence from Nigeria Demographic and Health Survey (2003–2013). PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Contreras, M.; Blandón, E.Z.; Persson, L.-Å.; Hjern, A.; Ekström, E.-C. Socio-economic resources, young child feeding practices, consumption of highly processed snacks and sugar-sweetened beverages: A population-based survey in rural northwestern Nicaragua. BMC Public Health 2015, 15, 25. [Google Scholar] [CrossRef] [Green Version]
- Beshara, M.; Hutchinson, A.; Wilson, C. Preparing meals under time stress. The experience of working mothers. Appetite 2010, 55, 695–700. [Google Scholar] [CrossRef]
- Jabs, J.; Devine, C.M.; Bisogni, C.A.; Farrell, T.J.; Jastran, M.; Wethington, E. Trying to Find the Quickest Way: Employed Mothers’ Constructions of Time for Food. J Nutr. Educ. Behav. 2007, 39, 18–25. [Google Scholar] [CrossRef]
- Kimani-Murage, E.; Schofield, L.; Wekesah, F.; Mohamed, S.; Mberu, B.; Ettarh, R.; Egondi, T.; Kyobutungi, C.; Ezeh, A. Vulnerability to Food Insecurity in Urban Slums: Experiences from Nairobi, Kenya. J. Urban Health 2014, 91, 1098–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekhar, S.; Aguayo, V.M.; Krishna, V.; Nair, R. Household food insecurity and children’s dietary diversity and nutrition in India. Evidence from the comprehensive nutrition survey in Maharashtra. Matern. Child Nutr. 2017, 13, e12447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Central Statistical Agency (CSA) Ethiopia; ICF. Ethiopia Demographic and Health Survey 2016; CSA: Addis Ababa, Ethiopia; ICF: Rockville, MD, USA, 2016; Available online: http://dhsprogram.com/publications/publication-FR328-DHS-Final-Reports.cfm (accessed on 25 February 2020).
- Amare, Z.Y.; Ahmed, M.E.; Mehari, A.B. Determinants of nutritional status among children under age 5 in Ethiopia: Further analysis of the 2016 Ethiopia demographic and health survey. Glob. Health 2019, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, S.H.; Muhammad, F.; Pakzad, R.; Alizadeh, S. Socioeconomic inequality in stunting among under-5 children in Ethiopia: A decomposition analysis. BMC Res. Notes. 2019, 12, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaliviero, M.; Cheru, F. State of Addis Ababa 2017: The Addis Ababa We Want. UN- Habitat. 2017. Available online: https://unhabitat.org/books/the-state-of-addis-ababa-2017-the-addis-ababa-we-want/ (accessed on 25 February 2020).
- The World Bank. Ethiopia at a Glance-Overview. Available online: https://www.worldbank.org/en/country/ethiopia/overview (accessed on 26 February 2020).
- Central Statistical Agency (CSA) Ethiopia. Population Projections of Ethiopia 2007–2037; CSA: Addis Ababa, Ethiopia, 2013. Available online: http://www.csa.gov.et/census-report/population-projections/category/368-population-projection-2007-2037# (accessed on 26 February 2020).
- Central Statistics Agency. Summary and Statistical Report of the 2007 Population and Housing Census: Population Size by Age and Sex; UNFPA: New York, NY, USA, 2008. [Google Scholar]
- The World Bank. Enhancing Urban Resilience. Available online: https://www.worldbank.org/en/topic/urbandevelopment/publication/addis-ababa-ethiopia-enhancing-urban-resilience (accessed on 26 February 2020).
- World Health Organization. PROCESS of Translation and Adaptation of Instruments. Available online: https://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 26 February 2020).
- Cogill, B. Anthropometric Indicators Measurement Guide; Food and Nutrition Technical Assistance Project, Academy for Educational Development: Washington, DC, USA, 2001. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- World Health Organization. Training Course on Child Growth Assessment; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- World Education News Reviews. Education in Ethiopia. Available online: https://wenr.wes.org/2018/11/education-in-ethiopia (accessed on 26 February 2020).
