Timing of Nutrient Ingestion after Mild to Moderate Cycling Exercise Does Not Affect Gastric Emptying Rate in Humans

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Preliminary Test Session
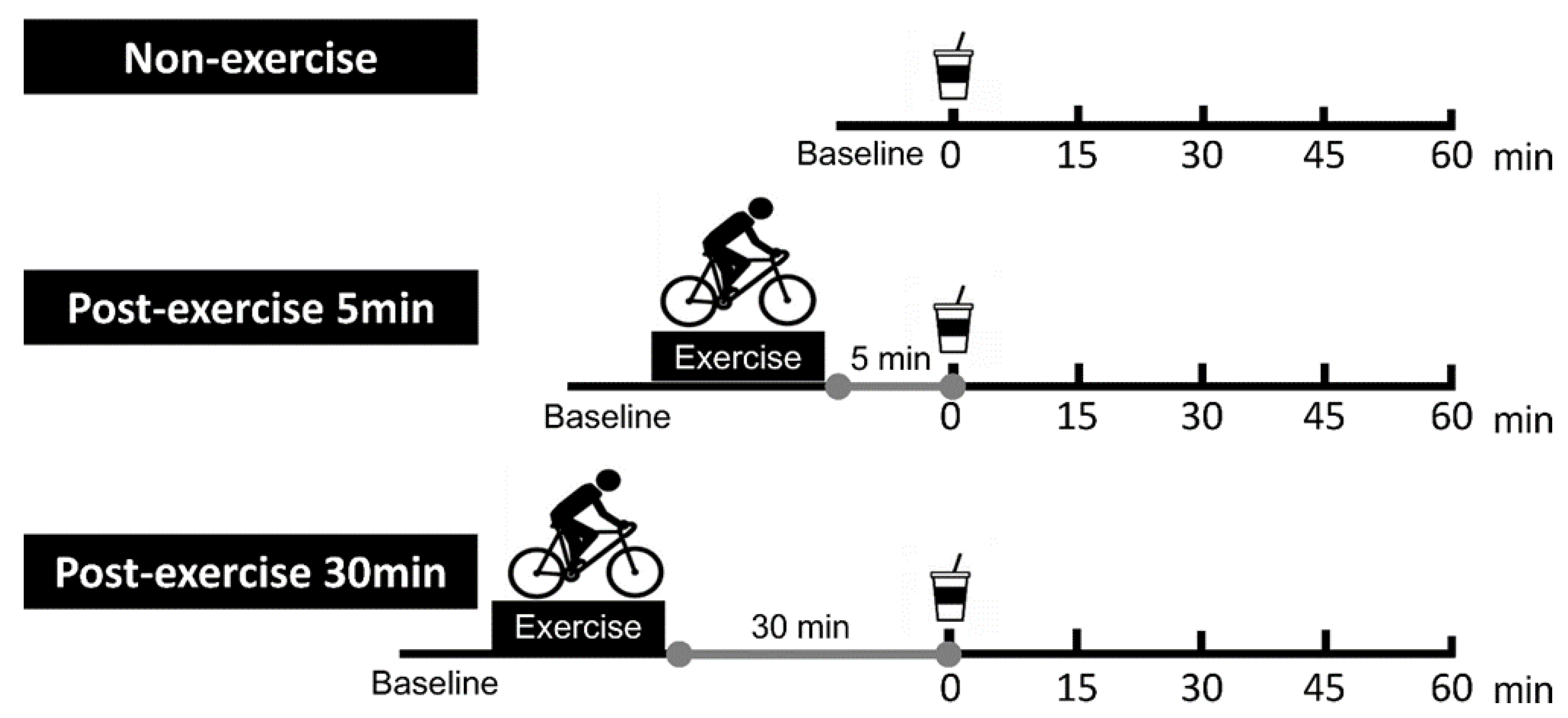
2.3. Main Trial Session
2.4. Measurements
2.4.1. GE Rate and GI Blood Flow
2.4.2. Rating Perceived Exertion, Heart Rate, Blood Lactate, Blood Glucose, and Plasma Insulin
2.5. Statistical Analysis
3. Results
3.1. Participants’ Fitness
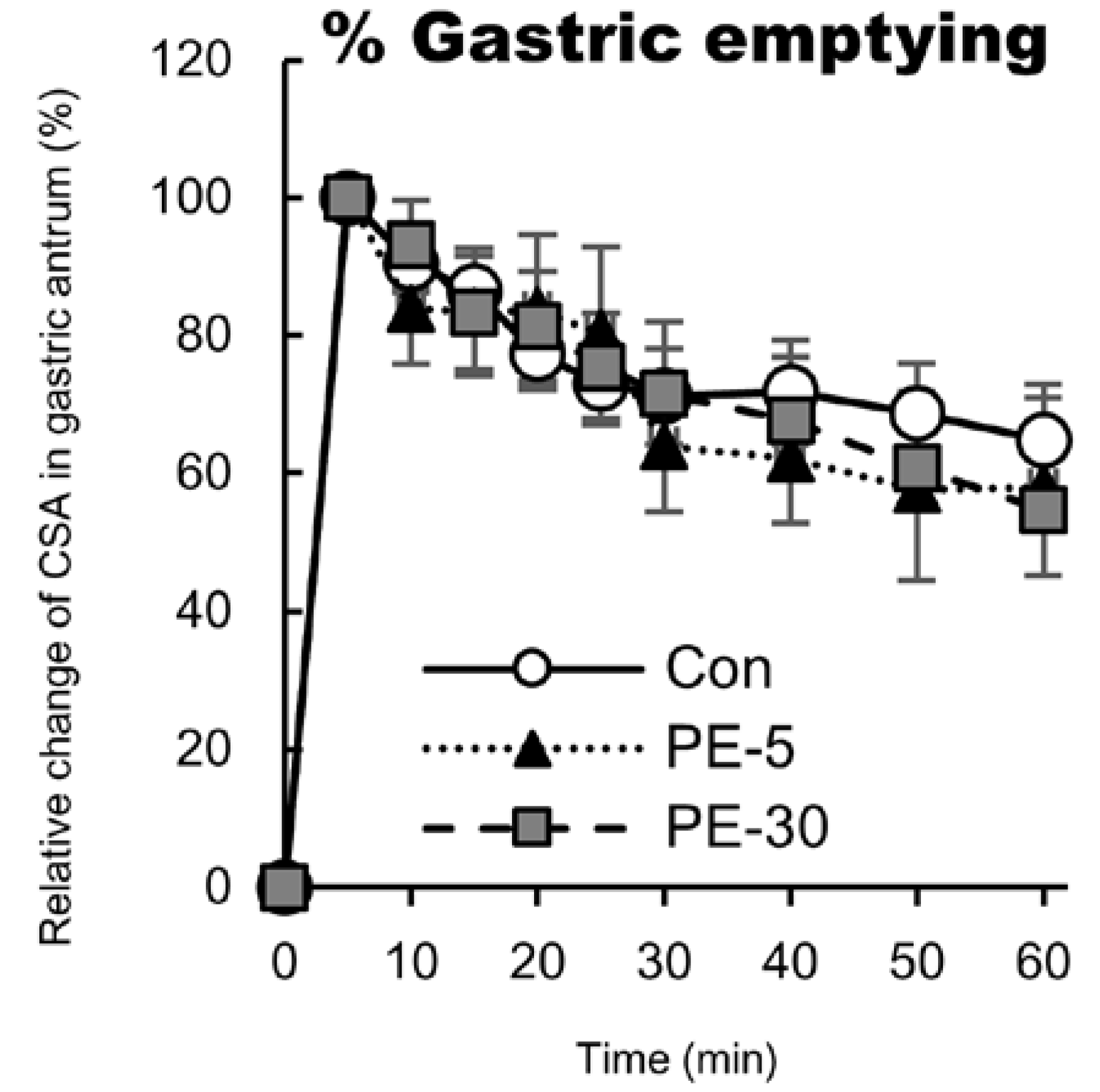
3.2. GE Rate
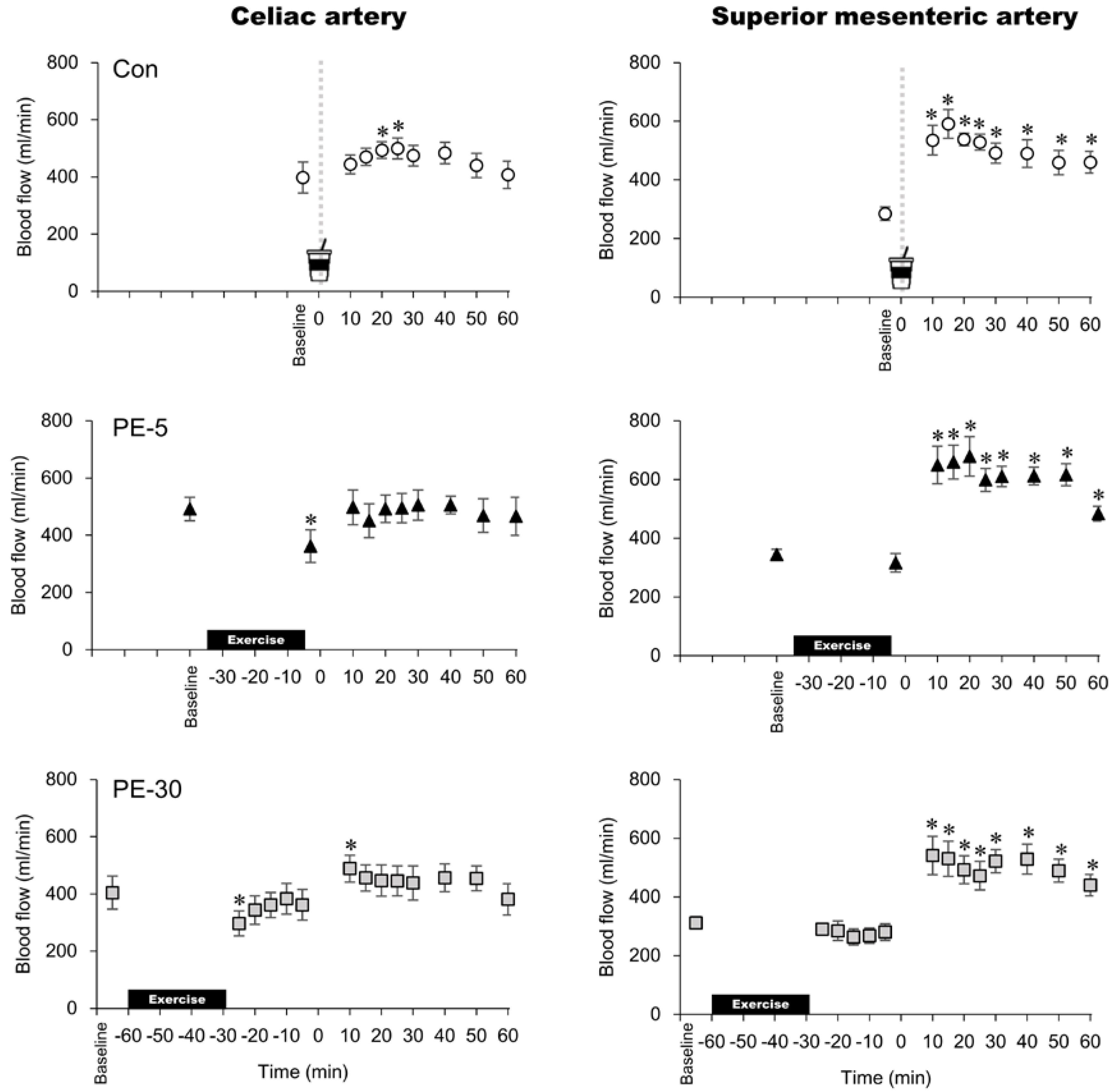
3.3. GI Blood Flow Responses
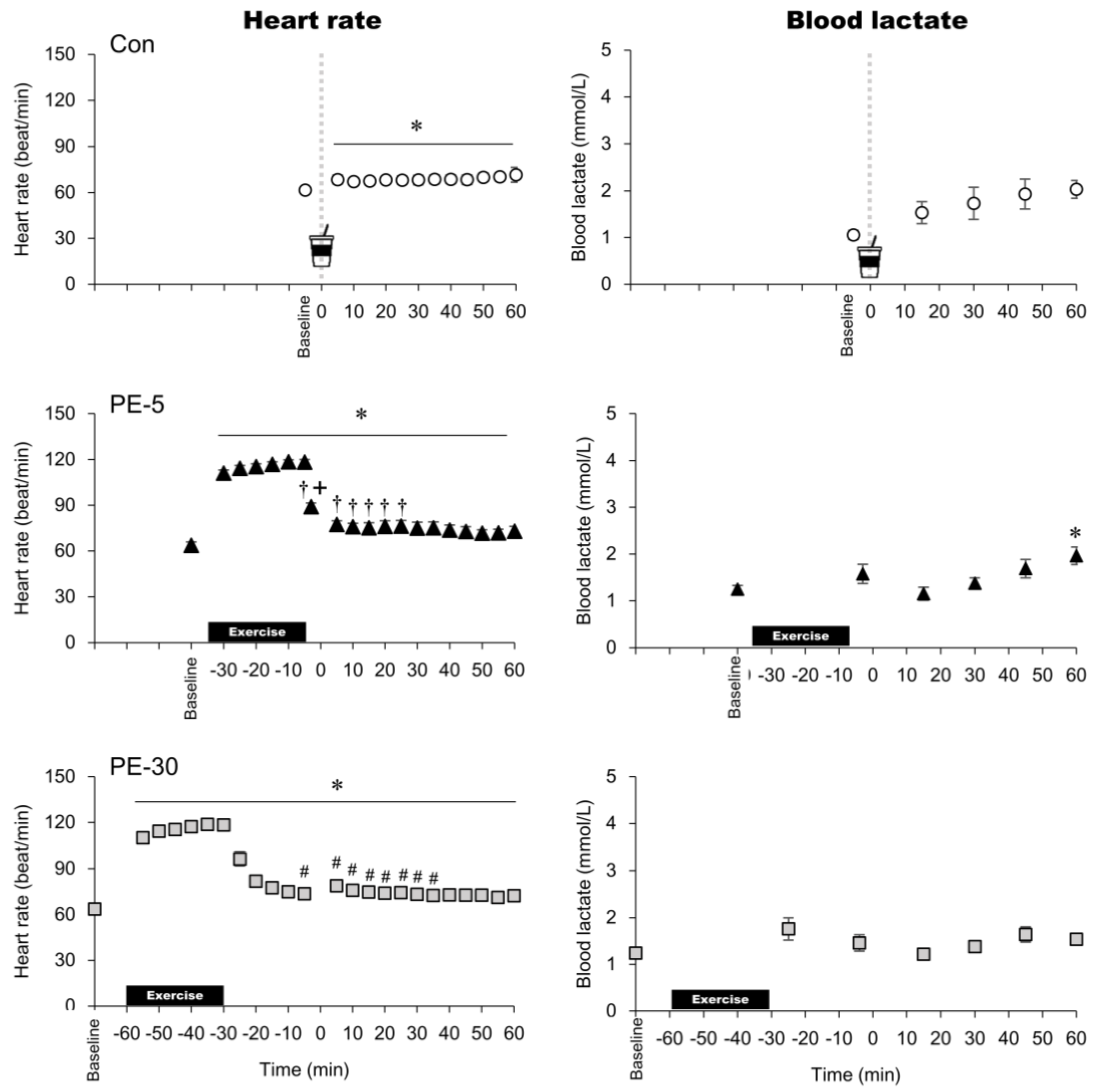
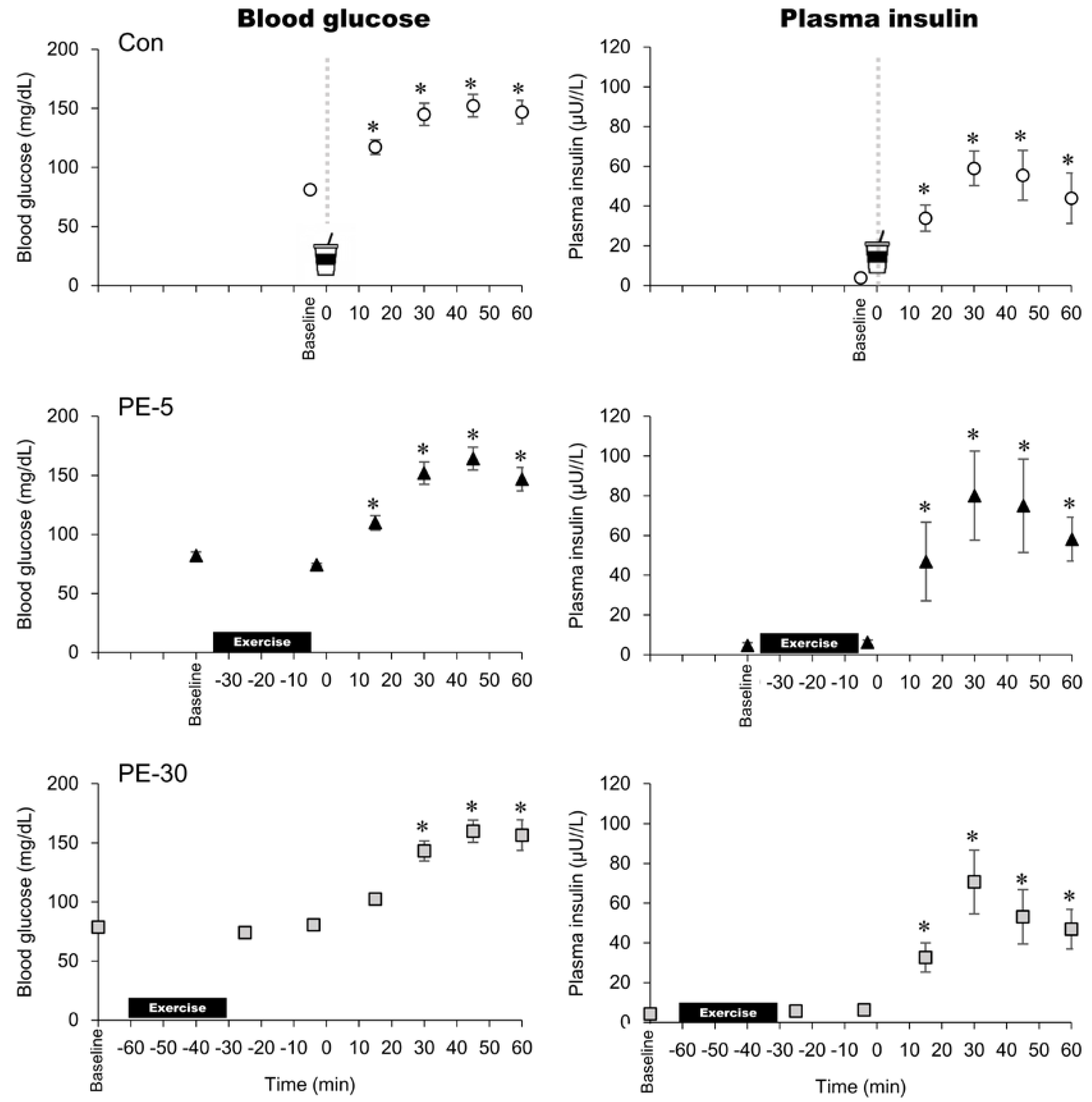
3.4. Rating Perceived Exertion, Heart Rate, Blood Lactate, Blood Glucose, and Plasma Insulin Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ter Steege, R.W.; Kolkman, J.J. Review article: The pathophysiology and management of gastrointestinal symptoms during physical exercise, and the role of splanchnic blood flow. Aliment. Pharmacol. Ther. 2012, 35, 516–528. [Google Scholar] [CrossRef]
- Van Wijck, K.; Lenaerts, K.; Grootjans, J.; Karolina, A.P.W.; Martijn, P.; van Luc, J.C.L.; Cornelis, H.C.D.; Wim, A.B. Physiology and pathophysiology of splanchnic hypoperfusion and intestinal injury during exercise: Strategies for evaluation and prevention. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G155–G168. [Google Scholar] [CrossRef] [Green Version]
