Evaluation of Food-Intake Behavior in a Healthy Population: Personalized vs. One-Size-Fits-All

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Participants
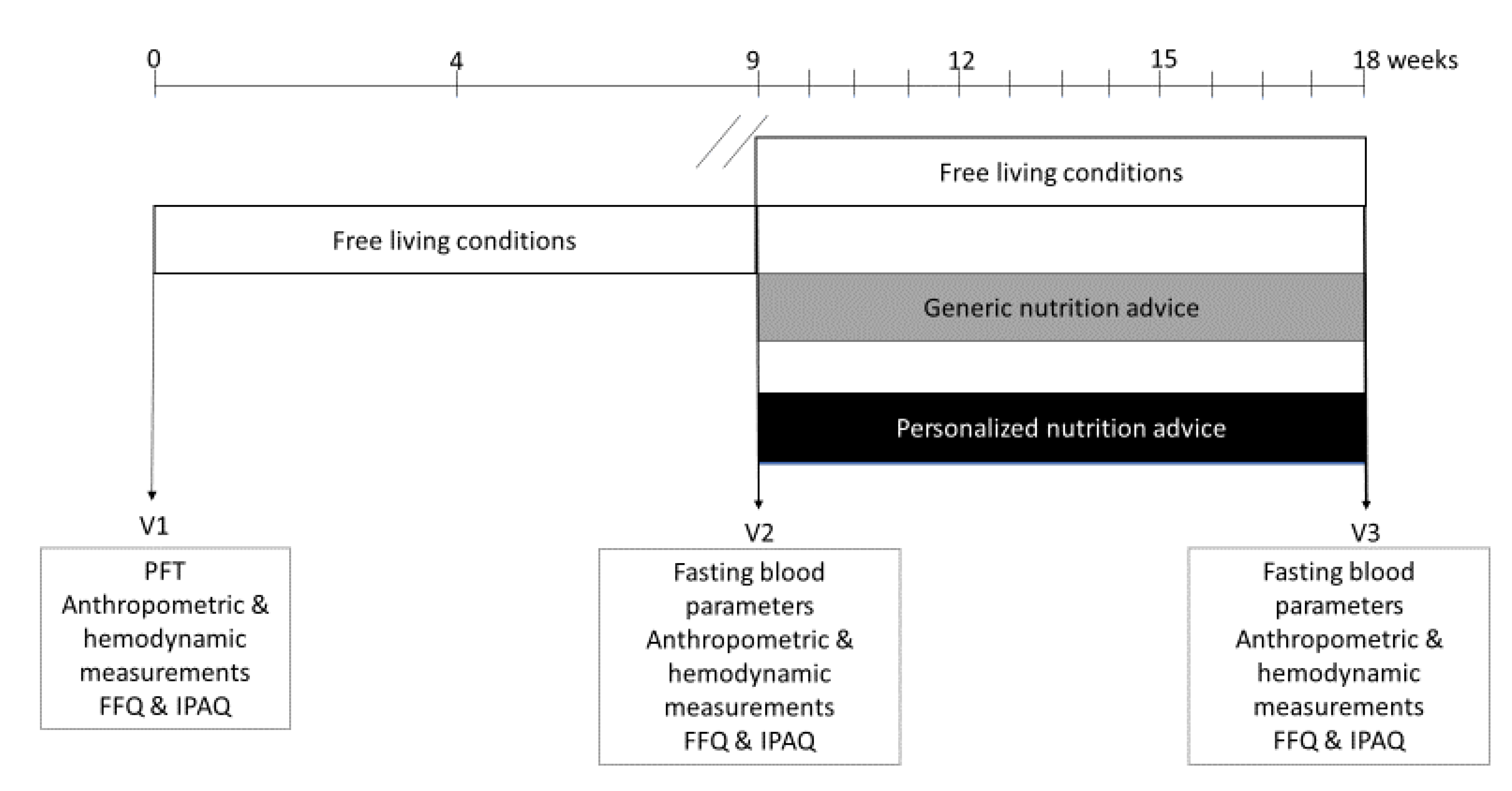
2.3. Study Design
2.4. Study Procedures
2.5. Anthropometric Parameters
2.6. Metabolic Parameters
2.7. Insulin Resistance Indices
2.8. Hemodynamic Parameters
2.9. Dietary Intake and Physical Activity
2.10. Treatment of the Control and GNA Group
2.11. Automated Health Feedback for the PNA Group
2.12. Personalization of Dietary Advice for the PNA Group
2.13. Statistical Analysis
3. Results
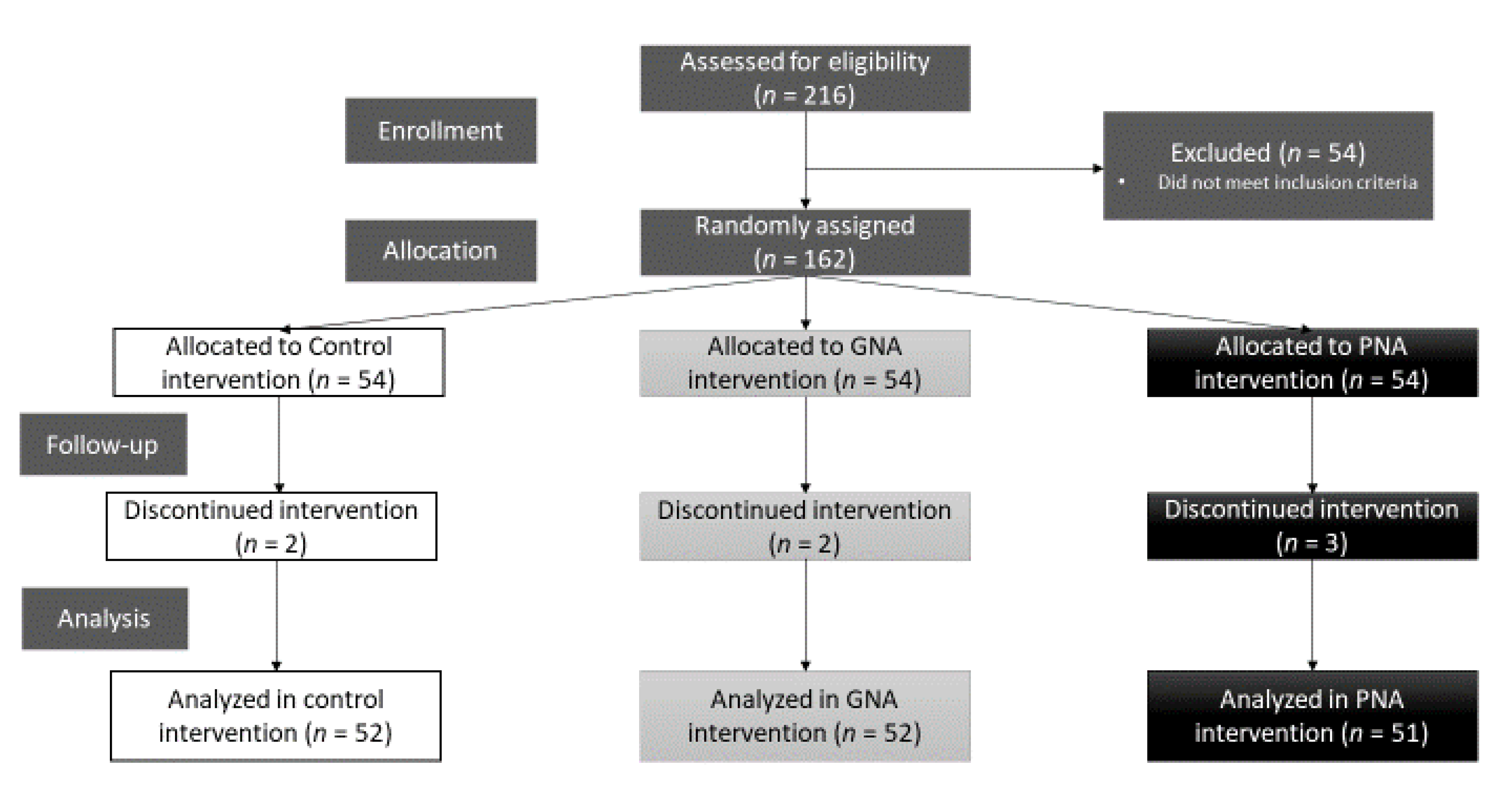
3.1. Study Logistics
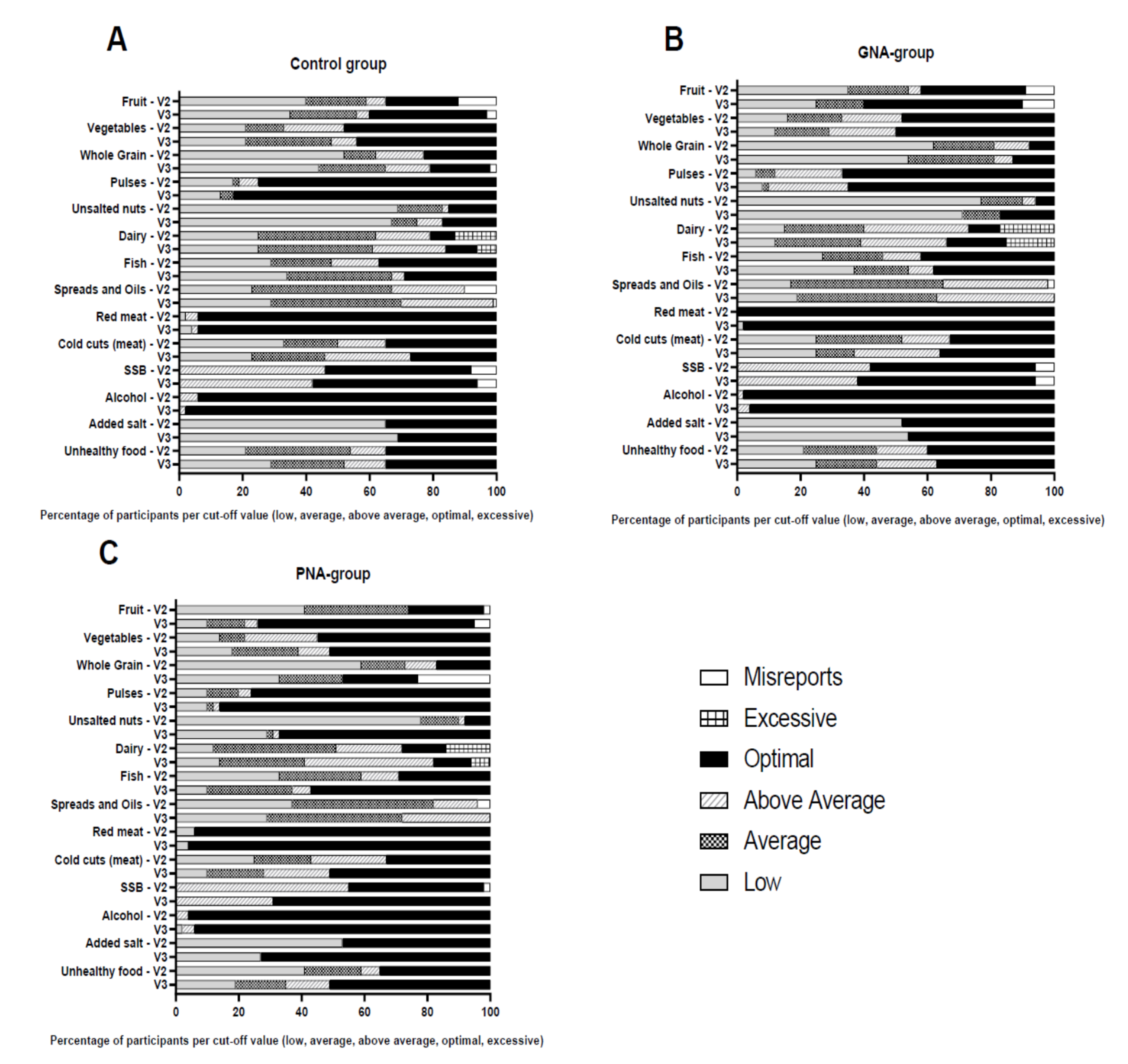
3.2. Effect of PNA on Nutrition Intake Status and Health Compared to Control and GNA
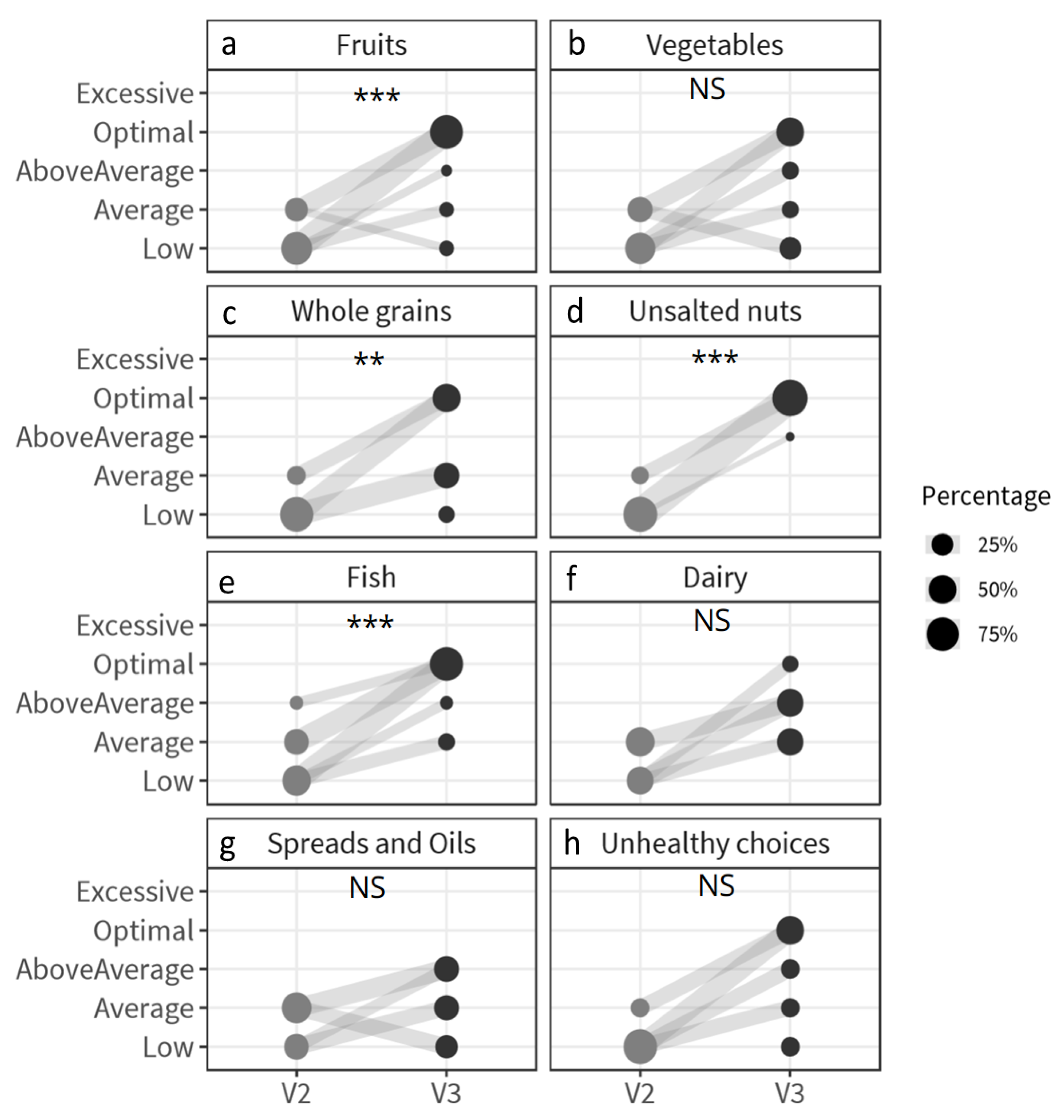
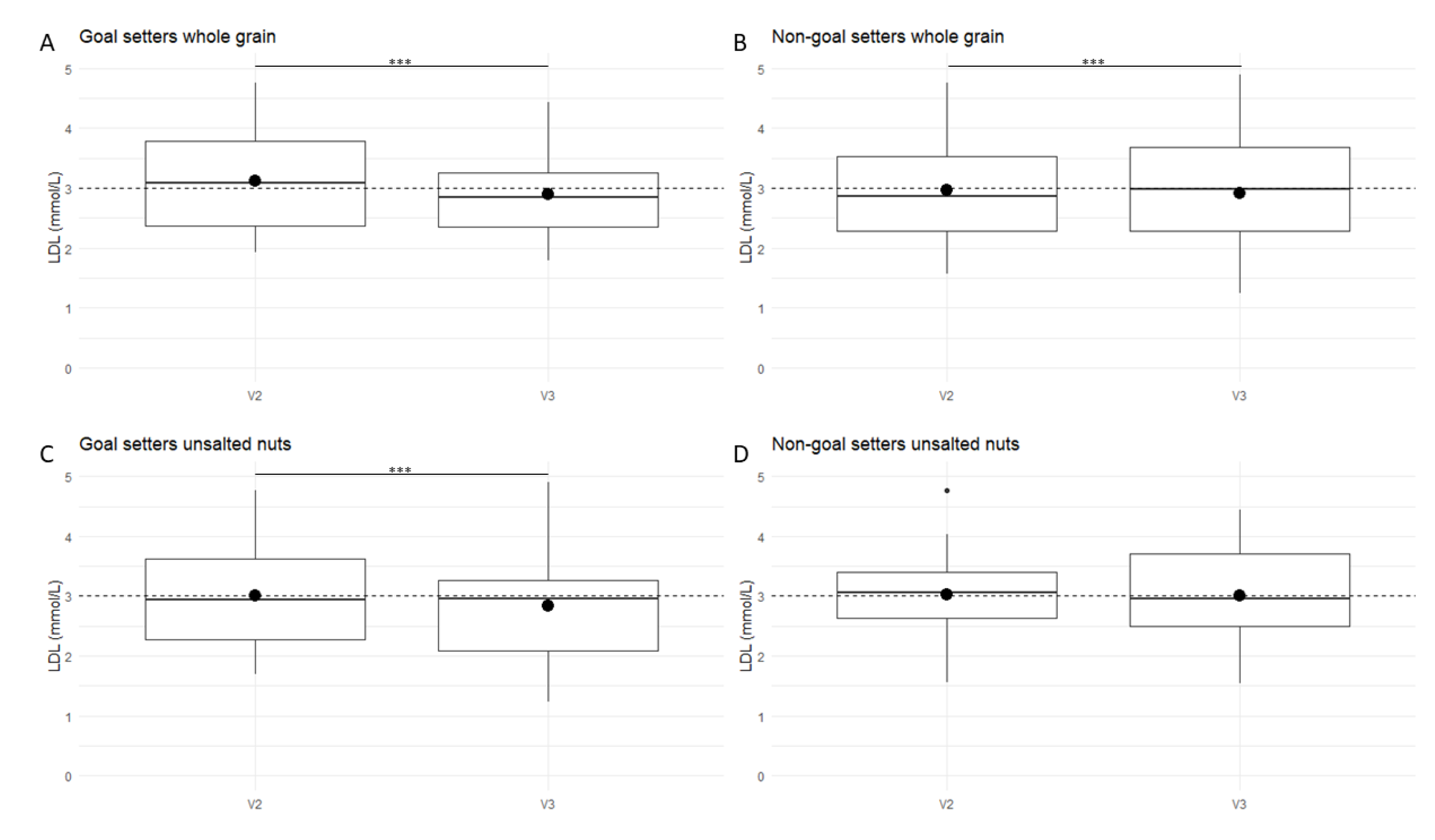
3.3. The Effect of Goal-Setting on Nutrition Intake Status and Health Parameters in the PNA Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rieken, M.; Struckmann, V.; Dyakova, M.; Melchieorre, M.G.; Rissanen, S.; van Ginneken, E.; On the Behalf of the ICARE4EU Partners. ICARE 4EU: Improving Care for People with Multiple Chronic Condition in Europe. Eurohealth (Lond.) 2013, 19, 29–31. [Google Scholar]
- Agha, M.; Agha, R. The Rising Prevalence of Obesity: Part A: Impact on Public Health. Int. J. Surg. Oncol. 2017, 2, e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Andersen, C.J.; Fernandez, M.L. Dietary Strategies to Reduce Metabolic Syndrome. Rev. Endocr. Metab. Disord. 2013, 14, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.-M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The Effect of Mediterranean Diet on Metabolic Syndrome and Its Components: A Meta-Analysis of 50 Studies and 534,906 Individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [Green Version]
