Therapeutic Effect, Rheological Properties and α-Amylase Resistance of a New Mixed Starch and Xanthan Gum Thickener on Four Different Phenotypes of Patients with Oropharyngeal Dysphagia

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
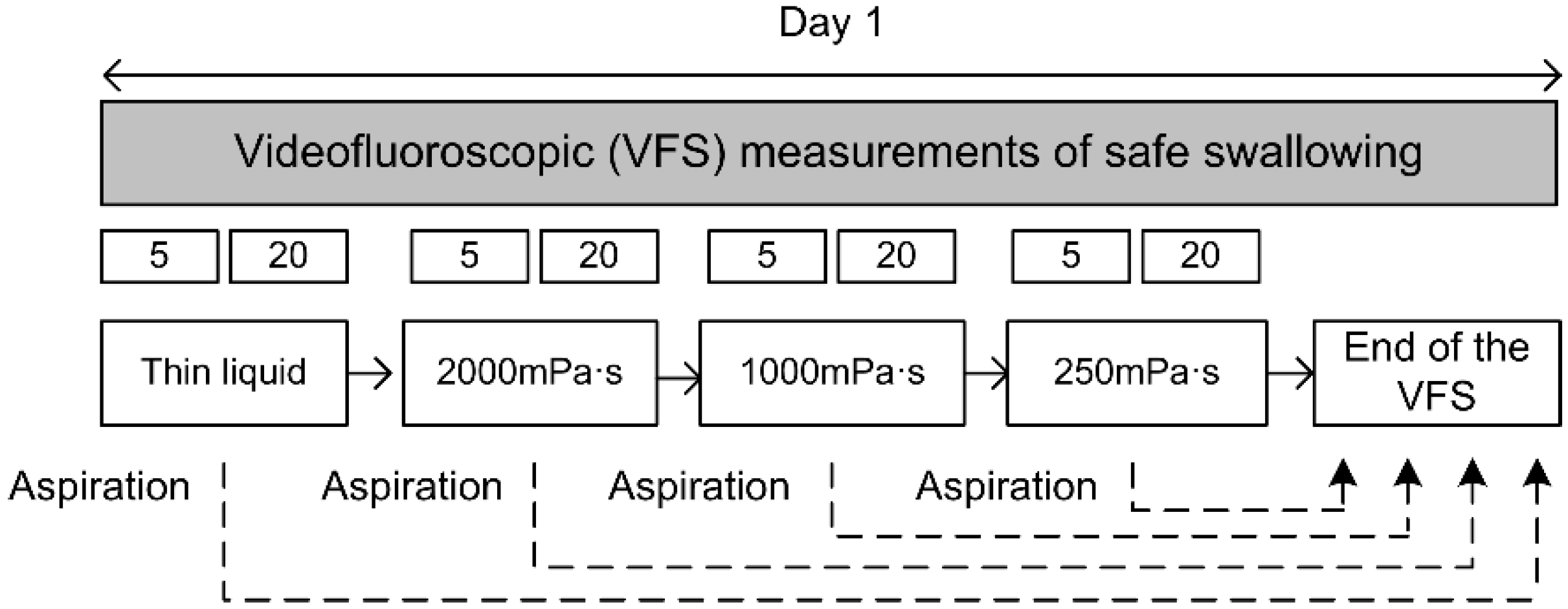
