Levels of n-3 and n-6 Fatty Acids in Maternal Erythrocytes during Pregnancy and in Human Milk and Its Association with Perinatal Mental Health

 , and
, and
Abstract
:1. Introduction
- (1)
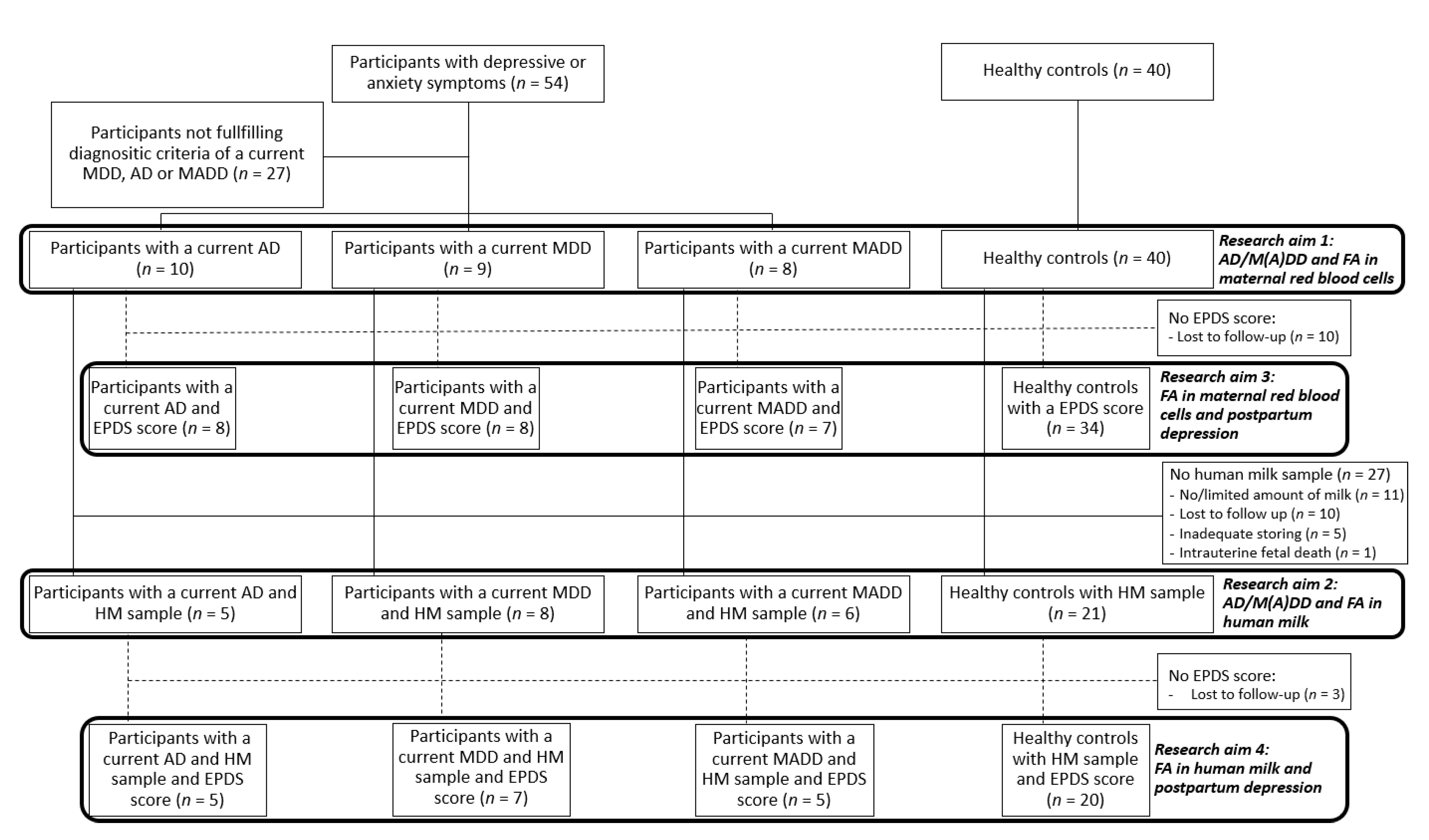
- Is there a difference in levels of n-3/n-6 FA in maternal erythrocytes at 32 weeks of gestation between women with antenatal anxiety and/or depression and healthy controls?
- (2)
- Is there a difference in levels of n-3/n-6 FA in human milk in the first week postpartum between women with antenatal anxiety and/or depression and healthy controls?
- (3)
- Is there an association between the levels of n-3/n-6 FA in maternal erythrocytes at 32 weeks of gestation and postpartum depression?
- (4)
- Is there an association between levels of n-3/n-6 FA in human milk in the first week postpartum and postpartum depression?
