Clinical and Nutritional Effectiveness of a Nutritional Protocol with Oligomeric Enteral Nutrition in Patients with Oncology Treatment-Related Diarrhea

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Study Population
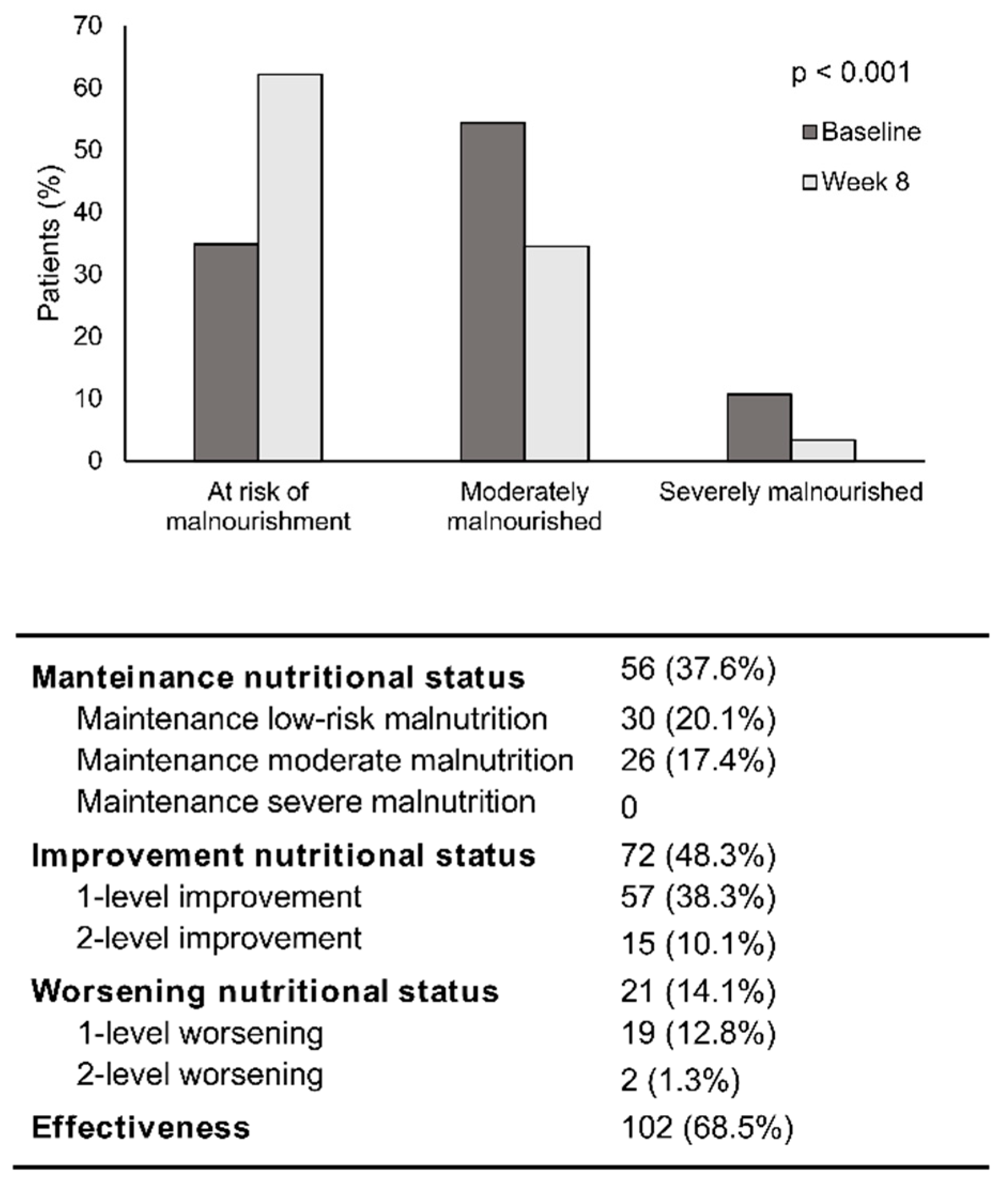
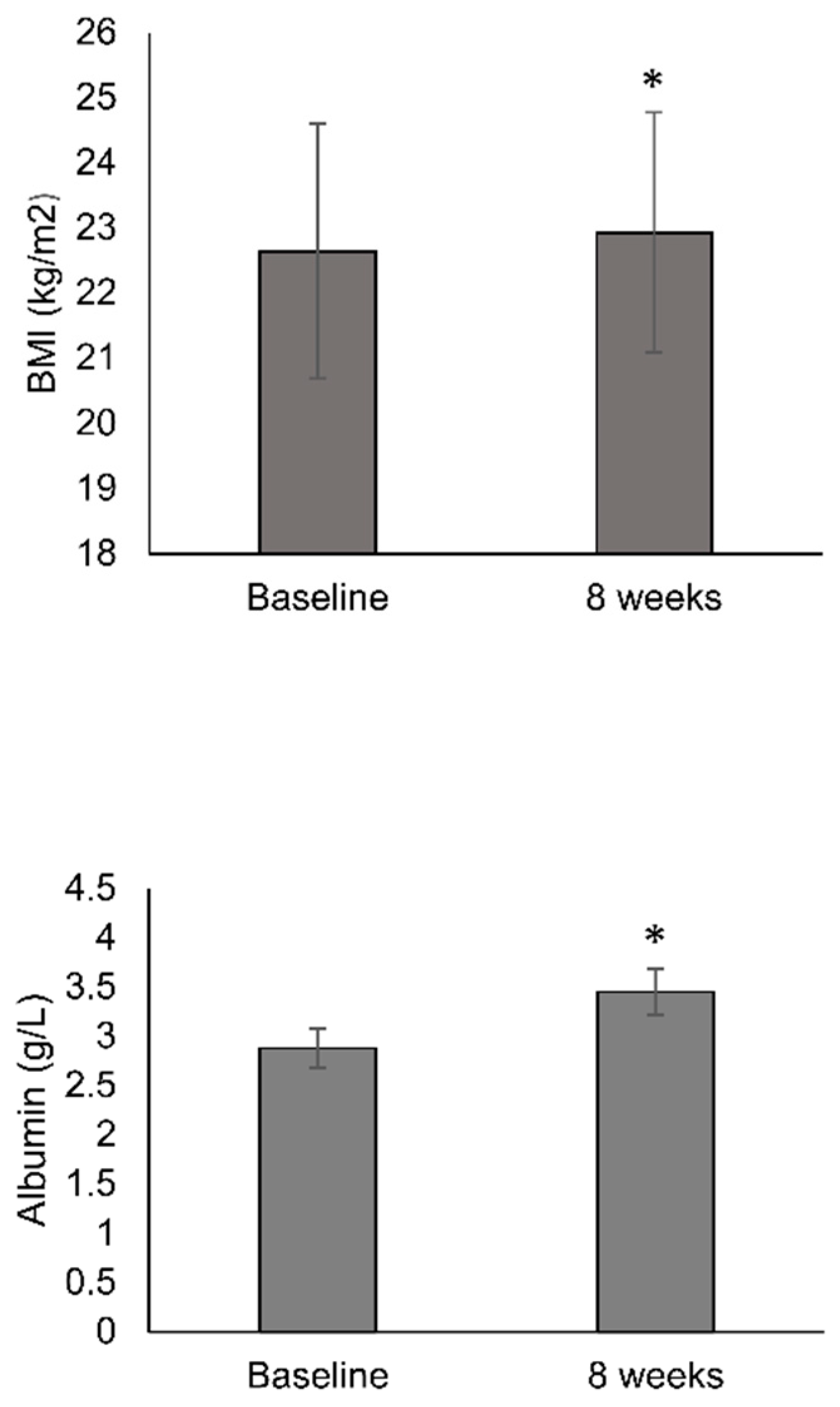
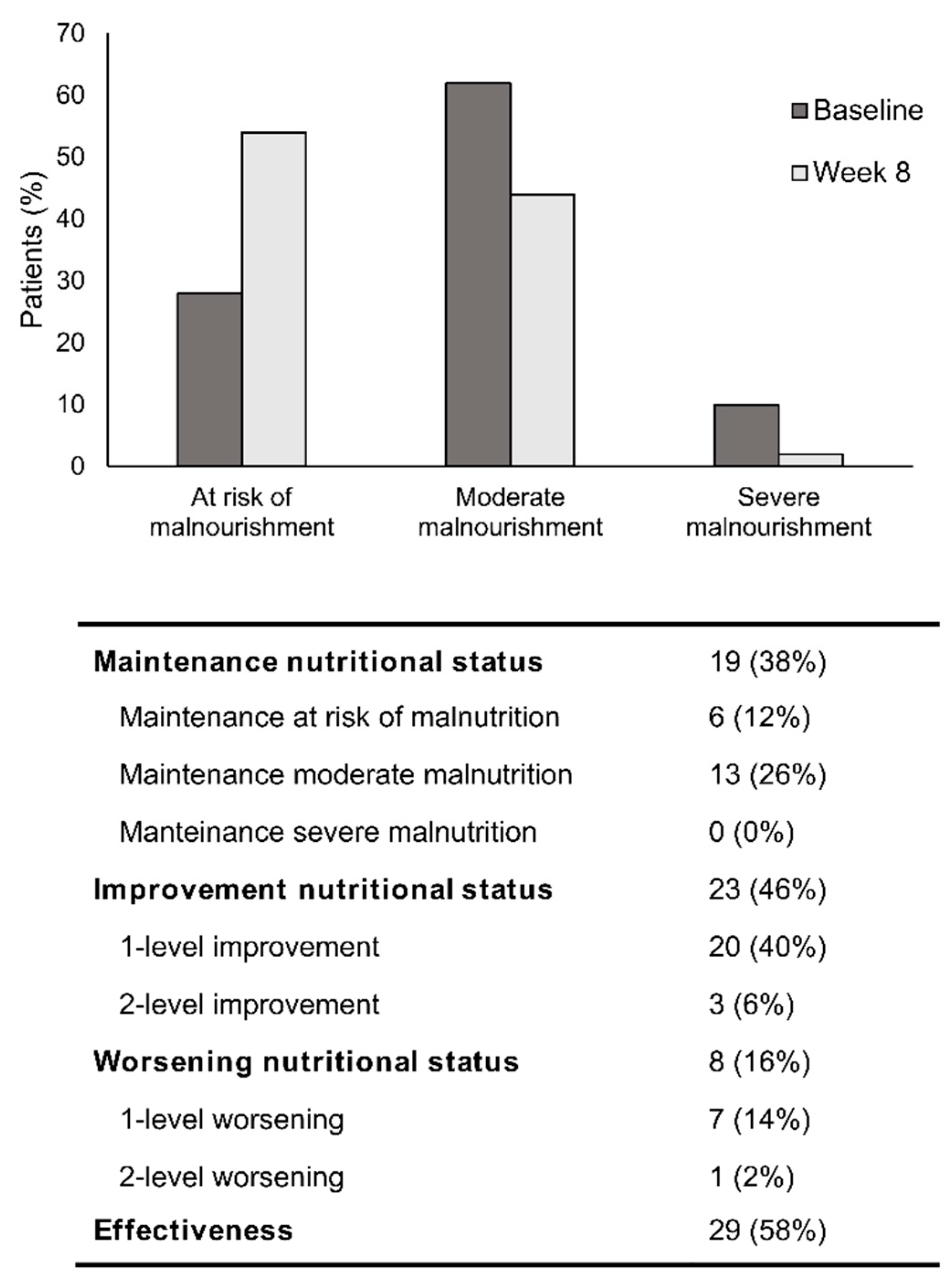
3.2. Nutritional Status
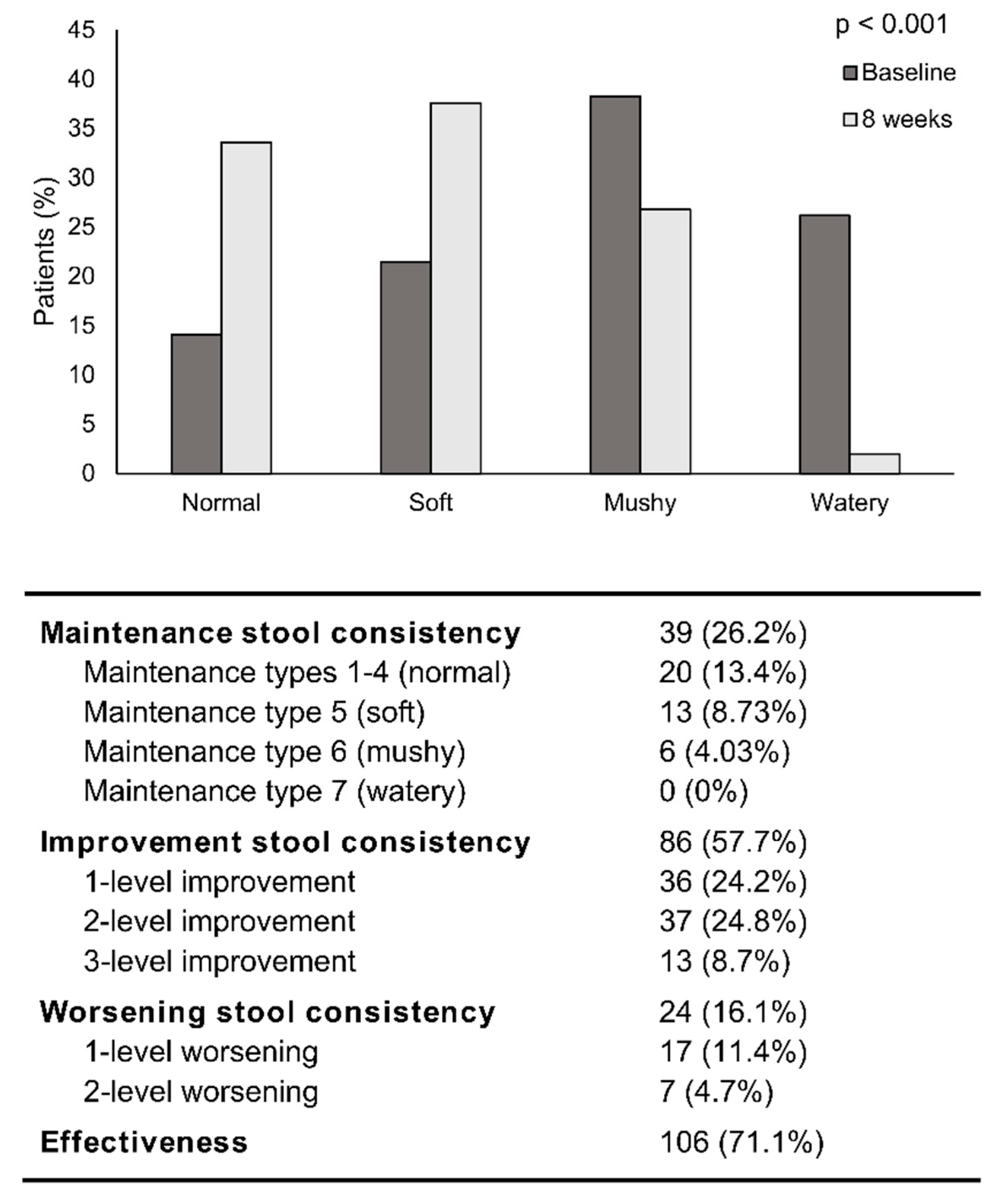
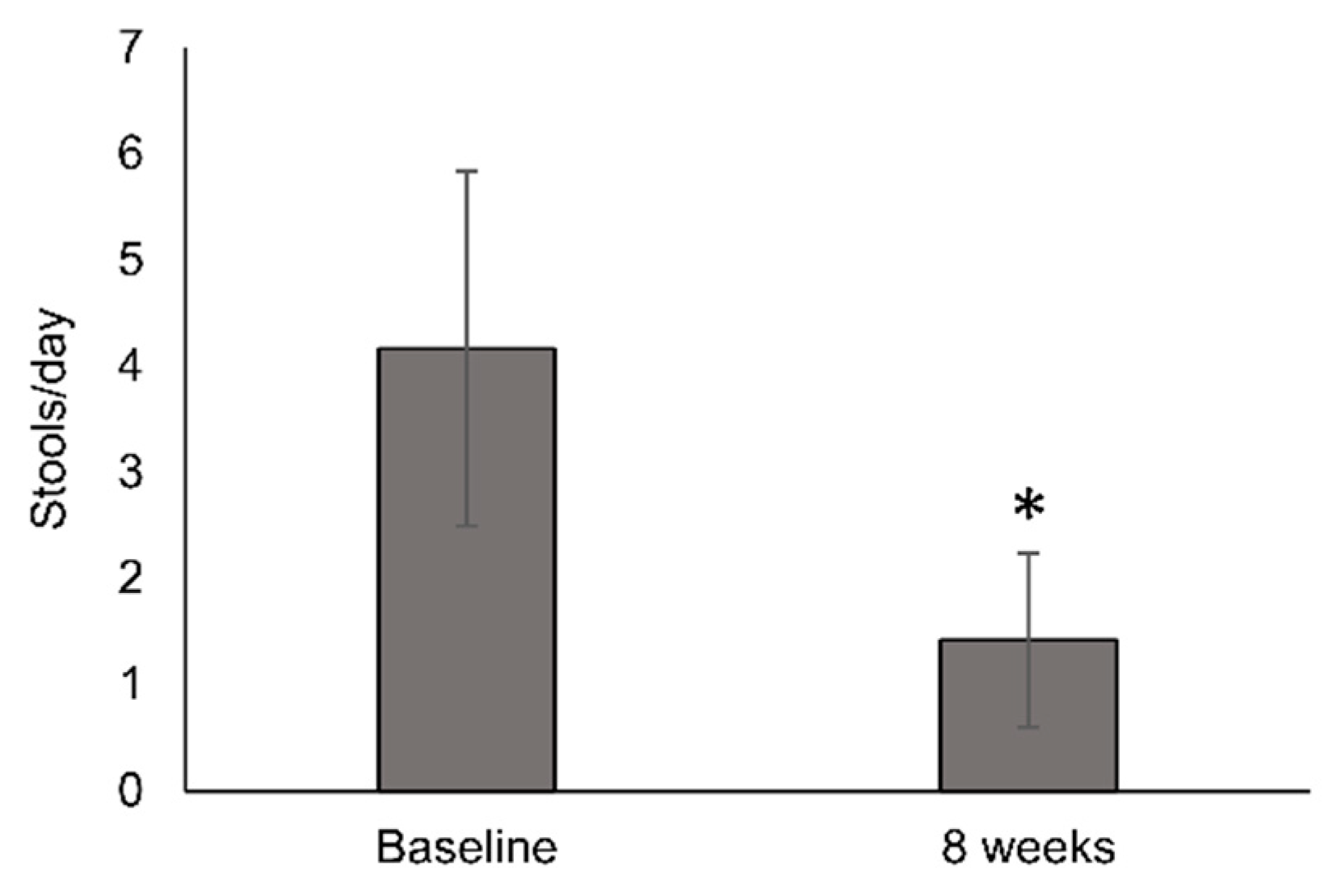
3.3. Stool Consistency and Frequency
3.4. Patients with Persistent Diarrhea
3.5. Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Elting, L.S.; Cooksley, C.; Chambers, M.; Cantor, S.B.; Manzullo, E.; Rubenstein, E.B. The burdens of cancer therapy: Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer 2003, 98, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.; Kravits, K. Symptoms and their impact on nutrition. Semin. Oncol. Nurs. 2000, 16, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Richardson, G.; Dobish, R. Chemotherapy induced diarrhea. J. Oncol. Pharm. Pract. 2007, 13, 181–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreyev, J.; Ross, P.; Donnellan, C.; Lennan, E.; Leonard, P.; Waters, C.; Wedlake, L.; Bridgewater, J.; Glynne-Jones, R.; Allum, W.; et al. Guidance on the management of diarrhoea during cancer chemotherapy. Lancet Oncol. 2014, 15, e447–e460. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.M.; Voss, A.C.; Piemonte, T. Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310. [Google Scholar] [CrossRef]