- Rutstein, S.O. Steps to Constructing the New DHS Wealth Index; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v. 3); Food and Nutrition Technical Assistance Project, Academy for Educational Development: Washington, DC, USA, August 2007; Available online: http://www.fao.org/fileadmin/user_upload/eufao-fsi4dm/doc-training/hfias.pdf (accessed on 26 February 2020).
- Kennedy, G.; Ballard, T.; Dop, M.-C. Guidelines for Measuring Household and Individual Dietary Diversity; FAO: Rome, Italy, 2011. [Google Scholar]
- World Health Organization; UNICEF; USAID; AED; UCDAVIS; IFPRI. Indicators for assessing infant and young child feeding practices: Part 2: Measurement. 2010, p. 81. Available online: https://www.who.int/nutrition/publications/infantfeeding/9789241599290/en/ (accessed on 26 February 2020).
- World Health Organization. WHO Anthro for Personal Computers. January 2011. Available online: https://www.who.int/childgrowth/software/en/ (accessed on 2 April 2019).
- United Nations. The Sustainable Development Goals Report 2019; United Nations: New York, NY, USA, 2019; Available online: https://unstats.un.org/sdgs/report/2019/The-Sustainable-Development-Goals-Report-2019.pdf (accessed on 26 February 2020).
- De Onis, M.; Borghi, E.; Arimond, M.; Webb, P.; Croft, T.; Saha, K.; De-Regil, L.M.; Thuita, F.; Heidkamp, R.; Krasevec, J.; et al. Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutr. 2018, 22, 175–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebrie, A.; Alebel, A.; Zegeye, A.; Tesfaye, B.; Ferede, A. Prevalence and associated factors of overweight/ obesity among children and adolescents in Ethiopia: A systematic review and meta-analysis. BMC Obes. 2018, 5, 1–12. [Google Scholar] [CrossRef]
- Ethiopian Public Health Institute. Ethiopia National Food Consumption Survey; Ethiopian Public Health Institute: Addis Ababa, Ethiopia, 2013. [Google Scholar]
- Mekonnen, N.; Asfaw, S.; Mamo, A.; Mulu, Y.; Fentahun, N. Barriers and facilitators of child-feeding practice in a small sample of individuals from Gozamin District, Northwest of Ethiopia: A qualitative study. BMC Nutr. 2018, 4, 25. [Google Scholar] [CrossRef]
- Solomon, D.; Aderaw, Z.; Tegegne, T.K. Minimum dietary diversity and associated factors among children aged 6–23 months in Addis Ababa, Ethiopia. Int. J. Equity Health 2017, 16, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Khattak, U.K.; Iqbal, S.P.; Ghazanfar, H. The Role of Parents’ Literacy in Malnutrition of Children Under the Age of Five Years in a Semi-Urban Community of Pakistan: A Case-Control Study. Cureus 2017, 9. [Google Scholar] [CrossRef] [Green Version]
- Kandala, N.-B.; Madungu, T.P.; Emina, J.B.; Nzita, K.P.; Cappuccio, F.P. Malnutrition among children under the age of five in the Democratic Republic of Congo (DRC): Does geographic location matter? BMC Public Health 2011, 11, 261. [Google Scholar] [CrossRef] [Green Version]
