Red Bull Increases Heart Rate at Near Sea Level and Pulmonary Shunt Fraction at High Altitude in a Porcine Model

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Protocol
2.3. Statistical Analysis
3. Results
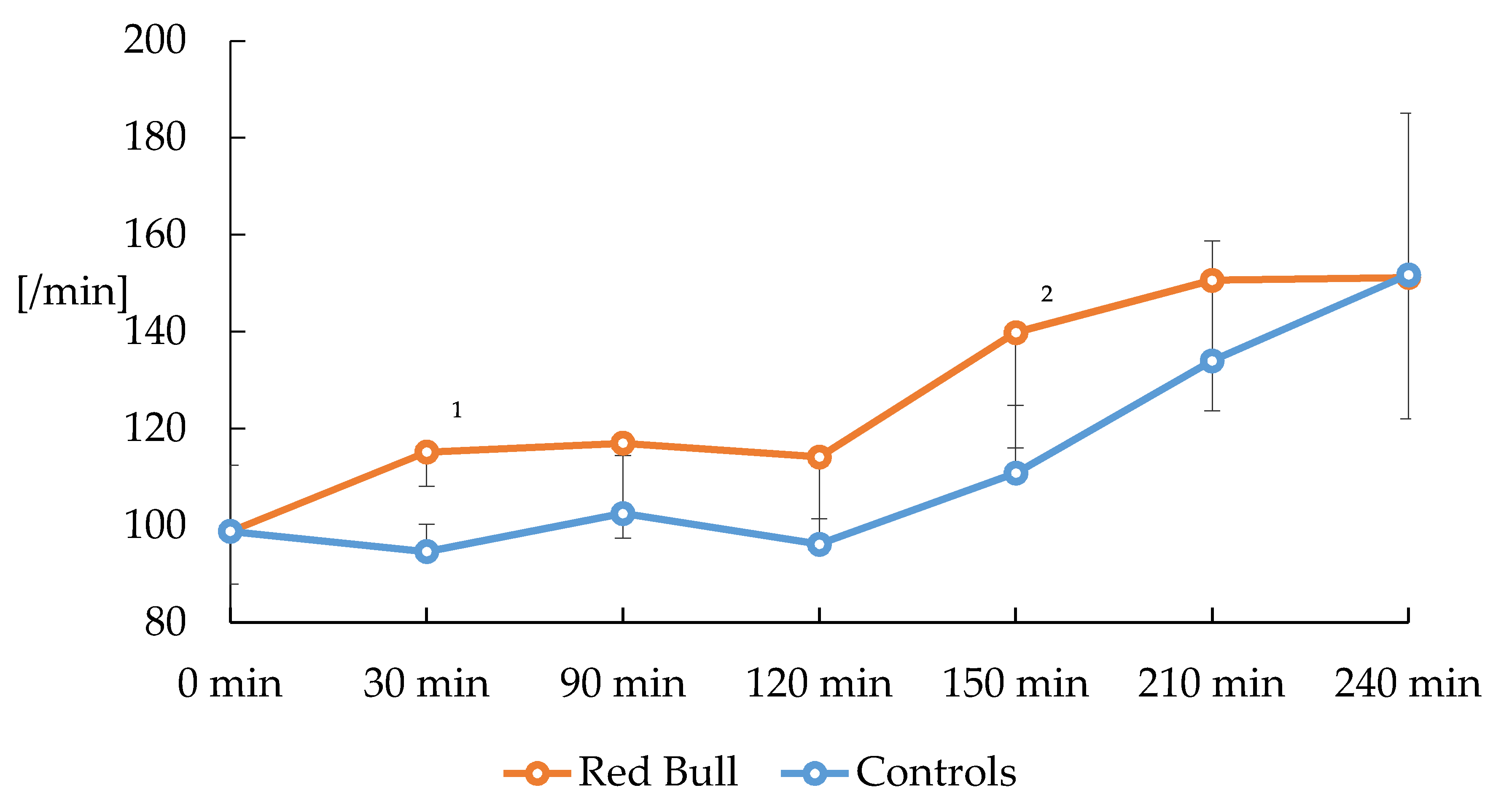
3.1. Hemodynamic Changes
3.2. Bloodgas Changes
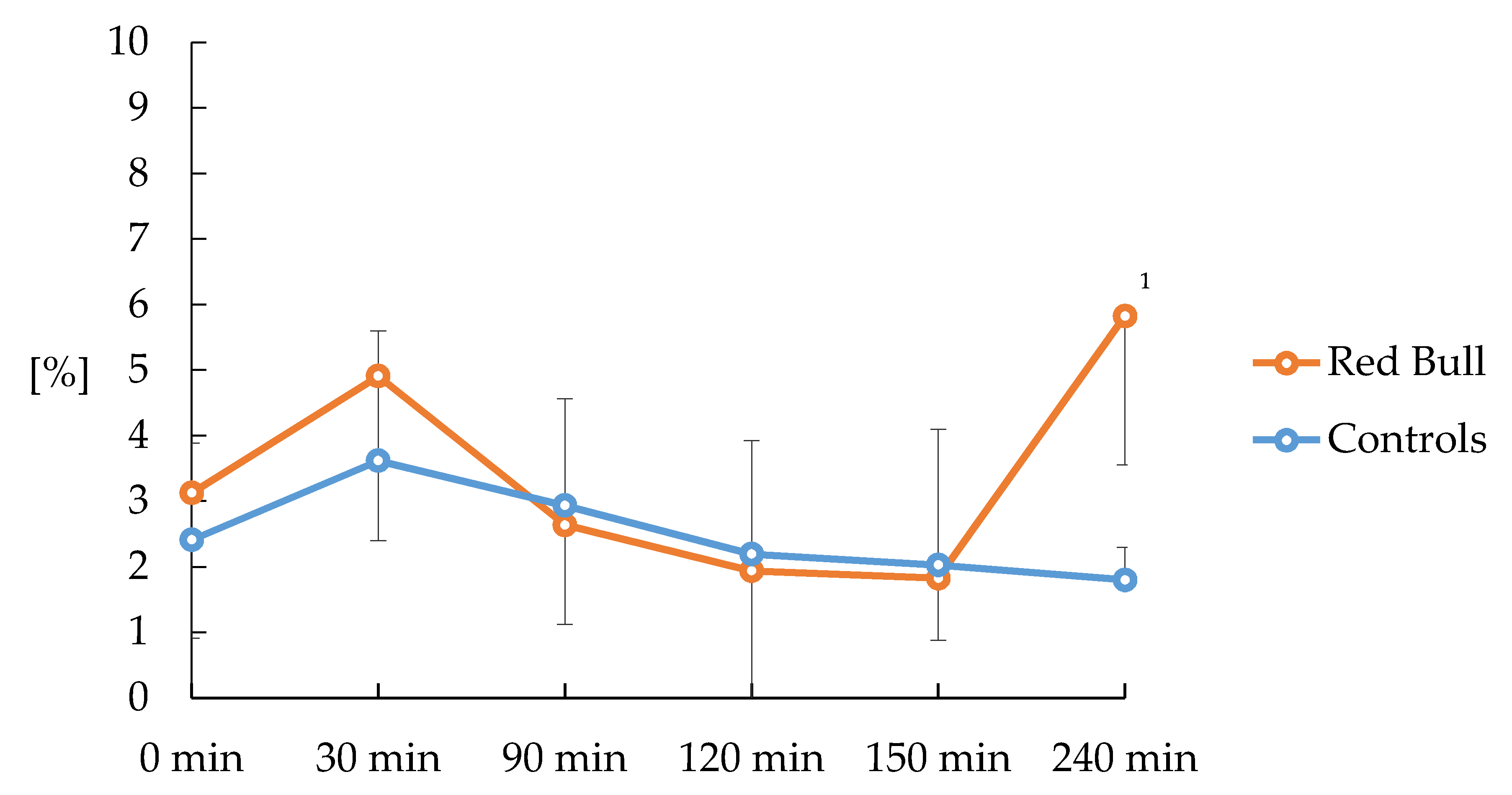
3.3. Ventilation/Perfusion Changes
4. Discussion
Limits
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CO | cardiac output |
| CO2 | carbon dioxide |
| CVD | central venous pressure |
| DBP | diastolic blood pressure |
| HPV | hypoxic pulmonary vasoconstriction |
| MAP | mean arterial blood pressure |
| LogSDQ | logarithmic deviation of standard of the mean of the distribution of perfusion |
| Mean of Q | mean of the distribution of perfusion |
| MIGET | multiple inert gas elimination technique |
| MPAP | mean pulmonary arterial blood pressure |
| MR | magnetic resonance |
| O2 | oxygen |
| PaO2 | arterial partial pressure of oxygen |
| PaCO2 | arterial partial pressure of carbon dioxide |
| PCWP | pulmonary capillary wedge pressure |
| PEEP | positive end-expiratory pressure |
| pH | arterial pH |
| PvO2 | mixed venous partial pressure of oxygen |
| PvCO2 | mixed venous partial pressure of carbon dioxide |
| RSS | remaining sum of squares |
| SBP | systolic blood pressure |
| TV | Tidal volumes |
| VA/Q | Ventilation/perfusion |
| VO2max | maximal oxygen consumption |
References
- Higgins, J.P.; Tuttle, T.D.; Higgins, C.L. Energy beverages: Content and safety. Mayo Clin. Proc. 2010, 85, 1033–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alford, C.; Cox, H.; Wescott, R. The effects of Red Bull Energy Drink on human performance and mood. Amino Acids 2001, 21, 139–150. [Google Scholar] [CrossRef]
- Grasser, E.K.; Yepuri, G.; Dulloo, A.G.; Montani, J.-P. Cardio- and cerebrovascular responses to the energy drink Red Bull in young adults: A randomized cross-over study. Eur. J. Nutr. 2014, 53, 1561–1571. [Google Scholar] [CrossRef] [Green Version]
