The Effect of Acute Hypohydration on Indicators of Glycemic Regulation, Appetite, Metabolism and Stress: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
1.1. Glycemic Regulation
1.2. Appetite
1.3. Stress
1.4. Metabolism
1.5. Mode of Dehydration
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Screening and Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
2.6. Data Analysis
3. Results
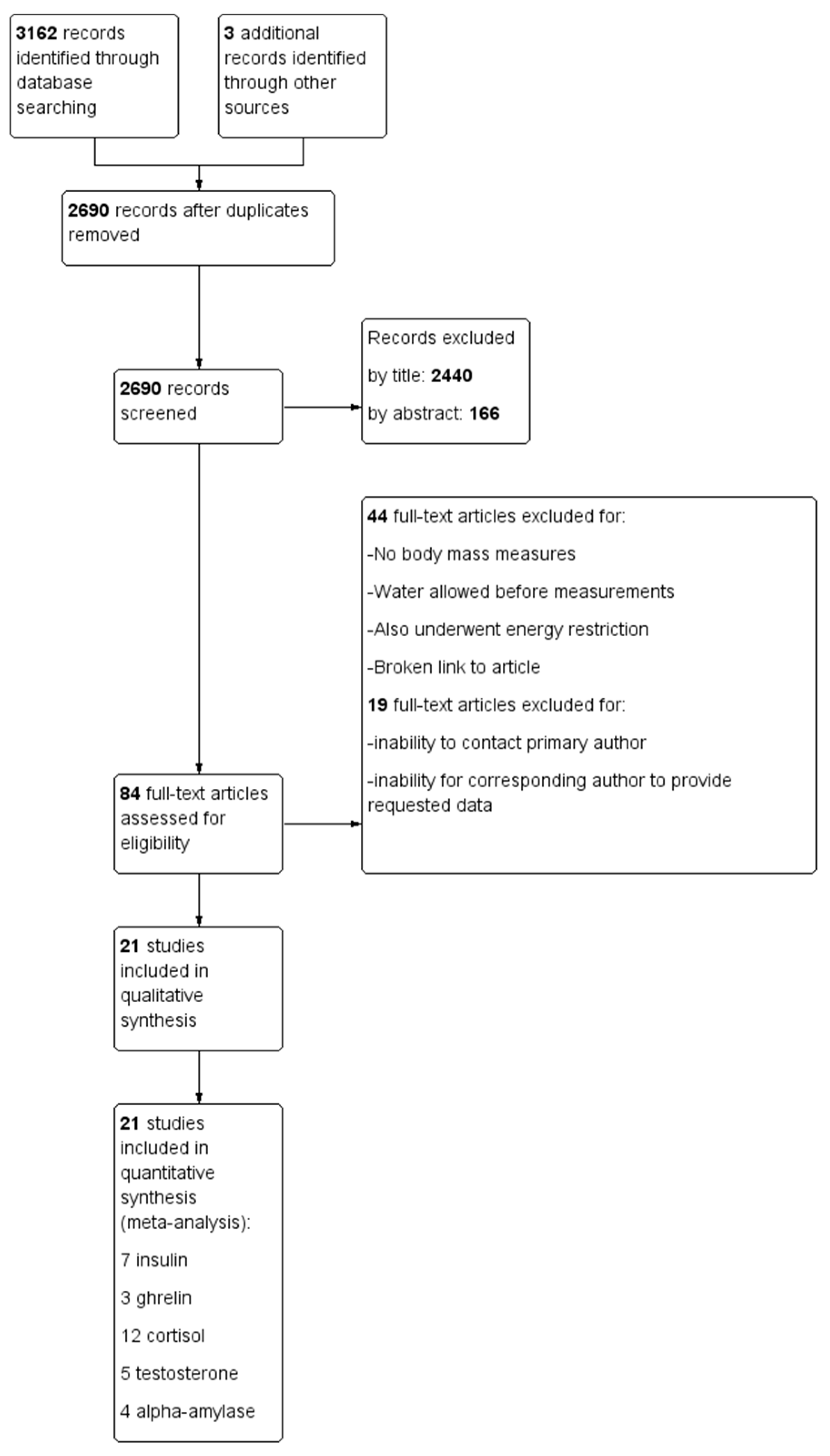
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Effect of Hypohydration on Selected Hormonal Responses
3.4.1. Effect of Hypohydration on Hormones Involved in Glycemic Regulation
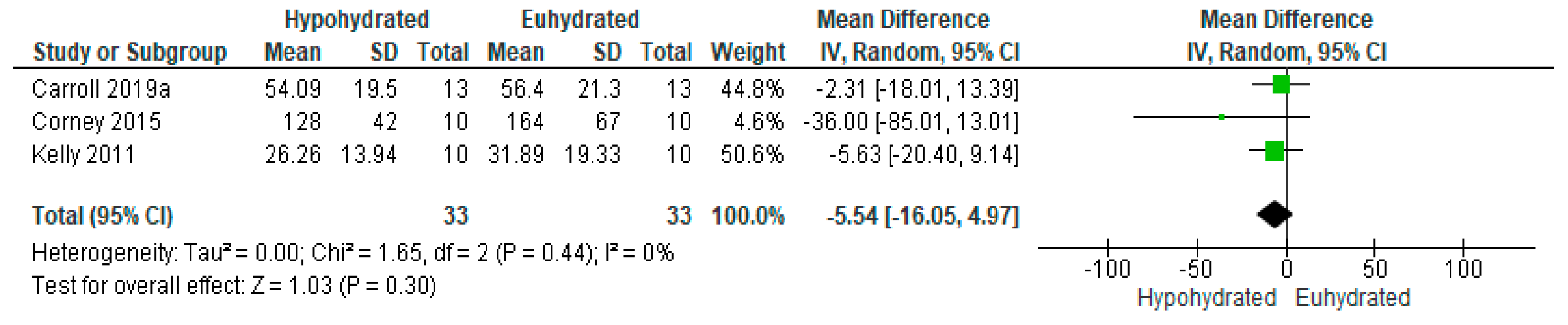
3.4.2. Effect of Hypohydration on Appetite Regulatory Hormones
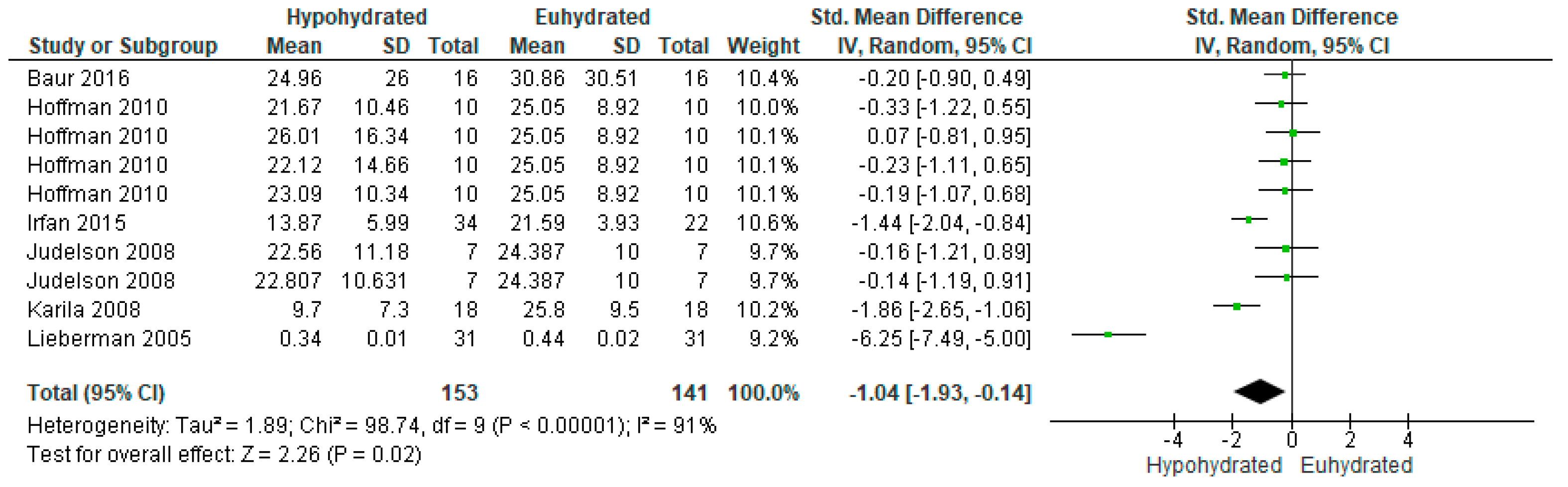
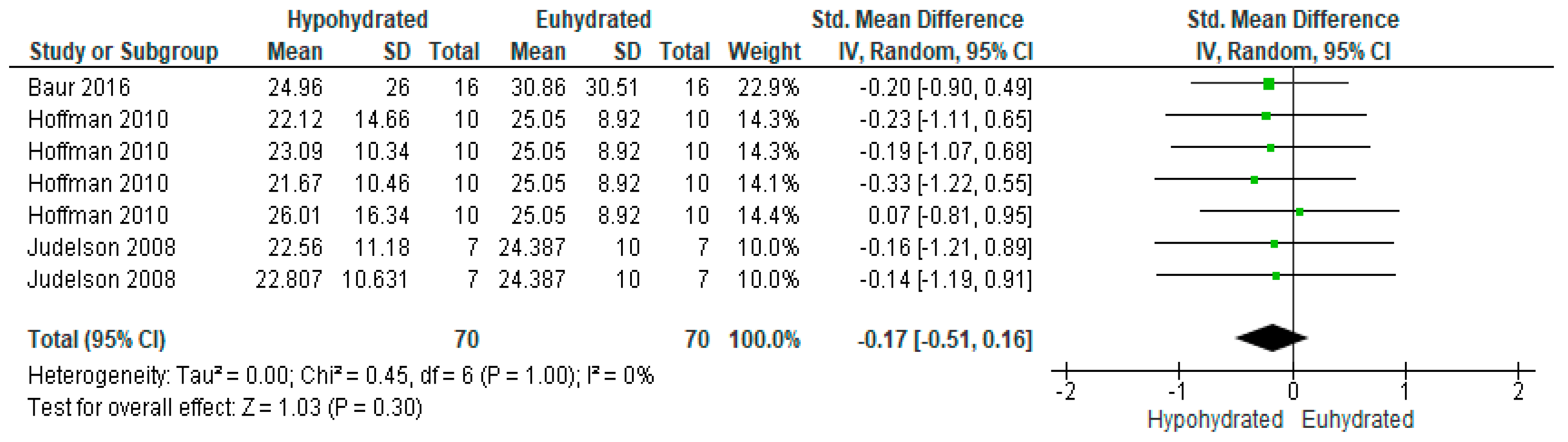
3.4.3. Effect of Hypohydration on Markers of Metabolism and Stress
4. Discussion
4.1. Glycemic Regulation
4.2. Appetite
4.3. Metabolism and Stress
4.4. Influence of the Method to Reduce Total Body Water
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- James, L.J.; Funnell, M.P.; James, R.M.; Mears, S.A. Does Hypohydration Really Impair Endurance Performance? Methodological Considerations for Interpreting Hydration Research. Sports Med. Auckl. N. Z. 2019, 49, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, assessment, and performance effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Kenefick, R.W.; Montain, S.J.; Sawka, M.N. Mechanisms of aerobic performance impairment with heat stress and dehydration. J. Appl. Physiol. 2010, 109, 1989–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savoie, F.-A.; Kenefick, R.W.; Ely, B.R.; Cheuvront, S.N.; Goulet, E.D.B. Effect of Hypohydration on Muscle Endurance, Strength, Anaerobic Power and Capacity and Vertical Jumping Ability: A Meta-Analysis. Sports Med. 2015, 45, 1207–1227. [Google Scholar] [CrossRef]
- Judelson, D.A.; Maresh, C.M.; Farrell, M.J.; Yamamoto, L.M.; Armstrong, L.E.; Kraemer, W.J.; Volek, J.S.; Spiering, B.A.; Casa, D.J.; Anderson, J.M. Effect of hydration state on strength, power, and resistance exercise performance. Med. Sci. Sports Exerc. 2007, 39, 1817–1824. [Google Scholar] [CrossRef]
- Judelson, D.A.; Maresh, C.M.; Anderson, J.M.; Armstrong, L.E.; Casa, D.J.; Kraemer, W.J.; Volek, J.S. Hydration and muscular performance: Does fluid balance affect strength, power and high-intensity endurance? Sports Med. Auckl. N. Z. 2007, 37, 907–921. [Google Scholar] [CrossRef]
- Jones, L.C.; Cleary, M.A.; Lopez, R.M.; Zuri, R.E.; Lopez, R. Active dehydration impairs upper and lower body anaerobic muscular power. J. Strength Cond. Res. 2008, 22, 455–463. [Google Scholar] [CrossRef]
- Zhang, N.; Du, S.M.; Zhang, J.F.; Ma, G.S. Effects of Dehydration and Rehydration on Cognitive Performance and Mood among Male College Students in Cangzhou, China: A Self-Controlled Trial. Int. J. Environ. Res. Public. Health 2019, 16, 1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cian, C.; Barraud, P.A.; Melin, B.; Raphel, C. Effects of fluid ingestion on cognitive function after heat stress or exercise-induced dehydration. Int. J. Psychophysiol Off. J. Int. Organ. Psychophysiol. 2001, 42, 243–251. [Google Scholar] [CrossRef]
- Goodman, S.P.J.; Moreland, A.T.; Marino, F.E. The effect of active hypohydration on cognitive function: A systematic review and meta-analysis. Physiol. Behav. 2019, 204, 297–308. [Google Scholar] [CrossRef]
- Irwin, C.; Campagnolo, N.; Iudakhina, E.; Cox, G.R.; Desbrow, B. Effects of acute exercise, dehydration and rehydration on cognitive function in well-trained athletes. J. Sports Sci. 2018, 36, 247–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavouras, S.A. Hydration, dehydration, underhydration, optimal hydration: Are we barking up the wrong tree? Eur. J. Nutr. 2019, 58, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Laja García, A.I.; Moráis-Moreno, C.; Samaniego-Vaesken, M.d.L.; Puga, A.M.; Partearroyo, T.; Varela-Moreiras, G. Influence of Water Intake and Balance on Body Composition in Healthy Young Adults from Spain. Nutrients 2019, 11, 1923. [Google Scholar] [CrossRef] [Green Version]