- Lock, K.; Pomerleau, J.; Causer, L.; Altmann, D.R.; McKee, M. The Global Burden of Disease Attributable to Low Consumption of Fruit and Vegetables: Implications for the Global Strategy on Diet. Bull. World Health Organ. 2005, 83, 100–108. [Google Scholar]
- Lagström, H.; Stenholm, S.; Akbaraly, T.; Pentti, J.; Vahtera, J.; Kivimäki, M.; Head, J. Diet Quality as a Predictor of Cardiometabolic Disease–Free Life Expectancy: The Whitehall II Cohort Study. Am. J. Clin. Nutr. 2020, 111, 787–794. [Google Scholar] [CrossRef]
- Kimokoti, R.W.; Millen, B.E. Nutrition for the Prevention of Chronic Diseases. Med. Clin. N. Am. 2016. [Google Scholar] [CrossRef]
- Agriculture., U. S. D. of H. and H. S. and U. S. D. of. 2015–2020 Dietary Guidelines for Americans. 8th Edition. Available online: https://health.gov/our-work/food-nutrition/2015-2020-dietary-guidelines/guidelines/chapter-2/current-eating-patterns-in-the-united-states/ (accessed on 14 April 2020).
- Bechthold, A.; Boeing, H.; Tetens, I.; Schwingshackl, L.; Nöthlings, U. Perspective: Food-Based Dietary Guidelines in Europe—Scientific Concepts, Current Status, and Perspectives. Adv. Nutr. 2018, 9, 544–560. [Google Scholar] [CrossRef]
- Brug, J.; Campbell, M.; van Assema, P. The Application and Impact of Computer-Generated Personalized Nutrition Education: A Review of the Literature. Patient Educ. Couns. 1999, 36, 145–156. [Google Scholar] [CrossRef]