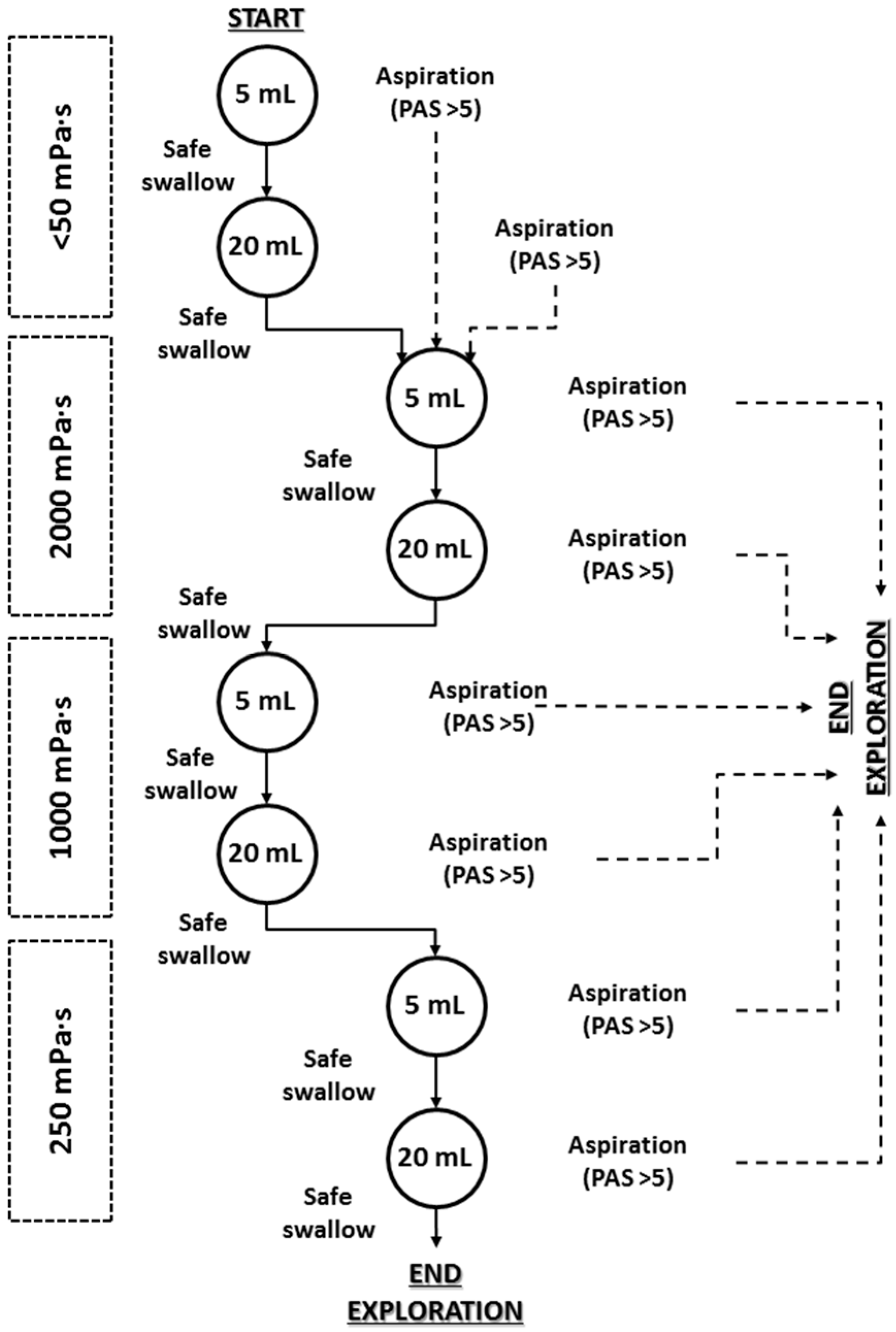
2.1. Study Design
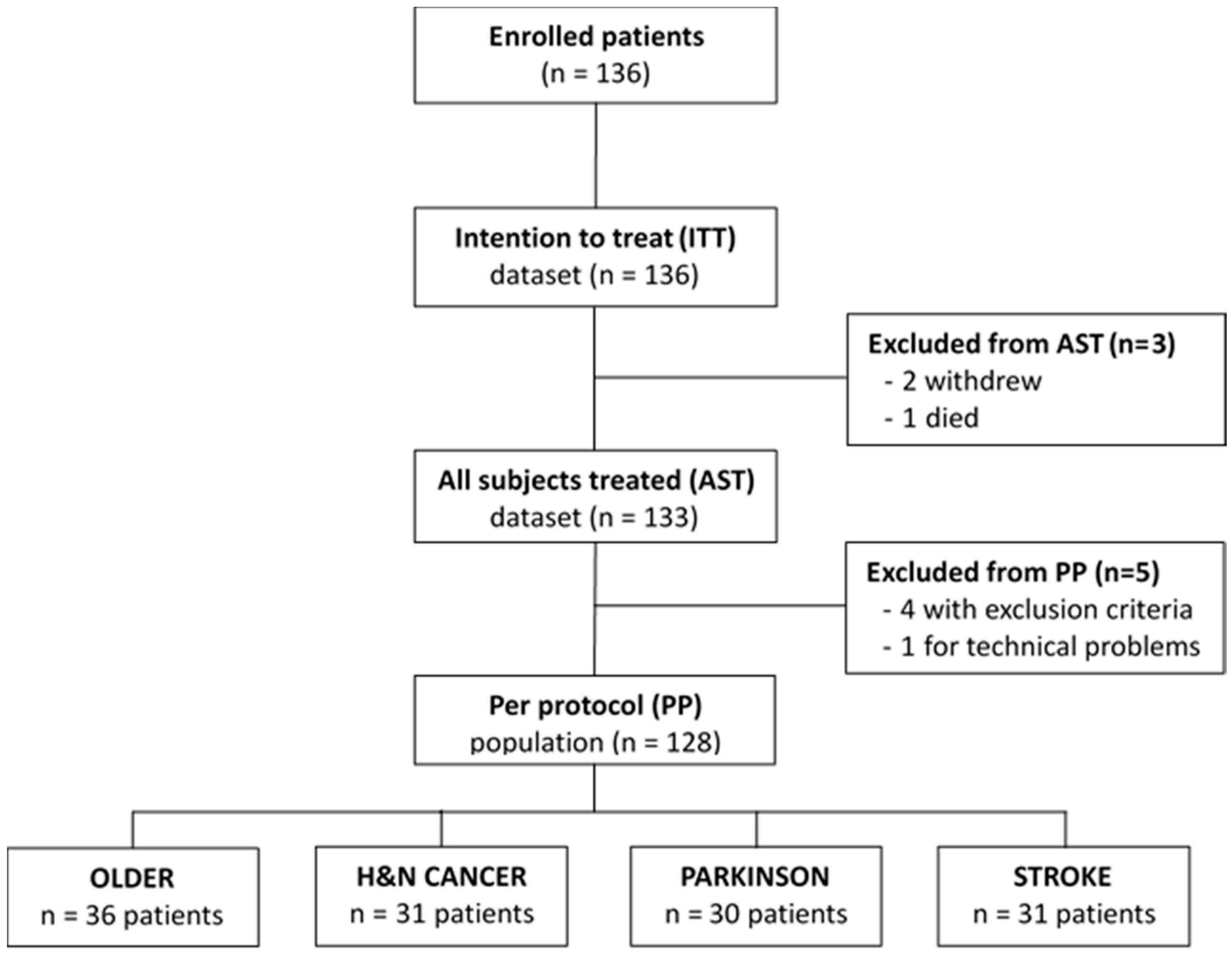
2.2. Study Population
2.3. Study Product and Bolus Rheology
2.4. Swallowing Evaluation Measurements
2.4.1. Screening (V-VST)
2.4.2. Instrumental Evaluation (Videofluoroscopy)
2.5. Rheological Characterization