- Franks, A.M.; Schmidt, J.M.; McCain, K.R.; Fraer, M. Comparison of the Effects of Energy Drink Versus Caffeine Supplementation on Indices of 24-Hour Ambulatory Blood Pressure. Ann. Pharmacother. 2012, 46, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Elitok, A.; Oz, F.; Panc, C.; Sarikaya, R.; Sezikli, S.; Pala, Y.; Bugan, O.S.; Ates, M.; Parildar, H.; Ayaz, M.B.; et al. Acute effects of Red Bull energy drink on ventricular repolarization in healthy young volunteers: A prospective study. Anatol. J. Cardiol. 2015, 15, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Ragsdale, F.R.; Gronli, T.D.; Batool, N.; Haight, N.; Mehaffey, A.; McMahon, E.C.; Nalli, T.W.; Mannello, C.M.; Sell, C.J.; McCann, P.J.; et al. Effect of Red Bull energy drink on cardiovascular and renal function. Amino Acids 2010, 38, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Grasser, E.K.; Dulloo, A.G.; Montani, J.-P. Cardiovascular and Cerebrovascular Effects in Response to Red Bull Consumption Combined With Mental Stress. Am. J. Cardiol. 2015, 115, 183–189. [Google Scholar] [CrossRef]
- Doerner, J.M.; Kuetting, D.L.; Luetkens, J.A.; Naehle, C.P.; Dabir, D.; Homsi, R.; Nadal, J.; Schild, H.H.; Thomas, D.K. Caffeine and taurine containing energy drink increases left ventricular contractility in healthy volunteers. Int. J. Cardiovasc. Imaging 2015, 31, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Menci, D.; Righini, F.M.; Cameli, M.; Lisi, M.; Benincasa, S.; Focardi, M.; Mondillo, S. Acute Effects of an Energy Drink on Myocardial Function Assessed by Conventional Echo-Doppler Analysis and by Speckle Tracking Echocardiography on Young Healthy Subjects. J. Amino Acids 2013, 2013, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hajsadeghi, S.; Mohammadpour, F.; Manteghi, M.J.; Kordshakeri, K.; Tokazebani, M.; Rahmani, E.; Hassanzadeh, M. Effects of energy drinks on blood pressure, heart rate, and electrocardiographic parameters: An experimental study on healthy young adults. Anatol. J. Cardiol. 2015, 16, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.; Weiß, M. The influence of a taurine containing drink on cardiac parameters before and after exercise measured by echocardiography. Amino Acids 2001, 20, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.; Buchholtz, J. Über das Minutenvolum des Herzens beim Hunde und über den Einfluss des Coffeins auf die Grösse des Minutenvolums. Arch. Exp. Pathol. Pharmakol. 1920, 88, 192–215. [Google Scholar] [CrossRef]