- Ordovas, J.M.; Ferguson, L.R.; Tai, E.S.; Mathers, J.C. Personalised Nutrition and Health. BMJ 2018, 361, bmj-k2173. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N. Individualised Nutritional Support in Medical Inpatients at Nutritional Risk: A Randomised Clinical Trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A Meta-Analysis of Computer-Tailored Interventions for Health Behavior Change. Prev. Med. (Baltim) 2010, 51, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celis-Morales, C.; Livingstone, K.M.; Marsaux, C.F.M.; Macready, A.L.; Fallaize, R.; O’Donovan, C.B.; Woolhead, C.; Forster, H.; Walsh, M.C.; Navas-Carretero, S. Effect of Personalized Nutrition on Health-Related Behaviour Change: Evidence from the Food4me European Randomized Controlled Trial. Int. J. Epidemiol. 2016, 46, 578–588. [Google Scholar] [CrossRef] [Green Version]
- Fjeldsoe, B.S.; Marshall, A.L.; Miller, Y.D. Behavior Change Interventions Delivered by Mobile Telephone Short-Message Service. Am. J. Prev. Med. 2009, 36, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.H.; Anthony, J.C.; Carvajal, R.; Chae, L.; Khoo, C.S.H.; Latulippe, M.E.; Matusheski, N.V.; McClung, H.L.; Rozga, M.; Schmid, C.H. Perspective: Guiding Principles for the Implementation of Personalized Nutrition Approaches That Benefit Health and Function. Adv. Nutr. 2020, 11, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Bouwman, J.; Vogels, J.T.W.E.; Wopereis, S.; Rubingh, C.M.; Bijlsma, S.; van Ommen, B. Visualization and Identification of Health Space, Based on Personalized Molecular Phenotype and