Persistent Iron Deficiency Anemia in Patients with Celiac Disease Despite a Gluten-Free Diet

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
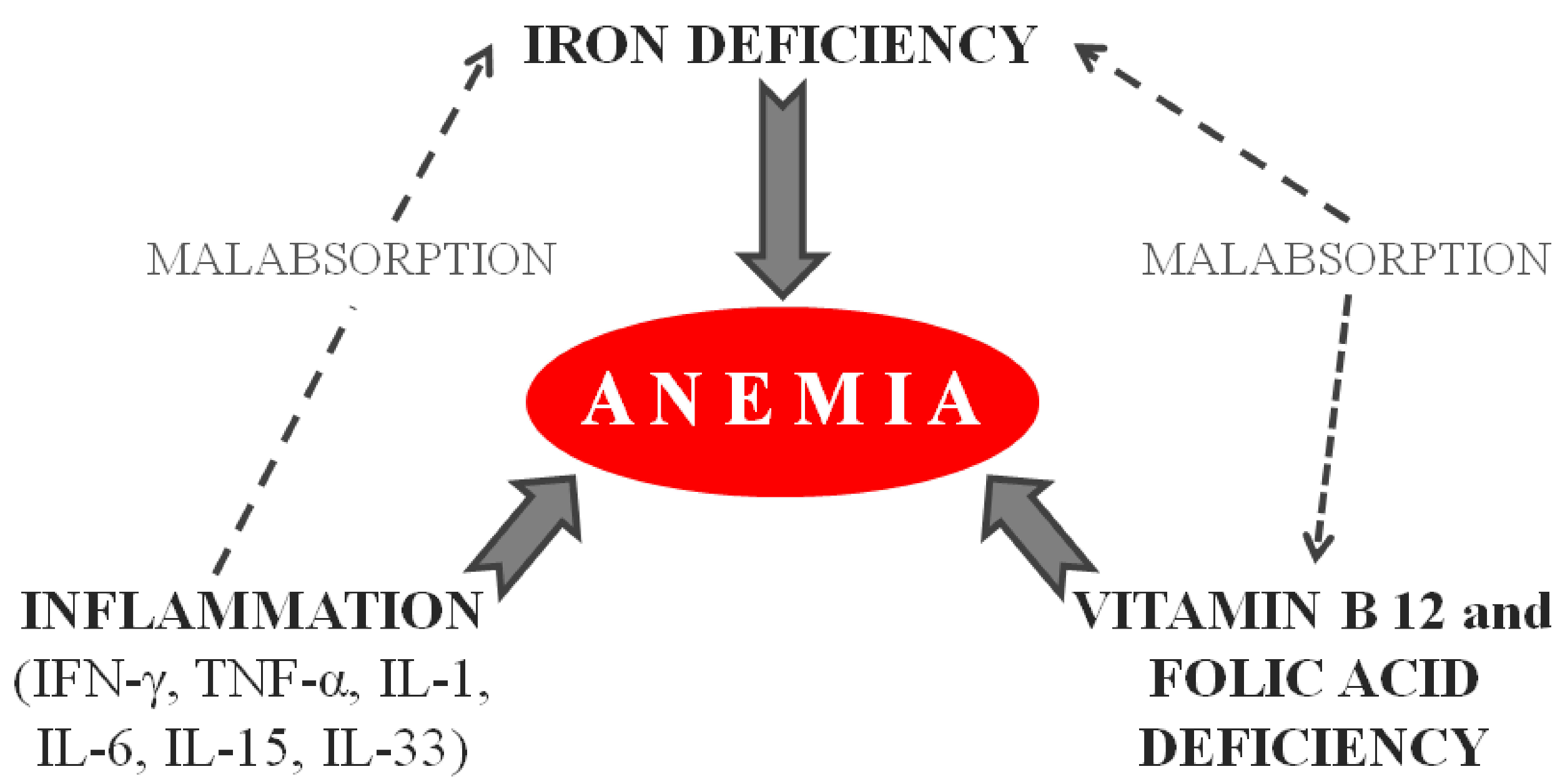
3.1. Iron Deficiency Anemia and Relationship with Clinical and Histological Features
3.2. Underlying Causes of IDA in Celiac Disease
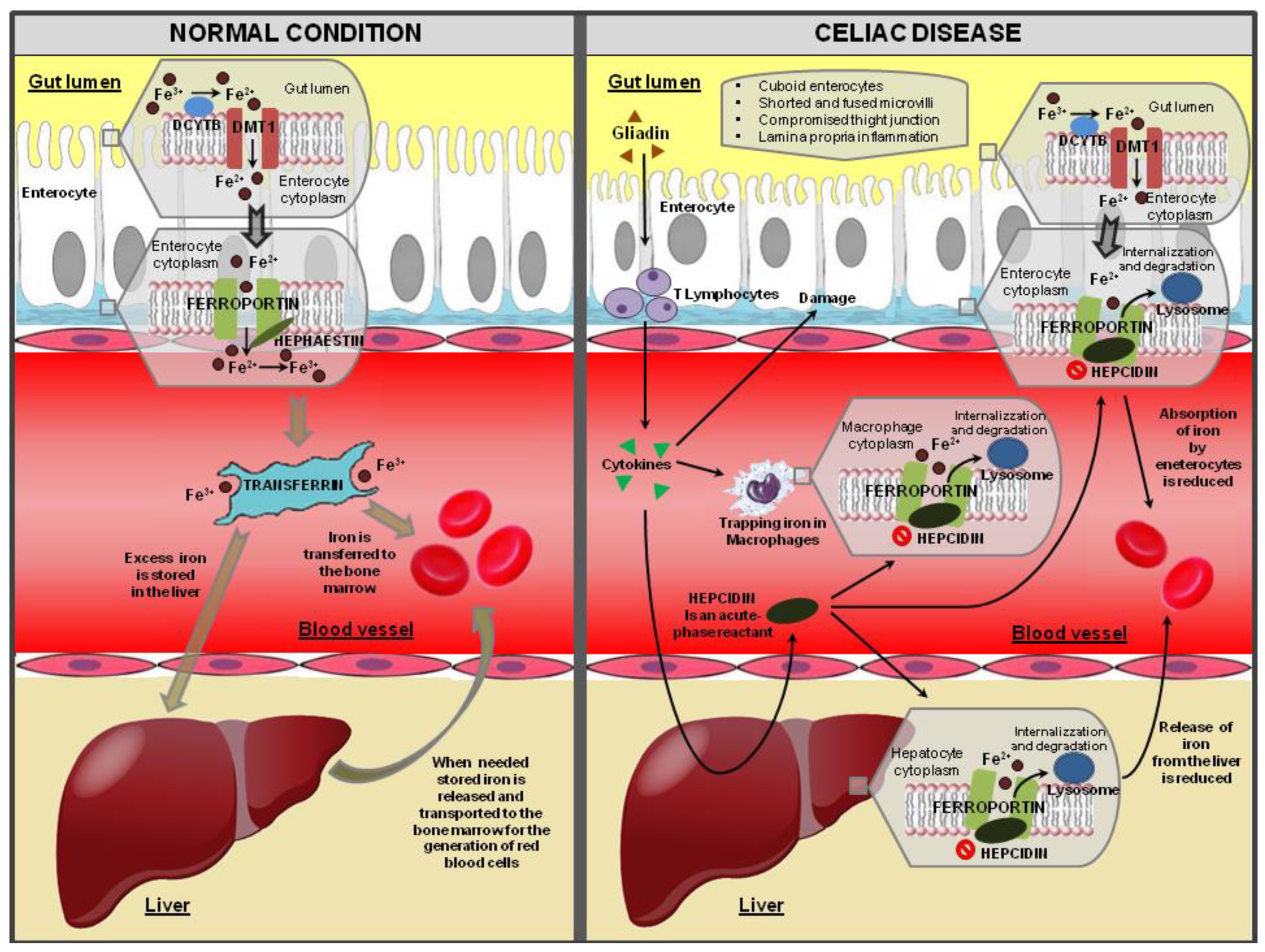
3.2.1. Iron Malabsorption
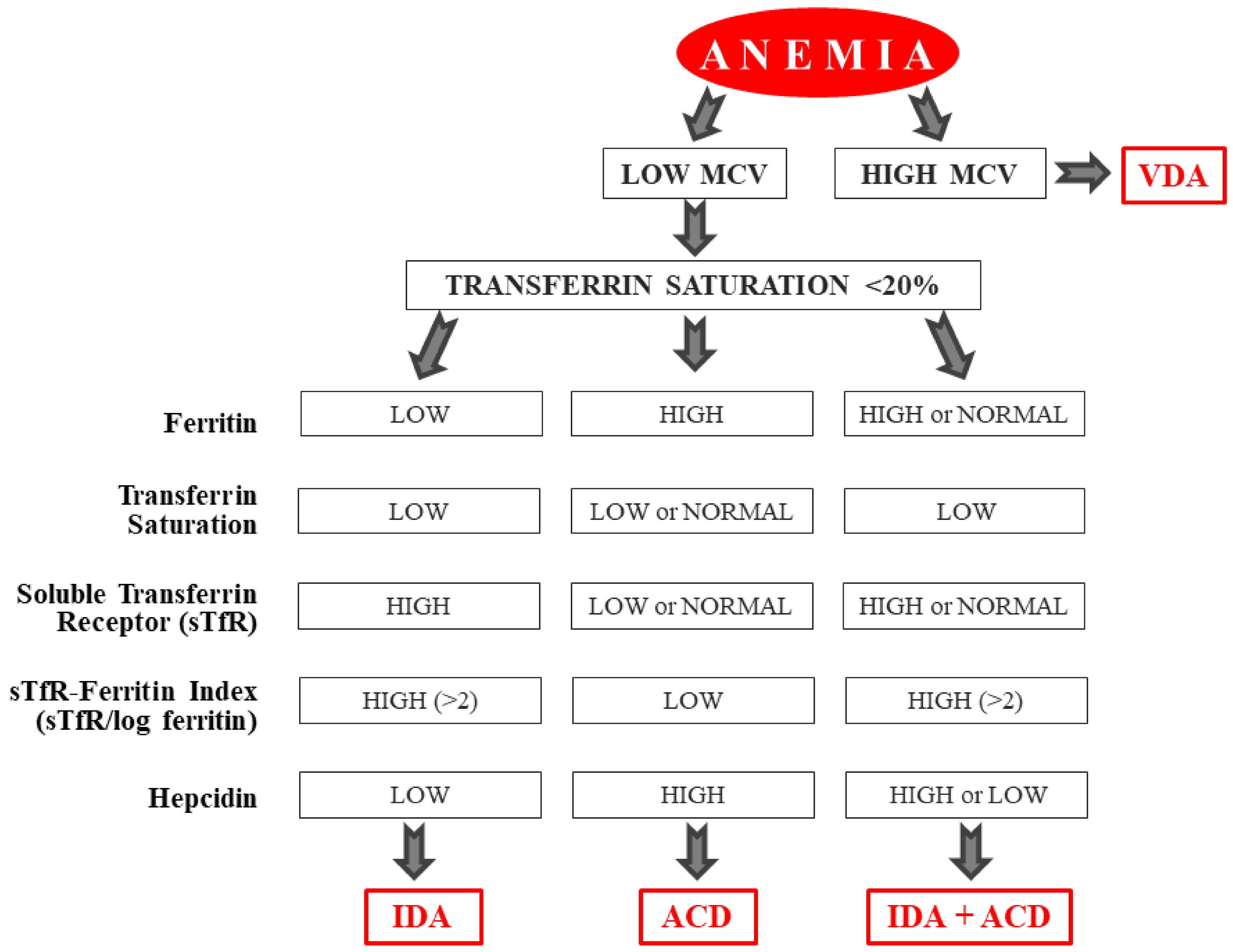
3.2.2. Chronic Inflammation
3.2.3. Other Causes of Iron Deficiency Anemia in Celiac Patients
3.3. Persistence of Anemia in Patients with CD Despite Adopting a GFD
3.3.1. Ultrastructural and Molecular Alterations of Enterocytes
3.3.2. Genetic factors
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CD | Celiac disease |
| IDA | Iron deficiency anemia |
| GFD | Gluten-free diet |
| IEL | Intraepithelial lymphocytosis |
| tTG | Anti-tissue-transglutaminase antibodies |
| EMA | Anti-endomysial antibodies |
| ACD | Anemia of chronic disease |
| IFN-y | Interferon-gamma |
| TNF-α | Tumor necrosis factor-α |
| IBD | Inflammatory bowel diseases |
| Fe3+ | Ferric form |
| Fe2+ | Ferrous form |
| DCYTB | Duodenal cytochrome B |
| DMT1 | Divalent metal transporter 1 |
| MTP 1 | Metal transporter 1 |
| MICA | Major histocompatibility complex class I-related chain A |
| NKG2D | Natural killer cell receptors |
| CRP | C-reactive protein |
| H. pylori | Helicobacter pylori |
| IELs | Intestinal intraepithelial lymphocytes |
| NCGS | Non-coeliac gluten sensitivity |
| FP1 | Ferroportin 1 |
| TfR1 | Transferrin receptor 1 |
| IRP | Iron regulatory protein |
| HFE | Hemochromatosis |
References
- Green, P.H.R.; Jabri, B. Coeliac disease. Lancet Lond. Engl. 2003, 362, 383–391. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.S.P.; Fountain, J.R. Incidence of the Sprue Syndrome. Br. Med. J. 1950, 1, 1157–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; deBruyn, J.; Ronksley, P.E.; Shaheen, A.-A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Goggins, M.; Kelleher, D. Celiac disease and other nutrient related injuries to the gastrointestinal tract. Am. J. Gastroenterol. 1994, 89, S2–S17. [Google Scholar] [PubMed]
- Kolho, K.L.; Färkkilä, M.A.; Savilahti, E. Undiagnosed coeliac disease is common in Finnish adults. Scand. J. Gastroenterol. 1998, 33, 1280–1283. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.R.; Mohammadkhani, A.; Fakheri, H.; Javad Zahedi, M.; Shahbazkhani, B.; Nouraie, M.; Sotoudeh, M.; Shakeri, R.; Malekzadeh, R. Screening of the adult population in Iran for coeliac disease: Comparison of the tissue-transglutaminase antibody and anti-endomysial antibody tests. Eur. J. Gastroenterol. Hepatol. 2006, 18, 1181–1186. [Google Scholar] [CrossRef]
- Martucci, S.; Biagi, F.; Di Sabatino, A.; Corazza, G.R. Coeliac disease. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2002, 34, S150–S153. [Google Scholar] [CrossRef]
- Biagi, F.; Corazza, G.R. Clinical features of coeliac disease. Dig. Liver Dis. 2002, 34, 225–228. [Google Scholar] [CrossRef]
- Leffler, D.A.; Green, P.H.R.; Fasano, A. Extraintestinal manifestations of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 561–571. [Google Scholar] [CrossRef]
- Halfdanarson, T.R.; Litzow, M.R.; Murray, J.A. Hematologic manifestations of celiac disease. Blood 2007, 109, 412–421. [Google Scholar] [CrossRef] [Green Version]