- Abuya, B.A.; Ciera, J.; Kimani-Murage, E. Effect of mother’s education on child’s nutritional status in the slums of Nairobi. BMC Pediatr. 2012, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsi, D.J.; Mejía-Guevara, I.; Subramanian, S.V. Risk factors for chronic undernutrition among children in India: Estimating relative importance, population attributable risk and fractions. Soc. Sci. Med. 2016, 157, 165–185. [Google Scholar] [CrossRef] [PubMed]
- Smith Greenaway, E.; Leon, J.; Baker, D.P. Understanding the association between maternal education and use of health services in Ghana: Exploring the role of health knowledge. J. Biosoc. Sci. 2012, 44, 733–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ickes, S.B.; Hurst, T.E.; Flax, V.L. Maternal Literacy, Facility Birth, and Education Are Positively Associated with Better Infant and Young Child Feeding Practices and Nutritional Status among Ugandan Children. J. Nutr. 2015, 145, 2578–2586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shroff, M.; Griffiths, P.; Adair, L.; Suchindran, C.; Bentley, M. Maternal autonomy is inversely related to child stunting in Andhra Pradesh, India. Matern. Child Nutr. 2009, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, K.; Ruel, M.; Ferguson, E.; Uauy, R. Women’s empowerment and child nutritional status in South Asia: A synthesis of the literature: Women’s empowerment and child nutrition: South Asia. Matern. Child Nutr. 2015, 11, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Mutisya, M.; Kandala, N.; Ngware, M.W.; Kabiru, C.W. Household food (in)security and nutritional status of urban poor children aged 6 to 23 months in Kenya. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.-T.; Chang, Y.-H.; Lee, M.-S.; Wahlqvist, M.L. Health and nutrition economics: Diet costs are associated with diet quality. Asia Pac. J. Clin. Nutr. 2009, 18, 598–604. [Google Scholar]
- Hawkes, C. Uneven dietary development: Linking the policies and processes of globalization with the nutrition transition, obesity and diet-related chronic diseases. Glob. Health. 2006, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Ford, N.D.; Patel, S.A.; Narayan, K.M.V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health. 2017, 38, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J. Physical activity, sedentary behaviour and energy balance in the preschool child: Opportunities for early obesity prevention: Symposium on ‘Behavioural nutrition and energy balance in the young’. Proc. Nutr. Soc. 2008, 67, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Wamani, H.; Åstrøm, A.N.; Peterson, S.; Tumwine, J.K.; Tylleskär, T. Boys are more stunted than girls in Sub-Saharan Africa: A meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muenchhoff, M.; Goulder, P.J.R. Sex Differences in Pediatric Infectious Diseases. J. Infect Dis. 2014, 209, S120–S126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumilowicz, A.; Habicht, J.-P.; Pelto, G.; Pelletier, D.L. Gender perceptions predict sex differences in growth patterns of indigenous Guatemalan infants and young children. Am. J. Clin. Nutr. 2015, 102, 1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Double-Duty Actions for Nutrition: Policy Brief; WHO: Geneva, Switzerland, 2017; Available online: http://www.who.int/nutrition/publications/double-duty-actions-nutrition-policybrief/en/ (accessed on 26 February 2020).