- Kashima, H.; Harada, N.; Miyamoto, K.; Fujimoto, M.; Fujita, C.; Endo, M.Y.; Kobayashi, T.; Miura, A.; Fukuba, Y. Timing of post-exercise carbohydrate-protein supplementation: Roles of gastrointestinal blood flow and mucosal cell damage on gastric emptying in humans. J. Appl. Physiol. 2017, 123, 606–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashima, H.; Sugimura, K.; Taniyawa, K.; Kondo, R.; Endo, Y.M.; Tanimoto, S.; Kobayashi, T.; Miura, A.; Fukuba, Y. Timing of post-resistance exercise nutrient ingestion: Effects on gastric emptying and glucose and amino acid responses in humans. Br. J. Nutr. 2018, 120, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- van Wijck, K.; Pennings, B.; van Bijnen, A.A.; Senden, J.M.; Buurman, W.A.; Dejong, C.H.; van Loon, L.J.; Lenaerts, K. Dietary protein digestion and absorption are impaired during acute postexercise recovery in young men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R356–R361. [Google Scholar] [CrossRef] [Green Version]
- Granger, D.N.; Holm, L.; Kvietys, P. The Gastrointestinal Circulation: Physiology and Pathophysiology. Compr. Physiol. 2015, 5, 1541–1583. [Google Scholar] [PubMed]
- Kashima, H.; Eguchi, E.; Miyamoto, K.; Fujimoto, M.; Endo, M.Y.; Aso-Someya, N.; Kobayashi, T.; Hayashi, N.; Fukuba, Y. Suppression of oral sweet taste sensation with Gymnema sylvestre affects postprandial gastrointestinal blood flow and gastric emptying in humans. Chem. Senses 2017, 42, 295–302. [Google Scholar] [CrossRef]