2. Materials and Methods
2.1. Subjects
2.2. Study Design and Sample Collection
2.3. Diagnostic Criteria for Mental Disorders
2.4. Fatty Acid Analyses in Blood and Human Milk
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Research Question 1: Is There a Difference in Levels of n-3/n-6 FA in Maternal Erythrocytes at 32 Weeks of Gestation between Women with Antenatal Anxiety and/or Depression and Healthy Controls?
3.3. Research Question 2: Is There a Difference in Levels of n-3/n-6 FA in Human Milk in the First Week Postpartum between Women with Antenatal Anxiety and/or Depression and Healthy Controls?
3.4. Research Question 3: Is There an Association between the Levels of n-3/n-6 FA in Maternal Erythrocytes at 32 Weeks of Gestation and Postpartum Depression?
3.5. Research Question 4: Is There an Association between Levels of n-3/n-6 FA in Human Milk in the First Week Postpartum and Postpartum Depression?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ashley, J.M.; Harper, B.D.; Arms-Chavez, C.J.; LoBello, S.G. Estimated prevalence of antenatal depression in the US population. Arch. Women’s Ment. Health 2016, 19, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.A.; Einarson, A.; Taddio, A.; Koren, G.; Einarson, T.R. Prevalence of depression during pregnancy: Systematic review. Obstet. Gynecol. 2004, 103, 698–709. [Google Scholar] [CrossRef] [PubMed]
- Faisal-Cury, A.; Rossi Menezes, P. Prevalence of anxiety and depression during pregnancy in a private setting sample. Arch. Women’s Ment. Health 2007, 10, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Getinet, W.; Amare, T.; Boru, B.; Shumet, S.; Worku, W.; Azale, T. Prevalence and Risk Factors for Antenatal Depression in Ethiopia: Systematic Review. Depress. Res. Treat. 2018, 2018, 3649269. [Google Scholar] [CrossRef]
- Letourneau, N.L.; Dennis, C.L.; Cosic, N.; Linder, J. The effect of perinatal depression treatment for mothers on parenting and child development: A systematic review. Depress. Anxiety 2017, 34, 928–966. [Google Scholar] [CrossRef]
- Mahendran, R.; Puthussery, S.; Amalan, M. Prevalence of antenatal depression in South Asia: A systematic review and meta-analysis. J. Epidemiol. Community Health 2019, 73, 768–777. [Google Scholar] [CrossRef] [Green Version]
- Marcus, S.M.; Flynn, H.A.; Blow, F.C.; Barry, K.L. Depressive symptoms among pregnant women screened in obstetrics settings. J. Women’s Health 2003, 12, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Okagbue, H.I.; Adamu, P.I.; Bishop, S.A.; Oguntunde, P.E.; Opanuga, A.A.; Akhmetshin, E.M. Systematic Review of Prevalence of Antepartum Depression during the Trimesters of Pregnancy. Open Access Maced. J. Med. Sci. 2019, 7, 1555–1560. [Google Scholar] [CrossRef] [Green Version]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Kingston, D.; Tough, S.; Whitfield, H. Prenatal and postpartum maternal psychological distress and infant development: A systematic review. Child Psychiatry Hum. Dev. 2012, 43, 683–714. [Google Scholar] [CrossRef]
- O’Connor, T.G.; Heron, J.; Golding, J.; Beveridge, M.; Glover, V. Maternal antenatal anxiety and children’s behavioural/emotional problems at 4 years. Report from the Avon Longitudinal Study of Parents and Children. Br. J. Psychiatry J. Ment. Sci. 2002, 180, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Thiel, F.; Iffland, L.; Drozd, F.; Haga, S.M.; Martini, J.; Weidner, K.; Eberhard-Gran, M.; Garthus-Niegel, S. Specific relations of dimensional anxiety and manifest anxiety disorders during pregnancy with difficult early infant temperament: A longitudinal cohort study. Arch. Women’s Ment. Health 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, C.T. A meta-analysis of predictors of postpartum depression. Nurs. Res. 1996, 45, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, N.K.; Boyacioglu, N.E.; Dinc, H. Postpartum Depression Prevalence and Risk Factors in Turkey: A Systematic Review and Meta-Analysis. Arch. Psychiatr. Nurs. 2017, 31, 420–428. [Google Scholar] [CrossRef]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; Tam, W.W.S.