Treatment Response to Relevant Underlying Biological Processes. BMC Med. Genomics 2012, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, S.; Horner, S.D. Barriers That Influence Eating Behaviors in Adolescents. J. Pediatr. Nurs. 2005, 20, 258–267. [Google Scholar] [CrossRef]
- Van Ommen, B.; Wopereis, S.; van Empelen, P.; van Keulen, H.M.; Otten, W.; Kasteleyn, M.; Molema, J.J.W.; de Hoogh, I.M.; Chavannes, N.H.; Numans, M.E.; et al. From Diabetes Care to Diabetes Cure—The Integration of Systems Biology, EHealth, and Behavioral Change. Front. Endocrinol. (Lausanne) 2018, 8, 381. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Taylor, D.S.; Smiciklas-Wright, H.; Mitchell, D.C.; Bekhuis, T.C.; Olson, B.H.; Slonim, A.B. High-Soluble-Fiber Foods in Conjunction with a Telephone-Based, Personalized Behavior Change Support Service Result in Favorable Changes in Lipids and Lifestyles after 7 Weeks. J. Am. Diet. Assoc. 2002, 102, 503–510. [Google Scholar] [CrossRef]
- Parekh, S.; Vandelanotte, C.; King, D.; Boyle, F.M. Design and Baseline Characteristics of the 10 Small Steps Study: A Randomised Controlled Trial of an Intervention to Promote Healthy Behaviour Using a Lifestyle Score and Personalised Feedback. BMC Public Health 2012, 12, 179. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.K.; DeVellis, B.M.; Strecher, V.J.; Ammerman, A.S.; DeVellis, R.F.; Sandler, R.S. Improving Dietary Behavior: The Effectiveness of Tailored Messages in Primary Care Settings. Am. J. Public Health 1994, 84, 783–787. [Google Scholar] [CrossRef] [Green Version]
