Postprandial Endotoxin Transporters LBP and sCD14 Differ in Obese vs. Overweight and Normal Weight Men during Fat-Rich Meal Digestion

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Trials and Subjects
2.2. Plasma sCD14 and LBP
2.3. Plasma Analyses
2.4. Anthropometry and Body Composition
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
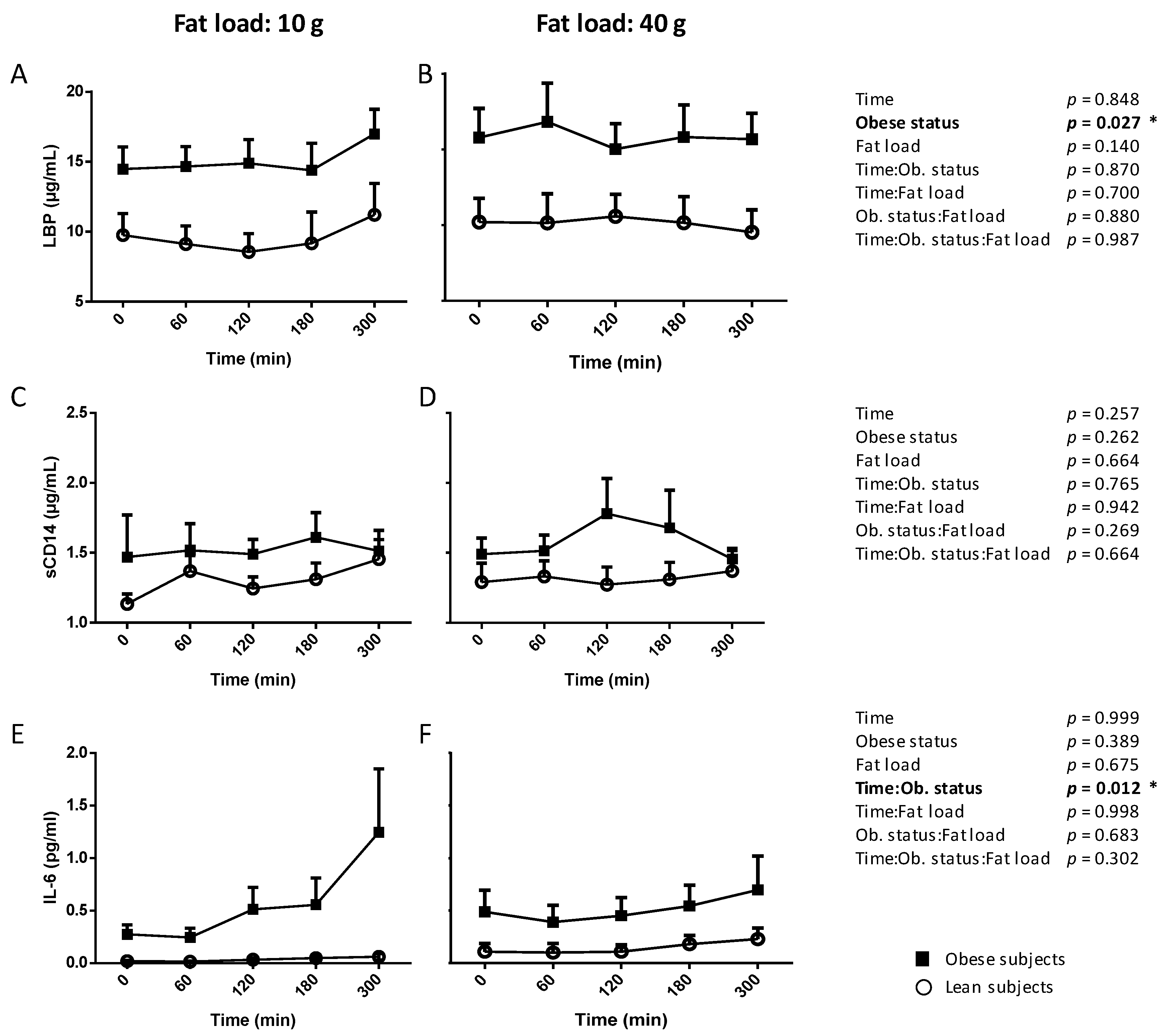
3.2. Postprandial Kinetics of LBP, sCD14 and IL-6 in Normal Weight and Obese Subjects (Lipinflox Study)
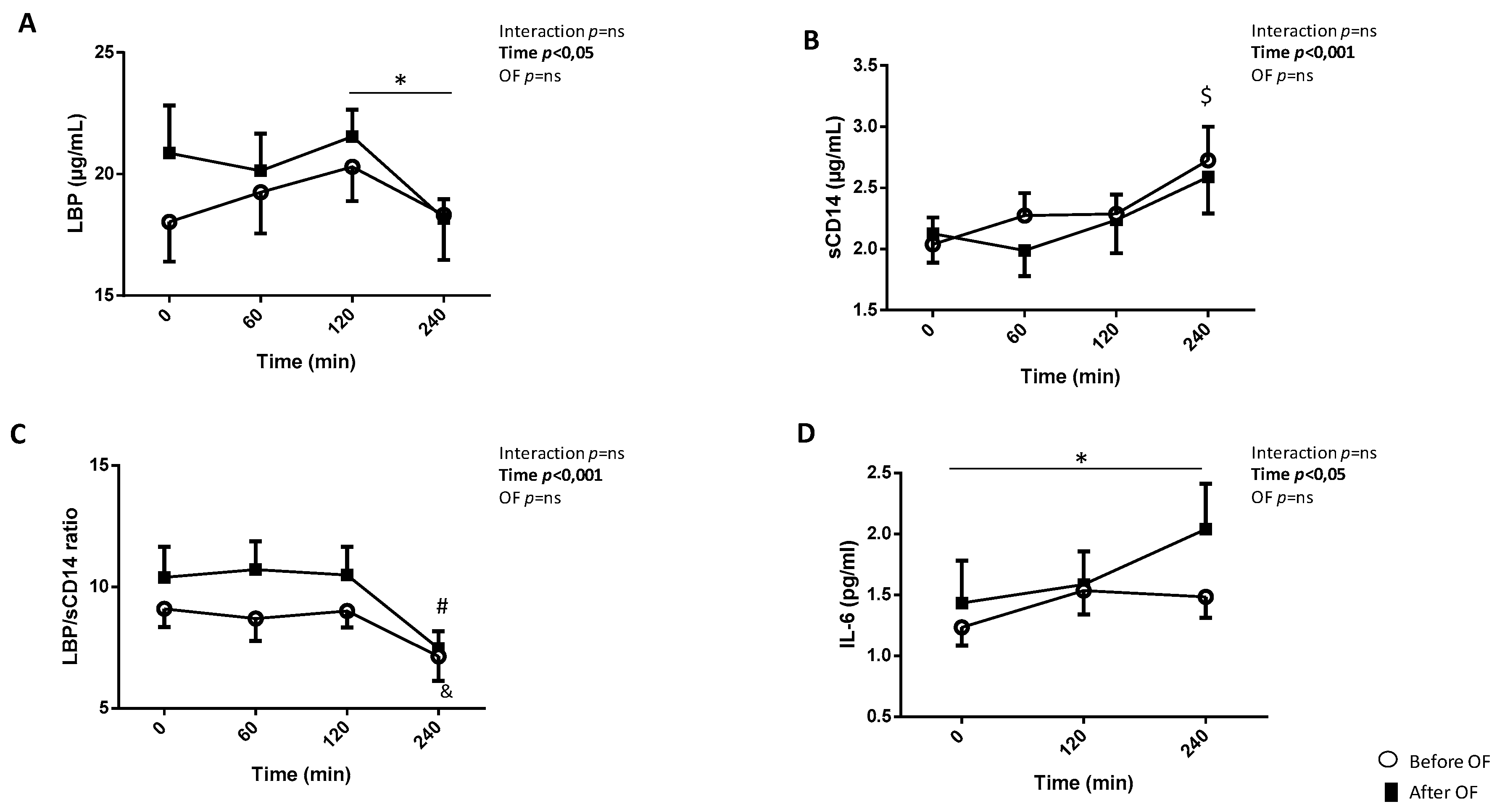
3.3. Postprandial Kinetics of LBP, sCD14 and IL-6 Before and After Overfeeding
3.4. Associations between Fasting and Postprandial LBP and Selected Parameters of Dietary Trials and Intervention
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
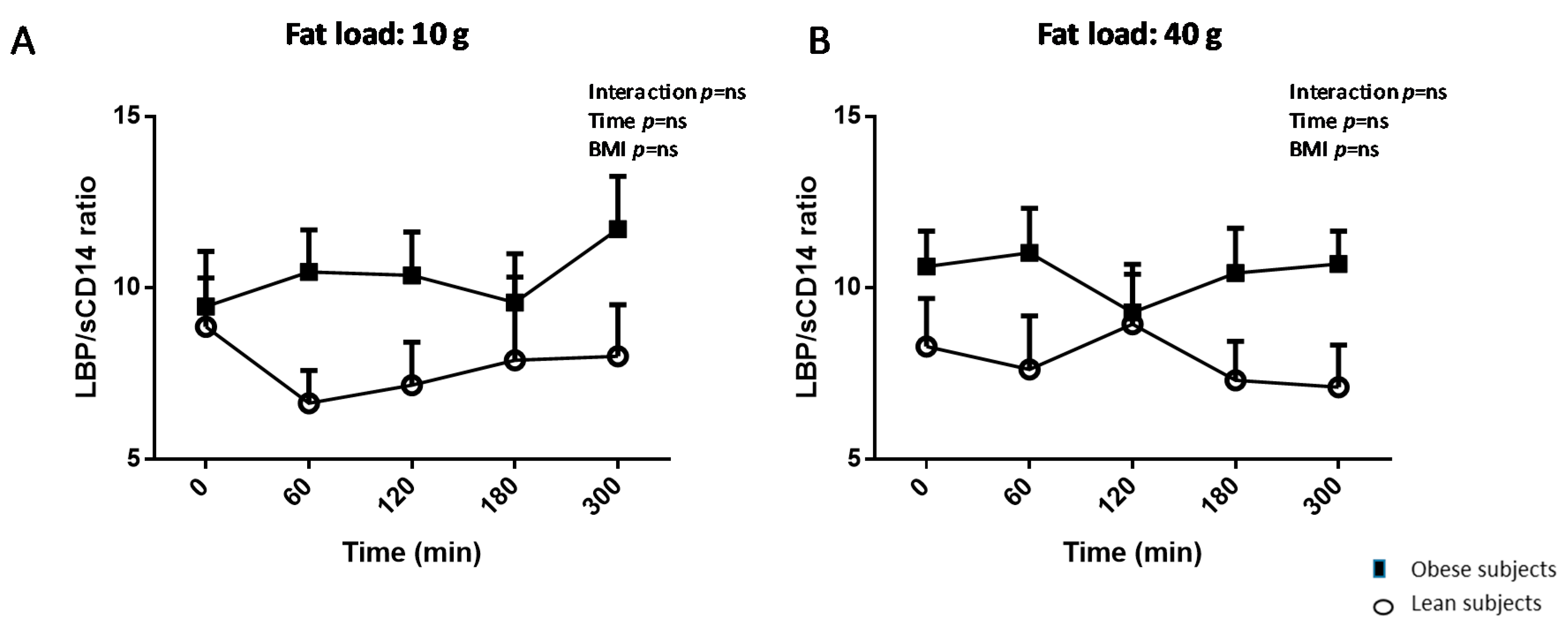
Appendix A. Postprandial Kinetics of LBP/sCD14 after 10 g vs. 40 g Fat Load. Data Are Means ± SEM

References
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Erridge, C.; Attina, T.; Spickett, C.M.; Webb, D.J. A high-fat meal induces low-grade endotoxemia: Evidence of a novel mechanism of postprandial inflammation. Am. J. Clin. Nutr. 2007, 86, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, S.; Witta, J.; Zhong, J.; de Villiers, W.; Eckhardt, E. Chylomicrons promote intestinal absorption of lipopolysaccharides. J. Lipid Res. 2009, 50, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laugerette, F.; Vors, C.; Geloen, A.; Chauvin, M.A.; Soulage, C.; Lambert-Porcheron, S.; Peretti, N.; Alligier, M.; Burcelin, R.; Laville, M.; et al. Emulsified lipids increase endotoxemia: Possible role in early postprandial low-grade inflammation. J. Nutr. Biochem. 2011, 22, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herieka, M.; Erridge, C. High-fat meal induced postprandial inflammation. Mol. Nutr. Food Res. 2014, 58, 136–146. [Google Scholar] [CrossRef]
- Clemente-Postigo, M.; Queipo-Ortuno, M.I.; Murri, M.; Boto-Ordonez, M.; Perez-Martinez, P.; Andres-Lacueva, C.; Cardona, F.; Tinahones, F.J. Endotoxin increase after fat overload is related to postprandial hypertriglyceridemia in morbidly obese patients. J. Lipid Res. 2012, 53, 973–978. [Google Scholar] [CrossRef] [Green Version]