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Upadhyay, R.P.; Chowdhury, R.; Aslyeh, S.; Sarkar, K.; Singh, S.K.; Sinha, B.; Pawar, A.; Rajalakshmi, A.K.; Kumar, A. Postpartum depression in India: A systematic review and meta-analysis. Bull. World Health Organ. 2017, 95, 706. [Google Scholar] [CrossRef]
- Markhus, M.W.; Skotheim, S.; Graff, I.E.; Froyland, L.; Braarud, H.C.; Stormark, K.M.; Malde, M.K. Low omega-3 index in pregnancy is a possible biological risk factor for postpartum depression. PLoS ONE 2013, 8, e67617. [Google Scholar] [CrossRef] [Green Version]
- Luoma, I.; Tamminen, T.; Kaukonen, P.; Laippala, P.; Puura, K.; Salmelin, R.; Almqvist, F. Longitudinal study of maternal depressive symptoms and child well-being. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1367–1374. [Google Scholar] [CrossRef]
- Dennis, C.L.; Dowswell, T. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Systematic Review—Intervention. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Sparling, T.M.; Henschke, N.; Nesbitt, R.C.; Gabrysch, S. The role of diet and nutritional supplementation in perinatal depression: A systematic review. Matern. Child Nutr. 2017, 13. [Google Scholar] [CrossRef]
- Nakamura, M.; Miura, A.; Nagahata, T.; Shibata, Y.; Okada, E.; Ojima, T. Low Zinc, Copper, and Manganese Intake is Associated with Depression and Anxiety Symptoms in the Japanese Working Population: Findings from the Eating Habit and Well-Being Study. Nutrients 2019, 11, 847. [Google Scholar] [CrossRef] [Green Version]
- Rechenberg, K.; Humphries, D. Nutritional interventions in depression and perinatal depression. Yale J. Biol. Med. 2013, 86, 127–137. [Google Scholar]
- Mocking, R.J.T.; Assies, J.; Ruhe, H.G.; Schene, A.H. Focus on fatty acids in the neurometabolic pathophysiology of psychiatric disorders. J. Inherit. Metab. Dis. 2018, 41, 597–611. [Google Scholar] [CrossRef] [Green Version]
- Al, M.D.; van Houwelingen, A.C.; Hornstra, G. Long-chain polyunsaturated fatty acids, pregnancy, and pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, 285S–291S. [Google Scholar] [CrossRef]
- Hornstra, G. Essential fatty acids in mothers and their neonates. Am. J. Clin. Nutr. 2000, 71, 1262S–1269S. [Google Scholar] [CrossRef]
- Coletta, J.M.; Bell, S.J.; Roman, A.S. Omega-3 Fatty acids and pregnancy. Rev. Obstet. Gynecol. 2010, 3, 163–171. [Google Scholar]
- Browne, J.C.; Scott, K.M.; Silvers, K.M. Fish consumption in pregnancy and omega-3 status after birth are not associated with postnatal depression. J. Affect. Disord. 2006, 90, 131–139. [Google Scholar] [CrossRef]
- Golding, J.; Steer, C.; Emmett, P.; Davis, J.M.; Hibbeln, J.R. High levels of depressive symptoms in pregnancy with low omega-3 fatty acid intake from fish. Epidemiology 2009, 20, 598–603. [Google Scholar] [CrossRef]
- Hamazaki, K.; Takamori, A.; Tsuchida, A.; Kigawa, M.; Tanaka, T.; Ito, M.; Adachi, Y.; Saito, S.; Origasa, H.; Inadera, H. Dietary intake of fish and n-3 polyunsaturated fatty acids and risks of perinatal depression: The Japan Environment and Children’s Study (JECS). J. Psychiatr. Res. 2018, 98, 9–16. [Google Scholar] [CrossRef]