2.6. Palatability of the Product
2.7. Adverse Events
2.8. Data and Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Population
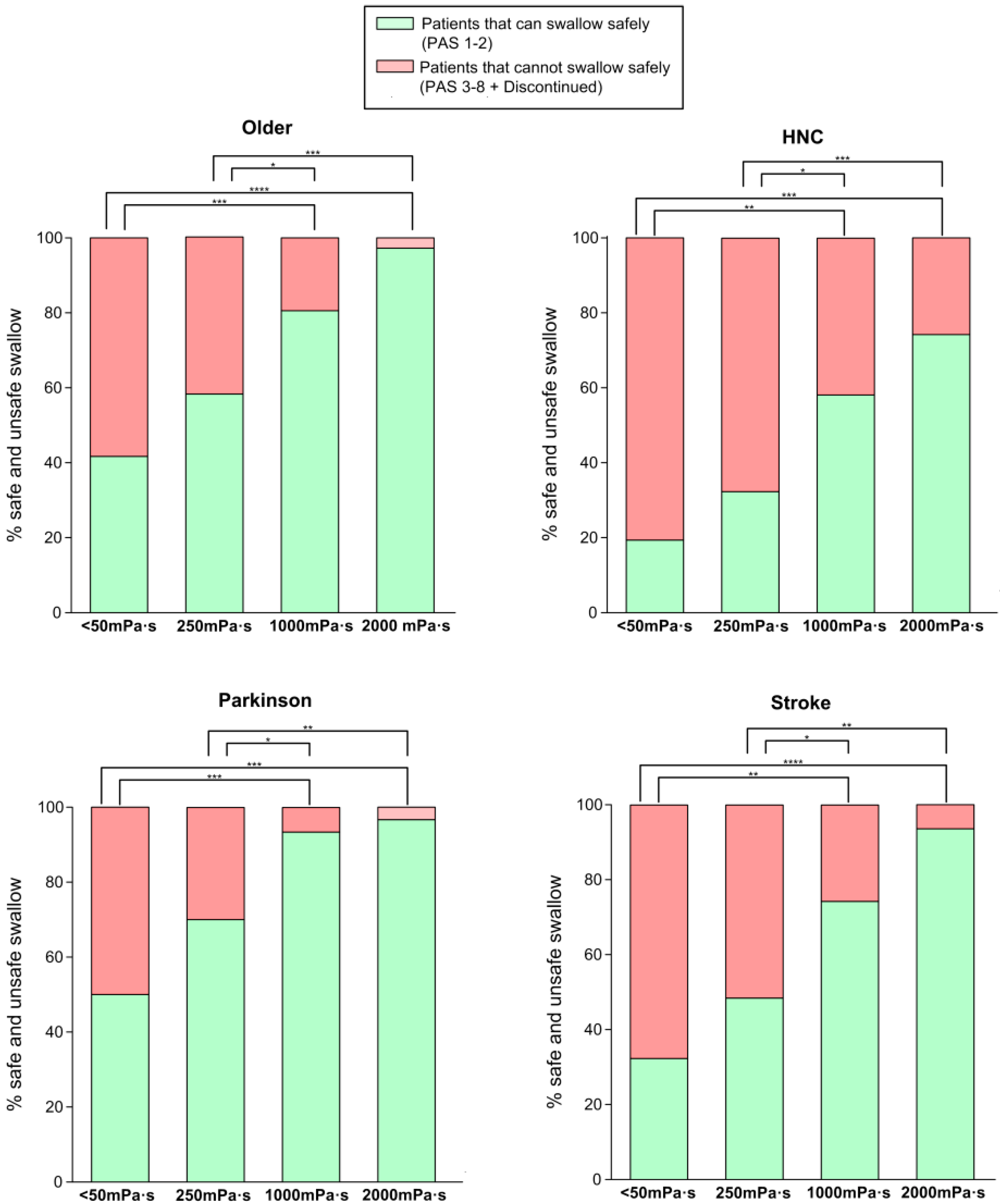
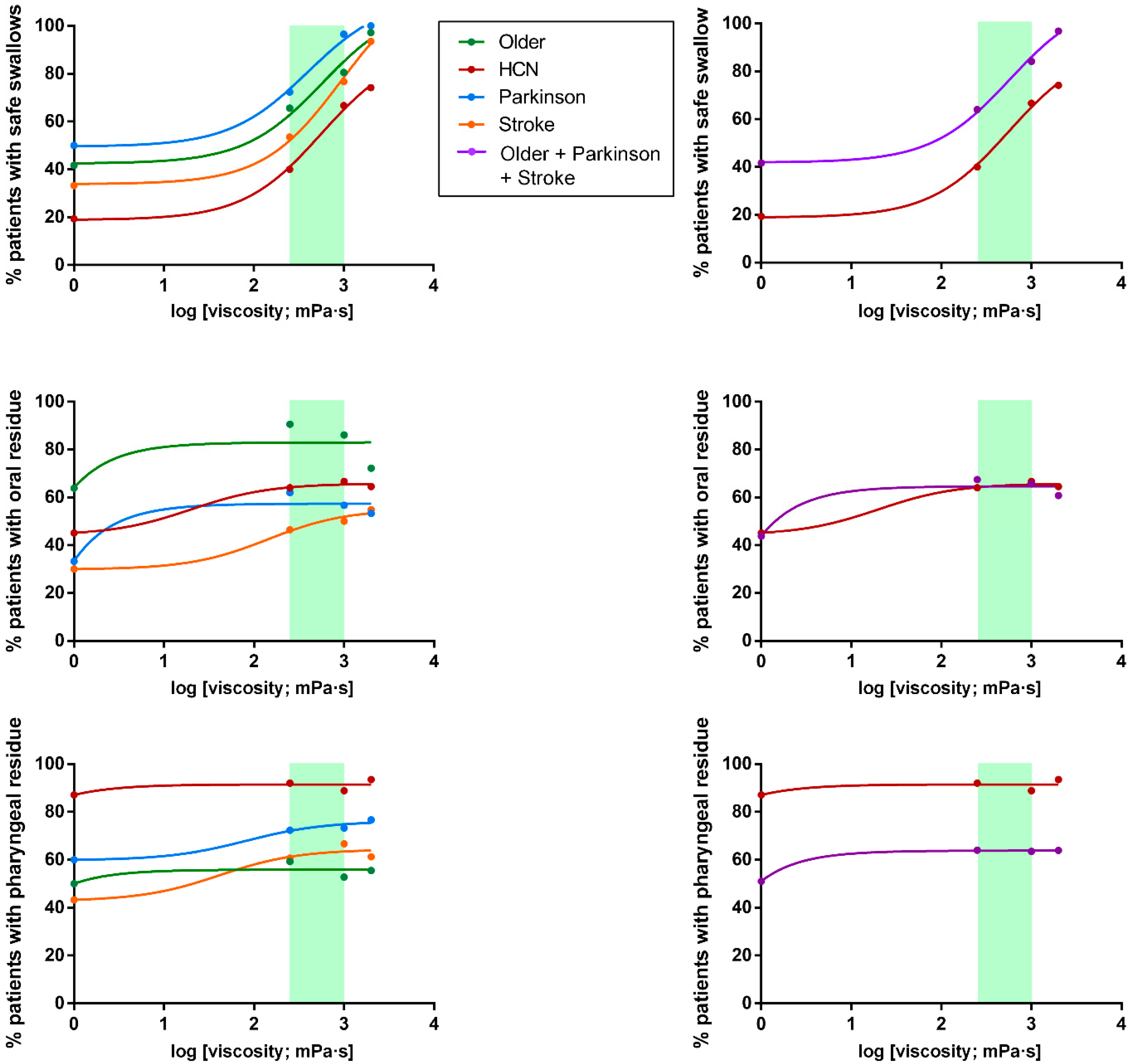
3.2. Swallowing Evaluation by Videofluoroscopy (VFS)
3.2.1. Videofluoroscopic Signs