- Someya, N.; Endo, M.Y.; Fukuba, Y.; Hayashi, N. Blood flow responses in celiac and superior mesenteric arteries in the initial phase of digestion. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, R1790–R1796. [Google Scholar] [CrossRef]
- Islam, H.; Townsend, L.K.; McKie, G.L.; Medeiros, P.J.; Gurd, B.J.; Hazell, T.L. Potential involvement of lactate and interleukin-6 in the appetite-regulatory hormonal response to an acute exercise bout. J. Appl. Physiol. 2017, 123, 614–623. [Google Scholar] [CrossRef] [Green Version]
- Horner, K.M.; Schubert, M.M.; Desbrow, B.; Byrne, N.M.; King, N.A. Acute exercise and gastric emptying: A meta-analysis and implications for appetite control. Sports Med. 2015, 45, 659–678. [Google Scholar] [CrossRef]
- Evans, G.H.; Watson, P.; Shirreffs, S.M.; Maughan, R.J. The effect of exercise intensity on subsequent gastric emptying rate in humans. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Mattin, L.R.; Yau, A.M.W.; McIver, V.; James, L.J.; Evans, G.H. The effect of exercise intensity on gastric emptying rate, appetite and gut derived hormone responses after consuming a standardised semi-solid meal in healthy males. Nutrients 2018, 10, 787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marathe, C.S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. Relationships