- Basrai, M.; Schweinlin, A.; Menzel, J.; Mielke, H.; Weikert, C.; Dusemund, B.; Putze, K.; Watzl, B.; Lampen, A.; Bischoff, S.C. Energy Drinks Induce Acute Cardiovascular and Metabolic Changes Pointing to Potential Risks for Young Adults: A Randomized Controlled Trial. J. Nutr. 2019, 149, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Berglund, B.; Hemmingsson, P. Effects of Caffeine Ingestion on Exercise Performance at Low and High Altitudes in Cross-Country Skiers. Int. J. Sports Med. 1982, 3, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Fulco, C.S.; Rock, P.B.; Trad, L.A.; Rose, M.S.; Forte, V.A.; Young, P.M.; Cymerman, A. Effect of caffeine on submaximal exercise performance at altitude. Aviat. Space Environ. Med. 1994, 65, 539–545. [Google Scholar] [PubMed]
- Smirmaul, B.P.C.; de Moraes, A.C.; Angius, L.; Marcora, S.M. Effects of caffeine on neuromuscular fatigue and performance during high-intensity cycling exercise in moderate hypoxia. Eur. J. Appl. Physiol. 2017, 117, 27–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadheim, H.K.; Nossum, E.M.; Olsen, R.; Spencer, M.; Jensen, J. Caffeine improves performance in double poling during acute exposure to 2000-m altitude. J. Appl. Physiol. 2015, 119, 1501–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles-Chan, J.L.; Charrière, N.; Grasser, E.K.; Montani, J.-P.; Dulloo, A.G. The blood pressure-elevating effect of Red Bull energy drink is mimicked by caffeine but through different hemodynamic pathways. Physiol. Rep. 2015, 3, e12290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, P.D.; Naumann, P.F.; Laravuso, R.B. Simultaneous measurement of eight foreign gases in blood by gas chromatography. J. Appl. Physiol. 1974, 36, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.D.; Saltzman, H.A.; West, J.B. Measurement of continuous distributions of ventilation-perfusion ratios: Theory. J. Appl. Physiol. 1974, 36, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Farhi, L.E.; Olszowka, A.J. Analysis of alveolar gas exchange in the presence of soluble inert gases. Respir. Physiol. 1968, 5, 53–67. [Google Scholar] [CrossRef]