- Sontrop, J.; Avison, W.R.; Evers, S.E.; Speechley, K.N.; Campbell, M.K. Depressive symptoms during pregnancy in relation to fish consumption and intake of n-3 polyunsaturated fatty acids. Paediatr. Perinat. Epidemiol. 2008, 22, 389–399. [Google Scholar] [CrossRef]
- Strom, M.; Mortensen, E.L.; Halldorsson, T.I.; Thorsdottir, I.; Olsen, S.F. Fish and long-chain n-3 polyunsaturated fatty acid intakes during pregnancy and risk of postpartum depression: A prospective study based on a large national birth cohort. Am. J. Clin. Nutr. 2009, 90, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Wisner, K.L.; Luther, J.F.; Powers, R.W.; Evans, R.W.; Gallaher, M.J.; Newby, P.K. An exploratory factor analysis of nutritional biomarkers associated with major depression in pregnancy. Public Health Nutr. 2012, 15, 1078–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, M.F.; Ong, Y.L.; Calder, P.C.; Colega, M.; Wong, J.X.; Tan, C.S.; Lim, A.L.; Fisk, H.L.; Cai, S.; Pang, W.W.; et al. Long-chain polyunsaturated fatty acid status during pregnancy and maternal mental health in pregnancy and the postpartum period: Results from the GUSTO study. J. Clin. Psychiatry 2015, 76, e848–e856. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.; Vieira, M.C.; Lepsch, J.; Rebelo, F.; Poston, L.; Pasupathy, D.; Kac, G. A systematic review of the associations between maternal nutritional biomarkers and depression and/or anxiety during pregnancy and postpartum. J. Affect. Disord. 2018, 232, 185–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Rocha, C.M.; Kac, G. High dietary ratio of omega-6 to omega-3 polyunsaturated acids during pregnancy and prevalence of post-partum depression. Matern. Child Nutr. 2012, 8, 36–48. [Google Scholar] [CrossRef]
- Saccone, G.; Saccone, I.; Berghella, V. Omega-3 long-chain polyunsaturated fatty acids and fish oil supplementation during pregnancy: Which evidence? J. Matern. Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obs. 2016, 29, 2389–2397. [Google Scholar] [CrossRef] [Green Version]
- Gould, J.F.; Best, K.; Makrides, M. Perinatal nutrition interventions and post-partum depressive symptoms. J. Affect. Disord. 2017, 224, 2–9. [Google Scholar] [CrossRef]
- Hsu, M.C.; Tung, C.Y.; Chen, H.E. Omega-3 polyunsaturated fatty acid supplementation in prevention and treatment of maternal depression: Putative mechanism and recommendation. J. Affect. Disord. 2018, 238, 47–61. [Google Scholar] [CrossRef]
- Wojcicki, J.M.; Heyman, M.B. Maternal omega-3 fatty acid supplementation and risk for perinatal maternal depression. J. Matern. Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obs. 2011, 24, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Jans, L.A.; Giltay, E.J.; Van der Does, A.J. The efficacy of n-3 fatty acids DHA and EPA (fish oil) for perinatal depression. Br. J. Nutr. 2010, 104, 1577–1585. [Google Scholar] [CrossRef] [Green Version]
- Rees, A.M.; Austin, M.P.; Parker, G.B. Omega-3 fatty acids as a treatment for perinatal depression: Randomized double-blind placebo-controlled trial. Aust. N. Z. J. Psychiatry 2008, 42, 199–205. [Google Scholar] [CrossRef]
- Keim, S.A.; Daniels, J.L.; Siega-Riz, A.M.; Dole, N.; Herring, A.H.; Scheidt, P.C. Depressive symptoms during pregnancy and the concentration of fatty acids in breast milk. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2012, 28, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B. Human Milk Lipids. Ann. Nutr. Metab. 2016, 69, 28–40. [Google Scholar] [CrossRef] [Green Version]