- Dranitsaris, G.; Maroun, J.; Shah, A. Estimating the cost of illness in colorectal cancer patients who were hospitalized for severe chemotherapy-induced diarrhea. Can. J. Gastroenterol. 2005, 19, 83–87. [Google Scholar] [CrossRef]
- Benson, A.B.; Ajani, J.A.; Catalano, R.B.; Engelking, C.; Kornblau, S.M.; Martenson, J.A.; McCallum, R.; Mitchell, E.P.; O’Dorisio, T.M.; Vokes, E.E.; et al. Recommended guidelines for the treatment of cancer treatment-induced diarrhea. J. Clin. Oncol. 2004, 22, 2918–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, D.E.; Boers-Doets, C.B.; Bensadoun, R.J.; Herrstedt, J. Management of oral and gastrointestinal mucosal injury: ESMO Clinical Practice Guidelines for diagnosis, treatment, and follow-up. Ann. Oncol. 2015, 26, v139–v151. [Google Scholar] [CrossRef] [Green Version]
- Wedlake, L.J.; Shaw, C.; Whelan, K.; Andreyev, H.J.N. Systematic review: The efficacy of nutritional interventions to counteract acute gastrointestinal toxicity during therapeutic pelvic radiotherapy. Aliment. Pharmacol. Ther. 2013, 37, 1046–1056. [Google Scholar] [CrossRef] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Peterson, S.J. Enteral Nutrition Formulas: Which Formula Is Right for Your Adult Patient? Nutr. Clin. Pract. 