Monoacylglycerol Form of Omega-3s Improves Its Bioavailability in Humans Compared to Other Forms

 , ,
, ,
Abstract
:
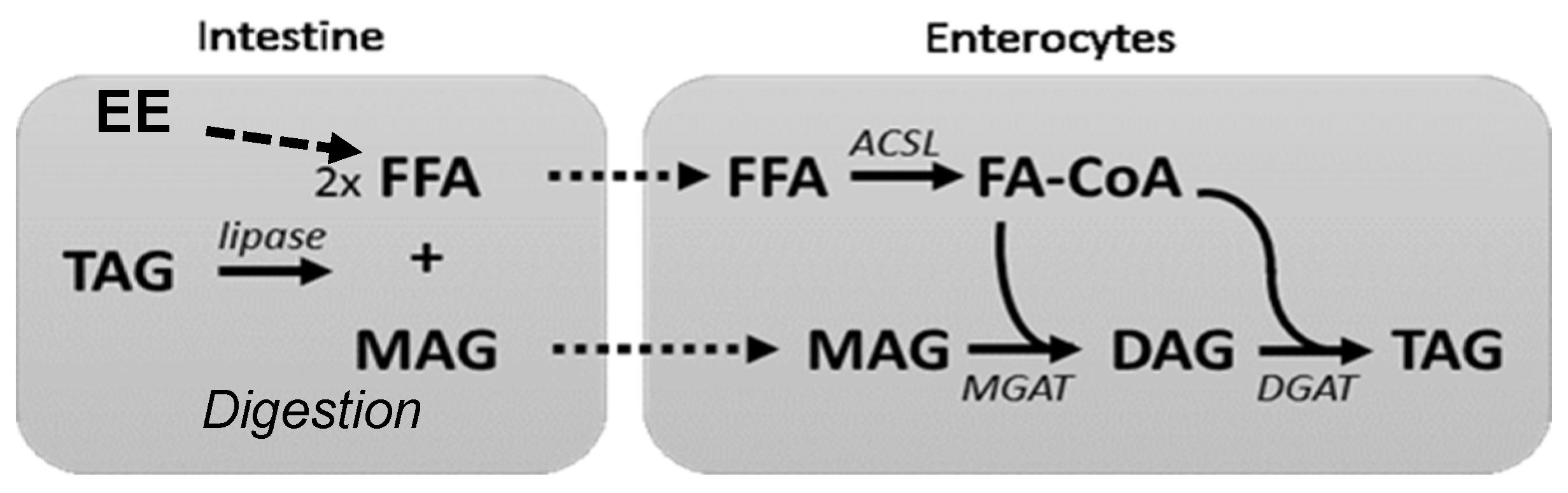
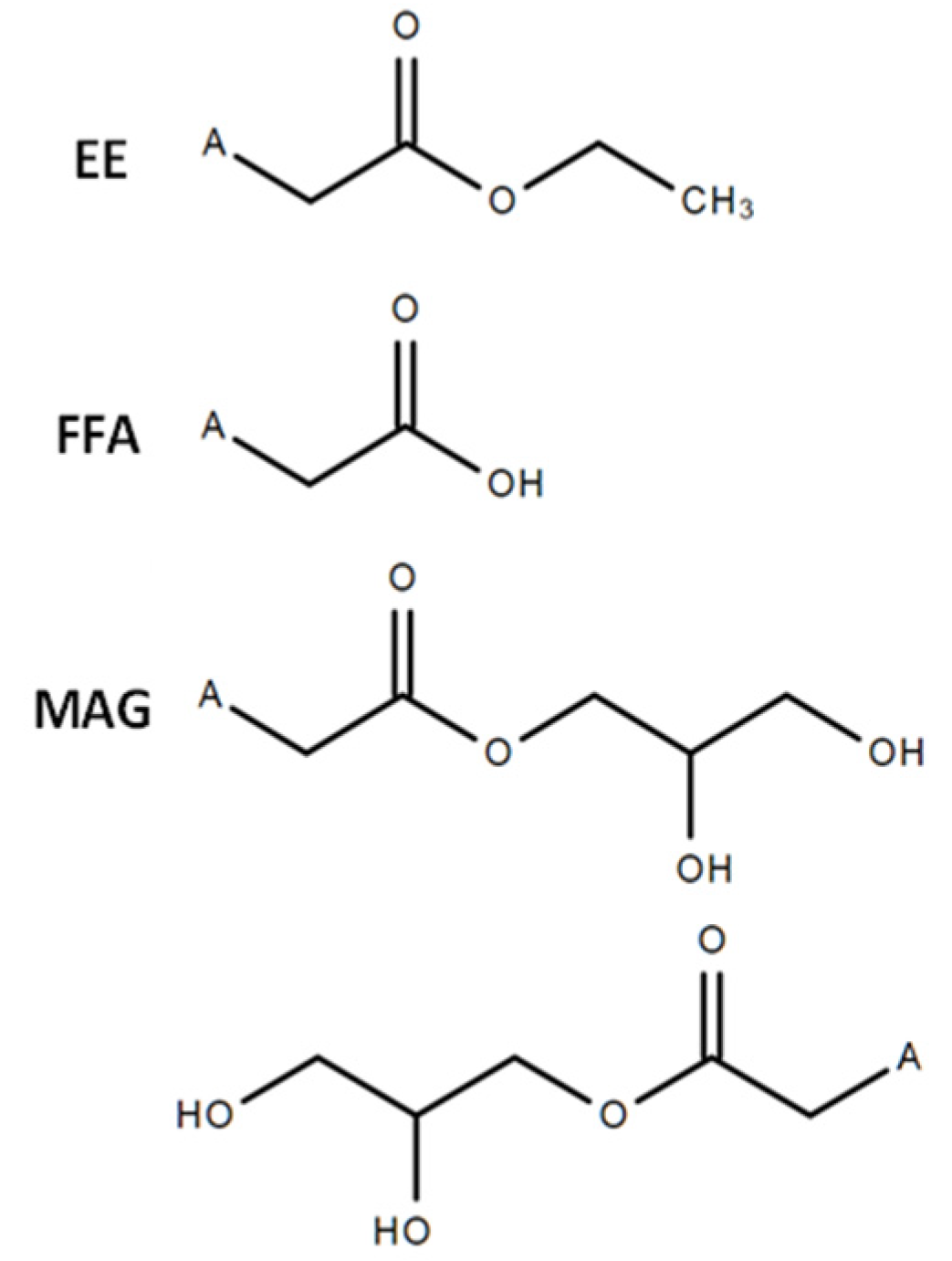
1. Introduction
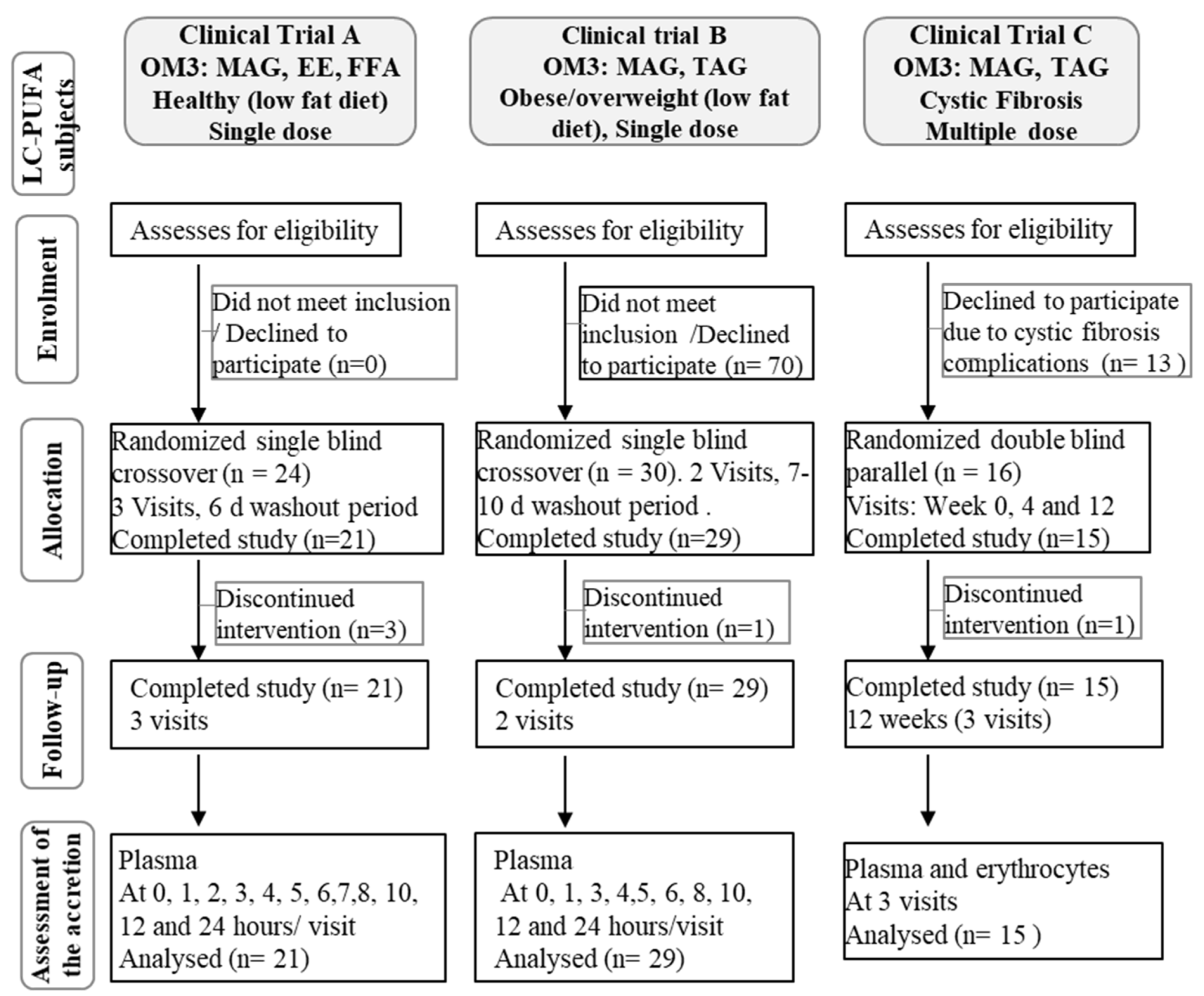
2. Materials and Methods
2.1. Clinical Trial Ethics
2.2. Subjects
2.3. Interventions
2.4. Study Design
2.5. Assessment of Accretion
2.6. Analysis of the Fatty Acid Composition in Blood Lipids
2.7. Statistical Analysis
3. Results
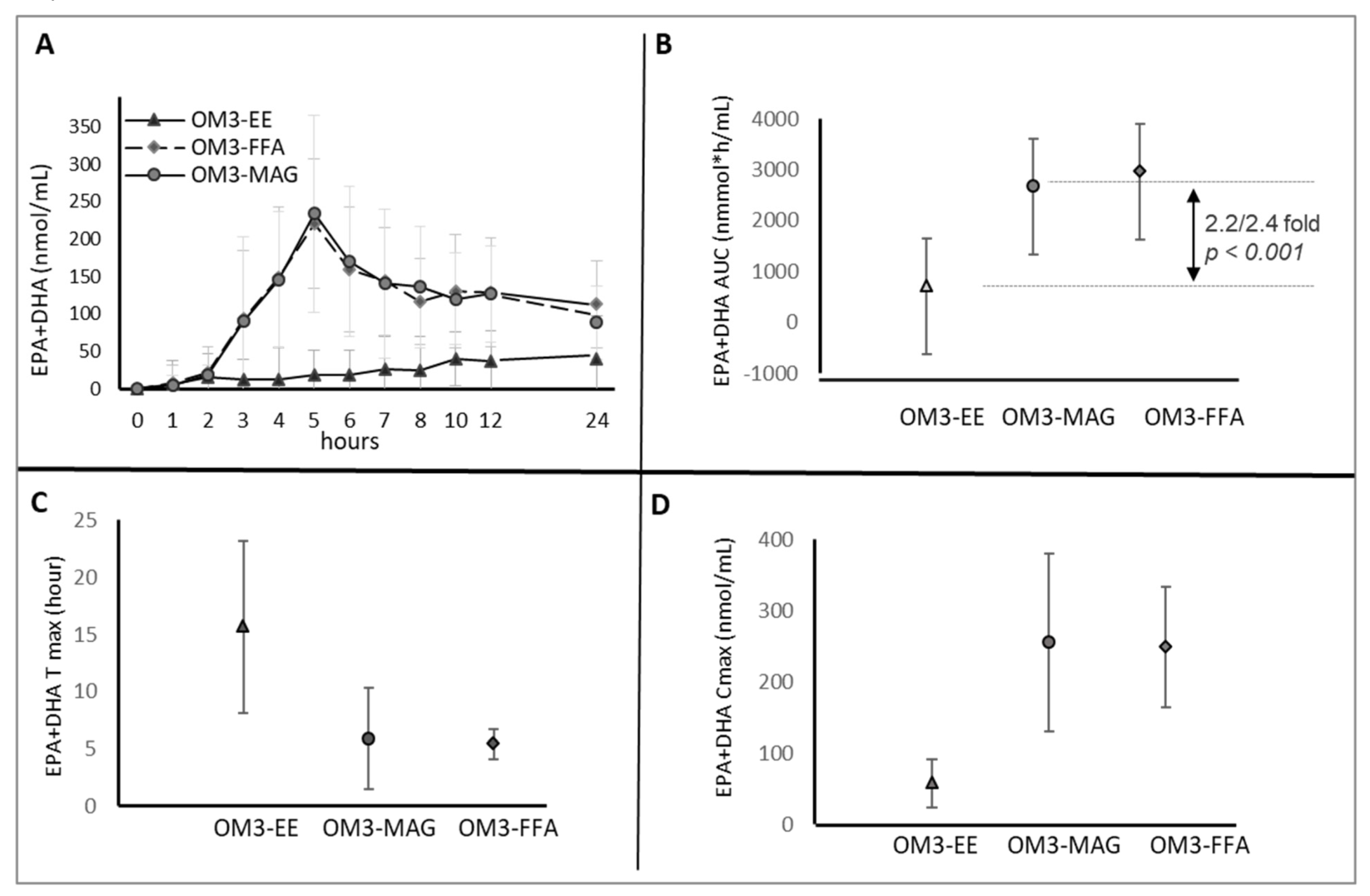
3.1. Clinical Trial A. Normal Weight Healthy Subjects with Low Fat Diet
3.1.1. Clinical and Compliance Evaluation
3.1.2. Incorporation of EPA and DHA in Plasma-Acute Phase
3.2. Clinical Trial B. Obese or Overweight Subjects
3.2.1. Clinical and Compliance Evaluation
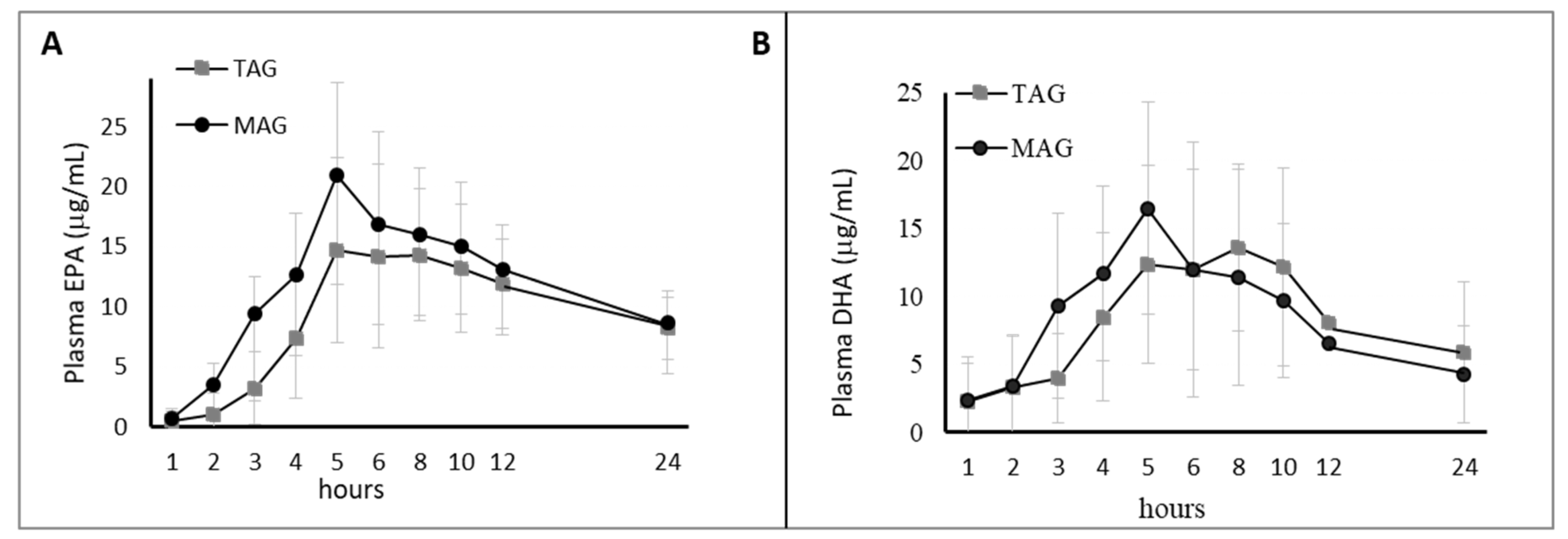
3.2.2. Incorporation of EPA and DHA in Plasma-Acute Phase
3.3. Clinical Trial C. Cystic Fibrosis Patients
3.3.1. Clinical and Compliance Evaluation
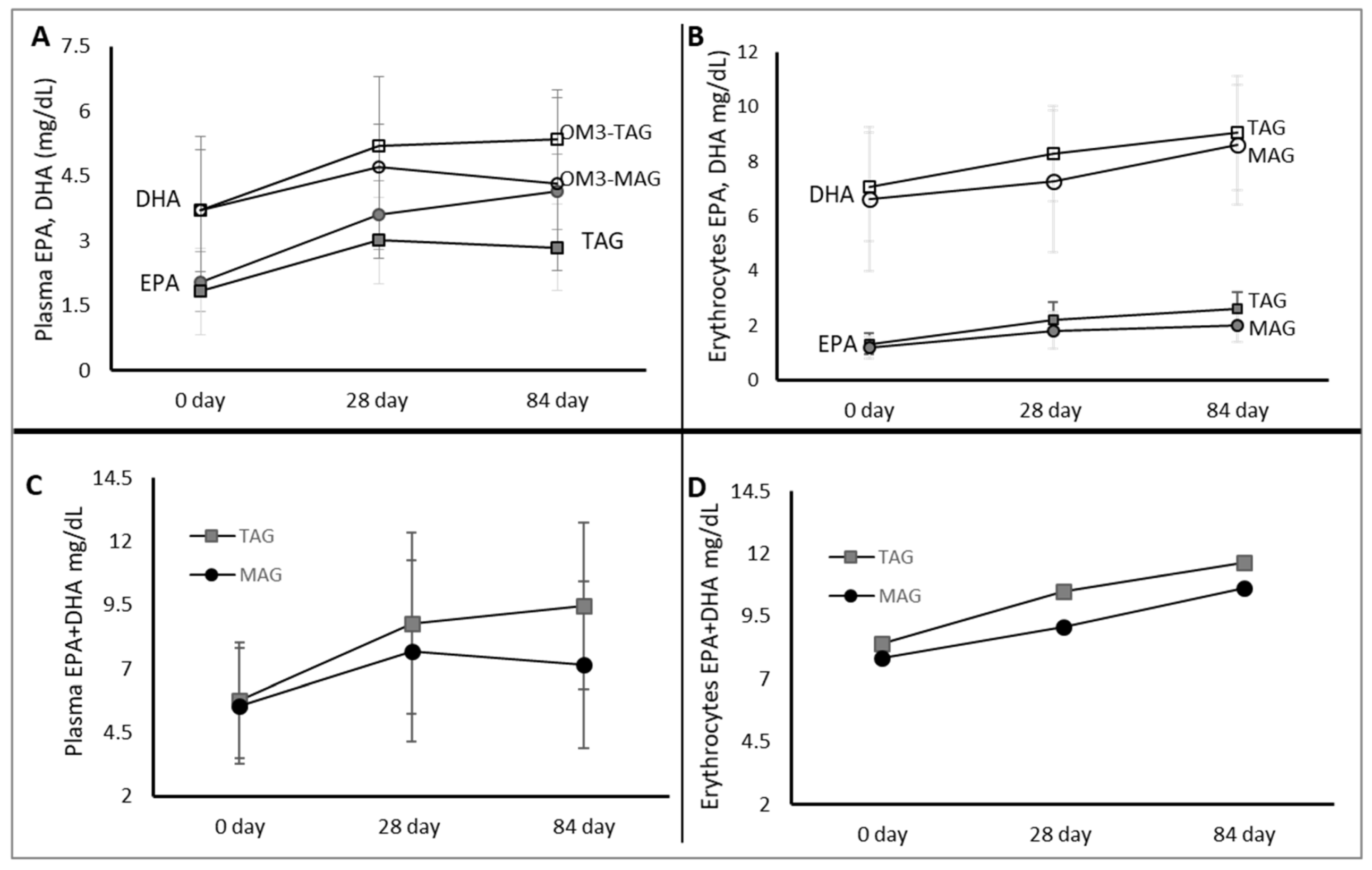
3.3.2. Incorporation of EPA and DHA in Erythrocytes and Plasma
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| OM3 | Omega-3 fatty acids |
| OM3-MAG | OM3-sn-1(3)-monoacylglycerol |
| FFA | free fatty acids |
| TAG | triacylglycerols |
| EPA | eicosapentaenoic acid |
| DHA | docosahexaenoic acid |
| LC-PUFAs | long chain polyunsaturated fatty acids |
| sn-2 MAG | sn-2 monoacylglycerol |
| FA | fatty acid |
| TC | total cholesterol |
| LDL-C | low-density lipoprotein-cholesterol |
| HDL-C | high-density lipoprotein-cholesterol |
| LCI | lung clearance index |
| FEV1 | forced expiratory vital capacity |
| FVC | forced expiratory volume per second |
| MEF 25/75 | mean exploratory flow between 25% and 75% of vital capacity |
| FAME | fatty acid methyl esters |
| AUC | area under the curve |
| GMR | geometric least-square means |
| LSMs | least square means |
| SAEs | serious adverse events |
| AEs | adverse events |
| TEAEs | treatment-emergent adverse events |
| GMRs | geometric least-square mean ratios |
References
