
Are Sensitivity to Punishment, Sensitivity to Reward and Effortful Control Transdiagnostic Mechanisms Underlying the Eating Disorder/Obesity Spectrum?

 , ,
, ,
Abstract
:1. Introduction
1.1. Punishment Sensitivity
1.2. Reward Sensitivity
1.3. Effortful Control
1.4. The Present Study
2. Materials and Methods
2.1. Participants & Procedure
2.2. Instruments
2.3. Analyses
3. Results
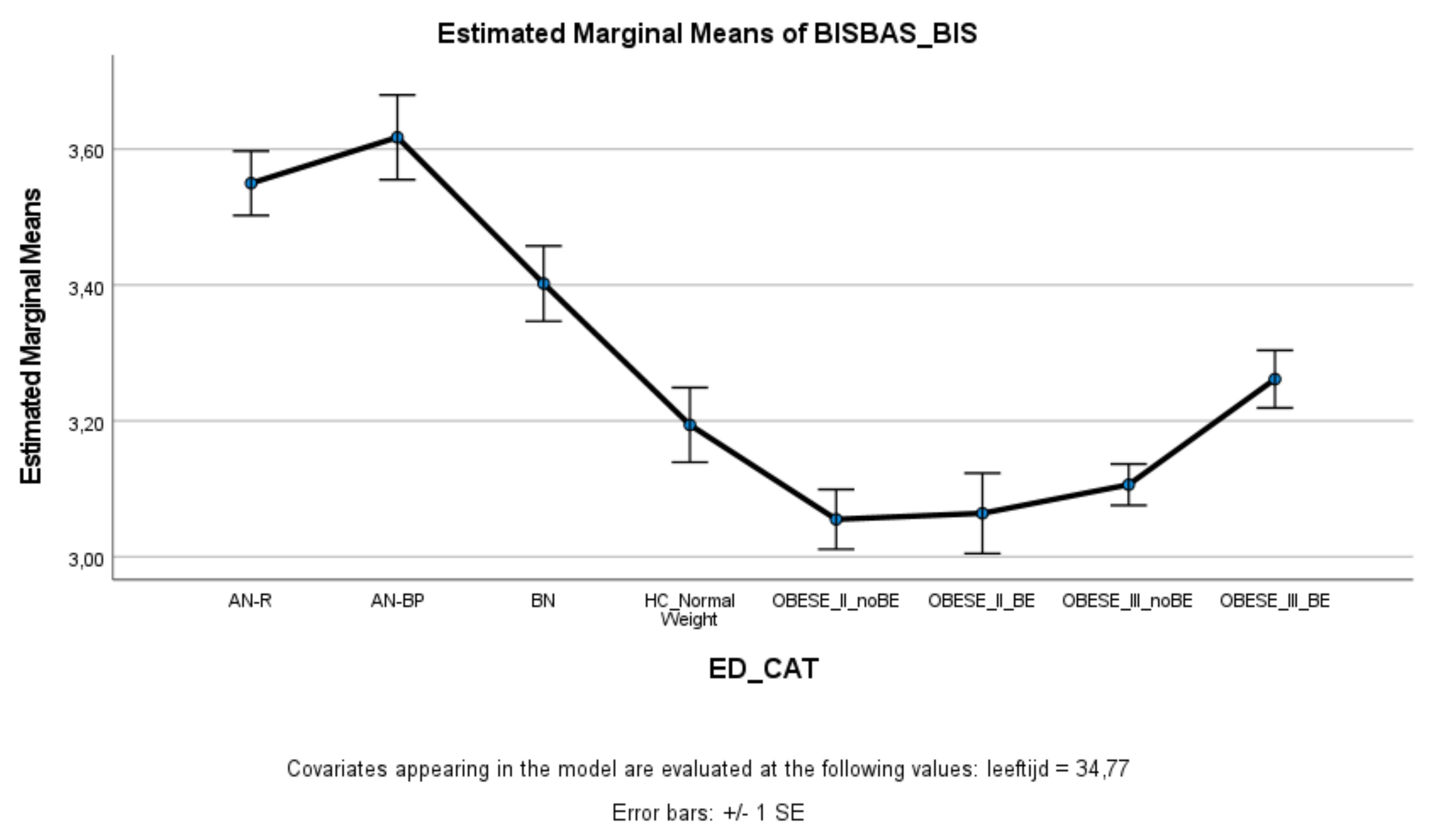
3.1. Punishment Sensitivity
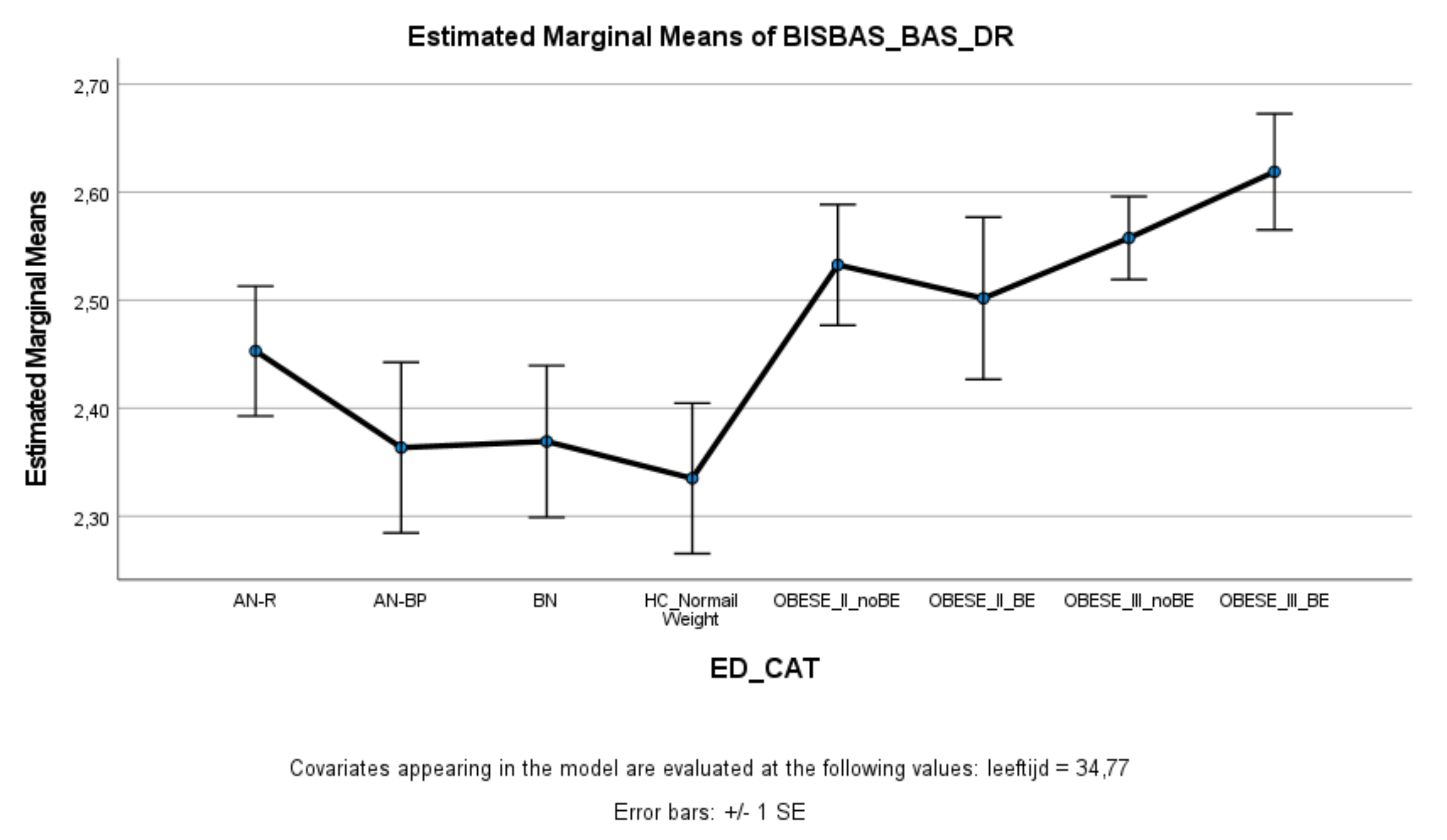
3.2. Reward Sensitivity
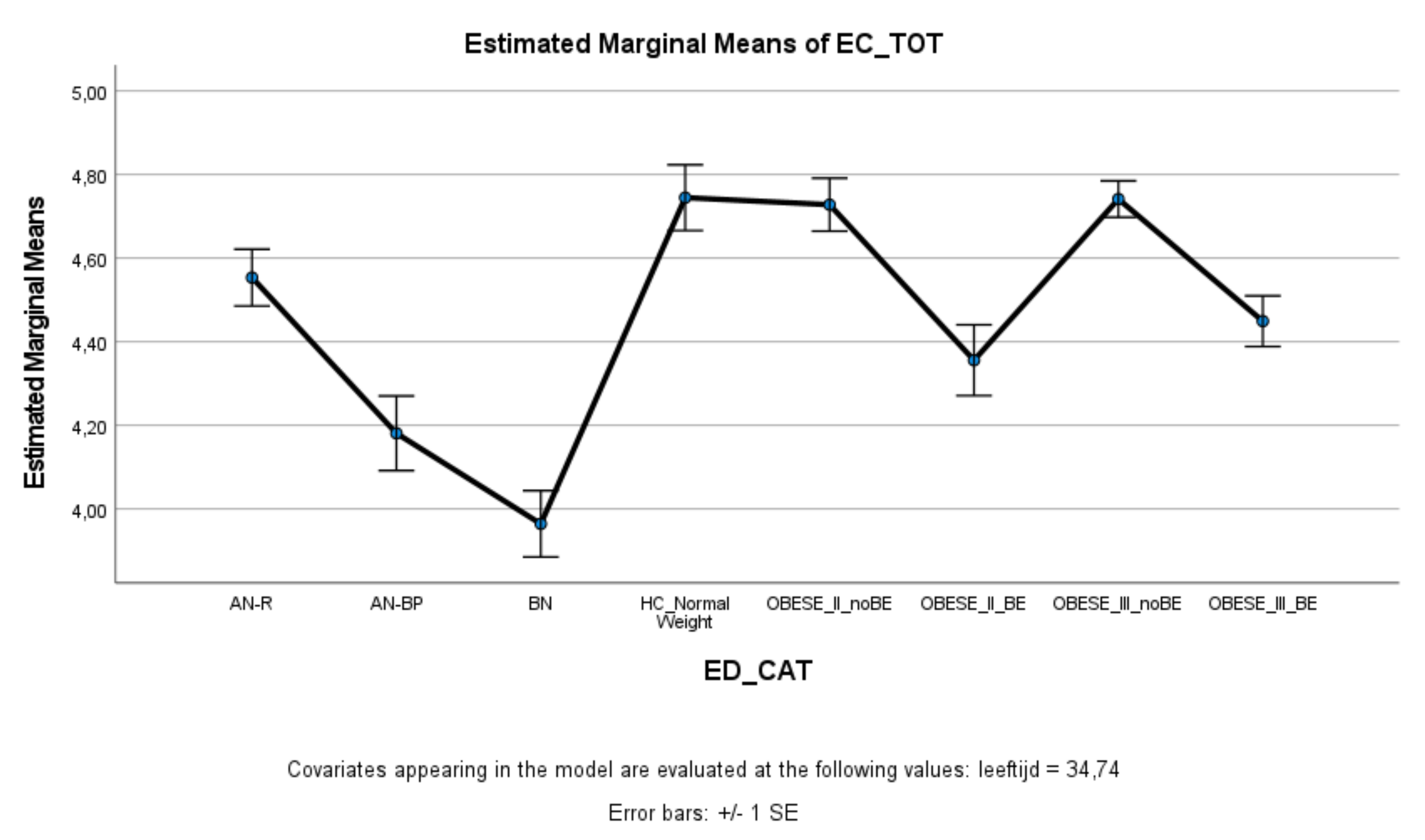
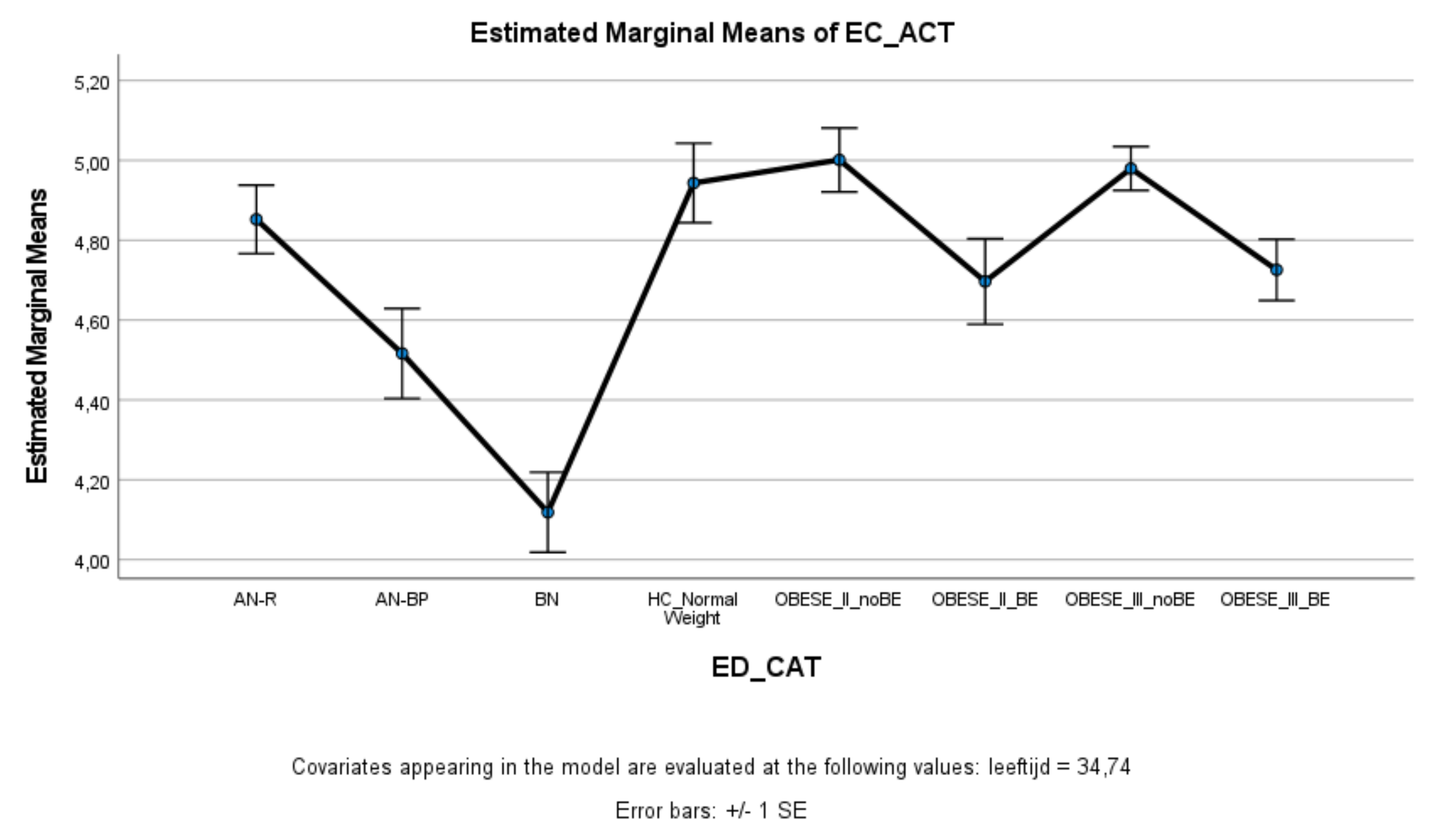
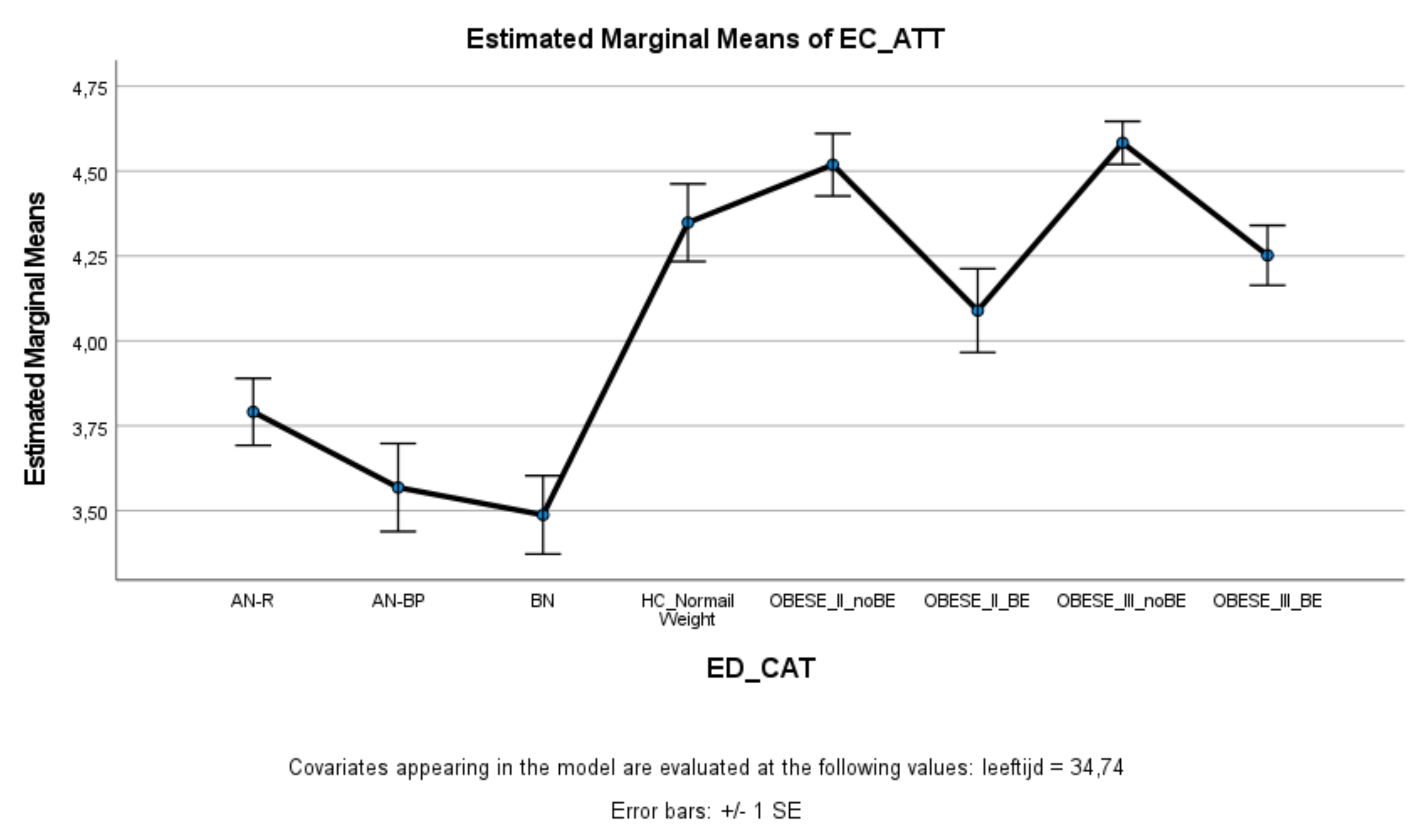
3.3. Effortful Control
4. Discussion
4.1. Sensitivity to Punishment
4.2. Effortful Control
4.3. Reward Sensitivity
4.4. Clinical Implications
4.5. Limitations and Suggestions for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Penñas-Lledoó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil de Bernabé, M.M.; et al. Lifetime Obesity in Patients with Eating Disorders: Increasing Prevalence, Clinical and Personality Correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, C.; Backholer, K.; Gearon, E.; Stevenson, C.; Swinburn, B.; Moodie, M.; Carter, R.; Peeters, A. Prevalence of class-I, class-II and class-III obesity in Australian adults between 1995 and 2011–12. Obes. Res. Clin. Pract. 2015, 9, 553–562. [Google Scholar] [CrossRef]
- Wu, M.; Brockmeyer, T.; Hartmann, M.; Skunde, M.; Herzog, W.; Friederich, H.-C. Set-shifting ability across the spectrum of eating disorders and in overweight and obesity: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 3365–3385. [Google Scholar] [CrossRef]
- Heshka, S.; Allison, D. Is obesity a disease? Int. J. Obes. 2001, 25, 1401–1404. [Google Scholar] [CrossRef] [Green Version]