- Gollwitzer, P.M. Implementation Intentions: Strong Effects of Simple Plans. Am. Psychol. 1999, 54, 493. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [Green Version]
- Adriaanse, M.A.; de Ridder, D.T.D.; de Wit, J.B.F. Finding the Critical Cue: Implementation Intentions to Change One’s Diet Work Best When Tailored to Personally Relevant Reasons for Unhealthy Eating. Personal. Soc. Psychol. Bull. 2009, 35, 60–71. [Google Scholar] [CrossRef]
- Doets, E.L.; de Hoogh, I.M.; Holthuysen, N.; Wopereis, S.; Verain, M.C.D.; van den Puttelaar, J.; Hogenelst, K.; Boorsma, A.; Bouwman, E.P.; Timmer, M. Beneficial Effect of Personalized Lifestyle Advice Compared to Generic Advice on Wellbeing among Dutch Seniors–An Explorative Study. Physiol. Behav. 2019, 210, 112642. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The Three-Factor Eating Questionnaire to Measure Dietary Restraint, Disinhibition and Hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Schoen, E.D.; Wopereis, S. Randomization of Subjects to Study-Arms of a Parallel Study in the Presence of Multiple Covariates. BMC Med. Res. Methodol. 2020. [Google Scholar] [CrossRef]
- Lally, P.; Van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How Are Habits Formed: Modelling Habit Formation in the Real World. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- Van den Broek, T.J.; Bakker, G.C.M.; Rubingh, C.M.; Bijlsma, S.; Stroeve, J.H.M.; van Ommen, B.; van Erk, M.J.; Wopereis, S. Ranges of Phenotypic Flexibility in Healthy Subjects. Genes Nutr. 2017, 12, 32. [Google Scholar] [CrossRef]