- Dubnov-Raz, G.; Constantini, N.W.; Yariv, H.; Nice, S.; Shapira, N. Influence of water drinking on resting energy expenditure in overweight children. Int. J. Obes. 2011, 35, 1295–1300. [Google Scholar] [CrossRef] [Green Version]
- Dennis, E.A.; Dengo, A.L.; Comber, D.L.; Flack, K.D.; Savla, J.; Davy, K.P.; Davy, B.M. Water consumption increases weight loss during a hypocaloric diet intervention in middle-aged and older adults. Obesity 2010, 18, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Milla-Tobarra, M.; García-Hermoso, A.; Lahoz-García, N.; Notario-Pacheco, B.; Lucas-de la Cruz, L.; Pozuelo-Carrascosa, D.P.; García-Meseguer, M.J.; Martínez-Vizcaíno, V. The association between water intake, body composition and cardiometabolic factors among children–The Cuenca study. Nutr. Hosp. 2016, 33, 312. [Google Scholar] [CrossRef] [Green Version]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef]
- Chang, T.; Ravi, N.; Plegue, M.A.; Sonneville, K.R.; Davis, M.M. Inadequate Hydration, BMI, and Obesity Among US Adults: NHANES 2009-2012. Ann. Fam. Med. 2016, 14, 320–324. [Google Scholar] [CrossRef]
- Enhörning, S.; Tasevska, I.; Roussel, R.; Bouby, N.; Persson, M.; Burri, P.; Bankir, L.; Melander, O. Effects of hydration on plasma copeptin, glycemia and gluco-regulatory hormones: A water intervention in humans. Eur. J. Nutr. 2019, 58, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Perrier, E.T.; Armstrong, L.E.; Bottin, J.H.; Clark, W.F.; Dolci, A.; Guelinckx, I.; Iroz, A.; Kavouras, S.A.; Lang, F.; Lieberman, H.R.; et al. Hydration for health hypothesis: A narrative review of supporting evidence. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Enhörning, S.; Bankir, L.; Bouby, N.; Struck, J.; Hedblad, B.; Persson, M.; Morgenthaler, N.G.; Nilsson, P.M.; Melander, O. Copeptin, a marker of vasopressin, in abdominal obesity, diabetes and microalbuminuria: The prospective Malmö Diet and Cancer Study cardiovascular cohort. Int. J. Obes. 2013, 37, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Stookey, J.D.; Kavouras, S.A.; Suh, H.; Lang, F. Underhydration Is Associated with Obesity, Chronic Diseases, and Death within 3 to 6 Years in the U.S. Population Aged 51–70 Years. Nutrients 2020, 12, 905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, W.F.; Sontrop, J.M.; Macnab, J.J.; Suri, R.S.; Moist, L.; Salvadori, M.; Garg, A.X. Urine volume and change in estimated GFR in a community-based cohort study. Clin. J. Am. Soc. Nephrol. CJASN 2011, 6, 2634–2641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, W.J.; Fry, A.C.; Rubin, M.R.; Triplett-McBride, T.; Gordon, S.E.; Koziris, L.P.; Lynch, J.M.; Volek, J.S.; Meuffels, D.E.; Newton, R.U.; et al. Physiological and performance responses to tournament wrestling. Med. Sci. Sports Exerc. 2001, 33, 1367–1378. [Google Scholar] [CrossRef]
- Hackney, A.C.; Walz, E.A. Hormonal adaptation and the stress of exercise training: The role of glucocorticoids. Trends Sport Sci. 2013, 20, 165–171. [Google Scholar]
- Thomas, D.D.; Corkey, B.E.; Istfan, N.W.; Apovian, C.M. Hyperinsulinemia: An Early Indicator of Metabolic Dysfunction. J. Endocr. Soc. 2019, 3, 1727–1747. [Google Scholar] [CrossRef]
- Miller, G.D. Appetite Regulation: Hormones, Peptides, and Neurotransmitters and Their Role in Obesity. Am. J. Lifestyle Med. 2017, 13, 586–601. [Google Scholar] [CrossRef]