2009, 24, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Paris, A.; Martinez-García, M.; Martinez-Trufero, J.; Lambea-Sorrosal, J.; Calvo-Gracia, F.; López-Alaminos, M.E. Oligomeric enteral nutrition in undernutrition, due to oncology treatment-related diarrhea. Systematic review and proposal of an algorithm of action. Nutrients 2019, 11, 1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Kitagawa, T.; Matsumoto, K. Impact of Elemental Diet on Mucosal Inflammation in Patients with Active Crohnʼs Disease: Cytokine Production and Endoscopic and Histological Findings. Inflamm. Bowel Dis. 2005, 11, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Detsky, A.; Baker, J.M.; Johnston, N.; Whittaker, S.; Mendelson, R.; Jeejeebhoy, K. What is subjective global assessment of nutritional status? J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.J.; Heaton, K.W. Stool Form Scale as a Useful Guide to Intestinal Transit Time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Ohkura, Y.; Ueno, M.; Shindoh, J.; Iizuka, T.; Udagawa, H. Randomized controlled trial on efficacy of oligomeric formula (HINE E-GEL®) versus polymeric formula (MEIN®) enteral nutrition after esophagectomy for esophageal cancer with gastric tube reconstruction. Dis. Esophagus 2019, 32, 1–10. [Google Scholar] [CrossRef]