- Wopereis, S.; Stroeve, J.H.M.; Stafleu, A.; Bakker, G.C.M.; Burggraaf, J.; van Erk, M.J.; Pellis, L.; Boessen, R.; Kardinaal, A.A.F.; van Ommen, B. Multi-Parameter Comparison of a Standardized Mixed Meal Tolerance Test in Healthy and Type 2 Diabetic Subjects: The PhenFlex Challenge. Genes Nutr. 2017, 12. [Google Scholar] [CrossRef]
- Stroeve, J.H.M.; van Wietmarschen, H.; Kremer, B.H.A.; van Ommen, B.; Wopereis, S. Phenotypic Flexibility as a Measure of Health: The Optimal Nutritional Stress Response Test. Genes Nutr. 2015, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Manson, J.E.; Tinker, L.; Howard, B.V.; Kuller, L.H.; Nathan, L.; Rifai, N.; Liu, S. Insulin Sensitivity and Insulin Secretion Determined by Homeostasis Model Assessment and Risk of Diabetes in a Multiethnic Cohort of Women: The Women’s Health Initiative Observational Study. Diabetes Care 2007, 30, 1747–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrat, E.; Aubineau, N.; Maillot, M.; Derbord, É.; Barthes, P.; Lescuyer, J.-F.; Boisseau, N.; Peltier, S.L. Repeatability and Relative Validity of a Quantitative Food-Frequency Questionnaire among French Adults. Food Nutr. Res. 2012, 56, 18472. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Britton, A.; McKee, M.; Black, N.; McPherson, K.; Sanderson, C.; Bain, C. Threats to Applicability of Randomised Trials: Exclusions and Selective Participation. J. Health Serv. Res. Policy 1999, 4, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Voedingscentrum. Available online: https://www.voedingscentrum.nl/nl/gezond-eten-met-de-schijf-van-vijf.aspx (accessed on 14 April 2020).
- Manger Bouger. Available online: https://www.mangerbouger.fr/PNNS (accessed on 14 April 2020).