- Martín-Masot, R.; Nestares, M.T.; Diaz-Castro, J.; López-Aliaga, I.; Alférez, M.J.M.; Moreno-Fernandez, J.; Maldonado, J. Multifactorial Etiology of Anemia in Celiac Disease and Effect of Gluten-Free Diet: A Comprehensive Review. Nutrients 2019, 11, 2557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, H.J. Iron deficiency anemia in celiac disease. World J. Gastroenterol. 2015, 21, 9233–9238. [Google Scholar] [CrossRef] [PubMed]
- Unsworth, D.J.; Lock, R.J.; Harvey, R.F. Improving the diagnosis of coeliac disease in anaemic women. Br. J. Haematol. 2000, 111, 898–901. [Google Scholar] [PubMed]
- Brandimarte, G.; Tursi, A.; Giorgetti, G.M. Changing trends in clinical form of celiac disease. Which is now the main form of celiac disease in clinical practice? Minerva Gastroenterol. Dietol. 2002, 48, 121–130. [Google Scholar] [PubMed]
- Anand, B.S.; Callender, S.T.; Warner, G.T. Absorption of inorganic and haemoglobin iron in coeliac disease. Br. J. Haematol. 1977, 37, 409–414. [Google Scholar] [CrossRef]
- Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A.E.; Berkenpas, M.; Mulder, C.J.J.; van Bodegraven, A.A. Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients. Nutrients 2013, 5, 3975–3992. [Google Scholar] [CrossRef]
- García-Manzanares, A.; Lucendo, A.J. Nutritional and dietary aspects of celiac disease. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2011, 26, 163–173. [Google Scholar] [CrossRef]
- Dinler, G.; Atalay, E.; Kalayci, A.G. Celiac disease in 87 children with typical and atypical symptoms in Black Sea region of Turkey. World J. Pediatr. WJP 2009, 5, 282–286. [Google Scholar] [CrossRef]
- Kuloğlu, Z.; Kirsaçlioğlu, C.T.; Kansu, A.; Ensari, A.; Girgin, N. Celiac disease: Presentation of 109 children. Yonsei Med. J. 2009, 50, 617–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergamaschi, G.; Markopoulos, K.; Albertini, R.; Di Sabatino, A.; Biagi, F.; Ciccocioppo, R.; Arbustini, E.; Corazza, G.R. Anemia of chronic disease and defective erythropoietin production in patients with celiac disease. Haematologica 2008, 93, 1785–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergamaschi, G.; Di Sabatino, A.; Corazza, G.R. Pathogenesis, diagnosis and treatment of anaemia in immune-mediated gastrointestinal disorders. Br. J. Haematol. 2018, 182, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, N.; Basha, J.; Varma, N.; Varma, S.; Prasad, K.K.; Vaiphei, K.; Dhaka, N.; Sinha, S.K.; Kochhar, R. Anemia in celiac disease is multifactorial in etiology: A prospective study from India: Anemia in celiac disease. JGH Open 2018, 2, 196–200. [Google Scholar] [CrossRef]
- Weiss, G.; Goodnough, L.T. Anemia of chronic disease. N. Engl. J. Med. 2005, 352, 1011–1023. [Google Scholar] [CrossRef] [Green Version]
- Hershko, C.; Patz, J. Ironing out the mechanism of anemia in celiac disease. Haematologica 2008, 93, 1761–1765. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [Green Version]
- Ciccone, A.; Gabrieli, D.; Cardinale, R.; Di Ruscio, M.; Vernia, F.; Stefanelli, G.; Necozione, S.; Melideo, D.; Viscido, A.; Frieri, G.; et al. Metabolic Alterations in Celiac Disease Occurring after Following a Gluten-Free Diet. Digestion 2019, 100, 262–268. [Google Scholar] [CrossRef]
- Valvano, M.; Longo, S.; Stefanelli, G.; Frieri, G.; Viscido, A.; Latella, G. Celiac Disease, Gluten-Free Diet, and Metabolic and Liver Disorders. Nutrients 2020, 12, 940. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.D. Diagnosis and management of iron-deficiency anaemia. Best Pract. Res. Clin. Haematol. 2005, 18, 319–332. [Google Scholar] [CrossRef]
- Guagnozzi, D.; Severi, C.; Ialongo, P.; Viscido, A.; Patrizi, F.; Testino, G.; Vannella, L.; Labriola, R.; Strom, R.; Caprilli, R. Ferritin as a simple indicator of iron deficiency in anemic IBD patients. Inflamm. Bowel Dis. 2006, 12, 150–151. [Google Scholar] [CrossRef] [PubMed]