- Arab, L. Biomarkers of fat and fatty acid intake. J. Nutr. 2003, 133, 925s–932s. [Google Scholar] [CrossRef] [Green Version]
- Şenol Eren, N.; Şencan, İ.; Aksoy, H.; Koç, E.M.; Kasım, İ.; Kahveci, R.; Samur, G.; Özkara, A. Evaluation of dietary habits during pregnancy. J. Turk. Soc. Obstet. Gynecol. 2015, 12, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Forbes, L.E.; Graham, J.E.; Berglund, C.; Bell, R.C. Dietary Change during Pregnancy and Women’s Reasons for Change. Nutrients 2018, 10, 1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picó, C.; Serra, F.; Rodríguez, A.M.; Keijer, J.; Palou, A. Biomarkers of Nutrition and Health: New Tools for New Approaches. Nutrients 2019, 11, 1092. [Google Scholar] [CrossRef] [Green Version]
- Bowen, A.; Muhajarine, N. Antenatal depression. Can. Nurse 2006, 102, 26–30. [Google Scholar]
- Skouteris, H.; Wertheim, E.H.; Rallis, S.; Milgrom, J.; Paxton, S.J. Depression and anxiety through pregnancy and the early postpartum: An examination of prospective relationships. J. Affect. Disord. 2009, 113, 303–308. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Lachner, G.; Wunderlich, U.; Pfister, H. Test-retest reliability of the computerized DSM-IV version of the Munich-Composite International Diagnostic Interview (M-CIDI). Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 568–578. [Google Scholar] [CrossRef]
- Bergant, A.M.; Nguyen, T.; Heim, K.; Ulmer, H.; Dapunt, O. German language version and validation of the Edinburgh postnatal depression scale. Dtsch. Med. Wochenschr. 1998, 123, 35–40. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepage, G.; Roy, C.C. Direct transesterification of all classes of lipids in a one-step reaction. J. Lipid Res. 1986, 27, 114–120. [Google Scholar]
- Simopoulos, A.P. Omega-6/omega-3 essential fatty acids: Biological effects. World Rev. Nutr. Diet. 2009, 99, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, F.; Ambigaipalan, P. Omega-3 Polyunsaturated Fatty Acids and Their Health Benefits. Annu. Rev. Food Sci. Technol. 2018, 9, 345–381. [Google Scholar] [CrossRef]
- Otto, S.J.; de Groot, R.H.; Hornstra, G. Increased risk of postpartum depressive symptoms is associated with slower normalization after pregnancy of the functional docosahexaenoic acid status. Prostaglandins Leukot. Essent. Fat. Acids 2003, 69, 237–243. [Google Scholar] [CrossRef]
- Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochim. Biophys. Acta 2015, 1851, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Sakai, C.; Ishida, M.; Ohba, H.; Yamashita, H.; Uchida, H.; Yoshizumi, M.; Ishida, T. Fish oil omega-3 polyunsaturated fatty acids attenuate oxidative stress-induced DNA damage in vascular endothelial cells. PLoS ONE 2017, 12, e0187934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simopoulos, A.P. Evolutionary aspects of diet: The omega-6/omega-3 ratio and the brain. Mol. Neurobiol. 2011, 44, 203–215. [Google Scholar] [CrossRef]
- Grosso, G.; Galvano, F.; Marventano, S.; Malaguarnera, M.; Bucolo, C.; Drago, F.; Caraci, F. Omega-3 fatty acids and depression: Scientific evidence and biological mechanisms. Oxid. Med. Cell. Longev. 2014, 2014, 313570. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Cherbuin, N.; Anstey, K.J.; Butterworth, P. Does reverse causality explain the relationship between diet and depression? J. Affect. Disord. 2015, 175, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; Rothon, C.; Taylor, S.; Berk, M.; Stansfeld, S.A. Diet quality and mental health problems in adolescents from East London: A prospective study. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.T.; Hao, J.H.; Qian, Q.W.; Cao, H.; Fu, J.L.; Sun, Y.; Huang, L.; Tao, F.B. Is there any relationship between dietary patterns and depression and anxiety in Chinese adolescents? Public Health Nutr. 2012, 15, 673–682. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhao, J.; Guo, W. Emotional Roles of Mono-Aminergic Neurotransmitters in Major Depressive Disorder and Anxiety Disorders. Front. Psychol. 2018, 9, 2201. [Google Scholar] [CrossRef] [PubMed]