- Fassino, S.; Leombruni, P.; Pierò, A.; Abbata-Daga, G.A.; Amianto, F.; Rovera, G.; Rovera, G.G. Temperament and character in obese women with and without binge eating disorder. Compr. Psychiatry 2002, 43, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Claes, L.; Mitchell, J.E.; Fischer, J.; Horbach, T.; De Zwaan, M. Binge Eating and Temperament in Morbidly Obese Prebariatric Surgery Patients. Eur. Eat. Disord. Rev. 2011, 20, e91–e95. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, A.; Federbusch, M.; Grellmann, C.; Villringer, A.; Horstmann, A. Body weight status, eating behavior, sensitivity to reward/punishment, and gender: Relationships and interdependencies. Front. Psychol. 2014, 5, 1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matton, A.; Goossens, L.; Vervaet, M.; Braet, C. Temperamental differences between adolescents and young adults with or without an eating disorder. Compr. Psychiatry 2015, 56, 229–238. [Google Scholar] [CrossRef]
- Strack, F.; Deutsch, R. Reflective and Impulsive Determinants of Social Behavior. Personal. Soc. Psychol. Rev. 2004, 8, 220–247. [Google Scholar] [CrossRef] [Green Version]
- Gray, J.A. The psychophysiological basis of introversion-extraversion. Behav. Res. Ther. 1970, 8, 249–266. [Google Scholar] [CrossRef]
- Gray, J.A. The Neuropsychology of Anxiety: An Inquiry into the Functions of the Septal–Hippocampal System; Oxford University Press: Oxford, UK, 1982. [Google Scholar]
- Claes, L.; Bijttebier, P.; Mitchell, J.E.; De Zwaan, M.; Mueller, A. The relationship between compulsive buying, eating disorder symptoms, and temperament in a sample of female students. Compr. Psychiatry 2011, 52, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Mardaga, S.; Hansenne, M. Relationships between Cloninger’s biosocial model of personality and the behavioral inhibition/approach systems (BIS/BAS). Personal. Individ. Differ. 2007, 42, 715–722. [Google Scholar] [CrossRef]
- Smits, D.J.M.; De Boeck, P. From BIS/BAS to the big five. Eur. J. Personal. 2006, 20, 255–270. [Google Scholar] [CrossRef]
- Gray, J.A. The Psychology of Fear and Stress; Cambridge University Press: Cambridge, UK, 1987. [Google Scholar]