- Johnson, E.C.; Bardis, C.N.; Jansen, L.T.; Adams, J.D.; Kirkland, T.W.; Kavouras, S.A. Reduced water intake deteriorates glucose regulation in patients with type 2 diabetes. Nutr. Res. N. Y. 2017, 43, 25–32. [Google Scholar] [CrossRef]
- Keller, U.; Szinnai, G.; Bilz, S.; Berneis, K. Effects of changes in hydration on protein, glucose and lipid metabolism in man: Impact on health. Eur. J. Clin. Nutr. 2003, 57, S69–S74. [Google Scholar] [CrossRef] [Green Version]
- Carroll, H.A.; Templeman, I.; Chen, Y.-C.; Edinburgh, R.M.; Burch, E.K.; Jewitt, J.T.; Povey, G.; Robinson, T.D.; Dooley, W.L.; Jones, R.; et al. Effect of acute hypohydration on glycemic regulation in healthy adults: A randomized crossover trial. J. Appl. Physiol. 2019, 126, 422–430. [Google Scholar] [CrossRef]
- Tanoue, A.; Ito, S.; Honda, K.; Oshikawa, S.; Kitagawa, Y.; Koshimizu, T.; Mori, T.; Tsujimoto, G. The vasopressin V1b receptor critically regulates hypothalamic-pituitary-adrenal axis activity under both stress and resting conditions. J. Clin. Investig. 2004, 113, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Mazzocchi, G.; Malendowicz, L.K.; Rebuffat, P.; Tortorella, C.; Nussdorfer, G.G. Arginine-vasopressin stimulates CRH and ACTH release by rat adrenal medulla, acting via the V1 receptor subtype and a protein kinase C-dependent pathway. Peptides 1997, 18, 191–195. [Google Scholar] [CrossRef]
- Nakamura, K.; Velho, G.; Bouby, N. Vasopressin and metabolic disorders: Translation from experimental models to clinical use. J. Intern. Med. 2017, 282, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Papatheodorou, K.; Banach, M.; Bekiari, E.; Rizzo, M.; Edmonds, M. Complications of Diabetes 2017. J. Diabetes Res. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Cermak, N.M.; van Loon, L.J.C. The use of carbohydrates during exercise as an ergogenic aid. Sports Med. Auckl. N. Z. 2013, 43, 1139–1155. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.J.; Guelfi, K.J.; Wallman, K.E.; Fairchild, T.J. Mild dehydration does not reduce postexercise appetite or energy intake. Med. Sci. Sports Exerc. 2012, 44, 516–524. [Google Scholar] [CrossRef]
- Pérez-Luco, C.; Díaz-Castro, F.; Jorquera, C.; Troncoso, R.; Zbinden-Foncea, H.; Johannsen, N.M.; Castro-Sepulveda, M. Fluid Restriction Decreases Solid Food Consumption Post-Exercise. Nutrients 2019, 11, 1209. [Google Scholar] [CrossRef] [Green Version]
- van Dijk, G.; Evers, S.S.; Guidotti, S.; Thornton, S.N.; Scheurink, A.J.W.; Nyakas, C. The lateral hypothalamus: A site for integration of nutrient and fluid balance. Behav. Brain Res. 2011, 221, 481–487. [Google Scholar] [CrossRef]
- Perry, B.; Wang, Y. Appetite regulation and weight control: The role of gut hormones. Nutr. Diabetes 2012, 2, e26. [Google Scholar] [CrossRef] [Green Version]
- Alghannam, A.F.; Gonzalez, J.T.; Betts, J.A. Restoration of Muscle Glycogen and Functional Capacity: Role of Post-Exercise Carbohydrate and Protein Co-Ingestion. Nutrients 2018, 10, 253. [Google Scholar] [CrossRef] [Green Version]
- Phillips, S.M.; Van Loon, L.J.C. Dietary protein for athletes: From requirements to optimum adaptation. J. Sports Sci. 2011, 29 (Suppl. 1), S29–S38. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.N. Effect of Pre-meal Water Consumption on Energy Intake and Satiety in Non-obese Young Adults. Clin. Nutr. Res. 2018, 7, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Davy, B.M.; Dennis, E.A.; Dengo, A.L.; Wilson, K.L.; Davy, K.P. Water consumption reduces energy intake at a breakfast meal in obese older adults. J. Am. Diet. Assoc. 2008, 108, 1236–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endalifer, M.L.; Diress, G. Epidemiology, Predisposing Factors, Biomarkers, and Prevention Mechanism of Obesity: A Systematic Review. Available online: https://www.hindawi.com/journals/jobe/2020/6134362/ (accessed on 4 August 2020).