- Harada, K.; Ferdous, T.; Horinaga, D.; Uchida, K.; Mano, T.; Mishima, K.; Park, S.; Hanazawa, H.; Takahashi, S.; Okita, A.; et al. Efficacy of elemental diet on prevention for chemoradiotherapy-induced oral mucositis in patients with oral squamous cell carcinoma. Support. Care Cancer 2016, 24, 953–959. [Google Scholar] [CrossRef]
- Harada, K.; Minami, H.; Ferdous, T.; Kato, Y.; Umeda, H.; Horinaga, D.; Uchida, K.; Park, S.; Hanazawa, H.; Takahashi, S.; et al. The Elental® elemental diet for chemoradiotherapy-induced oral mucositis: A prospective study in patients with oral squamous cell carcinoma. Mol. Clin. Oncol. 2018, 159–167. [Google Scholar] [CrossRef] [Green Version]
- Imamura, H.; Nishikawa, K.; Kishi, K.; Inoue, K.; Matsuyama, J.; Akamaru, Y.; Kimura, Y.; Tamura, S.; Kawabata, R.; Kawada, J.; et al. Effects of an Oral Elemental Nutritional Supplement on Post-gastrectomy Body Weight Loss in Gastric Cancer Patients: A Randomized Controlled Clinical Trial. Ann. Surg. Oncol. 2016, 23, 2928–2935. [Google Scholar] [CrossRef]
- Mcgough, C.; Wedlake, L.; Baldwin, C.; Hackett, C.; Norman, A.R.; Blake, P.; Harrington, K.; Tait, D.; Khoo, V.; Frost, G.; et al. Clinical trial: Normal diet vs. partial replacement with oral E028 formula for the prevention of gastrointestinal toxicity in cancer patients undergoing pelvic radiotherapy. Aliment. Pharmacol. Ther. 2008, 27, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Yasuda, T.; Doi, T.; Okayama, T.; Sakamoto, N.; Gen, Y.; Dohi, O.; Yoshida, N.; Kamada, K.; Uchiyama, K.; et