- Hailman, E.; Lichenstein, H.S.; Wurfel, M.M.; Miller, D.S.; Johnson, D.A.; Kelley, M.; Busse, L.A.; Zukowski, M.M.; Wright, S.D. Lipopolysaccharide (LPS)-binding protein accelerates the binding of LPS to CD14. J. Exp. Med. 1994, 179, 269–277. [Google Scholar] [CrossRef]
- Stoll, L.L.; Denning, G.M.; Weintraub, N.L. Potential role of endotoxin as a proinflammatory mediator of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 2227–2236. [Google Scholar] [CrossRef]
- Sun, L.; Yu, Z.; Ye, X.; Zou, S.; Li, H.; Yu, D.; Wu, H.; Chen, Y.; Dore, J.; Clement, K.; et al. A marker of endotoxemia is associated with obesity and related metabolic disorders in apparently healthy Chinese. Diabetes Care 2010, 33, 1925–1932. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Quintela, A.; Alonso, M.; Campos, J.; Vizcaino, L.; Loidi, L.; Gude, F. Determinants of serum concentrations of lipopolysaccharide-binding protein (LBP) in the adult population: The role of obesity. PLoS ONE 2013, 8, e54600. [Google Scholar] [CrossRef]
- Lepper, P.M.; Schumann, C.; Triantafilou, K.; Rasche, F.M.; Schuster, T.; Frank, H.; Schneider, E.M.; Triantafilou, M.; von Eynatten, M. Association of lipopolysaccharide-binding protein and coronary artery disease in men. J. Am. Coll. Cardiol. 2007, 50, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Navarrete, J.M.; Escote, X.; Ortega, F.; Camps, M.; Ricart, W.; Zorzano, A.; Vendrell, J.; Vidal-Puig, A.; Fernandez-Real, J.M. Lipopolysaccharide binding protein is an adipokine involved in the resilience of the mouse adipocyte to inflammation. Diabetologia 2015, 58, 2424–2434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakatos, P.L.; Kiss, L.S.; Palatka, K.; Altorjay, I.; Antal-Szalmas, P.; Palyu, E.; Udvardy, M.; Molnar, T.; Farkas, K.; Veres, G.; et al. Serum lipopolysaccharide-binding protein and soluble CD14 are markers of disease activity in patients with Crohn’s disease. Inflam. Bowel Dis. 2011, 17, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Laugerette, F.; Alligier, M.; Bastard, J.P.; Drai, J.; Chanseaume, E.; Lambert-Porcheron, S.; Laville, M.; Morio, B.; Vidal, H.; Michalski, M.C. Overfeeding increases postprandial endotoxemia in men: Inflammatory outcome may depend on LPS transporters LBP and sCD14. Mol. Nutr. Food Res. 2014, 58, 1513–1518. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, A.G.; Casafont, F.; Crespo, J.; Cayon, A.; Mayorga, M.; Estebanez, A.; Fernadez-Escalante, J.C.; Pons-Romero, F. Lipopolysaccharide-binding protein plasma levels and liver TNF-alpha gene expression in obese patients: Evidence for the potential role of endotoxin in the pathogenesis of non-alcoholic steatohepatitis. Obes. Surg. 2007, 17, 1374–1380. [Google Scholar] [CrossRef]
- Naghizadeh, M.; Baradaran, B.; Saghafi-Asl, M.; Amiri, P.; Shanehbandi, D.; Karamzad, N.; Mohamed-Khosroshahi, L. Toll-like receptor signaling and serum levels of interferon beta and lipopolysaccharide binding protein are related to abdominal obesity: A case-control study between metabolically healthy and metabolically unhealthy obese individuals. Nutr. Res. 2018, 55, 11–20. [Google Scholar] [CrossRef]
- Laugerette, F.; Furet, J.P.; Debard, C.; Daira, P.; Loizon, E.; Geloen, A.; Soulage, C.O.; Simonet, C.; Lefils-Lacourtablaise, J.; Bernoud-Hubac, N.; et al. Oil composition of high-fat diet affects metabolic inflammation differently in connection with endotoxin receptors in mice. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E374–E386. [Google Scholar] [CrossRef] [Green Version]
- Sakura, T.; Morioka, T.; Shioi, A.; Kakutani, Y.; Miki, Y.; Yamazaki, Y.; Motoyama, K.; Mori, K.; Fukumoto, S.; Shoji, T.; et al. Lipopolysaccharide-binding protein is associated with arterial stiffness in patients with type 2 diabetes: A cross-sectional study. Cardiovasc. Diabetol. 2017, 16, 62. [Google Scholar] [CrossRef]
- Serrano, M.; Moreno-Navarrete, J.M.; Puig, J.; Moreno, M.; Guerra, E.; Ortega, F.; Xifra, G.; Ricart, W.; Fernandez-Real, J.M. Serum lipopolysaccharide-binding protein as a marker of atherosclerosis. Atherosclerosis 2013, 230, 223–227. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Peris, E.; Wang, Y.; Tamae Kakazu, M.; Khalyfa, A.; Carreras, A.; Gozal, D. Lipopolysaccharide-binding protein plasma levels in children: Effects of obstructive sleep apnea and obesity. J. Clin. Endocrinol. Metab. 2014, 99, 656–663. [Google Scholar] [CrossRef] [Green Version]