- Gray, J.A.; McNaughton, N. The Neuropsychology of Anxiety: An Inquiry into the Functions of the Septo-Hippocampal System; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Nigg, J.T. On inhibition/disinhibition in developmental psychopathology: Views from cognitive and personality psychology and a working inhibition taxonomy. Psychol. Bull. 2000, 126, 220–246. [Google Scholar] [CrossRef]
- Rothbart, M.K. Temperament and Development. In Temperament in Childhood; Kohnstamm, G.A., Bates, J.E., Rothbart, M.K., Eds.; John Wiley: Hoboken, NJ, USA, 1989; pp. 187–247. [Google Scholar]
- Baumeister, R.F.; Heatherton, T.F.; Tice, D.M. Losing Control: How and Why People Fail at Self-Regulation; Academic Press: Cambridge, MA, USA, 1994. [Google Scholar]
- Matton, A.; Goossens, L.; Vervaet, M.; Braet, C. Effortful control as a moderator in the association between punishment and reward sensitivity and eating styles in adolescent boys and girls. Appetite 2017, 111, 177–186. [Google Scholar] [CrossRef]
- Carver, C.S.; White, T.L. Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS Scales. J. Personal. Soc. Psychol. 1994, 67, 319–333. [Google Scholar] [CrossRef]
- Torrubia, R.; Ávila, C.; Molto, J.; Caseras, X. The Sensitivity to Punishment and Sensitivity to Reward Questionnaire (SPSRQ) as a measure of Gray’s anxiety and impulsivity dimensions. Personal. Individ. Differ. 2001, 31, 837–862. [Google Scholar] [CrossRef]
- Claes, L.; Nederkoorn, C.; Vandereycken, W.; Guerrieri, R.; Vertommen, H. Impulsiveness and lack of inhibitory control in eating disorders. Eat. Behav. 2006, 7, 196–203. [Google Scholar] [CrossRef]
- Glashouwer, K.A.; Bloot, L.; Veenstra, E.M.; Franken, I.H.; De Jong, P.J. Heightened sensitivity to punishment and reward in anorexia nervosa. Appetite 2014, 75, 97–102. [Google Scholar] [CrossRef]
- Harrison, A.; Treasure, J.; Smillie, L. Approach and avoidance motivation in eating disorders. Psychiatry Res. 2011, 188, 396–401. [Google Scholar] [CrossRef]