- Bender, R.; Lange, S. Adjusting for multiple testing--when and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Li, G.; Taljaard, M.; Van den Heuvel, E.R.; Levine, M.A.; Cook, D.J.; Wells, G.A.; Devereaux, P.J.; Thabane, L. An introduction to multiplicity issues in clinical trials: The what, why, when and how. Int. J. Epidemiol. 2017, 46, 746–755. [Google Scholar] [CrossRef]
- Wason, J.M.; Stecher, L.; Mander, A.P. Correcting for multiple-testing in multi-arm trials: Is it necessary and is it done? Trials 2014, 15, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| AD 1 | MDD 2 | MADD 3 | Control 4 | |
|---|---|---|---|---|
| n = 10 | n = 9 | n = 8 | n = 40 | |
| Age 5 | 36.63 (4.3) a | 25.66 (4.6) b | 29.87 (3.6) b | 33.78 (4.5) a |
| Body mass index prior to pregnancy 5 | 24.27 (6.6) | 25.25 (6.0) | 23.50 (4.1) | 24.28 (5.6) |
| Parity 5 | 0.80 (0.7) | 0.56 (1.0) | 0.50 (0.5) | 0.55 (0.7) |
| Civil status 6 | ||||
| Married/Co-habiting | 78 ab | 50 b | 100 a | 92 a |
| Single | 0 a | 50 b | 0 a | 2.7 a |
| Divorced | 11 | 0 | 0 | 5.3 |
| Other | 11 a | 0 ab | 0 ab | 0 b |
| Nationality 6 | ||||
| Swiss or German | 90 | 67 | 100 | 88 |
| Highest level of education 6 | ||||
| Secondary school | 0 ab | 50 b | 12 ab | 5 a |
| High school | 11 | 0 | 0 | 14 |
| Apprenticeship | 22 | 33 | 25 | 22 |
| Technical college | 0 a | 0 ab | 38 b | 14 ab |
| University | 67 | 17 | 25 | 45 |
| Income 6 | ||||
| Below 3000 CHF | 0a | 50 b | 0 a | 12 a |
| 3000–4500 | 11 | 33 | 12 | 18 |
| 4500–7500 | 44 | 17 | 63 | 29 |
| Above 7500 | 45 | 0 | 25 | 41 |
| Infant’s birth weight (g )5 | 3185 (499) | 3239 (490) | 3233 (353) | 3311 (492) |
| Length of gestation (weeks) 5 | 38.8 (1.3) a | 39.1 (1.2) ab | 39.2 (0.9) ab | 39.8 (1.4) b |
| Smoking during pregnancy (yes, %) | 10 ab | 33 b | 12.5 ab | 5 a |
| Antidepressants use during pregn. (yes, %) | 0 ab | 0 ab | 25 b | 0 a |
| Multivitamin or folic acid use during pregn. (yes, %) | 30 | 33 | 37.5 | 27.5 |
| AD 1 (n = 10) | MDD 2 (n = 9) | MADD 3 (n = 8) | Control 4 (n = 40) | Unadjusted Model | Adjusted Model ± | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean [95% CI] | Mean [95% CI] | Mean [95% CI] | Mean [95% CI] | AD vs Control [95% CI] p-Value * | MDD vs Control [95% CI] p-Value † | MADD vs Control [95% CI] p-Value ‡ | AD vs Control [95% CI] p-Value * | MDD vs Control [95% CI] p-Value † | MADD vs Control [95% CI] p-Value ‡ | |
| Total n-3 | 7.73 [6.90; 8.56] | 6.69 [5.36; 8.02] | 7.48 [6.44; 8.53] | 7.84 [7.47; 8.21] | −0.11 [−0.99; 0.78] | −1.15 [−2.07; −0.23] | −0.35 [−1.32; 0.61] | −0.11 [−0.97; 0.75] | −1.09 [−2.43; −0.19] | −0.40 [−1.34; 0.54] |
| 0.81 | 0.016 | 0.47 | 0.80 | 0.018 | 0.40 | |||||
| ALA | 0.13 [0.11; 0.16] | 0.11 [0.090; 0.14] | 0.10 [0.077; 0.14] | 0.12 [0.11; 0.13] | 0.015 [−0.012; 0.043] | −0.0045 [−0.030; 0.021] | −0.014 [−0.039; 0.011] | 0.015 [−0.011; 0.042] | −0.0029 [−0.028; 0.022] | −0.015 [−0.039; 0.0085] |
| 0.27 | 0.72 | 0.26 | 0.25 | 0.81 | 0.20 | |||||
| EPA | 0.34 [0.25; 0.45] | 0.23 [0.17; 0.29] | 0.24 [0.16; 0.37] | 0.33 [0.29; 0.38] | 0.0054 [−0.090; 0.10] | −0.11 [−0.18; −0.032] | −0.089 [−0.17; −0.0081] | 0.0053 [−0.084; 0.095] | −0.10 [−0.17; −0.029] | −0.092 [−0.17; −0.019] |