- Verhoeven, A.A.C.; Adriaanse, M.A.; de Vet, E.; Fennis, B.M.; de Ridder, D.T.D. Identifying the ‘If’ for ‘If-Then’ Plans: Combining Implementation Intentions with Cue-Monitoring Targeting Unhealthy Snacking Behaviour. Psychol. Health 2014, 29, 1476–1492. [Google Scholar] [CrossRef]
- De Vet, E.; Oenema, A.; Brug, J. More or Better: Do the Number and Specificity of Implementation Intentions Matter in Increasing Physical Activity? Psychol. Sport Exerc. 2011, 12, 471–477. [Google Scholar] [CrossRef]
- Bellisle, F. Why Should We Study Human Food Intake Behaviour? Nutr. Metab. Cardiovasc. Dis. 2003, 13, 189–193. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and Vegetable Intake and the Risk of Cardiovascular Disease, Total Cancer and All-Cause Mortality—a Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Zhan, J.; Liu, Y.-J.; Cai, L.-B.; Xu, F.-R.; Xie, T.; He, Q.-Q. Fruit and Vegetable Consumption and Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Cohort Studies. Crit. Rev. Food. Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and Vegetable Consumption and Mortality from All Causes, Cardiovascular Disease, and Cancer: Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, C.A.; Ravia, J. A Systematic Review of Behavioral Interventions to Promote Intake of Fruit and Vegetables. J. Am. Diet. Assoc. 2011, 111, 1523–1535. [Google Scholar] [CrossRef]
- Ammerman, A.S.; Lindquist, C.H.; Lohr, K.N.; Hersey, J. The Efficacy of Behavioral Interventions to Modify Dietary Fat and Fruit and Vegetable Intake: A Review of the Evidence. Prev. Med. (Baltim) 2002, 35, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Davy, B.M.; Davy, K.P.; Ho, R.C.; Beske, S.D.; Davrath, L.R.; Melby, C.L. High-Fiber Oat Cereal Compared with Wheat Cereal Consumption Favorably Alters LDL-Cholesterol Subclass and Particle Numbers in Middle-Aged and Older Men. Am. J. Clin. Nutr. 2002, 76, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Tapsell, L.C.; Sabaté, J. Nuts and Berries for Heart Health. Curr. Atheroscler. Rep. 2010, 12, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Guasch-Ferre, M.; Bullo, M.; Sabate, J. Nuts in the Prevention and Treatment of Metabolic Syndrome. Am. J. Clin. Nutr. 2014, 100, 399S–407S. [Google Scholar] [CrossRef] [Green Version]
- Ye, E.Q.; Chacko, S.A.; Chou, E.L.; Kugizaki, M.; Liu, S. Greater Whole-Grain Intake Is Associated with Lower Risk of Type 2 Diabetes, Cardiovascular Disease, and Weight Gain. J. Nutr. 2012, 142, 1304–1313. [Google Scholar] [CrossRef]
- Ritz, C.; Astrup, A.; Larsen, T.; Hjorth, M. Weight Loss at Your Fingertips: Personalized Nutrition with Fasting Glucose and Insulin Using a Novel Statistical Approach. Eur. J. Clin. Nutr. 2019, 73, 1529–1535. [Google Scholar] [CrossRef]
- Hoevenaars, F.P.M.; Esser, D.; Schutte, S.; Priebe, M.G.; Vonk, R.J.; van den Brink, W.J.; van der Kamp, J.-W.; Stroeve, J.H.M.; Afman, L.A.; Wopereis, S. Whole Grain Wheat Consumption Affects Postprandial Inflammatory Response in a Randomized Controlled Trial in Overweight and Obese Adults with Mild Hypercholesterolemia in the Graandioos Study. J. Nutr. 2019, 149, 2133–2144. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Population | Control | GNA | PNA |
|---|---|---|---|---|
| Total (n) | 155 | 52 | 52 | 51 |
| Sex, female, n (%) | 100 (64.5) | 34 (65.4) | 34 (65.4) | 32 (62.7) |
| Age (years) | 42.3 ± 12.1 | 42.8 ± 11.8 | 41.8 ± 12.1 | 42.3 ± 12.6 |
| Anthropometrics | ||||
| BMI (kg/m2) | 25.2 ± 3.6 | 25.1 ± 3.9 | 25.4 ± 3.7 | 25.1 ± 3.0 |
| Waist circumference (cm) | 83.4 ± 10.6 | 83.6 ± 11.3 | 83.5 ± 10.7 | 83.2 ± 10.0 |
| Hip circumference (cm) | 100.4 ± 7.8 | 100.2 ± 9.4 | 100.7 ± 7.8 | 100.3 ± 5.7 |