- Makoka, D.; Masibo, P.K. Is there a threshold level of maternal education sufficient to reduce child undernutrition? Evidence from Malawi, Tanzania and Zimbabwe. BMC Pediatr. 2015, 15, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, S.; Peñalvo, J.L. Actions Targeting the Double Burden of Malnutrition: A Scoping Review. Nutrients 2019, 12, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terfa, B.K.; Chen, N.; Liu, D.; Zhang, X.; Niyogi, D. Urban Expansion in Ethiopia from 1987 to 2017: Characteristics, Spatial Patterns, and Driving Forces. Sustainability 2019, 11, 2973. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Level | Characteristics (n = 5467) | n | % |
|---|---|---|---|
| Household | Male headed households | 4729 | 86.5 |
| 2 to 4 family size | 3561 | 65.1 | |
| Housing ownership (n = 5452) | |||
| Privately owned | 1165 | 21.3 | |
| Rented from private | 2329 | 42.6 | |
| Rented from public | 1360 | 24.9 | |
| Rent-free | 598 | 11.0 | |
| Household food insecurity | |||
| Food secure | 3362 | 61.5 | |
| Mildly food insecure | 500 | 9.2 | |
| Moderately food insecure | 1070 | 19.6 | |
| Severely food insecure | 535 | 9.8 | |
| Maternal | Age | ||
| 15–24 | 864 | 15.8 | |
| 25–34 | 3342 | 61.1 | |
| 35–44 | 999 | 18.3 | |
| 45+ | 262 | 4.8 | |
| Marital status | |||
| Married/living together | 4813 | 88.1 | |
| Never married/divorced/widowed/separated | 654 | 11.9 | |
| Education | |||
| Never attended/ finished first grade | 752 | 13.8 | |
| Grade 1–4 | 498 | 9.1 | |
| Grade 5–8 | 1638 | 30.0 | |
| Grade 9–12 | 1482 | 27.1 | |
| College | 1097 | 20.1 | |
| Involved in income-earning activity | 1432 | 26.2 | |
| Child | Sex (Male) | 2847 | 52.1 |
| Age | |||
| 0–5 months | 556 | 10.2 | |
| 6–11 months | 657 | 12.0 | |
| 12–23 months | 1337 | 25.0 | |
| 24–35 months | 1286 | 23.5 | |
| 36–47 months | 945 | 17.3 | |
| 48–59 months | 686 | 12.6 | |
| Nutritional status (n = 5822) | |||
| Stunted | 1139 | 19.6 | |
| Wasted | 187 | 3.2 | |
| Overweight/Obese | 664 | 11.4 | |
| Diet diversity (>3 food groups) | 2911 | 59.9 |
| Stunted | Overweight/Obese | Wasted | |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| All | 1139 (19.6) | 664 (11.4) | 187 (3.2) |
| Household wealth | |||
| Lowest tertile (n = 1935) | 428 (22.1) | 187 (9.7) | 62 (3.2) |
| Middle tertile (n = 1953) | 377 (19.3) | 222 (11.4) | 58 (3.0) |
| Highest tertile (n = 1934) | 334 (17.3) | 255 (13.2) | 67 (3.5) |
| p = 0.0001 | p = 0.001 | p = 0.17 | |
| Mother’s Education | |||
| Never attended/less than first grade (n = 782) | 190 (24.3) | 64 (8.2) | 28 (3.6) |
| Grade 1–4 (n = 528) | 120 (22.7) | 57 (10.8) | 10 (1.9) |