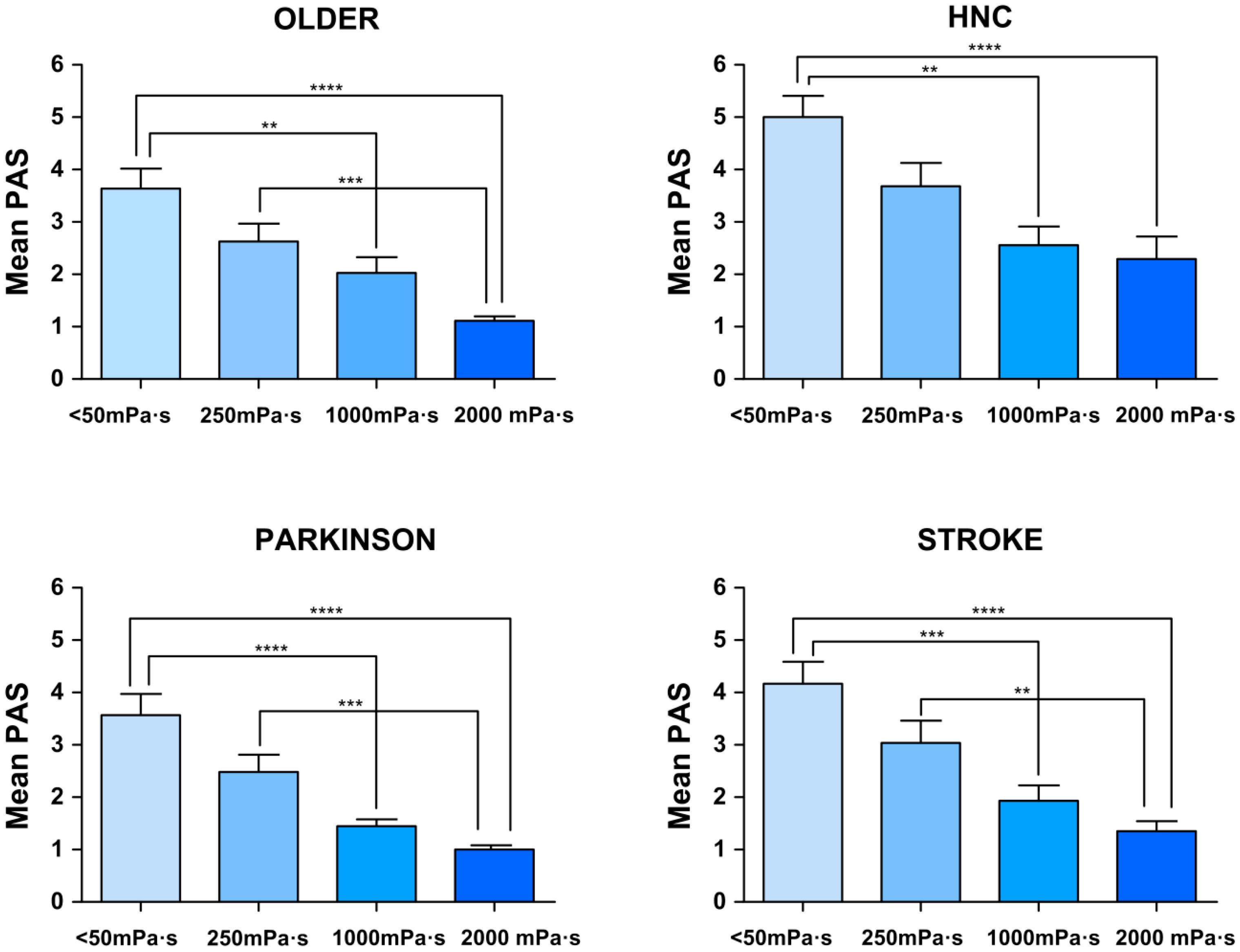
3.2.2. Oropharyngeal Swallow Response (OSR)
3.3. In Vitro Studies
3.4. Palatability of the Product
3.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. 2016. Available online: http://apps.who.int/classifications/icd10/browse/2016/en (accessed on 19 February 2020).