between gastric emptying, postprandial glycemia, and incretin hormones. Diabetes Care 2013, 36, 1396–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, I.M.; Feltrin, K.L.; Nair, N.S.; Hausken, T.; Little, T.J.; Gentilcore, D.; Wishart, J.M.; Jones, K.L.; Horowitz, M.; Feinle-Bisset, C. Effects of the phases of the menstrual cycle on gastric emptying, glycemia, plasma GLP-1 and insulin, and energy intake in healthy lean women. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G602–G610. [Google Scholar] [CrossRef] [Green Version]
- Hveem, K.; Jones, K.L.; Chatterton, B.E.; Horowitz, M. Scintigraphic measurement of gastric emptying and ultrasonographic assessment of antral area: Relation to appetite. Gut 1996, 38, 816–821. [Google Scholar] [CrossRef]
- Kruisselbrink, R.; Arzola, C.; Endersby, R.; Tse, C.; Chan, V.; Perlas, A. Intra-and interrater reliability of ultrasound assessment of gastric volume. Anesthesiology 2014, 121, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Borg, G.A. Perceived Exertion: A Note on ″History″ and Methods. Med. Sci. Sports 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Brown, N.W.; Ward, A.; Surwit, R.; Tiller, J.; Lightman, S.; Treasure, J.L.; Campbell, L.C. Evidence for metabolic and endocrine abnormalities in subjects recovered from anorexia nervosa. Metabolism 2003, 52, 296–302. [Google Scholar] [CrossRef]