- Looker, A.C.; Dallman, P.R.; Carroll, M.D.; Gunter, E.W.; Johnson, C.L. Prevalence of iron deficiency in the United States. JAMA 1997, 277, 973–976. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Cello, J.P. Evaluation of the gastrointestinal tract in patients with iron-deficiency anemia. N. Engl. J. Med. 1993, 329, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- American Gastroenterological Association. American Gastroenterological Association medical position statement: Evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 2000, 118, 197–201. [Google Scholar] [CrossRef]
- Khatoon, S.; Ahmed, A.; Yousaf, S. Iron Deficiency Anaemia In Pakistan: Celiac Disease An Underlying Cause. J. Ayub Med. Coll. Abbottabad JAMC 2018, 30, 372–376. [Google Scholar]
- Shahriari, M.; Honar, N.; Yousefi, A.; Javaherizadeh, H. Association of potential celiac disease and refractory iron deficiency anemia in children and adolescents. Arq. Gastroenterol. 2018, 55, 78–81. [Google Scholar] [CrossRef] [Green Version]
- Binicier, O.B.; Tosun, F. Evaluation of adult celiac disease from a tertiary reference center: A retrospective analysis. Rev. Assoc. Medica Bras. 2020, 66, 55–60. [Google Scholar] [CrossRef]
- Bottaro, G.; Cataldo, F.; Rotolo, N.; Spina, M.; Corazza, G.R. The clinical pattern of subclinical/silent celiac disease: An analysis on 1026 consecutive cases. Am. J. Gastroenterol. 1999, 94, 691–696. [Google Scholar] [CrossRef]
- Abu Daya, H.; Lebwohl, B.; Lewis, S.K.; Green, P.H. Celiac disease patients presenting with anemia have more severe disease than those presenting with diarrhea. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2013, 11, 1472–1477. [Google Scholar] [CrossRef]
- Sansotta, N.; Amirikian, K.; Guandalini, S.; Jericho, H. Celiac Disease Symptom Resolution: Effectiveness of the Gluten-free Diet. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 48–52. [Google Scholar] [CrossRef]
- Tolone, C.; Bellini, G.; Punzo, F.; Papparella, A.; Miele, E.; Vitale, A.; Nobili, B.; Strisciuglio, C.; Rossi, F. The DMT1 IVS4+44C>A polymorphism and the risk of iron deficiency anemia in children with celiac disease. PLoS ONE 2017, 12, e0185822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Falco, L.; Tortora, R.; Imperatore, N.; Bruno, M.; Capasso, M.; Girelli, D.; Castagna, A.; Caporaso, N.; Iolascon, A.; Rispo, A. The role of TMPRSS6 and HFE variants in iron deficiency anemia in celiac disease. Am. J. Hematol. 2018, 93, 383–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffbrand, A.V. Anaemia in adult coeliac disease. Clin. Gastroenterol. 1974, 3, 71–89. [Google Scholar] [PubMed]
- Gabrieli, D.; Ciccone, F.; Capannolo, A.; Viscido, A.; Valerii, G.; Serva, D.; Necozione, S.; Coletti, G.; Calvisi, G.; Melideo, D.; et al. Subtypes of chronic gastritis in patients with celiac disease before and after gluten-free diet. United Eur. Gastroenterol. J. 2017, 5, 805–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saukkonen, J.; Kaukinen, K.; Koivisto, A.-M.; Mäki, M.; Laurila, K.; Sievänen, H.; Collin, P.; Kurppa, K. Clinical Characteristics and the Dietary Response in Celiac Disease Patients Presenting With or Without Anemia. J. Clin. Gastroenterol. 2017, 51, 412–416. [Google Scholar] [CrossRef]