- Calder, P.C.; Deckelbaum, R.J. Omega-3 fatty acids and cardiovascular outcomes: An update. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.K. A Comparative overview of prescription omega-3 fatty acid products. Pharm. Ther. 2015, 40, 826–857. [Google Scholar]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Lemaitre, R.N.; King, I.B.; Song, X.; Huang, H.; Sacks, F.M.; Rimm, E.B.; Wang, M.; Siscovick, D.S. Plasma phospholipid long-chain omega-3 fatty acids and total and cause-specific mortality in older adults: A cohort study. Ann. Intern. Med. 2013, 158, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Davidson, M.H.; Stein, E.A.; Bays, H.E.; Maki, K.C.; Doyle, R.T.; Shalwitz, R.A.; Ballantyne, C.M.; Ginsberg, H.N. COMBination of prescription Omega-3 with Simvastatin (COMBOS) Investigators. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: An 8-week, randomized, double-blind, placebo-controlled study. Clin. Ther. 2007, 29, 1354–1367. [Google Scholar]
- Bays, H.E.; Tighe, A.P.; Sadovsky, R.; Davidson, M.H. Prescription omega-3 fatty acids and their lipid effects: Physiologic mechanisms of action and clinical implications. Expert Rev. Cardiovasc. Ther. 2008, 6, 391–409. [Google Scholar] [CrossRef]
- Offman, E.; Marenco, T.; Ferber, S.; Johnson, J.; Kling, D.; Curcio, D.; Davidson, M. Steady-state bioavailability of prescription omega-3 on a low-fat diet is significantly improved with a free fatty acid formulation compared with an ethyl ester formulation: The ECLIPSE II study. Vasc. Health Risk Manag. 2013, 9, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Laidlaw, M.; Cockerline, C.A.; Rowe, W.J. A Randomized clinical trial to determine the efficacy of manufacturers’ recommended doses of omega-3 fatty acids from different sources in facilitating cardiovascular disease risk reduction. Lipids Health Dis. 2014, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef]