- Vuguin, P.; Saenger, P.; Dimartino-Nardi, J. Fasting glucose insulin ratio: A useful measure of insulin resistance in girls with premature adrenarche. J. Clin. Endocrinol. Metab. 2001, 86, 4618–4621. [Google Scholar] [CrossRef]
- Silva, M.T.; Palheta-Junior, R.C.; Sousa, D.F.; Magalhães, P.F.A.; Okoba, W.; Campos, C.P.S.; Oliveira, R.B.; Magalhães, P.J.C.; Santos, A.A. Sodium bicarbonate treatment prevents gastric emptying delay caused by acute exercise in awake rats. J. Appl. Physiol. 2014, 116, 1133–1141. [Google Scholar] [CrossRef] [Green Version]
- Osada, T.; Iwane, H.; Katsumura, T.; Murase, N.; Higuchi, H.; Sakamoto, A.; Hamaoka, T.; Shimomitsu, T. Relationship between reduced lower abdominal blood flows and heart rate in recovery following cycling exercise. Acta. Physiol. 2012, 204, 344–353. [Google Scholar] [CrossRef]
- Sidery, M.B.; Macdonald, I.A.; Blackshaw, P.E. Superior mesenteric artery blood flow and gastric emptying in humans and the differential effects of high fat and high carbohydrate meals. Gut 1994, 35, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herd, J.A. Cardiovascular response to stress. Physiol. Rev. 1991, 71, 305–330. [Google Scholar] [CrossRef] [PubMed]
- Victor, R.G.; Leimbach, W.N., Jr.; Seals, D.R.; Wallin, B.G.; Mark, A.L. Effects of the cold pressor test on muscle sympathetic nerve activity in humans. Hypertension 1987, 9, 