al. The amino acid-rich elemental diet Elental® preserves lean body mass during chemo- or chemoradiotherapy for esophageal cancer. Oncol. Rep. 2016, 36, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, F.; Xin, F.; Yang, C.; Yang, D.; Mi, Y.; Yu, J.; Li, G. The Impact of Microbial Immune Enteral Nutrition on the Patients with Acute Radiation Enteritis in Bowel Function and Immune Status. Cell Biochem. Biophys. 2014, 69, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Toyomasu, Y.; Mochiki, E.; Yanai, M.; Suzuki, M.; Yanoma, T.; Kimura, A.; Kogure, N.; Ogata, K.; Kuwano, H. A prospective pilot study of an elemental nutritional supplement for prevention of oral mucositis during S-1 adjuvant chemotherapy for gastric cancer. Surg. Oncol. 2019, 29, 97–101. [Google Scholar] [CrossRef]
- Kong, H.; Kwon, O.K.; Yu, W. Changes of quality of life after gastric cancer surgery. J. Gastric Cancer 2012, 12, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Fuji, S.; Mori, T.; Khattry, N.; Cheng, J.; Do, Y.R.; Yakushijin, K.; Kohashi, S.; Fukuda, T.; Kim, S.W. Severe weight loss in 3 months after allogeneic hematopoietic SCT was associated with an increased risk of subsequent non-relapse mortality. Bone Marrow Transp. 