- Cozma, S.; Dima-Cozma, L.C.; Ghiciuc, C.M.; Pasquali, V.; Saponaro, A.; Patacchioli, F.R. Salivary cortisol and α-amylase: Subclinical indicators of stress as cardiometabolic risk. Braz. J. Med. Biol. Res. 2017, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- des Gachons, C.P.; Breslin, P.A.S. Salivary Amylase: Digestion and Metabolic Syndrome. Curr. Diab. Rep. 2016, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Rashkova, M.R.; Ribagin, L.S.; Toneva, N.G. Correlation between salivary alpha-amylase and stress-related anxiety. Folia Med. 2012, 54, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Chatterton, R.T.; Vogelsong, K.M.; Lu, Y.C.; Ellman, A.B.; Hudgens, G.A. Salivary alpha-amylase as a measure of endogenous adrenergic activity. Clin. Physiol. Oxf. Engl. 1996, 16, 433–448. [Google Scholar] [CrossRef]
- Ring, M.; Lohmueller, C.; Rauh, M.; Mester, J.; Eskofier, B.M. Salivary Markers for Quantitative Dehydration Estimation During Physical Exercise. IEEE J. Biomed. Health Inform. 2017, 21, 1306–1314. [Google Scholar] [CrossRef]
- Koibuchi, E.; Suzuki, Y. Exercise upregulates salivary amylase in humans (Review). Exp. Ther. Med. 2014, 7, 773–777. [Google Scholar] [CrossRef]
- Hayes, L.D.; Grace, F.M.; Baker, J.S.; Sculthorpe, N. Exercise-induced responses in salivary testosterone, cortisol, and their ratios in men: A meta-analysis. Sports Med. Auckl. N. Z. 2015, 45, 713–726. [Google Scholar] [CrossRef] [Green Version]
- Francesconi, R.P.; Sawka, M.N.; Pandolf, K.B.; Hubbard, R.W.; Young, A.J.; Muza, S. Plasma hormonal responses at graded hypohydration levels during exercise-heat stress. J. Appl. Physiol. 1985, 59, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Maresh, C.M.; Whittlesey, M.J.; Armstrong, L.E.; Yamamoto, L.M.; Judelson, D.A.; Fish, K.E.; Casa, D.J.; Kavouras, S.A.; Castracane, V.D. Effect of hydration state on testosterone and cortisol responses to training-intensity exercise in collegiate runners. Int. J. Sports Med. 2006, 27, 765–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fareau, G.G.; Vassilopoulou-Sellin, R. Hypercortisolemia and infection. Infect. Dis. Clin. N. Am. 2007, 21, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Min, L. Functional hypercortisolism, visceral obesity and metabolic syndrome. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2016, 22, 506–508. [Google Scholar] [CrossRef] [Green Version]
- Casa, D.J.; Maresh, C.M.; Armstrong, L.E.; Kavouras, S.A.; Herrera-Soto, J.A.; Hacker, F.T.; Scheett, T.P.; Stoppani, J. Intravenous versus oral rehydration during a brief period: Stress hormone responses to subsequent exhaustive exercise in the heat. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Hoffman, J.R.; Ratamess, N.A.; Kang, J.; Rashti, S.L.; Kelly, N.; Gonzalez, A.M.; Stec, M.; Anderson, S.; Bailey, B.L.; Yamamoto, L.M.; et al. Examination of the efficacy of acute L-alanyl-L-glutamine ingestion during hydration stress in endurance exercise. J. Int. Soc. Sports Nutr. 2010, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, K.K.; Moore, A.W.; Hackney, A.C. Relationship Between Circulating Cortisol and Testosterone: Influence of Physical Exercise. J. Sports Sci. Med. 2005, 4, 76–83. [Google Scholar]
- Hill, E.E.; Zack, E.; Battaglini, C.; Viru, M.; Viru, A.; Hackney, A.C. Exercise and circulating cortisol levels: The intensity threshold effect. J. Endocrinol. Investig. 2008, 31, 587–591. [Google Scholar] [CrossRef]
- Dipla, K.; Kraemer, R.R.; Constantini, N.W.; Hackney, A.C. Relative energy deficiency in sports (RED-S): Elucidation of endocrine changes affecting the health of males and females. Horm. Athens Greece 2020. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Cheuvront, S.N.; Montain, S.J. Myths and methodologies: Making sense of exercise mass and water balance. Exp. Physiol. 2017, 102, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quality Assessment Tool for Quantitative Studies. Available online: https://www.nccmt.ca/knowledge-repositories/search/14 (accessed on 8 August 2020).