429–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fone, D.R.; Horowitz, M.; Maddox, A.; Akkermans, L.M.; Read, N.W.; Dent, J. Gastroduodenal motility during the delayed gastric emptying induced by cold stress. Gastroenterology 1990, 98, 1155–1161. [Google Scholar] [CrossRef]
- Roland, J.; Dobbeleir, A.; Vandevivere, J.; Ham, H.R. Effect of mild mental stress on solid phase gastric emptying in healthy subjects. Nucl. Med. Commun. 1990, 11, 319–326. [Google Scholar] [CrossRef]
- Geeraerts, B.; Vandenberghe, J.; Van Oudenhove, L.; Gregory, L.J.; Aziz, Q.; Dupont, P.; Demyttenaere, K.; Janssens, J.; Tack, J. Influence of experimentally induced anxiety on gastric sensorimotor function in humans. Gastroenterology 2005, 129, 1437–1444. [Google Scholar] [CrossRef]
- Kato, M.; Sakai, T.; Yabe, K.; Miyamura, M.; Soya, H. Gastric myoelectrical activity increases after moderate-intensity exercise with no meals under suppressed vagal nerve activity. Jpn. J. Physiol. 2004, 54, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Kondo, T.; Suzukamo, Y.; Oouchida, Y.; Izumi1, S.I. Vagal nerve regulation is essential for the increase in gastric motility in response to mild exercise. Tohoku J. Exp. Med. 2010, 222, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, K.; Sato, H.; Hori, M.; Kusuoka, H.; Ozaki, H.; Yokoyama, H.; Takeda, H.; Inoue, M.; Kamada, T. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J. Am. Coll. Cardiol. 1994, 24, 1529–1535. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, J.; Suzuki, H.; Masaoka, T.; Tanaka, K.; Mori, H.; Kanai, T. Influence of regular exercise on gastric emptying in healthy men: A pilot study. J. Clin. Biochem. Nutr. 2016, 59, 130–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubert, M.M.; Sabapathy, S.; Leveritt, M.; Desbrow, B. Acute exercise and hormones related to appetite regulation: A meta-analysis. Sports Med. 2014, 44, 387–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashima, H.; Kamimura, S.; Honma, A.; Endo, M.Y.; Miura, A.; Kobayashi, T.; Fukuba, Y. Timing of Nutrient Ingestion after Mild to Moderate Cycling Exercise Does Not Affect Gastric Emptying Rate in Humans. Nutrients 2020, 12, 2118. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072118
Kashima H, Kamimura S, Honma A, Endo MY, Miura A, Kobayashi T, Fukuba Y. Timing of Nutrient Ingestion after Mild to Moderate Cycling Exercise Does Not Affect Gastric Emptying Rate in Humans. Nutrients. 2020; 12(7):2118. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072118
Chicago/Turabian StyleKashima, Hideaki, Saori Kamimura, Ayumi Honma, Masako Yamaoka Endo, Akira Miura, Toshio Kobayashi, and Yoshiyuki Fukuba. 2020. "Timing of Nutrient Ingestion after Mild to Moderate Cycling Exercise Does Not Affect Gastric Emptying Rate in Humans" Nutrients 12, no. 7: 2118. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072118