- Kong, Y.; Li, Z.; Tang, T.; Wu, H.; Liu, J.; Gu, L.; Zhao, T.; Huang, Q. The level of lipopolysaccharide-binding protein is elevated in adult patients with obstructive sleep apnea. BMC Pulm. Med. 2018, 18, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Buhr, M.F.; Hedrich, H.J.; Westendorf, A.M.; Obermeier, F.; Hofmann, C.; Zschemisch, N.H.; Buer, J.; Bumann, D.; Goyert, S.M.; Bleich, A. Analysis of Cd14 as a genetic modifier of experimental inflammatory bowel disease (IBD) in mice. Inflam. Bowel Dis. 2009, 15, 1824–1836. [Google Scholar] [CrossRef] [PubMed]
- Vors, C.; Pineau, G.; Drai, J.; Meugnier, E.; Pesenti, S.; Laville, M.; Laugerette, F.; Malpuech-Brugere, C.; Vidal, H.; Michalski, M.C. Postprandial Endotoxemia Linked With Chylomicrons and Lipopolysaccharides Handling in Obese Versus Lean Men: A Lipid Dose-Effect Trial. J. Clin. Endocrinol. Metab. 2015, 100, 3427–3435. [Google Scholar] [CrossRef] [PubMed]
- Pei, R.; DiMarco, D.M.; Putt, K.K.; Martin, D.A.; Chitchumroonchokchai, C.; Bruno, R.S.; Bolling, B.W. Premeal Low-Fat Yogurt Consumption Reduces Postprandial Inflammation and Markers of Endotoxin Exposure in Healthy Premenopausal Women in a Randomized Controlled Trial. J. Nutr. 2018, 148, 910–916. [Google Scholar] [CrossRef]
- Alligier, M.; Meugnier, E.; Debard, C.; Lambert-Porcheron, S.; Chanseaume, E.; Sothier, M.; Loizon, E.; Hssain, A.A.; Brozek, J.; Scoazec, J.Y.; et al. Subcutaneous adipose tissue remodeling during the initial phase of weight gain induced by overfeeding in humans. J. Clin. Endocrinol. Metab. 2012, 97, E183–E192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vors, C.; Drai, J.; Gabert, L.; Pineau, G.; Laville, M.; Vidal, H.; Guichard, E.; Michalski, M.C.; Feron, G. Salivary composition in obese vs normal-weight subjects: Towards a role in postprandial lipid metabolism? Int. J. Obes. (Lond.) 2015, 39, 1425–1428. [Google Scholar] [CrossRef] [PubMed]
- Alligier, M.; Gabert, L.; Meugnier, E.; Lambert-Porcheron, S.; Chanseaume, E.; Pilleul, F.; Debard, C.; Sauvinet, V.; Morio, B.; Vidal-Puig, A.; et al. Visceral fat accumulation during lipid overfeeding is related to subcutaneous adipose tissue characteristics in healthy men. J. Clin. Endocrinol. Metab. 2013, 98, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amar, J.; Burcelin, R.; Ruidavets, J.B.; Cani, P.D.; Fauvel, J.; Alessi, M.C.; Chamontin, B.; Ferrieres, J. Energy intake is associated with endotoxemia in apparently healthy men. Am. J. Clin. Nutr. 2008, 87, 1219–1223. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, G.; Liu, J.; Gao, L.R.; Liu, M.; Wang, C.J.; Chuai, M.; Bao, Y.; Li, G.; Li, R.M.; et al. Gut microbiota-derived endotoxin enhanced the incidence of cardia bifida during cardiogenesis. J. Cell. Physiol. 2018, 233, 9271–9283. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Real, J.M.; Perez del Pulgar, S.; Luche, E.; Moreno-Navarrete, J.M.; Waget, A.; Serino, M.; Sorianello, E.; Sanchez-Pla, A.; Pontaque, F.C.; Vendrell, J.; et al. CD14 modulates inflammation-driven insulin resistance. Diabetes 2011, 60, 2179–2186. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Salinas, C.A.; Garcia, E.G.; Robles, L.; Riano, D.; Ruiz-Gomez, D.G.; Garcia-Ulloa, A.C.; Melgarejo, M.A.; Zamora, M.; Guillen-Pineda, L.E.; Mehta, R.; et al. High adiponectin concentrations are associated with the metabolically healthy obese phenotype. J. Clin. Endocrinol. Metab. 2008, 93, 4075–4079. [Google Scholar] [CrossRef]
- Yang, P.J.; Lee, W.J.; Tseng, P.H.; Lee, P.H.; Lin, M.T.; Yang, W.S. Bariatric surgery decreased the serum level of an endotoxin-associated marker: Lipopolysaccharide-binding protein. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2014, 10, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Lepper, P.M.; Kleber, M.E.; Grammer, T.B.; Hoffmann, K.; Dietz, S.; Winkelmann, B.R.; Boehm, B.O.; Marz, W. Lipopolysaccharide-binding protein (LBP) is associated with total and cardiovascular mortality in individuals with or without stable coronary artery disease—Results from the Ludwigshafen Risk and Cardiovascular Health Study (LURIC). Atherosclerosis 2011, 219, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.S.; Chang, Y.K.; Wu, T.K. Serum Lipopolysaccharide-Binding Protein is Associated with Chronic Inflammation and Metabolic Syndrome in Hemodialysis Patients. Blood Purif. 2019, 47, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Nien, H.C.; Hsu, S.J.; Su, T.H.; Yang, P.J.; Sheu, J.C.; Wang, J.T.; Chow, L.P.; Chen, C.L.; Kao, J.H.; Yang, W.S. High Serum Lipopolysaccharide-Binding Protein Level in Chronic Hepatitis C Viral Infection Is Reduced by Anti-Viral Treatments. PLoS ONE 2017, 12, e0170028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, N.; Sanada, Y.; Urahashi, T.; Ihara, Y.; Yamada, N.; Hirata, Y.; Katano, T.; Otomo, S.; Ushijima, K.; Mizuta, K. Endotoxin Metabolism Reflects Hepatic Functional Reserve in End-Stage Liver Disease. Transplant. Proc. 2018, 50, 1360–1364. [Google Scholar] [CrossRef]