- Jappe, L.M.; Frank, G.K.; Bs, M.E.S.; Rollin, M.D.; Pryor, T.; Hagman, J.; Yang, T.T.; Davis, E. Heightened sensitivity to reward and punishment in anorexia nervosa. Int. J. Eat. Disord. 2011, 44, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Jonker, N.C.; Glashouwer, K.A.; Hoekzema, A.; Ostafin, B.D.; De Jong, P.J. Heightened self-reported punishment sensitivity, but no differential attention to cues signaling punishment or reward in anorexia nervosa. PLoS ONE 2020, 15, e0229742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kane, T.A.; Loxton, N.; Staiger, P.K.; Dawe, S. Does the tendency to act impulsively underlie binge eating and alcohol use problems? An empirical investigation. Personal. Individ. Differ. 2004, 36, 83–94. [Google Scholar] [CrossRef]
- Monteleone, P.; Scognamiglio, P.; Monteleone, A.M.; Perillo, D.; Maj, M. Cortisol awakening response in patients with anorexia nervosa or bulimia nervosa: Relationships to sensitivity to reward and sensitivity to punishment. Psychol. Med. 2014, 44, 2653–2660. [Google Scholar] [CrossRef]
- Beck, I.; Smits, D.; Claes, L.; Vandereycken, W.; Bijttebier, P. Psychometric evaluation of the behavioral inhibition/behavioral activation system scales and the sensitivity to punishment and sensitivity to reward questionnaire in a sample of eating disordered patients. Personal. Individ. Differ. 2009, 47, 407–412. [Google Scholar] [CrossRef]
- Claes, L.; Mitchell, J.E.; Vandereycken, W. Out of control? Inhibition processes in eating disorders from a personality and cognitive perspective. Int. J. Eat. Disord. 2011, 45, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Danner, U.N.; Ouwehand, C.; Haastert, N.L.; Hornsveld, H.; Ridder, D.T.D. Decision-making Impairments in Women with Binge Eating Disorder in Comparison with Obese and Normal Weight Women. Eur. Eat. Disord. Rev. 2011, 20, e56–e62. [Google Scholar] [CrossRef]
- Schienle, A.; Schäfer, A.; Hermann, A.; Vaitl, D. Binge-Eating Disorder: Reward Sensitivity and Brain Activation to Images of Food. Biol. Psychiatry 2009, 65, 654–661. [Google Scholar] [CrossRef]