- Nikolakopoulou, A.; Mavridis, D.; Salanti, G. Demystifying fixed and random effects meta-analysis. Evid. Based Ment. Health 2014, 17, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.R.; Maresh, C.M.; Armstrong, L.E.; Gabaree, C.L.; Bergeron, M.F.; Kenefick, R.W.; Castellani, J.W.; Ahlquist, L.E.; Ward, A. Effects of hydration state on plasma testosterone, cortisol and catecholamine concentrations before and during mild exercise at elevated temperature. Eur. J. Appl. Physiol. 1994, 69, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.; Ratamess, N.; Kang, J.; Rashti, S.; Kelly, N.; Gonzalez, A.; Stec, M.; Anderson, S.; Bailey, B.; Yamamoto, L.; et al. Acute L-alanyl-L-glutamine ingestion during short duration, high intensity exercise and a mild hydration stress. Kinesiology 2011, 43, 125–136. [Google Scholar]
- Echegaray, M.; Armstrong, L.E.; Maresh, C.M.; Riebe, D.; Kenefick, R.W.; Castellani, J.W.; Kavouras, S.; Casa, D. Blood glucose responses to carbohydrate feeding prior to exercise in the heat: Effects of hypohydration and rehydration. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 72–83. [Google Scholar] [CrossRef]
- Francesconi, R.P.; Sawka, M.N.; Pandolf, K.B. Hypohydration and acclimation: Effects on hormone responses to exercise/heat stress. Aviat. Space Environ. Med. 1984, 55, 365–369. [Google Scholar]
- Roy, B.D.; Green, H.J.; Burnett, M.E. Prolonged exercise following diuretic-induced hypohydration: Effects on cardiovascular and thermal strain. Can. J. Physiol. Pharmacol. 2000, 78, 541–547. [Google Scholar] [CrossRef]
- Brandenberger, G.; Candas, V.; Follenius, M.; Kahn, J.M. The influence of the initial state of hydration on endocrine responses to exercise in the heat. Eur. J. Appl. Physiol. 1989, 58, 674–679. [Google Scholar] [CrossRef]
- Brandenberger, G.; Candas, V.; Follenius, M.; Libert, J.P.; Kahn, J.M. Vascular fluid shifts and endocrine responses to exercise in the heat. Eur. J. Appl. Physiol. 1986, 55, 123–129. [Google Scholar] [CrossRef]
- González-Alonso, J.; Calbet, J.A.L.; Nielsen, B. Metabolic and thermodynamic responses to dehydration-induced reductions in muscle blood flow in exercising humans. J. Physiol. 1999, 520, 577–589. [Google Scholar] [CrossRef]
- Osterberg, K.L.; Pallardy, S.E.; Johnson, R.J.; Horswill, C.A. Carbohydrate exerts a mild influence on fluid retention following exercise-induced dehydration. J. Appl. Physiol. 2010, 108, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Follenius, M.; Candas, V.; Bothorel, B.; Brandenberger, G. Effect of rehydration on atrial natriuretic peptide release during exercise in the heat. J. Appl. Physiol. 1989, 66, 2516–2521. [Google Scholar] [CrossRef] [PubMed]
- McGregor, S.J.; Nicholas, C.W.; Lakomy, H.K.; Williams, C. The influence of intermittent high-intensity shuttle running and fluid ingestion on the performance of a soccer skill. J. Sports Sci. 1999, 17, 895–903. [Google Scholar] [CrossRef] [PubMed]
- McDermott, B.P.; Casa, D.J.; Lee, E.; Yamamoto, L.; Beasley, K.; Emmanuel, H.; Anderson, J.; Pescatello, L.; Armstrong, L.E.; Maresh, C. Thermoregulation and stress hormone recovery after exercise dehydration: Comparison of rehydration methods. J. Athl. Train. 2013, 48, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Costello, J.T.; Rendell, R.A.; Furber, M.; Massey, H.C.; Tipton, M.J.; Young, J.S.; Corbett, J. Effects of acute or chronic heat exposure, exercise and dehydration on plasma cortisol, IL-6 and CRP levels in trained males. Cytokine 2018, 110, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Corney, R.A.; Horina, A.; Sunderland, C.; James, L.J. Effect of hydration status and fluid availability on ad-libitum energy intake of a semi-solid breakfast. Appetite 2015, 91, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Rehrer, N.J.; Brouns, F.; Beckers, E.J.; Frey, W.O.; Villiger, B.; Riddoch, C.J.; Menheere, P.P.; Saris, W.H. Physiological changes and gastro-intestinal symptoms as a result of ultra-endurance running. Eur. J. Appl. Physiol. 1992, 64, 1–8. [Google Scholar] [CrossRef]
- Corney, R.A.; Sunderland, C.; James, L.J. The effect of hydration status on appetite and energy intake. J. Sports Sci. 2015, 33, 761–768. [Google Scholar] [CrossRef] [Green Version]
- İrfan, Y. Associations among dehydration, testosterone and stress hormones in terms of body weight loss before competition. Am. J. Med. Sci. 2015, 350, 103–108. [Google Scholar] [CrossRef]
- Bouhlel, E.; Zaouali, M.; Miled, A.; Tabka, Z.; Bigard, X.; Shephard, R. Ramadan fasting and the GH/IGF-1 axis of trained men during submaximal exercise. Ann. Nutr. Metab. 2008, 52, 261–266. [Google Scholar] [CrossRef]
- Carroll, H.A.; Templeman, I.; Chen, Y.-C.; Edinburgh, R.; Burch, E.K.; Jewitt, J.T.; Povey, G.; Robinson, T.D.; Dooley, W.L.; Buckley, C.; et al. Hydration status affects thirst and salt preference but not energy intake or postprandial ghrelin in healthy adults: A randomised crossover trial. Physiol. Behav. 2019, 212, 112725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellani, J.W.; Maresh, C.M.; Armstrong, L.E.; Kenefick, R.W.; Riebe, D.; Echegaray, M.; Kavouras, S.; Castracane, V.D. Endocrine responses during exercise-heat stress: Effects of prior isotonic and hypotonic intravenous rehydration. Eur. J. Appl. Physiol. 1998, 77, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.J.S.; Camões-Costa, V.; Snipe, R.M.J.; Dixon, D.; Russo, I.; Huschtscha, Z. Impact of exercise-induced hypohydration on gastrointestinal integrity, function, symptoms, and systemic endotoxin and inflammatory profile. J. Appl. Physiol. 2019, 126, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Fortes, M.B.; Diment, B.C.; Di Felice, U.; Walsh, N.P. Dehydration decreases saliva antimicrobial proteins important for mucosal immunity. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2012, 37, 850–859. [Google Scholar] [CrossRef]
- Gill, S.K.; Teixeira, A.M.; Rosado, F.; Hankey, J.; Wright, A.; Marczak, S.; Murray, A.; Costa, R.J.S. The impact of a 24-h ultra-marathon on salivary antimicrobial protein responses. Int. J. Sports Med. 2014, 35, 966–971. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Noakes, T.D.; Soldin, S.J.; Verbalis, J.G. Acute changes in endocrine and fluid balance markers during high-intensity, steady-state, and prolonged endurance running: Unexpected increases in oxytocin and brain natriuretic peptide during exercise. Eur. J. Endocrinol. 2008, 159, 729–737. [Google Scholar] [CrossRef] [Green Version]