- Nurminen, S.; Kivelä, L.; Huhtala, H.; Kaukinen, K.; Kurppa, K. Extraintestinal manifestations were common in children with coeliac disease and were more prevalent in patients with more severe clinical and histological presentation. Acta Paediatr. 2019, 108, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Bhadada, S.K.; Rastogi, A.; Agarwal, A.; Kochhar, R.; Kochhar, R.; Bhansali, A. Comparative study of clinical features of patients with celiac disease & those with concurrent celiac disease & type 1 diabetes mellitus. Indian J. Med. Res. 2017, 145, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Harper, J.W.; Holleran, S.F.; Ramakrishnan, R.; Bhagat, G.; Green, P.H.R. Anemia in celiac disease is multifactorial in etiology. Am. J. Hematol. 2007, 82, 996–1000. [Google Scholar] [CrossRef]
- Annibale, B.; Severi, C.; Chistolini, A.; Antonelli, G.; Lahner, E.; Marcheggiano, A.; Iannoni, C.; Monarca, B.; Delle Fave, G. Efficacy of gluten-free diet alone on recovery from iron deficiency anemia in adult celiac patients. Am. J. Gastroenterol. 2001, 96, 132–137. [Google Scholar] [CrossRef]
- Repo, M.; Lindfors, K.; Mäki, M.; Huhtala, H.; Laurila, K.; Lähdeaho, M.-L.; Saavalainen, P.; Kaukinen, K.; Kurppa, K. Anemia and Iron Deficiency in Children With Potential Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Efthymakis, K.; Milano, A.; Laterza, F.; Serio, M.; Neri, M. Iron deficiency anemia despite effective gluten-free diet in celiac disease: Diagnostic role of small bowel capsule endoscopy. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2017, 49, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Feruś, K.; Drabińska, N.; Krupa-Kozak, U.; Jarocka-Cyrta, E. A Randomized, Placebo-Controlled, Pilot Clinical Trial to Evaluate the Effect of Supplementation with Prebiotic Synergy 1 on Iron Homeostasis in Children and Adolescents with Celiac Disease Treated with a Gluten-Free Diet. Nutrients 2018, 10, 1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantopoulos, K.; Porwal, S.K.; Tartakoff, A.; Devireddy, L. Mechanisms of mammalian iron homeostasis. Biochemistry 2012, 51, 5705–5724. [Google Scholar] [CrossRef] [PubMed]
- Illing, A.C.; Shawki, A.; Cunningham, C.L.; Mackenzie, B. Substrate profile and metal-ion selectivity of human divalent metal-ion transporter-1. J. Biol. Chem. 2012, 287, 30485–30496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLoughery, T.G. Microcytic anemia. N. Engl. J. Med. 2014, 371, 1324–1331. [Google Scholar] [CrossRef]
- Ganz, T. Hepcidin and iron regulation, 10 years later. Blood 2011, 117, 4425–4433. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Tuttle, M.S.; Powelson, J.; Vaughn, M.B.; Donovan, A.; Ward, D.M.; Ganz, T.; Kaplan, J. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science 2004, 306, 2090–2093. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG Clinical Guidelines: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [Green Version]
- Hüe, S.; Mention, J.-J.; Monteiro, R.C.; Zhang, S.; Cellier, C.; Schmitz, J.; Verkarre, V.; Fodil, N.; Bahram, S.; Cerf-Bensussan, N.; et al. A direct role for NKG2D/MICA interaction in villous atrophy during celiac disease. Immunity 2004, 21, 367–377. [Google Scholar] [CrossRef] [Green Version]
- Weiss, G.; Gasche, C. Pathogenesis and treatment of anemia in inflammatory bowel disease. Haematologica 2010, 95, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Ganz, T.; Nemeth, E. Hepcidin and disorders of iron metabolism. Annu. Rev. Med. 2011, 62, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, E.M.; Jahnsen, F.L.; Lundin, K.E.; Johansen, F.E.; Fausa, O.; Sollid, L.M.; Jahnsen, J.; Scott, H.; Brandtzaeg, P. Gluten induces an intestinal cytokine response strongly dominated by interferon gamma in patients with celiac disease. Gastroenterology 1998, 115, 551–563. [Google Scholar] [CrossRef]