- Davis, C.; Levitan, R.D.; Carter, J.; Kaplan, A.S.; Reid, C.; Curtis, C.; Patte, K.; Kennedy, J.L. Personality and eating behaviors: A case–control study of binge eating disorder. Int. J. Eat. Disord. 2007, 41, 243–250. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Jonker, N.C.; Bennik, E.C.; de Jong, P.J. Why Dieters Succeed or Fail: The Relationship Between Reward and Punishment Sensitivity and Restrained Eating and Dieting Success. Front. Psychol. 2021, 12, 636432. [Google Scholar] [CrossRef]
- Ruscitti, C.; Rufino, K.; Goodwin, N.; Wagner, R. Difficulties in emotion regulation in patients with eating disorders. Bord. Personal. Disord. Emot. Dysregul. 2016, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Davis, C. A Narrative Review of Binge Eating and Addictive Behaviors: Shared Associations with Seasonality and Personality Factors. Front. Psychiatry 2013, 4, 183. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Fox, J. Sensitivity to reward and body mass index (BMI): Evidence for a non-linear relationship. Appetite 2008, 50, 43–49. [Google Scholar] [CrossRef]
- Evans, D.E.; Rothbart, M.K. Developing a model for adult temperament. J. Res. Personal. 2007, 41, 868–888. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Ahadi, S.A.; Evans, D.E. Temperament and personality: Origins and outcomes. J. Personal. Soc. Psychol. 2000, 78, 122–135. [Google Scholar] [CrossRef]
- Bruch, H. Anorexia nervosa: The Golden Cage; Harvard University Press: Cambridge, MA, USA, 1978. [Google Scholar]
- Crisp, A.H. Anorexia nervosa: Patient’s Logbook; Erlbaum: Hove, UK, 1995. [Google Scholar]
- Garfinkel, P.E.; Garner, D.M. Anorexia Nervosa: A Multidimensional Perspective; Brunner/Mazel: New York, NY, USA, 1982. [Google Scholar]
- Selvine-Palazolli, M. Self-starvation: From the Intrapsychic to the Transpersonal Approach to Anorexia Nervosa; Human Context Books: London, UK, 1974. [Google Scholar]
- Button, E. Personal Construct Theory and Mental Health: Theory, Research and Practice; Croom Helm: London, UK, 1985. [Google Scholar]