| 0.91 | 0.0058 | 0.032 | 0.91 | 0.0064 | 0.015 | |||||
| DHA | 5.19 [4.45; 5.94] | 4.47 [3.49; 5.45] | 5.09 [4.43; 5.75] | 5.30 [5.02; 5.58] | −0.10 [−0.78; 0.57] | −0.82 [−1.53; −0.12] | −0.21 [−0.95; 0.53] | −0.19 [−0.85; 0.47] | −0.52 [−1.26; 0.21] | −0.21 [−0.93; 0.51] |
| 0.76 | 0.022 | 0.58 | 0.57 | 0.16 | 0.56 | |||||
| n-3 DPA | 2.13 [1.92; 2.34] | 1.93 [1.57; 2.28] | 2.07 [1.72; 2.42] | 2.13 [2.02; 2.25] | −0.0022 [−0.27; 0.26] | −0.21 [−0.48; 0.070] | −0.060 [−0.35; 0.23] | −0.015 [−0.26; 0.23] | −0.21 [−0.47; 0.049] | −0.10 [−0.38; 0.17] |
| 0.99 | 0.14 | 0.68 | 0.91 | 0.11 | 0.46 | |||||
| Total n-6 | 18.9 [17.8; 20.1] | 18.9 [16.7; 21.2] | 19.5 [18.2; 20.1] | 18.8 [18.3; 19.2] | 0.16 [−1.12; 1.44] | −0.042 [−1.37; 1.29] | 0.74 [−0.70; 2.19] | 0.34 [−0.92; 1.59] | −0.66 [−2.00; 0.69] | 0.75 [−0.65; 2.14] |
| 0.80 | 0.95 | 0.31 | 0.60 | 0.33 | 0.29 | |||||
| LA | 7.92 [7.34; 8.49] | 8.02 [6.65; 9.39] | 7.96 [6.77; 9.14] | 8.28 [7.98; 8.58] | −0.37 [−1.16; 0.43] | −0.26 [−1.09; 0.57] | −0.33 [−1.20; 0.55] | −0.37 [−1.16; 0.43] | −0.26 [−1.09; 0.57] | −0.33 [−1.20; 0.55] |
| 0.36 | 0.53 | 0.46 | 0.36 | 0.53 | 0.46 | |||||
| DGLA | 1.84 [1.65; 2.06] | 1.71 [1.40; 2.09] | 1.72 [1.38; 2.13] | 1.86 [1.75; 1.97] | −0.013 [−0.28; 0.25] | −0.14 [−0.40; 0.12] | −0.14 [−0.41; 0.13] | 0.035 [−0.22; 0.29] | −0.30 [−0.54; −0.053] | −0.14 [−0.40; 0.11] |
| 0.92 | 0.27 | 0.30 | 0.78 | 0.018 | 0.27 | |||||
| AA | 12.6 [11.9; 13.3] | 12.6 [11.0; 14.2] | 12.7 [11.8; 13.6] | 12.5 [12.3; 12.8] | 0.063 [−0.74; 0.87] | 0.064 [−0.78; 0.90] | 0.15 [−0.73; 1.03] | 0.063 [−0.74; 0.87] | 0.064 [−0.78; 0.90] | 0.15 [−0.73; 1.03] |
| 0.88 | 0.88 | 0.74 | 0.88 | 0.88 | 0.74 | |||||
| n-6 DPA | 0.78 [0.67; 0.89] | 0.95 [0.72; 1.18] | 1.08 [0.75; 1.42] | 0.78 [0.73; 0.84] | 0.000 [−0.16; 0.16] 1.00 | 0.17 [−0.002; 0.33] 0.053 | 0.30 [0.12; 0.48] 0.001 | 0.028 [−0.14; 0.19] 0.73 | 0.11 [−0.096; 0.32] 0.29 | 0.29 [0.12; 0.47] 0.001 |
| Ratios | ||||||||||
| n-6:n-3 | 2.53 [2.09; 2.97] | 2.98 [2.46; 3.50] | 2.70 [2.18; 3.21] | 2.46 [2.32; 2.61] | 0.073 [−0.31; 0.46] | 0.52 [0.13; 0.92] | 0.24 [−0.18; 0.66] | 0.073 [−0.29; 0.44] | 0.49 [0.11; 0.87] | 0.26 [−0.13; 0.66] |
| 0.70 | 0.011 | 0.26 | 0.69 | 0.012 | 0.19 | |||||
| LA:ALA | 60.8 [51.4; 70.2] | 70.9 [58.0; 83.9] | 78.6 [58.6; 98.6] | 72.1 [66.2; 78.1] | −11.3 [−24.3; 1.66] | −1.20 [−14.7; 12.3] | 6.44 [−7.76; 20.7] | −10.8 [−23.0; 1.36] | −1.17 [−13.9; 11.6] | 12.8 [−2.30; 27.9] |
| 0.086 | 0.86 | 0.37 | 0.081 | 0.85 | 0.095 | |||||
| AA:EPA | 37.8 [27.4; 52.1] | 54.6 [42.7; 69.7] | 51.9 [33.2; 81.0] | 37.6 [32.9; 43.0] | 0.17 [−11.2; 11.6] | 16.9 [0.62; 33.3] | 14.2 [−2.20; 30.7] | 0.18 [−10.6; 10.9] | 15.5 [0.49; 30.6] | 15.4 [−0.45; 31.2] |
| 0.98 | 0.042 | 0.089 | 0.97 | 0.043 | 0.057 | |||||
| n-6 DPA: DHA | 0.16 [0.12; 0.21] | 0.22 [0.17; 0.27] | 0.22 [0.13; 0.31] | 0.15 [0.14; 0.17] | 0.007 [−0.038; 0.053] 0.75 | 0.066 [0.019; 0.11] 0.007 | 0.069 [0.019; 0.12] 0.008 | 0.017 [−0.030; 0.065] 0.47 | 0.018 [−0.041; 0.078] 0.54 | 0.065 [0.015; 0.12] 0.011 |
| AD 1 (n = 5) | MDD 2 (n = 8) | MADD 3 (n = 6) | Control 4 (n = 21) | Crude Model | Adjusted Model * | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | [95% CI] | Mean | [95% CI] | Mean | [95% CI] | Mean | [95% CI] | p-Value | p-Value | |
| Total n-3 | 1.44 | [1.12; 1.75] | 1.27 | [0.99; 1.54] | 1.21 | [0.84; 1.59] | 1.46 | [1.29; 1.62] | 0.14 | 0.14 |
| ALA | 0.60 | [0.40; 0.89] | 0.58 | [0.43; 0.76] | 0.51 | [0.37; 0.70] | 0.61 | [0.53; 0.70] | 0.37 | 0.37 |
