Early Nutrition eAcademy Southeast Asia e-Learning for Enhancing Knowledge on Nutrition during the First 1000 Days of Life

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Early Nutrition eAcademy Southeast Asia Project (ENeA SEA)
2.2. Assessment of HCPs’ Needs and CME/CPD Landscape in SEA
- Identifying specific topics and their prioritisation to develop a targeted ENeA SEA curriculum and e-learning modules
- Creating appropriate, effective educational and technical formats optimally matching the needs of target groups
- Ensuring that the content was of high practical relevance and could be directly translated into clinical practice and counselling, and into CME/CPD programmes, complementing existing training activities.
2.3. Desktop Research
2.4. Online Surveys
2.5. Development of ENeA SEA e-Learning Platform, Curriculum and e-Modules and its Evaluation
2.6. Interdisciplinary, International Process of co-Creation and Capacity Building
2.7. Descriptive and Explorative Evaluation of e-Learning Platform and Modules
3. Results
3.1. Questionnaire 1: Online Survey with Closed Questions to HCPs
3.2. Questionnaire 2: Online Survey with Open Questions to HCPs
3.3. Questionnaire 3: Mixed Online Survey to Stakeholders in the CME/CPD Sector
3.4. Review of the CME/CPD System in Thailand and Malaysia and in the SEA Region
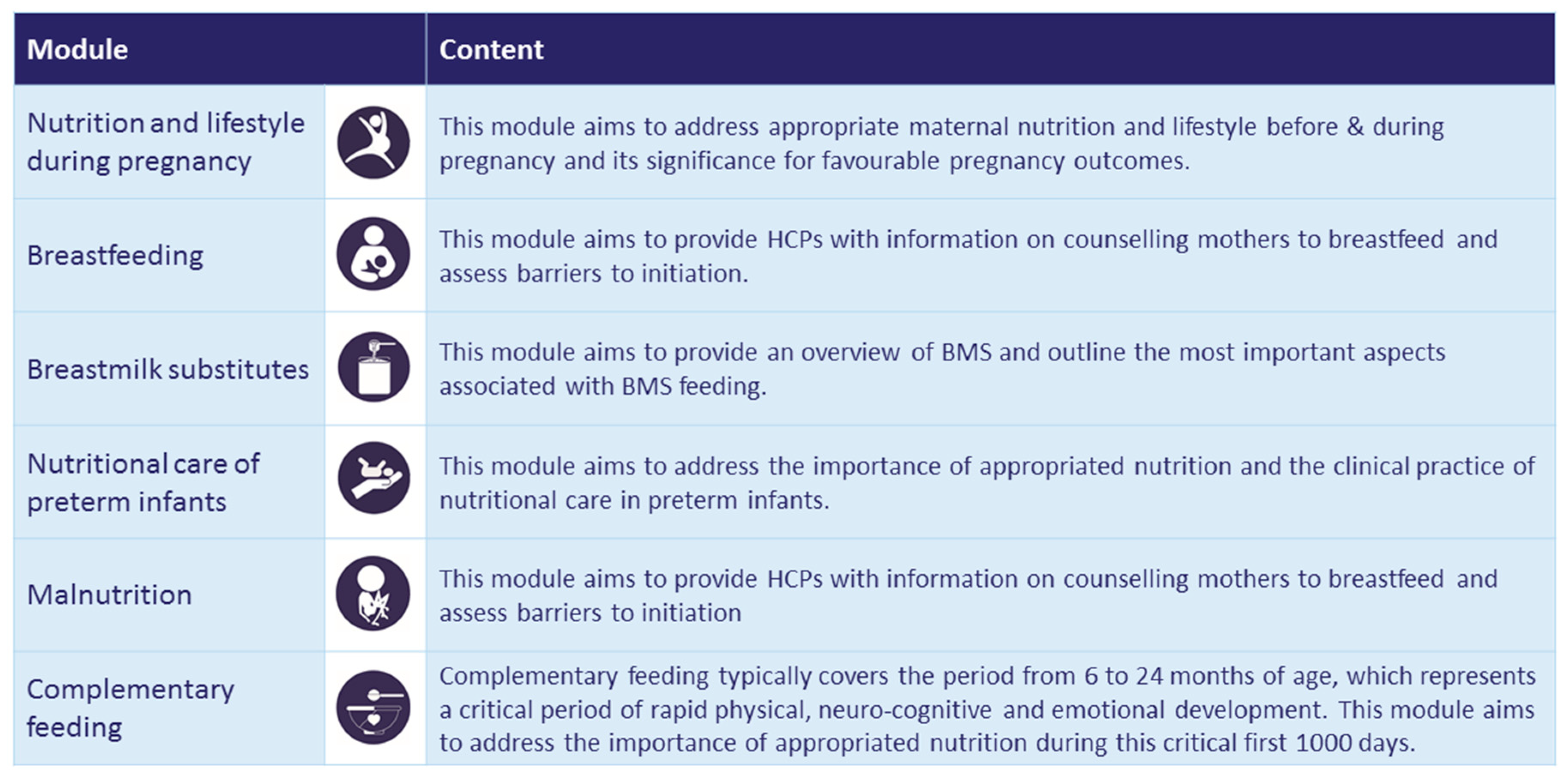
3.5. Development of the ENeA SEA e-Learning Platform, Curriculum and Modules and Its Evaluation
Descriptive and Explorative Evaluation in Users
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
|
|
|
|
|
|
|
|
|
|
| Question 1: | The module content was arranged in a clear and logical manner. |
| Question 2: | The interface was easy to use. |
| Question 3: | The module content was consistent with objectives. |
| Question 4: | This module met my needs in the field of early nutrition. |
| Question 5: | My confidence in counselling patients on > topic of module < has increased as a result of this module. |
| Question 6: | Using this module will lead to changing my perspectives and/or practice. |
| Question 7: | Based on this experience, I would take another e-learning module. |
| Question 8: | I would recommend this learning activity to others. |
| Question 9: | The content was relevant to South East Asia. |
| Question 10: | This e-learning platform has improved my knowledge in the field of early nutrition. |
| Question 11: | This course has helped me to inform or train other HCPs. |
References
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2019: Safeguarding against Economic Slowdowns and Downturns; FAO: Rome, Italy, 2019. [Google Scholar]
- Development Initiatives Poverty Research. 2020 Global Nutrition Report: Action on Equity to End Malnutrition; Development Initiatives Poverty Research Ltd.: Bristol, UK, 2020. [Google Scholar]
- Winichagoon, P. Thailand nutrition in transition: Situation and challenges of maternal and child nutrition. Asia Pac. J. Clin. Nutr. 2013, 22, 6–15. [Google Scholar] [PubMed]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision (ST/ESA/SER.A/420); United Nations: New York, NY, USA, 2019. [Google Scholar]
- Deloitte. 2015 Health Care Outlook Southest Asia; Southeast Asia, Deloitte Touche Tohmatsu Limited: Singapore, 2015. [Google Scholar]