- Steinke, L.; Lanfear, D.E.; Dhanapal, V.; Kalus, J.S. Effect of “energy drink” consumption on hemodynamic and electrocardiographic parameters in healthy young adults. Ann. Pharmacother. 2009, 43, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Geiß, K.R.; Jester, I.; Falke, W.; Hamm, M.; Waag, K.L. The effect of a taurine-containing drink on performance in 10 endurance-athletes. Amino Acids 1994, 7, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Bichler, A.; Swenson, A.; Harris, M.A. A combination of caffeine and taurine has no effect on short term memory but induces changes in heart rate and mean arterial blood pressure. Amino Acids 2006, 31, 471–476. [Google Scholar] [CrossRef]
- Robertson, D.; Wade, D.; Workman, R.; Woosley, R.L.; Oates, J.A. Tolerance to the humoral and hemodynamic effects of caffeine in man. J. Clin. Investig. 1981, 67, 1111–1117. [Google Scholar] [CrossRef] [Green Version]
- Siebenmann, C.; Lundby, C. Regulation of cardiac output in hypoxia. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. S4), 53–59. [Google Scholar] [CrossRef] [Green Version]
- Siebenmann, C.; Rasmussen, P.; Sørensen, H.; Bonne, T.C.; Zaar, M.; Aachmann-Andersen, N.J.; Nordsborg, N.B.; Secher, N.H.; Lundby, C. Hypoxia increases exercise heart rate despite combined inhibition of β-adrenergic and muscarinic receptors. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H1540–H1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cushney, A.R.J. On the pharmacology of the respiratory center. Pharmacol. Exper. Ther. 1913, 4, 363. [Google Scholar]
- Le Messurier, D.H. The site of action of caffeine as a respiratory stimulant. J. Pharmacol. Exp. Ther. 1936, 57, 458–463. [Google Scholar]
- Richmond, G.H. Action of caffeine and aminophylline as respiratory stimulants in man. J. Appl. Physiol. 1949, 2, 16–23. [Google Scholar] [CrossRef]