- Umoh, F.I.; Kato, I.; Ren, J.; Wachowiak, P.L.; Ruffin, M.T.; Turgeon, D.K.; Sen, A.; Brenner, D.E.; Djuric, Z. Markers of systemic exposures to products of intestinal bacteria in a dietary intervention study. Eur. J. Nutr. 2016, 55, 793–798. [Google Scholar] [CrossRef]
- Chen, M.; Liu, B.; Thompson, C.H.; Wittert, G.A.; Heilbronn, L.K. Acute Overfeeding Does Not Alter Liver or Adipose Tissue-Derived Cytokines in Healthy Humans. Ann. Nutr. Metab. 2016, 69, 165–170. [Google Scholar] [CrossRef]
- Tam, C.S.; Viardot, A.; Clement, K.; Tordjman, J.; Tonks, K.; Greenfield, J.R.; Campbell, L.V.; Samocha-Bonet, D.; Heilbronn, L.K. Short-term overfeeding may induce peripheral insulin resistance without altering subcutaneous adipose tissue macrophages in humans. Diabetes 2010, 59, 2164–2170. [Google Scholar] [CrossRef] [Green Version]
- Dixon, N.C.; Hurst, T.L.; Talbot, D.C.; Tyrrell, R.M.; Thompson, D. Active middle-aged men have lower fasting inflammatory markers but the postprandial inflammatory response is minimal and unaffected by physical activity status. J. Appl. Physiol. 2009, 107, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Thompson, D.; Dixon, N. Measurement of postprandial interleukin-6 via a catheter: What does it tell us? Eur. J. Appl. Physiol. 2009, 107, 621–622. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Overfeeding Clinical Trial | Lipinflox Clinical Trial | |||||
|---|---|---|---|---|---|---|
| Before OF | After OF | p Value | Normal Weight | Obese | p Value | |
| Age (year) | 26 ± 2 | 29 ± 1 | 31 ± 2 | 0.426 | ||
| Body weight (kg) | 78.9 ± 4.9 | 81.7 ± 4.9 | 0.005 ** | 72.5 ± 2.1 | 101.1 ± 2.1 | 0.001 ** |
| BMI (kg/m2) | 24.9 ± 1.5 | 25.7 ± 1.4 | 0.004 ** | 22.4 ± 0.5 | 31.8 ± 0.3 | 0.001 ** |
| Waist circumference (cm) | 84.9 ± 3.3 | 86.9 ± 3.3 | 0.038 * | 83.6 ± 1.7 | 105 ± 0.8 | 0.001 ** |
| hsCRP (µg/mL) | 0.6 ± 0.1 | 1.1 ± 0.5 | 0.38 | 1.96 ± 0.01 | 2.98 ± 0.47 | 0.036 * |
| IL-6 (pg/mL) | 1.23 ± 0.15 | 1.43 ± 0.35 | 0.53 | 0.18 ± 0.04 | 0.45 ± 0.16 | 0.006 * |