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders–European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.-C.; Wu, S.-C.; Chen, H.S.; Wang, T.-G.; Chen, M.-Y. Prevalence of impaired swallowing in institutionalized older people in taiwan. J. Am. Geriatr. Soc. 2002, 50, 1118–1123. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Hinojosa, G.; López, D.; Juan, M.; Fabré, E.; Voss, D.S.; Calvo, M.; Marta, V.; Ribó, L.; Palomera, E.; et al. Prevalence Of Oropharyngeal Dysphagia And Impaired Safety And Efficacy Of Swallow In Independently Living Older Persons. J. Am. Geriatr. Soc. 2011, 59, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Caudell, J.J.; Schaner, P.E.; Meredith, R.F.; Locher, J.; Nabell, L.M.; Carroll, W.R.; Magnuson, J.S.; Spencer, S.A.; Bonner, J.A. Factors Associated With Long-Term Dysphagia After Definitive Radiotherapy for Locally Advanced Head-and-Neck Cancer. Int. J. Radiat. Oncol. 2009, 73, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Martino, R.; Foley, N.C.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia After Stroke. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muriana, D. Factors de risc clínics, fisiopatològics i topogràfics associats a disfàgia orofaríngea en pacients amb ictus. Ph.D. Thesis, Unitat d’Exploracions Funcionals Digestives/Servei Neurologia/Departament Medicina, Universitat Autònoma de Barcelona, (UAB), Barcelona, Spain, 2016. [Google Scholar]
- Rofes, L.; Muriana, D.; Palomeras, E.; Vilardell, N.; Palomera, E.; Alvarez-Berdugo, D.; Casado, V.; Clavé, P. Prevalence, risk factors and complications of oropharyngeal dysphagia in stroke patients: A cohort study. Neurogastroenterol. Motil. 2018, 30, e13338. [Google Scholar] [CrossRef]
- Kalf, J.; De Swart, B.; Bloem, B.R.; Munneke, M. Prevalence of oropharyngeal dysphagia in Parkinson’s disease: A meta-analysis. Park. Relat. Disord. 2012, 18, 311–315. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Mir, P.; Cabre, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851–858.e230. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Palomera, M.; Gomez, C.; Sar-Shalom, D.; Saiz, A.; Montoya, J.G.; Navajas, M.; Clavé, P. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: A population-based prospective study. Age Ageing 2012, 41, 376–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Gastroenterological Association. American Gastroenterological Association medical position statement on management of oropharyngeal dysphagia. Gastroenterology 1999, 23, 452–454. [Google Scholar]
- Logemann, J.A. Manual for the Videofluorographic Study of Swallowing, 2nd ed.; Pro-Ed: Nerang, Australia, 1998. [Google Scholar]
- Logemann, J.A. Dysphagia: Evaluation and Treatment. Folia Phoniatr. et Logop. 1995, 47, 140–164. [Google Scholar] [CrossRef] [PubMed]
- Clavé, P.; De Kraa, M.; Arreola, V.; Girvent, M.; Farré, R.; Palomera, E.; Serra-Prat, M. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment. Pharmacol. Ther. 2006, 24, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Baijens, L.; Heijnen, M.; Zwijnenberg, I. Effects of Therapy in Oropharyngeal Dysphagia by Speech and Language Therapists: A Systematic Review. Dysphagia 2009, 25, 40–65. [Google Scholar] [CrossRef] [Green Version]
- Perlman, A.L.; Booth, B.M.; Grayhack, J.P. Videofluoroscopic predictors of aspiration in patients with oropharyngeal dysphagia. Dysphagia 1994, 9, 90–95. [Google Scholar] [CrossRef]
- Garcia, J.M.; Chambers, E.; Molander, M. Thickened liquids: Practice patterns of speech-language pathologists. Am. J. Speech-Language Pathol. 2005, 14, 4–13. [Google Scholar] [CrossRef]
- Rosenvinge, S.K.; Starke, I.D. Improving care for patients with dysphagia. Age Ageing 2005, 34, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Gallegos, C.; La Fuente, E.B.-D.; Clavé, P.; Costa, A.; Assegehegn, G. Nutritional Aspects of Dysphagia Management. Adv. Food Nutr. Res. 2017, 81, 271–318. [Google Scholar] [CrossRef] [PubMed]