- Brown, D.D.; Knowlton, R.G.; Sullivan, J.J.; Sanjabi, P.B. Effect of caffeine ingestion on alveolar ventilation during moderate exercise. Aviat. Space Environ. Med. 1991, 62, 860–864. [Google Scholar] [PubMed]
- D’Urzo, A.D.; Jhirad, R.; Jenne, H.; Avendano, M.A.; Rubinstein, I.; D’Costa, M.; Goldstein, R.S.; Rubenstein, I. Effect of caffeine on ventilatory responses to hypercapnia, hypoxia, and exercise in humans. J. Appl. Physiol. 1990, 68, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Cavka, A.; Stupin, M.; Panduric, A.; Plazibat, A.; Cosic, A.; Rasic, L.; Debeljak, Z.; Martinovic, G.; Drenjancevic, I. Adrenergic System Activation Mediates Changes in Cardiovascular and Psychomotoric Reactions in Young Individuals after Red Bull (©) Energy Drink Consumption. Int. J. Endocrinol. 2015, 2015, 751530. [Google Scholar] [CrossRef] [PubMed]
- Ruíz-Moreno, C.; Lara, B.; Brito de Souza, D.; Gutiérrez-Hellín, J.; Romero-Moraleda, B.; Cuéllar-Rayo, Á.; Del Coso, J. Acute caffeine intake increases muscle oxygen saturation during a maximal incremental exercise test. Br. J. Clin. Pharmacol. 2020, 86, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Shearer, J.; Graham, T.E. Performance effects and metabolic consequences of caffeine and caffeinated energy drink consumption on glucose disposal. Nutr. Rev. 2014, 72 (Suppl. S1), 121–136. [Google Scholar] [CrossRef] [PubMed]
- Abebe, W.; Mozaffari, M.S. Role of taurine in the vasculature: An overview of experimental and human studies. Am. J. Cardiovasc. Dis. 2011, 1, 293–311. [Google Scholar] [PubMed]
- Ehlers, A.; Marakis, G.; Lampen, A.; Hirsch-Ernst, K.I. Risk assessment of energy drinks with focus on cardiovascular parameters and energy drink consumption in Europe. Food Chem. Toxicol. 2019, 130, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, P.; Feldman, J.; Bloch, R.; Schwartz, J. Central cardiovascular effects of taurine: Comparison with homotaurine and muscimol. J. Pharmacol. Exp. Ther. 1981, 219, 213–218. [Google Scholar] [PubMed]