| Grade 5–8 (n = 1732) | 377 (21.8) | 180 (10.4) | 62 (3.6) |
| Grade 9–12 (n = 1582) | 279 (17.6) | 178 (11.3) | 45 (2.8) |
| College (n = 1198) | 173 (14.4) | 185 (15.4) | 42 (3.5) |
| p = 0.0001 | p = 0.0001 | p = 0.91 | |
| Household Food Insecurity | |||
| Food secure (n = 3581) | 625 (17.5) | 454 (12.7) | 105 (2.9) |
| Mildly insecure (n = 533) | 115 (21.6) | 56 (10.5) | 22 (4.1) |
| Moderately insecure (n = 1135) | 246 (21.7) | 104 (9.2) | 40 (3.5) |
| Severely insecure (n = 573) | 153 (26.7) | 50 (8.7) | 20 (3.5) |
| p = 0.0001 | p = 0.0001 | p = 0.26 | |
| Child Sex | |||
| Male (n = 3018) | 635 (21.0) | 341 (11.3) | 111 (3.7) |
| Female (n = 2804) | 504 (18.0) | 323 (11.5) | 76 (2.7) |
| p = 0.003 | p = 0.069 | p = 0.036 |
| Stunted | Overweight/Obese | Wasted | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Unadjusted OR (95% CI) a | Age-Adjusted OR (95% CI) b | Fully-Adjusted OR (95% CI) c | Unadjusted OR (95% CI) a | Age-Adjusted OR (95% CI) b | Fully-Adjusted OR (95% CI) c | Unadjusted OR (95% CI) a | Age-Adjusted OR (95% CI) b | Fully-Adjusted OR (95% CI) c | |
| Household Wealth | |||||||||
| Lowest Tertile | 1.37 * (1.16–1.60) | 1.35 * (1.15–1.59) | 1.14 (0.96–1.35) | 0.71 * (0.58–0.86) | 0.68 * (0.55–0.83) | 0.77 * (0.62–0.96) | 0.92 (0.65–1.31) | 0.93 (0.65–1.33) | 0.88 (0.61–1.29) |
| Middle Tertile | 1.15 (0.98–1.36) | 1.14 (0.97–1.35) | 1.03 (0.87–1.23) | 0.84 (0.69–1.02) | 0.83 (0.68–1.01) | 0.90 (0.74–1.10) | 0.85 (0.59–1.22) | 0.86 (0.60–1.23) | 0.82 (0.57–1.19) |
| Highest Tertile | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Mother’s Education | |||||||||
| Never Attended/ Finished First Grade | 1.86 * (1.48–2.34) | 2.00 * (1.57–2.54) | 1.75 * (1.36–2.24) | 0.49 * (0.36–0.67) | 0.52 * (0.38–0.71) | 0.61 * (0.44–0.84) | 1.01 (0.62–1.65) | 1.04 (0.62–1.72) | 0.95 (0.55–1.62) |
| Grade 1–4 | 1.72 * (1.33–2.24) | 1.73 * (1.33–2.26) | 1.54 * (1.17–2.02) | 0.67 * (0.49–0.92) | 0.69 * (0.50–0.95) | 0.78 (0.56–1.08) | 0.53 (0.26–1.06) | 0.54 (0.27–1.09) | 0.50 (0.25–1.03) |
| Grade 5–8 | 1.61 * (1.32–1.97) | 1.57 * (1.28–1.92) | 1.46 * (1.19–1.80) | 0.64 * (0.51–0.80) | 0.65 * (0.52–0.81) | 0.71 * (0.56–0.89) | 1.01 (0.68–1.51) | 1.04 (0.70–1.31) | 1.01 (0.66–1.53) |
| Grade 9–12 | 1.25 * (1.02–1.54) | 1.21 (0.98–1.48) | 1.18 (0.96–1.45) | 0.70 * (0.56–0.87) | 0.74 * (0.59–0.93) | 0.77 * (0.61–0.96) | 0.80 (0.52–1.22) | 0.85 (0.55–1.31) | 0.84 (0.55–1.30) |
| College | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Household Food Insecurity | |||||||||
| Severely Insecure | 1.67 * (1.36–2.06) | 1.69 * (1.37–2.08) | 1.42 * (1.14–1.76) | 0.67 * (0.49–0.91) | 0.70 * (0.52–0.96) | 0.84 (0.61-1.16) | 1.20 (0.74-1.95) | 1.22 (0.75-1.99) | 1.30 (0.77-2.18) |
| Moderately Insecure | 1.32 * (1.12–1.56) | 1.32 * (1.12–1.56) | 1.15 (0.97–1.38) | 0.70 * (0.56–0.87) | 0.70 * (0.56–0.88) | 0.81 (0.63–1.02) | 1.21 (0.84–1.76) | 1.23 (0.84–1.78) | 1.28 (0.87–1.91) |
| Mildly Insecure | 1.30 * (1.04–1.63) | 1.30 * (1.04–1.63) | 1.22 (0.97–1.53) | 0.81 (0.60–1.09) | 0.81 (0.60–1.09) | 0.87 (0.64–1.17 | 1.42 (0.89–2.28) | 1.41 (0.88–2.27) | 1.50 (0.93–2.42) |