2015, 50, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Morishita, T.; Tsushita, N.; Imai, K.; Sakai, T.; Miyao, K.; Sakemura, R.; Kato, T.; Niimi, K.; Ono, Y.; Sawa, M. The Efficacy of an Oral Elemental Diet in Patients Undergoing Hematopoietic Stem Cell Transplantation. Intern. Med. 2016, 55, 3561–3569. [Google Scholar] [CrossRef] [Green Version]
- Wall, C.L.; Gearry, R.B.; Day, A.S. Polymeric formula is more palatable than elemental formula to adults with Crohn’s disease. e-SPEN J. 2014, 9, e200–e203. [Google Scholar] [CrossRef]
- Tanaka, Y.; Ueno, T.; Yoshida, N.; Akutsu, Y.; Takeuchi, H.; Baba, H.; Matsubara, H.; Kitagawa, Y.; Yoshida, K. The effect of an elemental diet on oral mucositis of esophageal cancer patients treated with DCF chemotherapy: A multi-center prospective feasibility study (EPOC study). Esophagus 2018, 15, 239–248. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, S.J.D.; Lee, R.B.; Anderson, F.P.; Gennings, C.; Abou-Assi, S.; Clore, J.; Heuman, D.; Chey, W. Physiological effects of enteral and parenteral feeding on pancreaticobiliary secretion in humans. Am. J. Physiol. Liver Physiol. 2003, 284, G27–G36. [Google Scholar] [CrossRef] [Green Version]
- Ogata, Y.; Ishibashi, N.; Yamaguchi, K.; Uchida, S.; Kamei, H.; Nakayama, G.; Hirakawa, H.; Tanigawa, M.; Akagi, Y. Preventive effects of amino-acid-rich elemental diet Elental® on chemotherapy-induced oral mucositis in patients with colorectal cancer: A prospective pilot study. Support. Care Cancer 2016, 24, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, T.; Fujimoto, K.; Shima, Y.; Ogata, A.; Kumanogoh, A. Minimal neonatal transfer of certolizumab pegol in a Japanese patient with rheumatoid arthritis. Ann. Rheum. Dis. 2018, 77, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Laky, B.; Janda, M.; Cleghorn, G.; Obermair, A. Comparison of different nutritional assessments and body-composition measurements in detecting malnutrition among gynecologic cancer patients. Am. J. Clin. Nutr. 2008, 87, 1678–1685. [Google Scholar] [CrossRef]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 149 | |
|---|---|
| Age (years), Mean (SD) | 68.6 (12.6) |
| Median (min; max) | 69 (30; 92) |
| Gender, (%) | |
| Men | 82 (55.0%) |
| Woman | 67 (45.0%) |
| Weight (kg), Mean (SD) | 62.9 (12.1) |
| BMI (kg/m2), Mean (SD) | 22.6 (3.9) |
| Resectability (* n = 136) | |
| Unresectable | 64 (47.1%) |
| Localized | 72 (52.9%) |
| Type of treatment (* n = 131) | |
| Palliative | 65 (49.6%) |
| Curative | 66 (50.4%) |
| Treatment modality | |
| Chemotherapy | 56 (37.6%) |
| Radiotherapy | 24 (16.1%) |
| Chemotherapy + Radiotherapy | 69 (46.3%) |
| Targeted therapy | |
| Yes | 28 (18.8%) |
| No | 121 (81.2%) |
| Cytotoxic treatment | |
| Yes | 99 (66.4%) |
| No | 50 (33.6%) |
| Type of tumor | |
| Gynecologic/urologic | 29 (19.5%) |
| Colon | 78 (52.3%) |
| Esophagogastric | 22 (14.8%) |
| Other | 20 (13.4%) |
| Treatment Compliance (* n = 148) | |