- Azuma, J.; Sawamura, A.; Awata, N. Usefulness of Taurine in Chronic Congestive Heart Failure and Its Prospective Application. Jpn. Circ. J. 1992, 56, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Time Point | 0 min | 30 min | 90 min | 120 min | 150 min | 210 min | 240 min | |
|---|---|---|---|---|---|---|---|---|
| Normoxia (FiO2 = 0.21) | Hypoxia (FiO2 = 0.13) | |||||||
| MAP (torr) | RB | 87 ± 14 | 92 ± 12 | 97 ± 16 | 89 ± 12 | 86 ± 15 | 77 ± 9 | 82 ± 10 |
| control | 89 ± 9 | 101 ± 17 | 98 ± 6 | 94 ± 12 | 83 ± 8 | 83 ± 9 | 86 ± 16 | |
| mPAP (torr) | RB | 23 ± 3 | 24 ± 3 | 24 ± 2 | 24 ± 3 | 37 ± 4 | 40 ± 2 1 | 41 ± 3 1 |
| control | 23 ± 1 | 24 ± 2 | 24 ± 2 | 24 ± 2 | 38 ± 1 | 38 ± 5 | 39 ± 4 | |
| CO (l/min) | RB | 4.5 ± 0.7 | 4.3 ± 0.5 | 4.0 ± 1.0 | 4.2 ± 0.7 | 5.4 ± 0.6 2 | 4.8 ± 0.7 | 4.5 ± 1.1 |
| control | 4.5 ± 0.7 | 4.0 ± 0.6 | 4.0 ± 0.7 | 4.2 ± 1.2 | 4.3 ± 0.8 | 5.2 ± 1.3 | 4.6 ± 2.1 | |
| PCWP (torr) | RB | 13 ± 0 | 13 ± 1 | 12 ± 1 | 10 ± 2 | 9 ± 3 | 9 ± 3 | 10 ± 4 |
| control | 15 ± 2 | 15 ± 3 | 14 ± 2 | 12 ± 1 | 11 ± 1 | 10 ± 2 | 10 ± 2 | |
| CVD (torr) | RB | 9 ± 1 | 10 ± 2 | 10 ± 1 | 9 ± 3 | 9 ± 3 | 10 ± 1 | 10 ± 2 |
| Control | 10 ± 1 | 9 ± 1 | 9 ± 1 | 10 ± 1 | 11 ± 1 | 10 ± 2 | 10 ± 1 | |
| Time Point | 0 min | 30 min | 90 min | 120 min | 150 min | 210 min | 240 min | |
|---|---|---|---|---|---|---|---|---|
| Normoxia (FiO2 = 0.21) | Hypoxia (FiO2 = 0.13) | |||||||
| paO2 (torr) | RB | 98 ± 5 | 88 ± 4 | 88 ± 6 | 93 ± 4 | 35 ± 4 | 33 ± 2 | 33 ± 2 |
| control | 98 ± 6 | 90 ± 5 | 87 ± 3 | 93 ± 3 | 35 ± 5 | 33 ± 3 | 34 ± 4 | |
| paCO2 (torr) | RB | 37 ± 2 | 40 ± 3 1 | 39 ± 2 | 37 ± 1 | 38 ± 4 | 39 ± 5 | 39 ± 5 |
| control | 35 ± 2 | 35 ± 3 | 35 ± 3 | 36 ± 2 | 34 ± 5 | 36 ± 3 | 37 ± 3 | |
| pH | RB | 7.44 ± 0.03 | 7.40 ± 0.01 1 | 7.40 ± 0.02 | 7.43 ± 0.03 | 7.44 ± 0.04 | 7.33 ± 0.09 | 7.29 ± 0.10 |
| control | 7.46 ± 0.02 | 7.46 ± 0.03 | 7.43 ± 0.06 | 7.51 ± 0.02 | 7.48 ± 0.04 | 7.43 ± 0.04 | 7.39 ± 0.05 | |
| pvO2 (torr) | RB | 37 ± 2 | 35 ± 2 | 34 ± 2 | 34 ± 3 | 22 ± 1 | 17 ± 2 | 14 ± 2 1 |
| control | 36 ± 0 | 33 ± 2 | 33 ± 2 | 35 ± 3 | 22 ± 3 | 19 ± 2 | 21 ± 4 | |
| pvCO2 (torr) | RB | 41 ± 2 | 46 ± 3 1,2 | 46 ± 2 1,2 | 43 ± 2 | 43 ± 4 | 47 ± 6 3 | 48 ± 6 3 |