- Hanson, B.; O’Leary, M.T.; Smith, C.H. The Effect of Saliva on the Viscosity of Thickened Drinks. Dysphagia 2011, 27, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Vallons, K.J.R.; Helmens, H.J.; Oudhuis, A.A.C.M. Effect of human saliva on the consistency of thickened drinks for individuals with dysphagia. Int. J. Lang. Commun. Disord. 2014, 50, 165–175. [Google Scholar] [CrossRef]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249. [Google Scholar] [CrossRef] [Green Version]
- Rofes, L.; Arreola, V.; Mukherjee, R.; Swanson, J.; Clavé, P. The effects of a xanthan gum-based thickener on the swallowing function of patients with dysphagia. Aliment. Pharmacol. Ther. 2014, 39, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Vilardell, N.; Rofes, L.; Arreola, V.; Speyer, R.; Clavé, P. A Comparative Study Between Modified Starch and Xanthan Gum Thickeners in Post-Stroke Oropharyngeal Dysphagia. Dysphagia 2015, 31, 169–179. [Google Scholar] [CrossRef]
- Bolivar-Prados, M.; Rofes, L.; Arreola, V.; Guida, S.; Nascimento, W.; Martin, A.; Vilardell, N.; Ortega, O.; Ripken, D.; Lansink, M.; et al. Effect of a gum-based thickener on the safety of swallowing in patients with poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2019, 31, e13695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partal, P.; Franco, J.M. Non-Newtonian Fluids. In Rheology, Vol. I. Oxford: Encyclopaedia of Life Support Systems (EOLSS); Gallegos, C., Ed.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 96–119. [Google Scholar]
- Brito-de la Fuente, E.; Turcanu, M.; Ekberg, O.; Gallegos, C. Rheological Aspects of Swallowing and Dysphagia: Shear and Elongational Flows. In Dysphagia. Medical Radiology; Ekberg, O., Ed.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 687–716. [Google Scholar]
- Clavé, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. FUNCTIONAL EVALUATION: THE BARTHEL INDEX. Md. State Med, J. 1965, 14, 61–65. [Google Scholar]
- Rabin, R.; De Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, A.; et al. Validation of the Mini Nutritional Assessment short-form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Clavé, P. The Volume-Viscosity Swallow Test for Clinical Screening of Dysphagia and Aspiration. Nestlé Nutr. Inst. Workshop Ser. 2012, 72, 33–42. [Google Scholar]
- Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P.; Ortega, O. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716. [Google Scholar] [CrossRef]
- Rosenbek, J.C.; Robbins, J.A.; Roecker, E.B.; Coyle, J.L.; Wood, J.L. A penetration-aspiration scale. Dysphagia 1996, 11, 93–98. [Google Scholar] [CrossRef]
- Rofes, L.; Clavé, P.; Ouyang, A.; Scharitzer, M.; Pokieser, P.; Vilardell, N.; Ortega, O. Neuogenic and oropharyngeal dysphagia. Ann. N. Y. Acad. Sci. 2013, 1300, 1–10. [Google Scholar] [CrossRef]
- World Health Organization and Uppsala Monitoring Centre. The use of the WHO-UMC system for standardized case causality assessment. Uppsala Uppsala Monit. Cent. 2014, 48, 194–203. [Google Scholar]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and Management of Oropharyngeal Dysphagia Among Older Persons, State of the Art. J. Am. Med Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Vilardell, N.; Rofes, L.; Arreola, V.; Martin, A.; Muriana, D.; Palomeras, E.; Ortega, O.; Clavé, P. Videofluoroscopic assessment of the pathophysiology of chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2017, 29, e13111. [Google Scholar] [CrossRef]
- Rofes, L.; Cola, P.C.; Clave, P. The effects of sensory stimulation on neurogenic oropharyngeal dysphagia. J. Gastroenterol. Hepatol. Res. 2014, 3, 1066–1072. [Google Scholar]
- Wakabayashi, H. Presbyphagia and Sarcopenic Dysphagia: Association between Aging, Sarcopenia, and Deglutition Disorders. J. Frailty Aging 2014, 3, 97–103. [Google Scholar]