| EPA | 0.045 | [0.024; 0.087] | 0.042 | [0.029; 0.060] | 0.041 | [0.023; 0.072] | 0.0047 | [0.039; 0.055] | 0.49 | 0.28 |
| DHA | 0.38 | [0.23; 0.53] | 0.31 | [0.23; 0.40] | 0.36 | [0.18; 0.54] | 0.43 | [0.35; 0.51] | 0.10 | 0.29 |
| n-3 DPA | 0.16 | [0.077; 0.32] | 0.12 | [0.066; 0.23] | 0.13 | [0.11; 0.16] | 0.14 | [0.11; 0.17] | 0.78 | 0.78 |
| Total n-6 | 11.1 | [8.87; 13.8] | 11.4 | [9.45; 13.7] | 10.4 | [8.95; 12.1] | 12.2 | [11.1; 13.3] | 0.088 | 0.088 |
| LA | 8.79 | [7.00; 11.0] | 9.18 | [7.27; 11.6] | 8.19 | [7.09; 9.47] | 9.65 | [8.73; 10.7] | 0.17 | 0.17 |
| DGLA | 0.54 | [0.47; 0.60] | 0.46 | [0.31; 0.60] | 0.48 | [0.36; 0.60] | 0.55 | [0.48; 0.63] | 0.16 | 0.078 |
| AA | 0.64 | [0.45; 0.84] | 0.63 | [0.50; 0.76] | 0.62 | [0.42; 0.81] | 0.71 | [0.62; 0.81] | 0.16 | 0.16 |
| n-6 DPA | 0.096 | [0.036; 0.16] | 0.11 | [0.063; 0.15] | 0.11 | [0.069; 0.14] | 0.11 | [0.082; 0.13] | 0.82 | 0.82 |
| Ratios | ||||||||||
| n-6:n-3 | 7.80 | [5.19; 11.7] | 9.22 | [8.06; 10.5] | 8.85 | [6.84; 11.5] | 8.60 | [7.85; 9.42] | 0.85 | 0.94 |
| LA:ALA | 15.3 | [10.0; 20.5] | 16.1 | [14.0; 18.1] | 16.5 | [11.9; 21.2] | 16.3 | [14.3; 18.2] | 0.83 | 0.60 |
| AA:EPA | 13.2 | [6.24; 27.9] | 14.6 | 8.85; 24.1] | 14.9 | [9.87; 22.5] | 14.6 | [11.8; 18.2] | 0.89 | 0.46 |
| n-6 DPA: DHA | 0.27 | [0.11; 0.43] | 0.35 | [0.23; 0.47] | 0.32 | [0.23; 0.42] | 0.25 | [0.20; 0.30] | 0.057 | 0.057 |
| Unadjusted Odds Ratio [95% CI] | p-Value | Odds Ratio Adjusted for Antenatal Mental Health [95% CI] | p-Value | |
|---|---|---|---|---|
| Total n-3 | 0.61 [0.32; 1.00] | 0.049 | 0.72 [0.37; 1.20] | 0.20 |
| ALA | 0.60 [<0.001; 157.3] | 0.85 | 0.79 [<0.001; 372.4] | 0.94 |
| EPA | 0.019 [<0.001; 0.81] | 0.038 | 0.0094 [<0.001; 5.76] | 0.26 |
| DHA | 0.56 [0.26; 1.08] | 0.081 | 0.68 [0.30; 1.35] | 0.27 |
| n-3 DPA | 0.17 [0.017; 1.19] | 0.075 | 0.26 [0.025; 1.81] | 0.18 |
| Total n-6 | 0.98 [0.68; 1.54] | 0.91 | 0.95 [0.67; 1.38] | 0.78 |
| LA | 0.97 [0.49; 1.88] | 0.92 | 1.07 [0.58; 1.99] | 0.82 |
| DGLA | <0.001 [<0.001; 0.72] | 0.042 | <0.001 [<0.001; 6.90] | 0.13 |
| AA | 0.99 [0.59; 1.99] | 0.96 | 0.98 [0.60; 1.73] | 0.95 |
| n-6 DPA | 16.8 [1.49; 453.5] | 0.022 | 4.71 [0.41; 105.8] | 0.21 |
| Ratios | ||||
| n-6:n-3 | 3.14 [1.02; 11.1] | 0.047 | 2.02 [0.63; 7.52] | 0.24 |
| LA:ALA | 1.00 [0.96; 1.04] | 0.95 | 1.00 [0.96; 1.04] | 0.98 |
| AA:EPA | 33.0 [0.93; 1998] | 0.055 | 7.71 [0.15; 623.3] | 0.31 |
| n-6 DPA:DHA | 12.1 [3.05; 23.9] | 0.008 | 7.53 [0.16; 19.3] | 0.10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urech, C.; Eussen, S.R.B.M.; Alder, J.; Stahl, B.; Boehm, G.; Bitzer, J.; Bartke, N.; Hoesli, I. Levels of n-3 and n-6 Fatty Acids in Maternal Erythrocytes during Pregnancy and in Human Milk and Its Association with Perinatal Mental Health. Nutrients 2020, 12, 2773. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092773
Urech C, Eussen SRBM, Alder J, Stahl B, Boehm G, Bitzer J, Bartke N, Hoesli I. Levels of n-3 and n-6 Fatty Acids in Maternal Erythrocytes during Pregnancy and in Human Milk and Its Association with Perinatal Mental Health. Nutrients. 2020; 12(9):2773. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092773
Chicago/Turabian StyleUrech, Corinne, Simone R. B. M. Eussen, Judith Alder, Bernd Stahl, Günter Boehm, Johannes Bitzer, Nana Bartke, and Irene Hoesli. 2020. "Levels of n-3 and n-6 Fatty Acids in Maternal Erythrocytes during Pregnancy and in Human Milk and Its Association with Perinatal Mental Health" Nutrients 12, no. 9: 2773. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092773