|---|---|
| Total content prescribed | 107 (72.3%) |
| 2/3 bottle content prescribed | 31 (20.9%) |
| 1/2 bottle content prescribed | 10 (6.8%) |
| Treatment tolerance (*n = 147) | |
| Good tolerance | 118 (80.3%) |
| Moderate intolerance | 29 (19.7%) |
| Severe intolerance | 0 (0.0%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanz-Paris, A.; Martinez-Trufero, J.; Lambea-Sorrosal, J.; Calvo-Gracia, F.; Milà-Villarroel, R. Clinical and Nutritional Effectiveness of a Nutritional Protocol with Oligomeric Enteral Nutrition in Patients with Oncology Treatment-Related Diarrhea. Nutrients 2020, 12, 1534. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051534
Sanz-Paris A, Martinez-Trufero J, Lambea-Sorrosal J, Calvo-Gracia F, Milà-Villarroel R. Clinical and Nutritional Effectiveness of a Nutritional Protocol with Oligomeric Enteral Nutrition in Patients with Oncology Treatment-Related Diarrhea. Nutrients. 2020; 12(5):1534. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051534
Chicago/Turabian StyleSanz-Paris, Alejandro, Javier Martinez-Trufero, Julio Lambea-Sorrosal, Fernando Calvo-Gracia, and Raimon Milà-Villarroel. 2020. "Clinical and Nutritional Effectiveness of a Nutritional Protocol with Oligomeric Enteral Nutrition in Patients with Oncology Treatment-Related Diarrhea" Nutrients 12, no. 5: 1534. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051534