- Sacco, R.L.; Diamond, B.; Aviv, J.E.; Thomson, J.; Martin, J.H.; Tandon, R.; Close, L.G. Silent Laryngopharyngeal Sensory Deficits after Stroke. Ann. Otol. Rhinol. Laryngol. 1997, 106, 87–93. [Google Scholar] [CrossRef]
- Rofes, L.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P. Spatiotemporal characteristics of the pharyngeal event-related potential in healthy subjects and older patients with oropharyngeal dysfunction. Neurogastroenterol. Motil. 2016, 29, e12916. [Google Scholar] [CrossRef]
- Cabib, C.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P.; Rofes, L. Chronic post-stroke oropharyngeal dysphagia is associated with impaired cortical activation to pharyngeal sensory inputs. Eur. J. Neurol. 2017, 24, 1355–1362. [Google Scholar] [CrossRef]
- Yver, C.M.; Kennedy, W.P.; Mirza, N.A. Taste acceptability of thickening agents☆. World J. Otorhinolaryngol. -Head Neck Surg. 2018, 4, 145–147. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OLDER | HNC | PARKINSON | STROKE | p-Value | |
|---|---|---|---|---|---|
| N | 36 | 31 | 30 | 31 | - |
| Age | 82.96 ± 1.24 | 68. 29 ± 1.39 **** | 72.34 ± 1.92 **** | 79.42 ± 1.36 #### ŦŦŦ | <0.0001 |
| Sex (female, %) | 66.67 (24) | 32.26 (10) ** | 20.00 (6) *** | 35.48 (11) * | 0.0008 |
| Barthel (%) Optimum (100) (%) Sub-optimum (<100) (%) | 78.33 ± 4.25 38.89 (14) 61.11 (22) | 96.50 ± 1.68 * 67.34 (21) * 32.26 (10) | 77.33 ± 4.48 # 23.33 (7) ### 76.67 (23) | 74.83 ± 5.31#Ŧ 43.33 (13) 56.67 (17) | 0.0007 0.005 |
| MNA-sf (%) Well-nourished (12–14) At risk (8–11) Malnourished (0–7) | 10.97 ± 0.38 47.22 (17) 44.44 (16) 8.33 (3) | 11.50 ± 0.35 48.57 (17) 37.14 (13) 2.86 (1) | 11.7 ± 0.47 # 60.00 (18) 33.33 (10) 6.67 (2) | 10.6 ± 0.51## 36.67 (11) 56.67 (17) 6.67 (2) | 0.326 0.610 |
| BMI (kg/m2) | 27.59 ± 0.88 | 23.97 ± 0.69 * | 27.50 ± 0.85 | 27.78 ± 0.74 | 0.002 |
| Handgrip Force (kg) | 16.33 ± 1.42 | 22.78 ± 1.97 | 25.38 ± 1.78 ** | 17.77 ± 1.48Ŧ | 0.0009 |
| Health status self-perception (0–100) | 63.57 ± 3.32 | 70.83 ± 3.85 | 56.25 ± 3.74# | 58.67 ± 5.29 | 0.055 |
| ALL | OLDER | HNC | PARKINSON | STROKE | p-Value | |
|---|---|---|---|---|---|---|
| N | 128 | 36 | 31 | 30 | 31 | |
| Impaired Efficacy (%) Oral Residue Pharyngeal Residue | 98.44 (126) 82.81 (106) 80.47 (103) | 100.00 (36) 91.67 (33) 66.67 (24) | 100.00 (31) 80.65 (31) 96.80 (30) ** | 100.00 (30) 76.67 (23) ## 86.67 (26) #### | 96.67 (29) 61.29 (19) ** ### 74.19 (23) # Ŧ | nc 0.0002 <0.0001 |
| Impaired Safety (%) Penetrations Aspirations Silent Aspirations (PAS = 8) | 70.31 (90) 61.72 (79) 28.91 (37) 14.84 (19) | 63.89 (23) 58.3 (21) 25.00 (9) 11.11 (4) | 83.87 (26) 74.19 (23) 41.94 (13) 25.81 (8) | 56.67 (17) # 46.67 (14) # 13.33 (4) # 13.33 (4) | 77.42 (24) 67.74 (21) 35.48 (11) 9.67 (3) | 0.076 0.135 0.071 0.256 |
| Higher PAS score | 4.44 ± 0.20 | 4.08 ± 0.39 | 5.36 ± 0.41 | 3.80 ± 0.40# | 4.55 ± 0.41 | 0.038 |
| <50 mPa·s (5 mL) | 250 mPa·s (5 mL) | 1000 mPa·s (5 mL) | 2000 mPa·s (5 mL) | p-Value | ||
|---|---|---|---|---|---|---|
| ALL | LVC (ms) | 387.00 ± 13.32 | 359.00 ± 11.68 | 315.80 ± 9.59 *** # | 316.20 ± 10.92 **** ## | <0.0001 |
| UESO (ms) | 259.50 ± 9.79 | 257.20 ± 9.40 | 260.00 ± 8.61 | 290.10 ± 15.34 | 0.066 | |
| KE (mJ) | 0.96 ± 0.08 | 0.90 ± 0.06 | 0.83 ± 0.06 | 0.85 ± 0.10 | 0.112 | |
| Force (mN) | 14.87 ± 1.01 | 14.43 ± 1.08 | 13.19 ± 0.97 | 13.31 ± 1.42 | 0.228 | |
| bolus vel. (m/s) | 0.26 ± 0.01 | 0.27 ± 0.01 | 0.27 ± 0.01 | 0.24 ± 0.01 | 0.230 | |
| OLDER | LVC (ms) | 360.00 ± 20.85 | 336.25 ± 14.90 | 298.89 ± 14.78 | 284.57 ± 12.70 * | 0.006 |
| UESO (ms) | 260.00 ± 18.69 | 238.75 ± 13.85 | 232.22 ± 8.72 | 262.86 ± 14.21 | 0.304 | |
| KE (mJ) | 0.90 ± 0.11 | 0.90 ± 0.11 | 0.92 ± 0.10 | 0.80 ± 0.15 | 0.408 | |
| Force (mN) | 14.64 ± 1.63 | 15.24 ± 1.65 | 14.73 ± 1.23 | 12.48 ± 1.83 | 0.228 | |
| bolus vel. (m/s) | 0.26 ± 0.02 | 0.27 ± 0.01 | 0.27 ± 0.01 | 0.25 ± 0.02 | 0.541 | |
| HNC | LVC (ms) | 428.00 ± 35.11 | 370.00 ± 30.48 | 338.46 ± 26.37 | 360.00 ± 32.72 | 0.222 |