- Ivarsen, P.; Greisen, J.; Vilstrup, H. Acute effects of moderate dehydration on the hepatic conversion of amino nitrogen into urea nitrogen in healthy men. Clin. Sci. 2001, 101, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Judelson, D.A.; Maresh, C.M.; Yamamoto, L.M.; Farrell, M.J.; Armstrong, L.E.; Kraemer, W.J.; Volek, J.S.; Spiering, B.A.; Casa, D.J.; Anderson, J.M. Effect of hydration state on resistance exercise-induced endocrine markers of anabolism, catabolism, and metabolism. J. Appl. Physiol. 2008, 105, 816–824. [Google Scholar] [CrossRef]
- Karila, T.A.M.; Sarkkinen, P.; Marttinen, M.; Seppälä, T.; Mero, A.; Tallroth, K. Rapid weight loss decreases serum testosterone. Int. J. Sports Med. 2008, 29, 872–877. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Bathalon, G.P.; Falco, C.M.; Kramer, F.M.; Morgan, C.A.; Niro, P. Severe decrements in cognition function and mood induced by sleep loss, heat, dehydration, and undernutrition during simulated combat. Biol. Psychiatry 2005, 57, 422–429. [Google Scholar] [CrossRef]
- Mitchell, J.B.; Dugas, J.P.; McFarlin, B.K.; Nelson, M.J. Effect of exercise, heat stress, and hydration on immune cell number and function. Med. Sci. Sports Exerc. 2002, 34, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Rutherfurd-Markwick, K.; Starck, C.; Dulson, D.K.; Ali, A. Salivary diagnostic markers in males and females during rest and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baur, D.A.; Bach, C.W.; Hyder, W.J.; Ormsbee, M.J. Fluid retention, muscle damage, and altered body composition at the Ultraman triathlon. Eur. J. Appl. Physiol. 2016, 116, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Torella, R.; Sgambato, S.; D’Onofrio, F. Effect of furosemide on insulin and glucagon responses to arginine in normal subjects. Diabetologia 1980, 18, 293–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contreras-Aguilar, M.D.; Escribano, D.; Martínez-Subiela, S.; Martínez-Miró, S.; Rubio, M.; Tvarijonaviciute, A.; Tecles, F.; Cerón, J.J. Influence of the way of reporting alpha-Amylase values in saliva in different naturalistic situations: A pilot study. PLoS ONE 2017, 12, e0180100. [Google Scholar] [CrossRef] [Green Version]
- Jansen, L.T.; Suh, H.; Adams, J.D.; Sprong, C.A.; Seal, A.D.; Scott, D.M.; Butts, C.L.; Melander, O.; Kirkland, T.W.; Vanhaecke, T.; et al. Osmotic stimulation of vasopressin acutely impairs glucose regulation: A counterbalanced, crossover trial. Am. J. Clin. Nutr. 2019, 110, 1344–1352. [Google Scholar] [CrossRef]
- Enhörning, S.; Wang, T.J.; Nilsson, P.M.; Almgren, P.; Hedblad, B.; Berglund, G.; Struck, J.; Morgenthaler, N.G.; Bergmann, A.; Lindholm, E.; et al. Plasma copeptin and the risk of diabetes mellitus. Circulation 2010, 121, 2102–2108. [Google Scholar] [CrossRef] [Green Version]
- Carroll, H.A.; James, L.J. Hydration, Arginine Vasopressin, and Glucoregulatory Health in Humans: A Critical Perspective. Nutrients 2019, 11, 1201. [Google Scholar] [CrossRef] [Green Version]
- Vatansever-Ozen, S.; Tiryaki-Sonmez, G.; Bugdayci, G.; Ozen, G. The Effects of Exercise on Food Intake and Hunger: Relationship with Acylated Ghrelin and Leptin. J. Sports Sci. Med. 2011, 10, 283–291. [Google Scholar]
- Tsai, C.-L.; Wang, C.-H.; Pan, C.-Y.; Chen, F.-C.; Huang, T.-H.; Chou, F.-Y. Executive function and endocrinological responses to acute resistance exercise. Front. Behav. Neurosci. 2014, 8, 262. [Google Scholar] [CrossRef] [Green Version]
- McGuigan, M.R.; Egan, A.D.; Foster, C. Salivary Cortisol Responses and Perceived Exertion during High Intensity and Low Intensity Bouts of Resistance Exercise. J. Sports Sci. Med. 2004, 3, 8–15. [Google Scholar] [PubMed]
- McMorris, T.; Swain, J.; Smith, M.; Corbett, J.; Delves, S.; Sale, C.; Harris, R.C.; Potter, J. Heat stress, plasma concentrations of adrenaline, noradrenaline, 5-hydroxytryptamine and cortisol, mood state and cognitive performance. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2006, 61, 204–215. [Google Scholar] [CrossRef]
- Cangemi, R.; Friedmann, A.J.; Holloszy, J.O.; Fontana, L. Long-term effects of calorie restriction on serum sex hormone concentrations in men. Aging Cell 2010, 9, 236–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.K.; Hoermann, R.; Grossmann, M. Reversible male hypogonadotropic hypogonadism due to energy deficit. Clin. Endocrinol. 2019, 91, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, N.; Nater, U.M. Salivary Alpha-Amylase as a Biomarker of Stress in Behavioral Medicine. Int. J. Behav. Med. 2020, 27, 337–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piras, M.; Hand, A.R.; Mednieks, M.I.; Piludu, M. Amylase and cyclic amp receptor protein expression in human diabetic parotid glands. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2010, 39, 715–721. [Google Scholar] [CrossRef]
- Lakshmi, P.V.S.D.; Sridevi, E.; Sai Sankar, A.J.; Manoj Kumar, M.G.; Sridhar, M.; Sujatha, B. Diagnostic perspective of saliva in insulin dependent diabetes mellitus children: An in vivo study. Contemp. Clin. Dent. 2015, 6, 443–447. [Google Scholar] [CrossRef]
- Dhabhar, F.S. Effects of stress on immune function: The good, the bad, and the beautiful. Immunol. Res. 2014, 58, 193–210. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Goulet, E.D.B.; Maughan, R.J. Considerations in the Use of Body Mass Change to Estimate Change in Hydration Status during a 161-Kilometer Ultramarathon Running Competition. Sports Med. Auckl. N. Z. 2018, 48, 243–250. [Google Scholar] [CrossRef]
- Kanaley, J.A.; Boileau, R.A.; Bahr, J.M.; Misner, J.E.; Nelson, R.A. Cortisol levels during prolonged exercise: The influence of menstrual phase and menstrual status. Int. J. Sports Med. 1992, 13, 332–336. [Google Scholar] [CrossRef]
- Montero-López, E.; Santos-Ruiz, A.; García-Ríos, M.C.; Rodríguez-Blázquez, M.; Rogers, H.L.; Peralta-Ramírez, M.I. The relationship between the menstrual cycle and cortisol secretion: Daily and stress-invoked cortisol patterns. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2018, 131, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campolier, M.; Thondre, S.P.; Clegg, M.; Shafat, A.; Mcintosh, A.; Lightowler, H. Changes in PYY and gastric emptying across the phases of the menstrual cycle and the influence of the ovarian hormones. Appetite 2016, 107, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.M.; Ogunro, P.S.; Elusanmi, G.F.; Ogunyemi, O.E.; Bolarinde, A.A. Changes in Serum Leptin during Phases of Menstrual Cycle of Fertile Women: Relationship to Age Groups and Fertility. Available online: https://sites.kowsarpub.com/ijem/articles/71986.html (accessed on 7 June 2020).