| LPS (EU/mL) | 0.11 ± 0.03 | 0.16 ± 0.10 | 0.59 | 0.19 ± 0.05 | 0.18 ± 0.04 | 0.729 |
| Lean mass (kg) | 57,3 ± 2.5 | 58.2 ± 2.60 | 0.032 * | - | - | |
| Fat mass (kg) | 15.8 ± 2.9 | 17.1 ±3.1 | 0.048 * | - | - | |
| Visceral fat (kg) | 66.0 ± 18.1 | 73.5 ± 16.5 | 0.469 | - | - | |
| All (n = 16) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Postprandial Time | 0 min | 60 min | 120 min | 180 min | 300 min | |||||
| r | p | r | p | r | p | r | p | r | p | |
| Age (years) | 0.66 | ns | −0.06 | ns | 0.065 | ns | −0.10 | 0.07 ns | 0.23 | ns |
| Weight (kg) | 0.26 | ns | 0.42 | ns | 0.43 | 0.058 | 0.37 | ns | 0.36 | ns |
| BMI (kg/m2) | 0.24 | ns | 0.35 | ns | 0.44 | 0.052 | 0.37 | ns | 0.36 | ns |
| Waist circumference (cm) | 0.58 | 0.007 ** | 0.58 | 0.006 ** | 0.63 | 0.003 ** | 0.41 | 0.07 | 0.51 | 0.02 * |
| AST (U/L) | 0.20 | ns | 0.1 | ns | 0.24 | ns | 0.27 | ns | 0.14 | ns |
| ALT (U/L) | 0.49 | 0.02 * | 0.57 | 0.008 ** | 0.63 | 0.003 ** | 0.53 | 0.016 * | 0.43 | 0.05 * |
| sCD14 T0 (µg/mL) | 0.41 | 0.06 | 0.45 | 0.04 * | 0.28 | ns | −0.15 | ns | 0.058 | ns |
| Lean (n = 8) | ||||||||||
| T0 min | T60 min | T120 min | T180 min | T300 min | ||||||
| r | p | r | p | r | p | r | p | r | p | |
| Age (years) | 0.7 | 0.02 * | 0.43 | ns | 0.43 | ns | 0.35 | ns | 0.47 | ns |
| Weight (kg) | −0.31 | ns | −0.16 | ns | −0.02 | ns | 0.09 | ns | 0.07 | ns |
| BMI (kg/m2) | −0.23 | ns | −0.18 | ns | −0.08 | ns | 0.02 | ns | 0.05 | ns |
| Waist circumference (cm) | 0.66 | 0.04 * | 0.60 | 0.06 | 0.71 | 0.02 * | 0.72 | 0.02 * | 0.58 | 0.08 |
| AST (U/L) | 0.55 | ns | 0.18 | ns | 0.22 | ns | 0.27 | ns | 0.23 | ns |
| ALT (U/L) | 0.69 | 0.03 * | 0.62 | 0.05 * | 0.68 | 0.03 * | 0.51 | ns | 0.38 | ns |
| sCD14 T0 (µg/mL) | 0.05 | ns | 0.05 | ns | −0.01 | ns | 0.17 | ns | −0.02 | ns |
| Obese (n = 8) | ||||||||||
| T0 min | T60 min | T120 min | T180 min | T300 min | ||||||
| r | p | r | p | r | p | r | p | r | p | |
| Age (years) | −0.48 | ns | −0.56 | ns | −0.17 | ns | −0.09 | ns | −0.04 | ns |
| Weight (kg) | −0.13 | ns | 0.18 | ns | −0.27 | ns | 0.25 | ns | 0.06 | ns |
| BMI (kg/m2) | −0.31 | ns | −0.46 | ns | −0.13 | ns | 0.07 | ns | 0.17 | ns |
| Waist circumference (cm) | 0.25 | ns | 0.05 | ns | 0.13 | ns | −0.13 | ns | 0.35 | ns |