- Ciccocioppo, R.; Di Sabatino, A.; Bauer, M.; Della Riccia, D.N.; Bizzini, F.; Biagi, F.; Cifone, M.G.; Corazza, G.R.; Schuppan, D. Matrix metalloproteinase pattern in celiac duodenal mucosa. Lab. Investig. J. Tech. Methods Pathol. 2005, 85, 397–407. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Ciccocioppo, R.; Cupelli, F.; Cinque, B.; Millimaggi, D.; Clarkson, M.M.; Paulli, M.; Cifone, M.G.; Corazza, G.R. Epithelium derived interleukin 15 regulates intraepithelial lymphocyte Th1 cytokine production, cytotoxicity, and survival in coeliac disease. Gut 2006, 55, 469–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.Q.; Udupa, K.B.; Lipschitz, D.A. Interferon-gamma exerts its negative regulatory effect primarily on the earliest stages of murine erythroid progenitor cell development. J. Cell. Physiol. 1995, 162, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Ludwiczek, S.; Aigner, E.; Theurl, I.; Weiss, G. Cytokine-mediated regulation of iron transport in human monocytic cells. Blood 2003, 101, 4148–4154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullarky, I.K.; Szaba, F.M.; Kummer, L.W.; Wilhelm, L.B.; Parent, M.A.; Johnson, L.L.; Smiley, S.T. Gamma interferon suppresses erythropoiesis via interleukin-15. Infect. Immun. 2007, 75, 2630–2633. [Google Scholar] [CrossRef] [Green Version]
- Benahmed, M.; Meresse, B.; Arnulf, B.; Barbe, U.; Mention, J.-J.; Verkarre, V.; Allez, M.; Cellier, C.; Hermine, O.; Cerf–Bensussan, N. Inhibition of TGF-β Signaling by IL-15: A New Role for IL-15 in the Loss of Immune Homeostasis in Celiac Disease. Gastroenterology 2007, 132, 994–1008. [Google Scholar] [CrossRef]
- Hershko, C.; Camaschella, C. How I treat unexplained refractory iron deficiency anemia. Blood 2014, 123, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Rostami-Nejad, M.; Villanacci, V.; Mashayakhi, R.; Molaei, M.; Bassotti, G.; Zojaji, H.; Mirstatari, D.; Rostami, K.; Zali, M.R. Celiac disease and Hp infection association in Iran. Rev. Espanola Enfermedades Dig. Organo Of. Soc. Espanola Patol. Dig. 2009, 101, 850–854. [Google Scholar] [CrossRef] [Green Version]
- Hershko, C.; Hoffbrand, A.V.; Keret, D.; Souroujon, M.; Maschler, I.; Monselise, Y.; Lahad, A. Role of autoimmune gastritis, Helicobacter pylori and celiac disease in refractory or unexplained iron deficiency anemia. Haematologica 2005, 90, 585–595. [Google Scholar] [PubMed]
- Cuoco, L.; Cammarota, G.; Jorizzo, R.A.; Santarelli, L.; Cianci, R.; Montalto, M.; Gasbarrini, A.; Gasbarrini, G. Link between Helicobacter pylori infection and iron-deficiency anaemia in patients with coeliac disease. Scand. J. Gastroenterol. 2001, 36, 1284–1288. [Google Scholar] [CrossRef] [PubMed]
- Demir, H.; Saltik, I.N.; Yüce, A.; Ozen, H.; Gürakan, F.; Koçak, N. Is there any relation between Helicobacter pylori infection and iron deficiency anemia in children with celiac disease? Helicobacter 2004, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Simondi, D.; Ribaldone, D.G.; Bonagura, G.A.; Foi, S.; Sapone, N.; Garavagno, M.; Villanacci, V.; Bernardi, D.; Pellicano, R.; Rizzetto, M.; et al. Helicobacter pylori in celiac disease and in duodenal intraepithelial lymphocytosis: Active protagonist or innocent bystander? Clin. Res. Hepatol. Gastroenterol. 2015, 39, 740–745. [Google Scholar] [CrossRef]
- Rostami-Nejad, M.; Aldulaimi, D.; Livett, H.; Rostami, K. H. pylori associated with iron deficiency anemia even in celiac disease patients; strongly evidence based but weakly reflected in practice. Gastroenterol. Hepatol. Bed Bench 2015, 8, 178–182. [Google Scholar]