- Maki, K.C.; Palacios, O.M.; Bell, M.; Toth, P.P. Use of supplemental long-chain omega-3 fatty acids and risk for cardiac death: An updated meta-analysis and review of research gaps. J. Clin. Lipidol. 2017, 11, 1152–1160.e2. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, T.; Khademi, H.; Moghadasian, M.H. The role of marine n-3 fatty acids in improving cardiovascular health: A review. Food Funct. 2013, 4, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Connor, W.E.; Alam, N.; Illingworth, D.R. Reduction of postprandial triglyceridemia in humans by dietary n-3 fatty acids. J. Lipid Res. 1988, 29, 1451–1460. [Google Scholar] [PubMed]
- Phillipson, B.E.; Rothrock, D.W.; Connor, W.E.; Harris, W.S.; Illingworth, D.R. Reduction of plasma lipids, lipoproteins, and apoproteins by dietary fish oils in patients with hypertriglyceridemia. N. Engl. J. Med. 1985, 312, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Small, D.M. The effects of glycerides structure on absorption and metabolism. Ann. Rev. Nutr. 1991, 11, 413–434. [Google Scholar] [CrossRef] [PubMed]
- Arterburn, L.M.; Hall, E.B.; Oken, H. Distribution, interconversion, and dose response of n-3 fatty acids in humans. Am. J. Clin. Nutr. 2006, 83, 1467S–1476S. [Google Scholar] [CrossRef]
- Morley, N.; Kuksis, A. Positional specificity of lipoprotein lipase. J. Biol. Chem. 1972, 247, 6389–6393. [Google Scholar]
- Querques, G.; Forte, R.; Souied, E.H. Retina and omega-3. J. Nutr. Metab. 2011, 2011, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.; Zirpoli, H.; Qi, K. n-3 fatty acids modulate adipose tissue inflammation and oxidative stress. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 124–132. [Google Scholar] [CrossRef]
- Anderson, B.M.; Ma, D.W. Are all n-3 polyunsaturated fatty acids created equal? Lipids Health Dis. 2009, 8, 33–53. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Hernandez, C.; Thakkar, S.K.; Moulin, J.; Oliveira, M.; Masserey-Elmelegy, I.; Dionisi, F.; Destaillats, F. Benefits of structured and free monoacylglycerols to deliver eicosapentaenoic (EPA) in a model of lipid malabsorption. Nutrients 2012, 4, 1781–1793. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Hernandez, C.; Destaillats, F.; Thakkar, S.K.; Goulet, L.; Wynn, E.; Grathwohl, D.; Roessle, C.; de Giorgi, S.; Tappy, L.; Giuffrida, F.; et al. Monoacylglycerol-enriched oil increases EPA/DHA delivery to circulatory system in humans with induced lipid malabsorption conditions. J. Lipid Res. 2016, 57, 2208–2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chase, H.P.; Welch, N.N.; Rabaglia, M.E.; Dupont, J. Linoleic acid absorption in children with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 1982, 1, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Christophe, A.; Verdonk, G.; Robberecht, E.; Mahathanakhun, R. Effect of supplementing medium chain triglycerides with linoleic acid-rich monoglycerides on severely disturbed serum lipid fatty acid patterns in patients with cystic fibrosis. Ann. Nutr. Metab. 1985, 29, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Brunton, S.; Collins, N. Differentiating prescription omega-3-acid ethyl esters (P-OM3) from dietary-supplement omega-3 fatty acids. Curr. Med. Res. Opin. 2007, 23, 1139–1145. [Google Scholar] [CrossRef]
- Lawson, L.D.; Hughes, B.G. Human absorption of fish oil fatty acids as triacylglycerols, free acids, or ethyl esters. Biochem. Biophys. Res. Commun. 1988, 152, 328–335. [Google Scholar] [CrossRef]
- el Boustani, S.; Colette, C.; Monnier, L.; Descomps, B.; Crastes de Paulet, A.; Mendy, F. Enteral absorption in man of eicosapentaenoic acid in different chemical forms. Lipids 1987, 22, 711–774. [Google Scholar] [CrossRef]
- Davidson, M.H.; Johnson, J.; Rooney, M.W.; Kyle, M.L.; Kling, D.F. A novel omega-3 free fatty acid formulation has dramatically improved bioavailability during a low-fat diet compared with omega-3-acid ethyl esters: The ECLIPSE (Epanova® compared to Lovaza® in a pharmacokinetic single-dose evaluation) study. J. Clin. Lipidol. 2012, 6, 573–584. [Google Scholar] [CrossRef]
- Mu, H.; Høy, C.E. The digestion of dietary triacylglycerols. Prog. Lipid Res. 2004, 43, 105–133. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, J.; et al. REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Eng. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Skulas-Ray, A.C.; Wilson, P.W.F.; Harris, W.S.; Brinton, E.A.; Kris-Etherton, P.M.; Richter, C.K.; Jacobson, T.A.; Engler, M.B.; Miller, M.; Robinson, J.G.; et al. American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Omega-3 fatty acids for the management of hypertriglyceridemia: A science advisory from the American Heart Association. Circulation 2019, 140, e673–e691. [Google Scholar]