| Food Secure | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Child Sex | |||||||||
| Male | 1.21 * (1.07–1.38) | 1.21 * (1.06–1.38) | 1.22 * (1.06–1.39) | 0.98 (0.83–1.15) | 0.99 (0.84–1.16) | 0.98 (0.84–1.16) | 1.37 * (1.02–1.84) | 1.38 * (1.02–1.86) | 1.38 * (1.03–1.86) |
| Female | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Minimum Dietary Diversity (≥4 Food Groups) | ||||
|---|---|---|---|---|
| n (%) | Unadjusted OR (95% CI) a | Age-Adjusted OR (95%CI) b | Fully-Adjusted OR (95% CI) c | |
| All | 2911 (59.9) | |||
| Household Wealth | ||||
| Lowest Terile (n = 1616) | 794 (49.1) | 0.40 * (0.35–0.47) | 0.40 * (0.34–0.46) | 0.60 * (0.51–0.71) |
| Middle Tertile (n = 1647) | 995 (60.4) | 0.63 * (0.55–0.73) | 0.62 * (0.53–0.72) | 0.80 * (0.68–0.93) |
| Highest Tertile (n = 1595) | 1122 (70.3) | Ref | Ref | Ref |
| Mother’s Education | ||||
| Never Attended/Less than First Grade (n = 688) | 293 (42.6) | 0.25 * (0.20–0.31) | 0.21 * (0.17–0.27) | 0.33 * (0.26–0.42) |
| Grade 1–4 (n = 440) | 191 (43.4) | 0.26 * (0.20–0.32) | 0.24 * (0.18–0.30) | 0.35 * (0.27–0.45) |
| Grade 5–8 (n = 1444) | 811 (56.2) | 0.43 * (0.36–0.51) | 0.41 * (0.34–0.50) | 0.52 * (0.43–0.64) |
| Grade 9–12 (n = 1338) | 901 (67.3) | 0.68 * (0.56–0.82) | 0.66 * (0.54–0.80) | 0.74 * (0.61–0.90) |
| College (n = 948) | 715 (75.4) | Ref | Ref | Ref |
| Household Food Security | ||||
| Severely Insecure (n = 476) | 158 (33.2) | 0.24 * (0.20–0.30) | 0.22 * (0.18–0.27) | 0.32 * (0.26–0.40) |
| Moderately Insecure (n = 952) | 466 (49.0) | 0.44 * (0.38–0.51) | 0.42 * (0.36–0.48) | 0.56 * (0.47–0.66) |
| Mildly Insecure (n = 455) | 251 (55.2) | 0.58 * (0.47–0.70) | 0.56 * (0.45–0.69) | 0.68 * (0.55–0.84) |
| Secure (n = 2975) | 2036 (68.4) | Ref | Ref | Ref |
| Child Sex | ||||
| Male (n = 2541) | 1545 (60.8) | 1.08 (0.97–1.21) | 1.08 (0.96–1.21) | 1.08 (0.96–1.23) |
| Female (n = 2317) | 1366 (59.0) | Ref | Ref | Ref |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berhane, H.Y.; Jirström, M.; Abdelmenan, S.; Berhane, Y.; Alsanius, B.; Trenholm, J.; Ekström, E.-C. Social Stratification, Diet Diversity and Malnutrition among Preschoolers: A Survey of Addis Ababa, Ethiopia. Nutrients 2020, 12, 712. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030712
Berhane HY, Jirström M, Abdelmenan S, Berhane Y, Alsanius B, Trenholm J, Ekström E-C. Social Stratification, Diet Diversity and Malnutrition among Preschoolers: A Survey of Addis Ababa, Ethiopia. Nutrients. 2020; 12(3):712. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030712
Chicago/Turabian StyleBerhane, Hanna Y., Magnus Jirström, Semira Abdelmenan, Yemane Berhane, Beatrix Alsanius, Jill Trenholm, and Eva-Charlotte Ekström. 2020. "Social Stratification, Diet Diversity and Malnutrition among Preschoolers: A Survey of Addis Ababa, Ethiopia" Nutrients 12, no. 3: 712. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030712