- Dalle Grave, R.D.; Calugi, S.; El Ghoch, M.; Marzocchi, R.; Marchesini, G. Personality Traits in Obesity Associated with Binge Eating and/or Night Eating. Curr. Obes. Rep. 2013, 3, 120–126. [Google Scholar] [CrossRef]
- Bijttebier, P.; Beck, I.; Claes, L.; Vandereycken, W. Gray’s Reinforcement Sensitivity Theory as a framework for research on personality–psychopathology associations. Clin. Psychol. Rev. 2009, 29, 421–430. [Google Scholar] [CrossRef]
- Harrison, A.; O’Brien, N.; Lopez, C.; Treasure, J. Sensitivity to reward and punishment in eating disorders. Psychiatry Res. 2010, 177, 1–11. [Google Scholar] [CrossRef]
- Vandereycken, W. The eating disorder evaluation scale (EDES). Eat. Disord. 1993, 1, 115–122. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorder psychopathology: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar]
- Swinbourne, J.; Hunt, C.; Abbott, M.; Russell, J.; St Clare, T.S.; Touyz, S. The comorbidity between eating disorders and anxiety disorders: Prevalence in an eating disorder sample and anxiety disorder sample. Aust. N. Z. J. Psychiatry 2012, 46, 118–131. [Google Scholar] [CrossRef]
- Wierenga, C.E.; Ely, A.; Bischoff-Grethe, A.; Bailer, U.F.; Simmons, A.N.; Kaye, W.H. Are Extremes of Consumption in Eating Disorders Related to an Altered Balance between Reward and Inhibition? Front. Behav. Neurosci. 2014, 8, 410. [Google Scholar] [CrossRef] [Green Version]
- De Zwaan, M.; Gruss, B.; Müller, A.; Philipsen, A.; Graap, H.; Martin, A.; Glaesmer, H.; Hilbert, A. Association between Obesity and Adult Attention-Deficit/Hyperactivity Disorder in a German Community-Based Sample (ADHD). Obes. Facts 2011, 4, 204–211. [Google Scholar] [CrossRef]
- Van Der Oord, S.; Braet, C.; Cortese, S.; Claes, L. Testing the dual pathway model of ADHD in obesity: A pilot study. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 23, 507–512. [Google Scholar] [CrossRef]