- Shaikh, N.A.; Yantha, J.; Shaikh, S.; Rowe, W.; Laidlaw, M.; Cockerline, C.; Ali, A.; Holub, B.; Jackowski, G. Efficacy of a unique omega-3 formulation on the correction of nutritional deficiency and its effects on cardiovascular disease risk factors in a randomized controlled VASCAZEN® REVEAL Trial. Mol. Cell Biochem. 2014, 396, 9–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banno, F.; Doisaki, S.; Shimizu, N.; Fujimoto, K. Lymphatic absorption of docosahexaenoic acid given as monoglyceride, diglyceride, triglyceride, and ethyl ester in rats. J. Nutr. Sci. Vitaminol. 2002, 48, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C. The role of marine omega-3 (n-3) fatty acids in inflammatory processes, atherosclerosis and plaque stability. Mol. Nut. Food Res. 2012, 56, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Stallings, V.A.; Mondick, J.T.; Schall, J.I.; Barrett, J.S.; Wilson, M.; Mascarenhas, M.R. Diagnosing malabsorption with systemic lipid profiling: Pharmacokinetics of pentadecanoic acid and triheptadecanoic acid following oral administration in healthy subjects and subjects with cystic fibrosis. Int. J. Clin. Pharmacol. Ther. 2013, 51, 263–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalivianakis, M.; Verkade, H.J. The mechanisms of fat malabsorption in cystic fibrosis patients. Nutrition 1999, 15, 167–169. [Google Scholar]
- Fieker, A.; Philpott, J.; Armand, M. Enzyme replacement therapy for pancreatic insufficiency: Present and future. Clin. Exp. Gastroenterol. 2011, 4, 55–73. [Google Scholar]
- Yen, C.L.; Stone, S.J.; Cases, S.; Zhou, P.; Farese, R.V., Jr. Identification of a gene encoding MGAT1, a monoacylglycerol acyltransferase. Proc. Natl. Acad Sci. USA 2002, 99, 8512–8517. [Google Scholar] [CrossRef] [Green Version]
- Yen, C.L.; Farese, R.V., Jr. MGAT2, a monoacylglycerol acyltransferase expressed in the small intestine. J. Biol. Chem. 2003, 278, 18532–18537. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.; Cantin, A.M.; Vézina, F.A.; Fortin, S.T. The Efficacy of MAG-DHA for Correcting AA/DHA Imbalance of Cystic Fibrosis Patients. Mar. Drugs 2018, 16, 184. [Google Scholar] [CrossRef] [Green Version]