- Samasca, G.; Deleanu, D.; Sur, G.; Lupan, I.; Giulia, A.; Carpa, R. Is it necessary to screen Helicobacter pylori infection in patients with celiac disease and iron deficiency? Gastroenterol. Hepatol. Bed Bench 2016, 9, 345. [Google Scholar]
- Franceschi, F.; Zuccalà, G.; Roccarina, D.; Gasbarrini, A. Clinical effects of Helicobacter pylori outside the stomach. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 234–242. [Google Scholar] [CrossRef]
- Dickey, W.; Kenny, B.D.; McMillan, S.A.; Porter, K.G.; McConnell, J.B. Gastric as well as duodenal biopsies may be useful in the investigation of iron deficiency anaemia. Scand. J. Gastroenterol. 1997, 32, 469–472. [Google Scholar] [CrossRef]
- Muhsen, K.; Cohen, D. Helicobacter pylori infection and iron stores: A systematic review and meta-analysis. Helicobacter 2008, 13, 323–340. [Google Scholar] [CrossRef]
- Yuan, W.; Li, Y.; Yang, K.; Ma, B.; Guan, Q.; Wang, D.; Yang, L. Iron deficiency anemia in Helicobacter pylori infection: Meta-analysis of randomized controlled trials. Scand. J. Gastroenterol. 2010, 45, 665–676. [Google Scholar] [CrossRef]
- Emiralioglu, N.; Yenicesu, I.; Sari, S.; Egritas, O.; Poyraz, A.; Pasaoglu, O.T.; Celik, B.; Dalgic, B. An insight into the relationships between prohepcidin, iron deficiency anemia, and interleukin-6 values in pediatric Helicobacter pylori gastritis. Eur. J. Pediatr. 2015, 174, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Yoneyama, O.; Azumaya, M.; Takeuchi, M.; Sasaki, S.; Yokoyama, J.; Shioji, K.; Kawauchi, Y.; Hashimoto, S.; Nishigaki, Y.; et al. The relationship between iron deficiency in patients with Helicobacter pylori-infected nodular gastritis and the serum prohepcidin level. Helicobacter 2015, 20, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Azab, S.F.A.; Esh, A.M.H. Serum hepcidin levels in Helicobacter pylori-infected children with iron-deficiency anemia: A case-control study. Ann. Hematol. 2013, 92, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Sirufo, M.M.; Viscido, A.; Ginaldi, L. Food Allergies and Ageing. Int. J. Mol. Sci. 2019, 20, 5580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worst, D.J.; Otto, B.R.; de Graaff, J. Iron-repressible outer membrane proteins of Helicobacter pylori involved in heme uptake. Infect. Immun. 1995, 63, 4161–4165. [Google Scholar] [CrossRef] [Green Version]
- Kirschner, D.E.; Blaser, M.J. The dynamics of Helicobacter pylori infection of the human stomach. J. Theor. Biol. 1995, 176, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Pallav, K.; Leffler, D.A.; Tariq, S.; Kabbani, T.; Hansen, J.; Peer, A.; Bhansali, A.; Najarian, R.; Kelly, C.P. Noncoeliac enteropathy: The differential diagnosis of villous atrophy in contemporary clinical practice. Aliment. Pharmacol. Ther. 2012, 35, 380–390. [Google Scholar] [CrossRef]
- Capannolo, A.; Necozione, S.; Gabrieli, D.; Ciccone, F.; Sollima, L.; Melchiorri, L.; Viscido, A.; Frieri, G. Duodenal lymphocytosis in functional dyspepsia. Arab J. Gastroenterol. Off. Publ. Pan-Arab Assoc. Gastroenterol. 2019, 20, 91–94. [Google Scholar] [CrossRef]
- Koot, B.G.P.; ten Kate, F.J.W.; Juffrie, M.; Rosalina, I.; Taminiau, J.J.A.M.; Benninga, M.A. Does Giardia lamblia cause villous atrophy in children? A retrospective cohort study of the histological abnormalities in giardiasis. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 304–308. [Google Scholar] [CrossRef]