- Koletzko, B.; Brands, B.; Grote, V.; Kirchberg, F.F.; Prell, C.; Rzehak, P.; Early Nutrition Programming Project. Long-Term Health Impact of Early Nutrition: The Power of Programming. Ann. Nutr. Metab. 2017, 70, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Godfrey, K.M.; Poston, L.; Szajewska, H.; Van Goudoever, J.B.; De Waard, M.; Patro-Golab, B. Nutrition during Pregnancy, Lactation and Early Childhood and its Implications for Maternal and Long-Term Child Health: The Early Nutrition Project Recommendations. Ann. Nutr. Metab. 2019, 74, 93–106. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for South East Asia. Regional Guidelines for Continuing Medical Education (CME)/Continuing Professional Development (CPD) Activities; WHO Regional Office for South East Asia: New Delhi, India, 2010. [Google Scholar]
- Gutu-Robu, G.; Dascalu, M.; Carabas, M.; Elisei, A.; Trausan-Matu, S.; Nistor, N.; Sunhea, C.; Rebecca, S.; Koletzko, B. Curricula Customization with the ReaderBench Framework. In Proceedings of the 14th International Scientific Conference eLearning and Software for Education, Bucharest, Romania, 19–20 April 2018. [Google Scholar]
- Gabriel Gutu-Robu, D.M.; Carabas, M.; Dascalu, M.; Trausan-Matu, S.; Choi, S.; Godfrey, K.M.; Brands, B.A.; Koletzko, B. On behalf of the Early Nutrition eAcademy South East Asia Consortium. Cust. Curric. Manag. Moodle Integr. Semant. Recomm. 2020, in press. [Google Scholar]
- Nistor, N.; Dascălu, M.; Guțu, G.; Trăușan-Matu, Ș.; Choi, S.; Haberman-Lawson, A.; Brands, A.; Körner, C.; Koletzko, B. Mass Customization in Continuing Medical Education: Automated Extraction of E-Learning Topics; Springer: Cham, Switzerland, 2017; pp. 576–579. [Google Scholar]


| Question | Responses |
|---|---|
| Q1: Please rank the following topics on a scale of 1–5 (1 being most important and 5 being least important; each ranking number from 1–5 can only be used once) in which doctors in practice and other health care professionals (HCP) require continual medical education? | The topics “nutrition and lifestyle during pregnancy” (n = 61/142) and “breastfeeding” (n = 43/142), and nutritional care of preterm infants (n = 23/142) were reported as the most required topic areas (rated with 1) for HCPs to receive continuing medical education (CME). |
| Q2: In your opinion, do doctors in practice and other HCPs use the internet for professional purposes?”“In your opinion, are doctors in practice and other HCPs proficient enough in English to study an online course?” | 85–91% of HCPs reported using the internet for professional purposes. Doctors more often stated to be proficient in English to study online (89%) than other HCPs (63%). |
| Q3: How are the doctors in practice and other HCPs continually trained and educated in their area of study? | Most of the existing training for doctors (83%) and HCPs (85%) was at face-to-face events; e-learning was reported by slightly more doctors (41%) than other HCPs (35%). |
| Q4: Out of the following, which formats are preferred for training for doctors in practice and other HCPs? | Face to face events were the preferred mode of training for both doctors (72%) and other HCPs (76%). 57% of doctors and other HCPs preferred e-courses for their training. |
| Q5: Out of the following, which modes are preferred for e-learning for doctors in practice and other HCPs? | Availability on a smartphone, laptop or mobile phone were the preferred modes of e-learning, with fewer preferring a computer. |
| Q6: Are doctors in practice and other HCPs evaluated on a continuing medical education/professional development (CME/CPD) credit system in your country? | 81–85% of both doctors and other HCPs reported that they were evaluated on a CME/CPD system. |
| Q7: On a scale of 1–5, how important are CME/CPD credits for you (1 being highly important and 5 being least important)? | 37% of the doctors and other HCPs rated the importance of CME/CPD credits as very high; 21% rated the importance as high. |