- Atwood, M.E.; Friedman, A. A systematic review of enhanced cognitive behavioral therapy (CBT-E) for eating disorders. Int. J. Eat. Disord. 2019, 53, 311–330. [Google Scholar] [CrossRef]
- Fairburn, C.G. Cognitive Behavior Therapy and Eating Disorders; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Wisniewski, L.; Kelly, E. The application of dialectical behavior therapy to the treatment of eating disorders. Cogn. Behav. Pract. 2003, 10, 131–138. [Google Scholar] [CrossRef]
- Wisniewski, L.; Safer, D.; Chen, E.; Dimeff, L.A.; Koerner, K. Dialectical behavior therapy and eating disorders. In Dialectical Behavior Therapy in Clinical Practice: Applications Across Disorders and Settings; Dimeff, L.A., Koerner, K., Eds.; Guilford Press: New York, NY, USA, 2007; pp. 174–221. [Google Scholar]
- Grave, R.D.; Calugi, S.; El Ghoch, M. Are Personality Characteristics as Measured by the Temperament and Character Inventory (TCI) Associated with Obesity Treatment Outcomes? A Systematic Review. Curr. Obes. Rep. 2018, 7, 27–36. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Pietrabissa, G.; Manzoni, G.M.; Cattivelli, R.; Rossi, A.; Novelli, M.; Varallo, G.; Molinari, E. Cognitive behavioral therapy to aid weight loss in obese patients: Current perspectives. Psychol. Res. Behav. Manag. 2017, 10, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Dalle Grave, R.; Sartirana, M.; El Ghoch, M.; Calugi, S. Treating Obesity with Personalized Cognitive Behavioral Therapy; Springer: New York, NY, USA; Berlin, Germany, 2018. [Google Scholar]
- Kaye, W.H.; Wierenga, C.E.; Knatz, S.; Liang, J.; Boutelle, K.; Hill, L.; Eisler, I. Temperament-based Treatment for Anorexia Nervosa. Eur. Eat. Disord. Rev. 2014, 23, 12–18. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AN-R (N = 12) | AN-BP (N = 69) | BN (N = 89) | HC (N = 84) | Class II Obesity − BE (N = 138) | Class II Obesity + BE (N = 72) | Class III Obesity − BE (N = 289) | Class III Obesity + BE (N = 140) | F | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | ||