- Oberhuber, G.; Kastner, N.; Stolte, M. Giardiasis: A histologic analysis of 567 cases. Scand. J. Gastroenterol. 1997, 32, 48–51. [Google Scholar] [CrossRef]
- Granito, A.; Muratori, L.; Muratori, P.; Petrolini, N.; Bianchi, F.B.; Volta, U. Antitransglutaminase antibodies and giardiasis. Am. J. Gastroenterol. 2004, 99, 2505–2506. [Google Scholar] [CrossRef] [PubMed]
- Isaac-Renton, J.; Blatherwick, J.; Bowie, W.R.; Fyfe, M.; Khan, M.; Li, A.; King, A.; McLean, M.; Medd, L.; Moorehead, W.; et al. Epidemic and endemic seroprevalence of antibodies to Cryptosporidium and Giardia in residents of three communities with different drinking water supplies. Am. J. Trop. Med. Hyg. 1999, 60, 578–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenling, R.; Fredrikzon, B.; Engberg, S.; Falkmer, S. Surface infrastructure of the Small Intestine Mucosa in Children with Celiac Disease. I. Untreated Disease and Effects of Long-Term Gluten Elimination and Challenge. Ultrastruct. Pathol. 1984, 6, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Dyduch, A.; Karczewska, K.; Grzybek, H.; Kaminski, M. Transmission Electron Microscopy of Microvilli of Intestinal Epithelial Cells in Celiac Disease in Remission and Transient Gluten Enteropathy in Children After a Gluten-Free Diet. J. Pediatr. Gastroenterol. Nutr. 1993, 16, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Magliocca, F.M.; Bonamico, M.; Petrozza, V.; Correr, S.; Montuori, M.; Triglione, P.; Carpino, F. Scanning electron microscopy of the small intestine during gluten-challenge in celiac disease. Arch. Histol. Cytol. 1992, 55, 125–130. [Google Scholar] [CrossRef]
- Capannolo, A.; Viscido, A.; Barkad, M.A.; Valerii, G.; Ciccone, F.; Melideo, D.; Frieri, G.; Latella, G. Non-Celiac Gluten Sensitivity among Patients Perceiving Gluten-Related Symptoms. Digestion 2015, 92, 8–13. [Google Scholar] [CrossRef]
- Volta, U.; Bardella, M.T.; Calabrò, A.; Troncone, R.; Corazza, G.R.; The Study Group for Non-Celiac Gluten Sensitivity. An Italian prospective multicenter survey on patients suspected of having non-celiac gluten sensitivity. BMC Med. 2014, 12, 85. [Google Scholar] [CrossRef] [Green Version]
- Catassi, C. Gluten Sensitivity. Ann. Nutr. Metab. 2015, 67, 15–26. [Google Scholar] [CrossRef]
- Sbarbati, A.; Valletta, E.; Bertini, M.; Cipolli, M.; Morroni, M.; Pinelli, L.; Tatò, L. Gluten sensitivity and ‘normal’ histology: Is the intestinal mucosa really normal? Dig. Liver Dis. 2003, 35, 768–773. [Google Scholar] [CrossRef]
- Barbaro, M.R.; Cremon, C.; Morselli-Labate, A.M.; Di Sabatino, A.; Giuffrida, P.; Corazza, G.R.; Di Stefano, M.; Caio, G.; Latella, G.; Ciacci, C.; et al. Serum zonulin and its diagnostic performance in non-coeliac gluten sensitivity. Gut 2020. [Google Scholar] [CrossRef]
- Barisani, D.; Parafioriti, A.; Bardella, M.T.; Zoller, H.; Conte, D.; Armiraglio, E.; Trovato, C.; Koch, R.O.; Weiss, G. Adaptive changes of duodenal iron transport proteins in celiac disease. Physiol. Genom. 2004, 17, 316–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Begum, J.; Eksteen, B.; Elagib, A.; Brookes, M.; Cooper, B.T.; Tselepis, C.; Iqbal, T.H. Differential ferritin expression is associated with iron deficiency in coeliac disease. Eur. J. Gastroenterol. Hepatol. 2009, 21, 794–804. [Google Scholar] [CrossRef]
- Barisani, D.; Ceroni, S.; Del Bianco, S.; Meneveri, R.; Bardella, M.T. Hemochromatosis gene mutations and iron metabolism in celiac disease. Haematologica 2004, 89, 1299–1305. [Google Scholar]