| AST (U/L) | −0.33 | ns | −0.27 | ns | −0.07 | ns | 0.23 | ns | −0.13 | ns |
| ALT (U/L) | −0.11 | ns | 0.04 | ns | 0.18 | ns | 0.53 | ns | 0.16 | ns |
| sCD14 T0 (µg/mL) | 0.22 | ns | 0.4 | ns | 0.10 | ns | −0.13 | ns | −0.29 | ns |
| Before OF | |||
|---|---|---|---|
| Variable 1 | Variable 2 | r | p |
| LBP (µg/mL) | Trunk lean mas (kg) | 0.65 | 0.002 ** |
| Lean mass (kg) | 0.57 | 0.009 ** | |
| Waist circumference (cm) | 0.53 | 0.02 * | |
| BMI (kg/m2) | 0.47 | 0.04 * | |
| Fat trunk (kg) | 0.41 | ns | |
| Visceral fat (kg) | 0.52 | 0.03 * | |
| LBP/sCD14 | Lean mass (kg) | 0.62 | 0.004 ** |
| Fat trunk (kg) | 0.48 | 0.04 * | |
| BMI (kg/m2) | 0.62 | 0.004 ** | |
| After OF | |||
| Variable 1 | Variable 2 | r | p |
| LBP (µg/mL) | Trunk lean mas (kg) | 0.62 | 0.003 ** |
| Lean mass (kg) | 0.56 | 0.01 * | |
| Waist circumference (cm) | 0.51 | 0.02 * | |
| BMI (kg/m2) | 0.32 | ns | |
| Fat trunk (kg) | 0.47 | 0.04 * | |
| Visceral fat (kg) | 0.07 | ns | |
| LBP/sCD14 | Lean mass (kg) | 0.49 | 0.03 * |
| Fat trunk (kg) | 0.49 | 0.03 * | |
| BMI (kg/m2) | 0.49 | 0.03 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laugerette, F.; Vors, C.; Alligier, M.; Pineau, G.; Drai, J.; Knibbe, C.; Morio, B.; Lambert-Porcheron, S.; Laville, M.; Vidal, H.; et al. Postprandial Endotoxin Transporters LBP and sCD14 Differ in Obese vs. Overweight and Normal Weight Men during Fat-Rich Meal Digestion. Nutrients 2020, 12, 1820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061820
Laugerette F, Vors C, Alligier M, Pineau G, Drai J, Knibbe C, Morio B, Lambert-Porcheron S, Laville M, Vidal H, et al. Postprandial Endotoxin Transporters LBP and sCD14 Differ in Obese vs. Overweight and Normal Weight Men during Fat-Rich Meal Digestion. Nutrients. 2020; 12(6):1820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061820
Chicago/Turabian StyleLaugerette, Fabienne, Cécile Vors, Maud Alligier, Gaëlle Pineau, Jocelyne Drai, Carole Knibbe, Béatrice Morio, Stéphanie Lambert-Porcheron, Martine Laville, Hubert Vidal, and et al. 2020. "Postprandial Endotoxin Transporters LBP and sCD14 Differ in Obese vs. Overweight and Normal Weight Men during Fat-Rich Meal Digestion" Nutrients 12, no. 6: 1820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061820