| control | 41 ± 3 | 40 ± 5 | 41 ± 4 | 41 ± 4 | 39 ± 4 | 40 ± 3 | 42 ± 3 | |
| Time Point | 0 min | 30 min | 90 min | 120 min | 150 min | 240 min | |
|---|---|---|---|---|---|---|---|
| Normoxia (FiO2 = 0.21) | Hypoxia (FiO2 = 0.13) | ||||||
| Low VA/Q of Q (%) | RB | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| control | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 1.2 ± 1.8 | 0.7 ± 1.1 | |
| Norm VA/Q of Q (%) | RB | 96.8 ± 2.2 | 95.0 ± 2.5 | 97.3 ± 1.5 | 98.0 ± 2.5 | 98.1 ± 0.9 | 93.3 ± 2.2 |
| control | 99.1 ± 1.4 | 99.2 ± 1.9 | 98.8 ± 1.5 | 97.8 ± 1.7 | 96.7 ± 1.7 | 97.0 ± 1.7 | |
| High VA/Q of Q (%) | RB | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0.5 ± 0.9 |
| control | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | |
| Mean of Q | RB | 0.62 ± 0.18 | 0.60 ± 0.16 | 0.62 ± 0.11 | 0.73 ± 0.26 | 0.75 ± 0.32 | 1.26 ± 0.54 |
| control | 0.86 ± 0.19 | 0.88 ± 0.31 | 0.86 ± 0.20 | 0.63 ± 0.14 | 0.59 ± 0.21 | 0.67 ± 0.29 | |
| LogSDQ | RB | 0.39 ± 0.08 | 0.45 ± 0.16 | 0.43 ± 0.06 | 0.36 ± 0.05 | 0.43 ± 0.15 | 0.68 ± 0.27 |
| control | 0.45 ± 0.14 | 0.52 ± 0.12 | 0.47 ± 0.12 | 0.63 ± 0.20 | 0.57 ± 0.13 | 0.54 ± 0.06 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Treml, B.; Schöpf, E.; Geiger, R.; Niederwanger, C.; Löckinger, A.; Kleinsasser, A.; Bachler, M. Red Bull Increases Heart Rate at Near Sea Level and Pulmonary Shunt Fraction at High Altitude in a Porcine Model. Nutrients 2020, 12, 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061738
Treml B, Schöpf E, Geiger R, Niederwanger C, Löckinger A, Kleinsasser A, Bachler M. Red Bull Increases Heart Rate at Near Sea Level and Pulmonary Shunt Fraction at High Altitude in a Porcine Model. Nutrients. 2020; 12(6):1738. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061738
Chicago/Turabian StyleTreml, Benedikt, Elisabeth Schöpf, Ralf Geiger, Christian Niederwanger, Alexander Löckinger, Axel Kleinsasser, and Mirjam Bachler. 2020. "Red Bull Increases Heart Rate at Near Sea Level and Pulmonary Shunt Fraction at High Altitude in a Porcine Model" Nutrients 12, no. 6: 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061738