| Hemodynamics | ||||
| Diastolic BP (mmHg) | 73.1 ± 9.2 | 72.6 ± 9.6 | 73.9 ± 9.2 | 72.7 ± 8.8 |
| Systolic BP (mmHg) | 117.1 ± 13.0 | 116.7 ± 12.4 | 119.2 ± 14.4 | 115.6 ± 12.2 |
| Metabolic health fasting | ||||
| Total cholesterol (mmol/L) | 4.73 ± 0.99 | 4.64 ±1.05 | 4.90 ± 0.87 | 4.65 ± 1.04 |
| HDL cholesterol (mmol/L) | 1.48 ± 0.36 | 1.52 ± 0.39 | 1.50 ± 0.36 | 1.41 ± 0.34 |
| LDL cholesterol (mmol/L) | 2.81 ± 0.84 | 2.69 ± 0.81 | 2.96 ± 0.81 | 2.78 ± 0.89 |
| Triglycerides (mmol/L) | 0.29 ± 0.09 | 0.29 ± 0.09 | 0.29 ± 0.09 | 0.29 ± 0.1 |
| HbA1c (%) | 5.20 ± 0.24 | 5.21 ± 0.25 | 5.16 ± 0.25 | 5.22 ± 0.23 |
| NEFA (mmol/L) | 0.41 ± 0.19 | 0.41 ± 0.19 | 0.43 ± 0.21 | 0.37 ± 0.13 |
| Glucose and Insulin-related indices | ||||
| HOMA-IR | 1.58 ± 1.09 | 1.52 ± 1.14 | 1.61 ± 1.05 | 1.61 ± 1.10 |
| Health space analysis | ||||
| Metabolic age | 41.47 ± 11.49 | 41.29 ± 10.90 | 41.62 ± 10.48 | 41.51 ± 13.15 |
| Control | GNA | PNA | Interaction Effect | Interaction Effect | ||||
|---|---|---|---|---|---|---|---|---|
| Variables | V2 | V3 | V2 | V3 | V2 | V3 | PNA vs. control × Time | PNA vs. GNA × Time |
| Anthropometrics | ||||||||
| BMI (kg/m2) | 25.2 ± 4.0 | 25.4 ± 4.1 | 25.3 ± 3.7 | 25.3 ± 3.6 | 25.1 ± 3.0 | 25.1 ± 3.1 | 0.22 | 0.85 |
| Waist (cm) | 83.2 ± 11.1 | 83.0 ± 11.4 | 83.4 ± 10.8 | 82.6 ± 10.4 | 83.3 ± 10.1 | 82.5 ± 9.9 | 0.18 | 0.93 |
| Hip (cm) | 100.1 ± 9.4 | 99.6 ± 9.6 | 100.68 ± 8.0 | 99.8 ± 7.8 | 100.5 ± 5.7 | 99.8 ± 5.9 | 0.56 | 0.52 |
| Physical activity | ||||||||
| Metabolic equivalent of task (MET) per day | 732 ± 598 | 801 ± 777 | 1113 ±1005 | 972 ± 888 | 859 ± 609 | 842 ± 19 | 0.49 | 0.52 |
| Hemodynamics | ||||||||
| Diastolic BP (mmHg) | 73.0 ± 9.4 | 69.4 ± 10.4 | 73.9 ± 9.1 | 71.3 ± 10.3 | 72.7 ± 9.2 | 70.6 ± 9.0 | 0.35 | 0.72 |
| Systolic BP (mmHg) | 117.5 ± 13.1 | 119.5 ± 16.3 | 117.1 ± 14.8 | 121.3 ± 16.3 | 116.8 ± 1.7 | 120.9 ± 2.4 | 0.38 | 0.97 |
| Metabolic health fasting | ||||||||
| Total cholesterol (mmol/L) | 4.89 ± 1.13 | 4.84 ± 1.05 | 5.31 ± 1.09 | 5.19 ± 1.02 | 5.03 ± 1.07 | 4.81 ± 1.01 | 0.10 | 0.32 |
| HDL cholesterol (mmol/L) | 1.52 ± 0.37 | 1.52 ± 0.37 | 1.51 ± 0.35 | 1.54 ± 0.38 | 1.44 ± 0.34 | 1.41 ± 0.33 | 0.31 | 0.06 |
| LDL cholesterol (mmol/L) | 2.90 ± 0.92 | 2.86 ± 0.83 | 3.29 ± 0.96 | 3.18 ± 0.92 | 3.09 ± 0.89 | 2.95 ± 0.88 | 0.23 | 0.65 |
| Triglycerides (mmol/L) | 0.29 ± 0.11 | 0.29 ± 0.10 | 0.31 ± 0.11 | 0.3 ± 0.08 | 0.3 ± 0.11 | 0.29 ± 0.09 | 0.38 | 0.85 |
| HbA1c (%) | 5.27 ± 0.26 | 5.11 ± 0.28 | 5.25 ± 0.27 | 5.06 ± 0.25 | 5.25 ± 0.25 | 5.14 ± 0.24 | 0.39 | 0.10 |
| Glucose and Insulin-related indices | ||||||||
| HOMA-IR | 1.82 ± 1.07 | 1.88 ± 1.18 | 2.03 ± 2.13 | 1.90 ± 1.83 | 1.91 ± 1.61 | 2.04 ± 1.57 | 0.85 | 0.40 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoevenaars, F.P.M.; Berendsen, C.M.M.; Pasman, W.J.; van den Broek, T.J.; Barrat, E.; de Hoogh, I.M.; Wopereis, S. Evaluation of Food-Intake Behavior in a Healthy Population: Personalized vs. One-Size-Fits-All. Nutrients 2020, 12, 2819. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092819
Hoevenaars FPM, Berendsen CMM, Pasman WJ, van den Broek TJ, Barrat E, de Hoogh IM, Wopereis S. Evaluation of Food-Intake Behavior in a Healthy Population: Personalized vs. One-Size-Fits-All. Nutrients. 2020; 12(9):2819. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092819
Chicago/Turabian StyleHoevenaars, Femke P. M., Charlotte M. M. Berendsen, Wilrike J. Pasman, Tim J. van den Broek, Emmanuel Barrat, Iris M. de Hoogh, and Suzan Wopereis. 2020. "Evaluation of Food-Intake Behavior in a Healthy Population: Personalized vs. One-Size-Fits-All" Nutrients 12, no. 9: 2819. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092819