- Hentschel, J.; Müller, U.; Doht, F.; Fischer, N.; Böer, K.; Sonnemann, J.; Hipler, C.; Hünniger, K.; Kurzai, O.; Markert, U.R.; et al. Influences of nasal lavage collection-, processing- and storage methods on inflammatory markers--evaluation of a method for non-invasive sampling of epithelial lining fluid in cystic fibrosis and other respiratory diseases. J. Immunol. Methods 2014, 404, 41–51. [Google Scholar] [CrossRef]
- Cruz-Hernandez, C.; Thakkar, S.K.; Masserey-Elmelegy, I.; Buosi, W.; Fontannaz, P.; Giuffrida, F. Quantification of fatty acids in erythrocytes and plasma by fast gas chromatography. J. Sep. Sci. 2017, 40, 3289–3300. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, C.; Masi, A.; Sansone, A.; Giacometti, G.; Vita Larocca, A.; Menounou, G.; Scanferlato, R.; Tortorella, S.; Rota, D.; Conti, M.; et al. Fatty Acids in Membranes as Homeostatic, Metabolic and Nutritional Biomarkers: Recent advancements in analytics and diagnostics. Diagnostics 2017, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Wakil, A.; Mir, M.; Mellor, D.D.; Mellor, S.F.; Atkin, S.L. The bioavailability of eicosapentaenoic acid from reconstituted triglyceride fish oil is higher than that obtained from the triglyceride and monoglyceride forms. Asia Pac. J. Clin. Nutr. 2010, 19, 499–505. [Google Scholar] [PubMed]
- Christensen, M.S.; Høy, C.E.; Becker, C.C.; Redgrave, T.G. Redgrave. Intestinal absorption and lymphatic transport of eicosapentaenoic (EPA), docosahexaenoic (DHA), and decanoic acids: Dependence on intramolecular triacylglycerol structure. Am. J. Clin. Nutr. 1995, 61, 56–61. [Google Scholar] [CrossRef] [PubMed]
- AstraZeneca, FDA Approves EPANOVA for the Treatment of Adults with Severe Hypertriglkyceridemia Press Release. Wilmintton, DE: AstraZeneca Unitred States: 6 May 2014. Available online: http://www1.astrazeneca-us.com/media/press-releases/Article/20140506-epanova-press-release (accessed on 6 April 2020).