| Q8: On what basis are doctors in practice and other HCPs evaluated?” | A credit point-based system was slightly more relevant to HCPs (73%) than doctors (64%). |
| Q9: What types of CME/CPD certificates are recognised in your country? | 97% of doctors and 96% of other HCPs reported that national/local certificates were recognised. 11% of doctors and 7% of other HCPs stated that European (UEMS) and US American (AMA) CME credits were recognised in their countries. |
| Question | Responses |
|---|---|
| Q1: What knowledge, skills and competencies should the specialised doctors/health care professionals have in your country? | 54% of the responses related to nutrition and lifestyle, with 90% stating that it could be further clustered into the themes pregnancy, infant formula feeding, breastfeeding and complementary feeding. |
| Q2: What knowledge, skills and competencies are currently lacking in the specialised doctors/health care professionals according to your opinion? | 85% of the responses related to nutrition and lifestyle, with 90% stating it that could be further clustered into the themes pregnancy, preterm infants, infant formula feeding, and breastfeeding. |
| Q3: Training in early nutrition content: what contents should be included in the specialisation and CME/CPD programs? | 20% of the topics identified related to complementary feeding, 19% to infant formula feeding, 18% to breastfeeding, 15% to preterm infant nutrition and 11% to critical nutrients. |
| Q4: Is nutrition related content included in specialisation training for doctors/health care professionals? If yes, what percentage is dedicated to nutrition? | 10 out of 11 participants responded affirmatively. Nutrition content ranged from 5–10%. |
| Module | Nutrition and Lifestyle in Pregnancy | Breastfeeding | Breastmilk Substitutes | Complementary Feeding | Nutritional Care of Preterm Infants | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total of enrolled users | 421 | 636 | 266 | 293 | 216 | ||||||||||||||
| Users attempted CME test (n) | 46 | 378 | 140 | 184 | 116 | ||||||||||||||
| Users successfully passing CME test (n) | 38 | 262 | 95 | 150 | 93 | ||||||||||||||
| Passing rate 1 (%) | 83% | 69% | 68% | 82% | 80% | ||||||||||||||
| Unit | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 |
| Enrolled users in each unit (n) | 306 | 160 | 132 | 103 | 91 | 577 | 430 | 412 | 210 | 150 | 157 | 153 | 248 | 223 | 209 | 241 | 185 | 154 | 152 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brands, B.; Chomtho, S.; Suthutvoravut, U.; Chiong Meng Boey, C.; Tang, S.F.; Godfrey, K.M.; Koletzko, B.; for the ENeA SEA Project Group. Early Nutrition eAcademy Southeast Asia e-Learning for Enhancing Knowledge on Nutrition during the First 1000 Days of Life. Nutrients 2020, 12, 1817. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061817
Brands B, Chomtho S, Suthutvoravut U, Chiong Meng Boey C, Tang SF, Godfrey KM, Koletzko B, for the ENeA SEA Project Group. Early Nutrition eAcademy Southeast Asia e-Learning for Enhancing Knowledge on Nutrition during the First 1000 Days of Life. Nutrients. 2020; 12(6):1817. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061817
Chicago/Turabian StyleBrands, Brigitte, Sirinuch Chomtho, Umaporn Suthutvoravut, Christopher Chiong Meng Boey, Swee Fong Tang, Keith M. Godfrey, Berthold Koletzko, and for the ENeA SEA Project Group. 2020. "Early Nutrition eAcademy Southeast Asia e-Learning for Enhancing Knowledge on Nutrition during the First 1000 Days of Life" Nutrients 12, no. 6: 1817. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061817