- De Souza, M.J.; Leidy, H.J.; O’Donnell, E.; Lasley, B.; Williams, N.I. Fasting Ghrelin Levels in Physically Active Women: Relationship with Menstrual Disturbances and Metabolic Hormones. J. Clin. Endocrinol. Metab. 2004, 89, 3536–3542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E. Assessing hydration status: The elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef]
- Adams, W.M.; Hevel, D.J.; Maher, J.P.; McGuirt, J.T. Racial and Sex Differences in 24 Hour Urinary Hydration Markers among Male and Female Emerging Adults: A Pilot Study. Nutrients 2020, 12, 1068. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Comparison | Hormone/Biomarker | Participants | Age | Method to Reduce Total Body Water | % BML | Relative Hormone Change in Study | Absolute Hormone Change for Every 1% Increase in BML | Overall Outcome | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Baur (2016) | Pre vs Post Ultraman Triathlon | cortisol, testosterone | 18 (14 male, 4 female); cortisol (n = 17), testosterone (n = 16) | 40 ± 7 years | Multi-stage triathlon | 3.9 | cortisol: +245.35%; testosterone: −19.12% | cortisol: +104.47 nmol/L; testosterone: −1.51 nmol/L | Significant increase in cortisol (p = 0.00005) and significant decrease in testosterone (p = 0.033) from pre-post race. | moderate |
| Bouhlel (2008) | Before Ramadan vs 2 weeks into Ramadan | insulin | 9 young men from national rugby team | 19 ± 2 years | Reduced food and fluid intake (3.7 L average to 2.6 L average) | 2.24 | insulin: −18.51% | insulin: −3.94 pmol/L | No significant difference in fasting insulin levels after 2 weeks of Ramadan. | weak |
| Carroll (2019)a | Euhydration vs Hypohydration | ghrelin, insulin | 16 adults (8 female) | 30 ± 9 years | Low water content foods, 1 h dehydration in heat tent, water prescribed (3 mL/kg body mass vs 40 mL/kg lean mass plus 150% sweat losses). | 1.9 ± 1.2 | ghrelin: −9.63%; insulin: −9.61% | ghrelin: −10.12 pg/mL; insulin: −1.69 pmol/L | Post-prandial ghrelin similar between Euhydration and Hypohydration (p = 0.736) | weak |
| Carroll (2019)b | Euhydrated vs Hypohydration | cortisol, insulin | cortisol: −4.28%; insulin: −1.71% | cortisol: -7.43 nmol/L; insulin: −0.27 pmol/L | No significant difference in insulin (p = 0.200)) during OGTT. No difference in plasma cortisol (trial x time p = 0.674). | weak | ||||
| Castellani (1998) | Pre-DH and Post-DH for NF, ISO, HYPO | cortisol | 8 males | 22 ± 0.8 years | Alternating 25-min cycling and treadmill walking with 5-min rests between. CHO given prior to second piece of exercise to offset glycogen loss during DH. | 4.1 ± 0.1 | cortisol: NF +7.45%, ISO +0.6%, HYPO +60% | cortisol: NF +8.07 nmol/L, ISO + 0.68 nmol/L, HYPO +53.85 nmol/L | No significant difference in cortisol from pre- to post- dehydration under any condition (p > 0.05). | moderate |
| Corney (2015) | 13 h Post Exercise HYPO vs RE | acylated ghrelin | 10 males | 24 ± 1.2 years | Evening exercise in 35° C and either rehydrate with 175% BML (RE) or given 200 mL water (HYPO). | 2.78 ± 0.48 | acylated ghrelin: −22.0% | acylated ghrelin: −36 pmol/mL | No main effect of trial (p = 0.124) or interaction effect (p = 0.318) on acylated ghrelin. | weak |
| Costa (2019) | Water vs no water during exercise | cortisol | 11 competitive male endurance runners | 34 ± 11 years | 2-h running at 70% VO2 max in 24.7 ± 1.7 °C, 46 ± 9% RH. | 3.1 | cortisol: +7.42% | cortisol: +7.42 nmol/L | Insignificant increase in plasma cortisol pre- to post-exercise (p = 0.098). | moderate |
| Fortes (2012) | Progressive hypohydration with water vs without water | salivary alpha-amylase secretion rate | 13 healthy adults (9 males, 4 females) | 24 ± 5 years | Cycling at 55% Peak Power Output (152 ± 32 Watts) in 33C 50% RH | 1, 2, 3 | alpha-amylase secretion: −64.4% | alpha-amylase secretion: −2.0 U/mL | Significant decrease in SAA secretion rate at 3% BML (44%), p < 0.001; no effect on SAA activity (p = 0.89) | moderate |
| Gill (2014) | Ultra-endurance runners and controls | salivary alpha amylase concentration, salivary alpha-amylase Secretion, Salivary Cortisol | 25 ultra-endurance runners (19 males, 6 females); 17 Control (6 male, 11 female) | 39 ± 7 years ultra-endurance runners vs 32 ± 11 Years Control | Ultramarathon (122–208 km) | 1.6±2.0 | alpha-amylase concentration: +159.26%; alpha amylase secretion: +200%, cortisol: +218.61% | alpha-amylase concentration: +26.99 U/mL; alpha-amylase secretion: +13.75 U/mL, Cortisol: +5.88 nmol/L | Significantly increased salivary alpha-amylase secretion rate (p < 0.001) and Cortisol Responses (p < 0.001) | moderate |
| Hew-Butler (2008) | Post-exercise measures following all exercise bouts | cortisol | 7 well-trained endurance runners (5 males, 2 females) | 44 ± 4 years | Ultramarathon vs 60 min steady state run vs VO2 max test | Ultramarathon: 4±0.4 Steady state: 2.0 ± 0.1, VO2 max 0.30 ± 0.10 | cortisol Ultramarathon vs steady state: +213.46%; Ultramarathon vs VO2 max: +105%; Steady state vs VO2 max: −34.59% | cortisol Ultramarathon vs steady state: +306.25 nmol/L; Ultramarathon vs VO2 max: +124.53 nmol/L; Steady state vs VO2 max: −89.26 nmol/L | Significantly higher cortisol following ultramarathon compared to steady state (p < 0.01) and VO2 max (p < 0.01) | weak |
| Hoffman (2010) | Hypohydration vs Baseline for W, DHY, LDAG, HDAG trials | cortisol, testosterone | 10 active males | 20.8 ± 0.6 years | Overnight food and fluid restriction to 1.03(1.3)% body mass loss. Then active dehydration protocol next morning: treadmill walking at 3.4 mi/h at 2% incline in training suit (long cotton heavy weight fleece sweat pants and top). 62.5 (44.2) min to reach weight loss. | 2.5 | cortisol HHY vs BL for DHY trial: +34.81%; HHY vs BL for W trial: +38.9%; HHY vs BL for LDAG: +28.66%; HHY vs BL for HDAG: +2.92% testosterone: HHY vs BL for DHY trial: −7.82%; HHY vs BL for W trial: −13.49%; HHY vs BL for LDAG: 3.83%; HHY vs BL for HDAG: 11.69% | cortisol: HHY vs BL for DHY trial: +34.81%; HHY vs BL for W trial: +38.9%; HHY vs BL for LDAG: +28.66%; HHY vs BL for HDAG: testosterone: HHY vs BL for DHY trial: 0.784 nmol/L; HHY vs BL for W trial:1.35 nmol/L; HHY vs BL for LDAG: −0.384 nmol/L; HHY vs BL for HDAG: 1.17 nmol/L | No significant differences in cortisol or testosterone after hypohydration. | weak |
| Irfan (2015) | Plasma osmolarity > 290 mOsm/L vs <290 mOsm/L | cortisol, testosterone | 34 vs 22 elite male wrestlers | 22.30 ± 2.43 years | Variable among wrestlers, including sauna, intense exercise and fluid restriction 1–5 days before competition | 2.49 | cortisol: + 67%; testosterone: −35.75% | cortisol: + 68.35 nmol/L; testosterone: −3.10 ng/dL | Significant increase in cortisol (p = 0.001) and significant decrease in testosterone (p = 0.001) for those participants considered dehydrated compared to euhydrated based on plasma osmolarity. | weak |