- Harris, W.S. n-3 fatty acids and serum lipoproteins: Human studies. Am. J. Clin. Nutr. 1997, 65, 1645S–1654S. [Google Scholar] [CrossRef]
- Collins, N.; Tighe, A.P.; Brunton, S.A.; Kris-Etherton, P.M. Differences between dietary supplement and prescription drug omega-3 fatty acid formulations: A legislative and regulatory perspective. J. Am. Coll. Nutr. 2008, 27, 659–666. [Google Scholar] [CrossRef]
- Zierenberg, O.; Grundy, S.M. Intestinal absorption of polyenephosphatidylcholine in man. J. Lipid Res. 1982, 23, 1136–1142. [Google Scholar]
- Destaillats, F.; Oliveira, M.; Bastic Schmid, V.; Masserey-Elmelegy, I.; Giuffrida, F.; Thakkar, S.K.; Dupuis, L.; Gosoniu, M.L.; Cruz-Hernandez, C. Comparison of the Incorporation of DHA in Circulatory and Neural Tissue When Provided as Triacylglycerol (TAG), Monoacylglycerol (MAG) or Phospholipids (PL) Provides New Insight into Fatty Acid Bioavailability. Nutrients 2018, 10, 620. [Google Scholar] [CrossRef] [Green Version]
- Landon, C.; Kerner, J.A.; Castillo, R.; Adams, L.; Whalen, R.; Lewiston, N.J. Oral correction of essential fatty acid deficiency in cystic fibrosis. J. Parenter. Enteral Nutr. 1981, 5, 501–504. [Google Scholar] [CrossRef]
- Christophe, A.; Verdonk, G.; Robberecht, E.; Mahathanakhun, R. Fast improvement of severely distributed serum-lipid-fatty acid patterns in cystic fibrosis by means of feeding structure-modified natural fats. Archs Pysiol. Biochim. 1982, 90, B7. [Google Scholar]
- Lepage, G.; Yesair, D.W.; Ronco, N.; Champagne, J.; Bureau, N.; Chemtob, S.; Bérubé, D.; Roy, C.C. Effect of an organized lipid matrix on lipid absorption and clinical outcomes in patients with cystic fibrosis. J. Pediatr. 2002, 141, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.P.; Dupont, J. Abnormal levels of prostaglandins and fatty acids in blood of children with cystic fibrosis. Lancet 1978, 2, 236–238. [Google Scholar] [CrossRef]
- Panchaud, A.; Sauty, A.; Kernen, Y.; Decosterd, L.A.; Buclin, T.; Boulat, O.; Hug, C.; Pilet, M.; Roulet, M. Biological effects of a dietary omega-3 polyunsaturated fatty acids supplementation in cystic fibrosis patients: A randomized, crossover placebo-controlled trial. Clin. Nutr. 2006, 25, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Keen, C.; Olin, A.C.; Eriksson, S.; Ekman, A.; Lindblad, A.; Basu, S.; Beermann, C.; Strandvik, B. Supplementation with fatty acids influences the airway nitric oxide and inflammatory markers in patients with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 537–544. [Google Scholar] [CrossRef]
- Alicandro, G.; Faelli, N.; Gagliardini, R.; Santini, B.; Magazzù, G.; Biffi, A.; Risé, P.; Galli, C.; Tirelli, A.S.; Loi, S.; et al. A randomized placebo-controlled study on high-dose oral algal docosahexaenoic acid supplementation in children with cystic fibrosis. Prostaglandins Leukot Essent Fatty Acids 2013, 88, 163–169. [Google Scholar] [CrossRef]
- Lloyd-Still, J.D.; Powers, C.A.; Hoffman, D.R.; Boyd-Trull, K.; Lester, L.A.; Benisek, D.C.; Arterburn, L.M. Bioavailability and safety of a high dose of docosahexaenoic acid triacylglycerol of algal origin in cystic fibrosis patients: A randomized, controlled study. Nutrition 2006, 22, 36–46. [Google Scholar] [CrossRef]
- Lawrence, R.; Sorrell, T. Eicosapentaenoic acid in cystic fibrosis: Evidence of a pathogenetic role for leukotriene B4. Lancet 1993, 342, 465–469. [Google Scholar] [CrossRef]
- Dessì, M.; Noce, A.; Bertucci, P.; Manca di Villahermosa, S.; Zenobi, R.; Castagnola, V.; Addessi, E.; Di Daniele, N. Atherosclerosis, dyslipidemia, and inflammation: The significant role of polyunsaturated fatty acids. ISRN Inflamm. 2013, 2013, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Richter, W.O.; Jacob, B.G.; Ritter, M.M.; Schwandt, P. Treatment of primary chylomicronemia due to familial hypertriglyceridemia by omega-3 fatty acids. Metabolism 1992, 41, 1100–1105. [Google Scholar] [CrossRef]
- Löhr, J.M.; Panic, N.; Vujasinovic, M.; Verbeke, C.S. The ageing pancreas: A systematic review of the evidence and analysis of the consequences. J. Intern. Med. 2018, 283, 446–460. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trial | Population | Age | Capsules | ACTIVE ARM | CONTROL ARM | ||
|---|---|---|---|---|---|---|---|
| OM3 | /Day | (mg/day) | (mg/day) | ||||
| OM3-MAG | OM3-TAG | ||||||
| EPA | DHA | EPA | DHA | ||||
| A. MAG | Normal weight | Adult | 5 | 1655 | 1275 | ||
| Ethyl ester | 4 | 1700 | 1380 | ||||
| FFA | 4 | 1748 | 1516 | ||||
| B. MAG-TAG | Obese/overweight | Adult | 9 | 560 | 362 | 774 | 564 |
| C. MAG-TAG | Cystic fibrosis | 4–10 years old | 4 | 249 | 161 | 258 | 188 |