| UESO (ms) | 240.00 ± 21.07 | 257.60 ± 19.47 | 280.00 ± 19.80 | 282.80 ± 25.26 | 0.153 | |
| KE (mJ) | 1.28 ± 0.25 | 0.82 ± 0.12 | 0.62 ± 0.07 | 0.81 ± 0.16 | 0.160 | |
| Force (mN) | 18.57 ± 3.08 | 12.13 ± 1.57 | 9.50 ± 1.11 | 12.28 ± 2.22 | 0.136 | |
| bolus vel. (m/s) | 0.33 ± 0.03 | 0.28 ± 0.02 | 0.25 ± 0.01 | 0.27 ± 0.02 | 0.157 | |
| PARKINSON | LVC (ms) | 373.33 ± 21.81 | 342.07 ± 26.68 | 293.33 ± 17.82 * | 289.33 ± 12.08 * | 0.009 |
| UESO (ms) | 257.33 ± 20.18 | 249.66 ± 24.20 | 237.33 ± 16.49 | 241.33 ± 15.16 | 0.862 | |
| KE (mJ) | 0.89 ± 0.11 | 1.08 ± 0.18 | 0.99 ± 0.16 | 1.23 ± 0.32 | 0.963 | |
| Force (mN) | 14.18 ± 1.61 | 17.80 ± 3.30 | 16.50 ± 3.16 | 19.33 ± 4.78 | 0.946 | |
| bolus vel. (m/s) | 0.27 ± 0.02 | 0.29 ± 0.02 | 0.29 ± 0.02 | 0.30 ± 0.03 | 0.920 | |
| STROKE | LVC (ms) | 392.00 ± 27.55 | 390.67 ± 21.92 | 338.06 ± 18.35 | 335.48 ± 23.14 | 0.148 |
| UESO (ms) | 281.33 ± 18.14 | 284.00 ± 16.98 | 296.77 ± 21.37 | 326.45 ± 23.18 | 0.421 | |
| KE (mJ) | 0.74 ± 0.07 | 0.77 ± 0.10 | 0.73 ± 0.10 | 0.58 ± 0.07 | 0.317 | |
| Force (mN) | 11.90 ± 1.14 | 12.17 ± 1.44 | 11.34 ± 1.47 | 9.26 ± 1.13 | 0.325 | |
| bolus vel. (m/s) | 0.24 ± 0.01 | 0.24 ± 0.02 | 0.24 ± 0.02 | 0.21 ± 0.01 | 0.3367 | |
| OLDER + PARKINSON + STROKE | LVC (ms) | 374.20 ± 13.47 | 356.40 ± 12.59 | 309.70 ± 9.88 *** # | 302.5 ± 9.78 *** ## | <0.0001 |
| UESO (ms) | 265.80 ± 11.00 | 256.40 ± 10.87 | 254.40 ± 9.51 | 276.70 ± 10.82 | 0.170 | |
| KE (mJ) | 0.85 ± 0.06 | 0.92 ± 0.08 | 0.88 ± 0.07 | 0.87 ± 0.12 | 0.220 | |
| Force (mN) | 13.66 ± 0.87 | 15.07 ± 1.31 | 14.22 ± 1.19 | 13.63 ± 1.72 | 0.147 | |
| bolus vel. (m/s) | 0.26 ± 0.01 | 0.27 ± 0.01 | 0.27 ± 0.01 | 0.26 ± 0.01 | 0.267 |
| % Change (Viscosity at 50 s−1 before and after Oral Incubation) | p-Value | Shear-Thinning Effect (Linear Regression from 0 to 1000 s−1) | Correlation Coefficient‘r’ | |
|---|---|---|---|---|
| ALL | +7.85 | 0.637 | fx = −0.91x + 4.18 | 0.99 |
| +7.16 | 0.135 | fx= −0.93x + 4.71 | 0.99 | |
| −2.96 | 0.560 | fx= −0.91x + 4.94 | 0.99 | |
| OLDER | +30.47 | 0.062 | fx= −0.83x + 4.067 | 0.99 |
| −4.01 | 0.471 | fx= −0.83x + 4.39 | 0.99 | |
| −2.29 | 0.659 | fx= −0.81x + 4.69 | 0.99 | |
| HNC | +9.30 | 0.459 | fx= −0.90x + 4.15 | 0.99 |
| +4.17 | 0.531 | fx= −0.91x + 4.64 | 0.99 | |
| −1.86 | 0.706 | fx= −0.91x + 4.91 | 0.99 | |
| PARK. | +9.47 | 0.447 | fx= −0.92x + 4.2 | 0.99 |
| +11.64 | 0.061 | fx= −0.93x + 4.68 | 0.99 | |
| −5.22 | 0.424 | fx= −0.88x + 4.86 | 0.99 | |
| STROKE | −10.17 | 0.327 | fx= −0.90x + 4.09 | 0.99 |
| +14.11 | 0.025 | fx= −0.92x + 4.69 | 0.99 | |
| −2.62 | 0.683 | fx= −0.91x + 4.93 | 0.99 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, O.; Bolívar-Prados, M.; Arreola, V.; Nascimento, W.V.; Tomsen, N.; Gallegos, C.; Brito-de La Fuente, E.; Clavé, P. Therapeutic Effect, Rheological Properties and α-Amylase Resistance of a New Mixed Starch and Xanthan Gum Thickener on Four Different Phenotypes of Patients with Oropharyngeal Dysphagia. Nutrients 2020, 12, 1873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061873
Ortega O, Bolívar-Prados M, Arreola V, Nascimento WV, Tomsen N, Gallegos C, Brito-de La Fuente E, Clavé P. Therapeutic Effect, Rheological Properties and α-Amylase Resistance of a New Mixed Starch and Xanthan Gum Thickener on Four Different Phenotypes of Patients with Oropharyngeal Dysphagia. Nutrients. 2020; 12(6):1873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061873
Chicago/Turabian StyleOrtega, Omar, Mireia Bolívar-Prados, Viridiana Arreola, Weslania Viviane Nascimento, Noemí Tomsen, Crispulo Gallegos, Edmundo Brito-de La Fuente, and Pere Clavé. 2020. "Therapeutic Effect, Rheological Properties and α-Amylase Resistance of a New Mixed Starch and Xanthan Gum Thickener on Four Different Phenotypes of Patients with Oropharyngeal Dysphagia" Nutrients 12, no. 6: 1873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061873