- Elli, L.; Poggiali, E.; Tomba, C.; Andreozzi, F.; Nava, I.; Bardella, M.T.; Campostrini, N.; Girelli, D.; Conte, D.; Cappellini, M.D. Does TMPRSS6 RS855791 polymorphism contribute to iron deficiency in treated celiac disease? Am. J. Gastroenterol. 2015, 110, 200–202. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Onken, J.E. Improved Hemoglobin Response with Ferric Carboxymaltose in Patients with Gastrointestinal-Related Iron-Deficiency Anemia Versus Oral Iron. Dig. Dis. Sci. 2018, 63, 3009–3019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giancotti, L.; Talarico, V.; Mazza, G.A.; Marrazzo, S.; Gangemi, P.; Miniero, R.; Bertini, M. FeralgineTM a New Approach for Iron Deficiency Anemia in Celiac Patients. Nutrients 2019, 11, 887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elli, L.; Ferretti, F.; Branchi, F.; Tomba, C.; Lombardo, V.; Scricciolo, A.; Doneda, L.; Roncoroni, L. Sucrosomial Iron Supplementation in Anemic Patients with Celiac Disease Not Tolerating Oral Ferrous Sulfate: A Prospective Study. Nutrients 2018, 10, 330. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Adults Patients | |||||||
| Study (Year) | Study Location | Study Design | Number of CD Patients | Men N.(%) | Follow-up | CD patients with IDA before the start of a GFD N. (%) | CD patients with IDA after the start of a GFD (%) |
| Kolho et al. (1998) [7] | Finland | Cross-sectional | 8 | 1 (13) | n.a. | 2 (25) | n.a. |
| Akbari et al. (2006) [8] | Iran | Cross-sectional | 27 | 14 (52) | n.a. | 14 (52) | n.a. |
| Bergamaschi et al. (2008) [22] | Italy | Prospective Cohort | 132 | 47 (36) | 12 months | 45 (34) | n.a. |
| Berry et al. (2018) ** [24] | India | Prospective cohort | 103 | 48 (47) | n.a. | 84 (82) | n.a. |
| Binicier et al. (2020) [37] | Turkey | Retrospective Cohort | 195 | 44 (23) | 58 months * | 104 (53) | n.a. |
| Bottaro et al. (1999) [38] | Italy | Cross-sectional | 313 | n.a. | n.a. | 145 (46) | n.a. |
| Abu Daya et al. (2013) [39] | USA | Cross-sectional | 727 | 203 (28) | n.a. | 152 (21) | n.a. |
| Sansotta et al. (2018) [40] | USA | Retrospective Cohort | 327 | n.a. | 24 months * | 157 (48) | (15) |
| De Falco et al. (2018) [42] | Italy | Prospective Cohort | 505 | 106(21) | 12 months | 229 (45) | (21) |
| Pediatric Patients | |||||||
| Study (Year) | Study Location | Study Design | Number of CD Patients | Men N.(%) | Follow-up | CD patients with IDA before the start of a GFD N. (%) | CD patients with IDA after the start of a GFD (%) |
| Bottaro et al. (1999) [38] | Italy | Cross-sectional | 485 | n.a. | n.a. | 169 (35) | n.a. |
| Sansotta et al. (2018) [40] | USA | Retrospective Cohort | 227 | n.a. | 31 months * | 27 (12) | (16) |
| Tolone et al. (2017) [41] | Italy | Cross-sectional | 387 | 152 (39) | 84 months | 134 (35) | n.a. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanelli, G.; Viscido, A.; Longo, S.; Magistroni, M.; Latella, G. Persistent Iron Deficiency Anemia in Patients with Celiac Disease Despite a Gluten-Free Diet. Nutrients 2020, 12, 2176. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082176
Stefanelli G, Viscido A, Longo S, Magistroni M, Latella G. Persistent Iron Deficiency Anemia in Patients with Celiac Disease Despite a Gluten-Free Diet. Nutrients. 2020; 12(8):2176. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082176
Chicago/Turabian StyleStefanelli, Gianpiero, Angelo Viscido, Salvatore Longo, Marco Magistroni, and Giovanni Latella. 2020. "Persistent Iron Deficiency Anemia in Patients with Celiac Disease Despite a Gluten-Free Diet" Nutrients 12, no. 8: 2176. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082176