| 11–18 years old | 8 | 498 | 322 | 516 | 376 | ||
| OIL | Clinical Trial A OM3: MAG, Ethyl Ester. FFA | Clinical Trial B OM3: MAG, TAG | Clinical Trial C OM3: MAG, TAG |
|---|---|---|---|
| Inclusion | Healthy adults (18–65 years old) BMI normal to overweight range (18.5–29.9 kg/m2) | Overweight or obese adults (18–65 years old) BMI 25.0 to 34.9 kg/m2 (inclusive) | 16 female/male patients diagnosed with CF and exocrine pancreatic insufficiency from 4–18 years old |
| Exclusion |
|
|
|
| OM3-MAG | OM3-Ethyl Ester | OM3-FFA | OM3-MAG | OM3-TAG | |
|---|---|---|---|---|---|
| Capsule | 1 g | 1 g | 1 g | 0.380 g | 0.380 g |
| Total OM3- (% w/w) as: | MAG 90 | Ethyl ester 92 | FFA 91 | MAG 92 | TAG 90 |
| EPA (mg) | 331 | 425 | 437 | 62.25 | 64.5 |
| DHA (mg) | 255 | 345 | 379 | 40.25 | 47 |
| SFA (mg) | <1.0 | <1.0 | <1.0 | 22.8 | 38 |
| Other FA | 400 | 230 | 184 | 277 | 268 |
| OM3 Study Group | OM3 Study Group Comparison | |||||
|---|---|---|---|---|---|---|
| MAG (n = 21) | FFA (n = 21) | Ethyl Ester (n = 23) | MAG-Ethyl Ester | FFA-Ethyl Ester | MAG-FFA | |
| AUC0-24 h EPA | 1486 ± 626 | 1496 ± 734 | 163 ± 251 | 3.41-fold p < 0.001 | 3.60-fold p < 0.001 | 0.95-fold, p = 0.60 |
| C max EPA | 143 ± 71 | 124 ± 48 | 17 ± 10 | 9.96-fold p < 0.001 | 8.58-fold p < 0.001 | 1.16-fold, p = 0.31 |
| T max EPA | 6.3 ± 4.4 | 5.2 ± 0.9 | 9.7 ± 6.5 | 3 h, p = 0.003 | 3 h, p < 0.001 | 0 h, p = 0.47 |
| AUC0-24h DHA | 1206 ± 600 | 1356 ± 676 | 562 ± 695 | 2.10-fold p < 0.001 | 2.34-fold, p < 0.001 | 0.90-fold, p = 0.49 |
| C max DHA | 113 ± 55 | 117 ± 39 | 44 ± 25 | 2.37-fold p < 0.001 | 2.48-fold p < 0.001 | 0.96-fold, p = 0.72 |
| T max DHA | 4.9 ± 0.9 | 5.7 ± 1.7 | 16.0 ± 8.3 | 7 h, p < 0.001 | 7 h, p < 0.001 | 0 h, p = 0.07 |
| Study Groups | ||
|---|---|---|
| OM3-MAG (n = 29) | OM3-TAG (n = 30) | |
| Age (years) | 44.72 ± 9.83 | 44.10 ± 10.24 |
| Male | 11 (37.93%) | 12 (40.00%) |
| Female | 18 (62.07%) | 18 (60.00%) |
| Weight (kg) | 82.60 ± 12.86 | 82.12 ± 12.90 |
| BMI (kg/m2) | 29.64 ± 2.67 | 29.48 ± 2.77 |
| Total cholesterol (mg/dl) | 193.31 ± 29.08 | 194.30 ± 29.09 |
| LDL-C (mg/dl) | 117.41 ± 23.48 | 118.57 ± 23.92 |
| HDL-C (mg/dl) | 54.24 ± 10.91 | 53.97 ± 10.83 |
| Triglycerides (mg/dl) | 110.00 ± 37.59 | 110.53 ± 37.05 |
| Study Groups | Study Group Comparison | ||
|---|---|---|---|
| OM3-MAG (n = 29) | OM3-TAG (n = 30) | OM3-MAG/OM3-TAG | |
| AUC0-24h EPA | 278 ± 108 | 236 ± 76.8 | 16% higher # |
| C max EPA | 18.2 ± 8.27 | 17.3 ± 6.8 | 29% higher # |
| T max EPA | 5 (3, 12) * | 6 (5, 12) | 5 vs. 6 p < 0.05 |
| AUC0-24h DHA | 173 ± 98 | 189 ± 105 | 11% lower ## |
| C max DHA | 113 ± 55 | 117 ± 39 | No difference |
| T max DHA | 5 (3, 10) * | 6 (4, 12) | 5 vs. 6 p < 0.05 |
| Study Groups | Age | Weight | LCI | FEV1 | FVC | MEF | IL-1β | IL-6 | IL-8 | IP-10 | NE | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DAY | Years | Kg | Log pg/mL | |||||||||
| OM3-TAG n = 8 | 0 | 11.8 ± 3.4 | 38.7 ± 13.6 | 11.75 ± 3.2 | 2.67 ± 1.27 | 2.02 ± 0.99 | 2.23 ± 1.64 | 0.21 ± 0.49 | 0.46 ± 1.64 | 1.79 ± 0.57 | 0.51 ± 0.61 | 2.36 ± 0.36 |
| Mean ± SD | 84 | 39.7 ± 13.6 | 12.29 ± 3.3 | 2.68 ± 1.25 | 2.05 ± 0.96 | 2.36 ± 1.67 | 0.25 ± 0.45 | 0.61 ± 1.67 | 1.93 ± 0.44 | 0.69 ± 0.58 | 2.45 ± 0.40 | |
| OM3-MAG n = 7 | 0 | 11.5 ± 3.6 | 39.3 ± 13.5 | 11.6 ± 3.6 | 2.71 ± 1.28 | 2.20 ± 1.22 | 1.76 ± 0.99 | 0.21 ± 0.28 | 0.67 ± 0.33 | 1.86 ± 0.55 | 0.81 ± 0.65 | 2.62 ± 0.35 |
| Mean ± SD | 84 | 40.04 ± 13.4 | 12.70 ± 2.7 | 2.77 ± 1.34 | 2.23 ± 1.21 | 1.73 ± 0.93 | 0.18 ± 0.44 | 0.61 ± 0.64 | 1.89 ± 0.59 | 0.67 ± 0.86 | 2.53 ± 0.60 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuenoud, B.; Rochat, I.; Gosoniu, M.L.; Dupuis, L.; Berk, E.; Jaudszus, A.; Mainz, J.G.; Hafen, G.; Beaumont, M.; Cruz-Hernandez, C. Monoacylglycerol Form of Omega-3s Improves Its Bioavailability in Humans Compared to Other Forms. Nutrients 2020, 12, 1014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041014
Cuenoud B, Rochat I, Gosoniu ML, Dupuis L, Berk E, Jaudszus A, Mainz JG, Hafen G, Beaumont M, Cruz-Hernandez C. Monoacylglycerol Form of Omega-3s Improves Its Bioavailability in Humans Compared to Other Forms. Nutrients. 2020; 12(4):1014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041014
Chicago/Turabian StyleCuenoud, Bernard, Isabelle Rochat, Maria Laura Gosoniu, Lenaick Dupuis, Evan Berk, Anke Jaudszus, Jochen G. Mainz, Gaudenz Hafen, Maurice Beaumont, and Cristina Cruz-Hernandez. 2020. "Monoacylglycerol Form of Omega-3s Improves Its Bioavailability in Humans Compared to Other Forms" Nutrients 12, no. 4: 1014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12041014