| Ivarsen (2001) | Euhydrated vs Hypohydration | glucagon, insulin | 7 healthy males | 23 | Diuretic (furosemide) | 1 | glucagon: +23.52% insulin: −3.03% | glucagon: 36 pg/mL; insulin: +1 pmol/L | Significant increase in plasma glucagon concentration during alanine infusion (p < 005); no significant difference in insulin concentration | weak |
| Judelson (2008) | Euhydrated vs 2% Hypohydration; Euhydrated vs 5% Hypohydration pre-exercise | cortisol, insulin, testosterone | 7 resistance trained males | 23 ± 4 years | Combination fluid/fluid-rich food restriction, then returned and walked on treadmill 1.5 m/s 3% incline in environmental chamber 36–37C, 40–50% RH), repeated walking during all trials. Rehydrated with normal saline to achieve +0.5% over desired dehydration level to account for overnight water losses. | 2.5, 5 | cortisol EUH vs HY50: +23.05%; EUH vs HY25: +5.38%; testosterone EUH vs HY50: −7.49%; EUH vs HY25: −6.48% | cortisol EUH vs HY50: +23.37 nmol/L; EUH vs HY25: +11.40 nmol/L; testosterone EUH vs HY50: 0.83 nmol/L; EUH vs HY25: 0.34 nmol/L | HY50 cortisol significantly greater than EU before resistance exercise; pre-resistance exercise insulin levels significantly higher in HY50 vs EU; no significant difference in testosterone pre-exercise. | weak |
| Karila (2008) | Before versus After rapid weight reduction | testosterone | 12 healthy male wrestlers | 21.9 (17.8–31.7) years | Combination food and fluid‘ restriction by decreasing carbohydrate and fat intake in first 2–3 weeks, caloric restriction, then heavy exercise in hot sauna and fluid restriction. | 8.2 ± 2.3 loss from all combined | testosterone: −63% | testosterone: −1.96 nmol/L | Significant decrease in serum testosterone. | weak |
| Kelly (2012) | Exercise DH vs Exercise HY Post Meal | ghrelin, leptin, PYY, insulin | 10 healthy, active males | 21.4 ± 1.3 years | Treadmill running for 45 min at 70% VO2 peak followed by fluid restriction. | 2.3 | ghrelin: −17.6%; leptin: 6.52% decrease; PYY: −3.92%;insulin: +45.2% | ghrelin: -18.56 pg/mL; leptin: -102.85 pg/mL; PYY: −3.59 pg/mL; insulin: +14.60 pmol/L | Significant decrease in ghrelin during DH compared with CON (p = 0.045) and HY trials (p = 0.014). No significant effect of hypohydration on leptin or PYY. | moderate |
| Kraemer (2001) | Baseline AM vs Pre-Match 1 | insulin | 12 male collegiate wrestlers | 19.33 ± 1.16 years | Variable food and fluid restriction, exercise | 3.89 | insulin: −8.93% | insulin: −3.94 pmol/L | No significant difference in insulin (p > 0.05) | weak |
| Lieberman (2005) | Prefield Day 1 6 pm vs Postfield Day 4 6 pm | Salivary cortisol, salivary testosterone | 31 male U.S. Army officers from an elite unit | 31.6 ± 0.4 years | Simulated combat, food restriction, fluid restriction, sleep deprivation | 5 | cortisol: +76.16%, testosterone: −23.16% | cortisol: +0.88 nmol/L; testosterone: −0.02 nmol/L | Significant increase in salivary cortisol and significant decrease in salivary testosterone (p < 0.001) | weak |
| Mitchell (2002) | Euhydrated + Heat (EH) vs Hypohydrated + Heat (HH); Euhydrated Neutral (EN) vs Hypohydrated Neutral (HN) | cortisol | 10 moderately trained males | 24.7 ± 6.6 years | 4 cycle ergometer rides at 55% VO2 peak either in a hot or neutral environment and either with or without fluid replacement throughout exercise | 1, 2.4 | cortisol: EH vs HH: +6.23%; EN vs HN +25.28% | cortisol: EH vs HH +30.62 nmol/L; EN vs HN +64.25 nmol/L | Significant increase in cortisol in hot environment regardless of hydration status. Cortisol significantly lower compared to pre-exercise in all conditions except after completing exercise hypohydrated in a hot environment (p < 0.05). | weak |
| Ring (2017) | Baseline vs Post Last Interval | salivary alpha-amylase concentration, salivary cortisol | 10 males | 25.5 ± 3.7 years | 120 min of running in eight 15-min intervals with 8 min of rest between each | 2.9 | alpha-amylase: +197.69%; cortisol: +314.67% | alpha-amylase: +152.52 U/mL; cortisol: +3.5 nmol/L | Non-linear increase in salivary cortisol and salivary alpha amylase with progressive hypohydration. | moderate |
| Rutherfurd-Markwick (2017) | Control vs Exercise | salivary alpha amylase activity; salivary alpha amylase secretion rate; salivary cortisol | 20 active adults (8 males, 12 females) | 27.4 ± 5.9 years | Moderate intensity cycling (70% peak power) for 60 min | 0.23 (males), 0.70 (females) | alpha amylase activity males: +15.18%; alpha amylase activity females: +90.85%; alpha amylase secretion males: +10.51%; alpha amylase secretion females: +82.3% | alpha amylase activity males: +25.78 U/mL; alpha amylase activity females: +38.61 U/mL; alpha amylase secretion males: +12.89 U/mL; alpha amylase secretion females: +13.4 U/mL | Significant increase in salivary alpha amylase activity (p = 0.001) and secretion rate (p = 0.023) in females but not males. Trend for higher levels of cortisol in females than males at rest (p −0.099) and during exercise (p = 0.070). | weak |
| Reference Ranges for Biomarkers | ||||||||||
| Alpha-amylase: Concentration: Mean 92.4 U/mL Secretion rate (Euhydrated mean): 15.9 U/mL Activity (Euhydrated mean): 36.0 U/mL | Cortisol: 8:00 AM 140–690 nmol/L 4:00 PM 80–330 nmol/L Saliva: 11 pm-midnight < 0.248 ug/dL | Ghrelin: Total 520–700 pg/mL | Glucagon: 50–100 pg/mL | Insulin: 43–186 pmol/L (fasted) | Leptin: Males: 0.7–5.3 ng/mL Females: 3.3–18.3 ng/mL | PYY: (Euhydrated mean): 92.5 pg/mL | Testosterone: Men 10–35 nmol/L Women <3.5 nmol/L | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaplatosch, M.E.; Adams, W.M. The Effect of Acute Hypohydration on Indicators of Glycemic Regulation, Appetite, Metabolism and Stress: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2526. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092526
Zaplatosch ME, Adams WM. The Effect of Acute Hypohydration on Indicators of Glycemic Regulation, Appetite, Metabolism and Stress: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(9):2526. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092526
Chicago/Turabian StyleZaplatosch, Mitchell E., and William M. Adams. 2020. "The Effect of Acute Hypohydration on Indicators of Glycemic Regulation, Appetite, Metabolism and Stress: A Systematic Review and Meta-Analysis" Nutrients 12, no. 9: 2526. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092526