| Age | 24.60 a | (6.17) | 24.52 b | (5.04) | 24.41 c | (5.22) | 38.05 a,b,c,d | (12.15) | 42.07 a,b,c,d,e | (10.19) | 37.19 a,b,c,e,f | (11.07) | 39.42 a,b,c,e,g | (12.74) | 35.53 a,b,c,e,g | (11.75) | 58.55 *** |
| BMI | 15.40 a | (1.66) | 16.27 b | (1.67) | 20.96 a,b,c | (1.77) | 21.65 a,b,d | (1.74) | 37.52 a,b,c,d,e | (1.45) | 37.78 a,b,c,d,f | (1.58) | 43.74 a,b,c,d,e,f,g | (4.03) | 43.89 a,b,c,d,e,f | (4.32) | 2223.92 *** |
| M | (SE) | M | (SE) | M | (SE) | M | (SE) | M | (SE) | M | (SE) | M | (SE) | M | (SE) | ||
| BIS-TOT | 3.55 a | (0.05) | 3.62 b | (0.06) | 3.40 a,b,c | (0.06) | 3.19 a,b,c,d | (0.06) | 3.06 a,b,c,d,e | (0.04) | 3.06 a,b,c,f | (0.06) | 3.11 a,b,c,g | (0.03) | 3.26 a,b,c,e,f,g | (0.04) | 15.33 *** |
| BAS-TOT | 2.79 | (0.04) | 2.74 | (0.06) | 2.78 | (0.05) | 2.75 | (0.05) | 2.79 | (0.04) | 2.85 | (0.05) | 2.85 | (0.03) | 2.92 | (0.04) | 1.91 |
| BAS-DR | 2.45 a | (0.06) | 2.36 b | (0.08) | 2.37c | (0.07) | 2.34 d | (0.07) | 2.53 d,e | (0.06) | 2.50 f | (0.08) | 2.56 b,c,d,g | (0.04) | 2.62 a,b,c,d | (0.05) | 2.70 ** |
| BAS-FS | 2.60 | (0.05) | 2.67 | (0.07) | 2.71 | (0.06) | 2.65 | (0.06) | 2.60 | (0.05) | 2.74 | (0.06) | 2.64 | (0.03) | 2.76 | (0.05) | 1.61 |
| BAS-RR | 3.20 | (0.04) | 3.10 | (0.06) | 3.16 | (0.05) | 3.17 | (0.05) | 3.16 | (0.04) | 3.23 | (0.06) | 3.24 | (0.03) | 3.29 | (0.04) | 1.80 |
| EC-TOT | 4.55 a | (0.07) | 4.18 a,b | (0.09) | 3.96 a,c | (0.08) | 4.75 b,c,d | (0.08) | 4.73 b,c,e | (0.06) | 4.36 c,d,e,f | (0.09) | 4.74 a,b,c,f,g | (0.04) | 4.45 b,c,d,e,g | (0.06) | 14.45 *** |
| EC-INH | 4.81 a | (0.08) | 4.28 a,b | (0.11) | 4.16 a,c | (0.10) | 4.83 b,c,d | (0.10) | 4.61 b,c,e | (0.08) | 4.19 a,d,e,f | (0.11) | 4.62 b,c,f,g | (0.05) | 4.31 a,d,e,g | (0.08) | 9.15 *** |
| EC-ACT | 4.85 a | (0.09) | 4.52 a,b | (0.11) | 4.12 a,b,c | (0.10) | 4.94 b,c,d | (0.10) | 5.00 b,c,e | (0.08) | 4.70 c,e,f | (0.10) | 4.98 b,c,f,g | (0.06) | 4.73 c,e,g | (0.08) | 9.68 *** |
| EC-ATT | 3.79 a | (0.10) | 3.57 b | (0.13) | 3.49 a,c | (0.12) | 4.35 a,b,c,d | (0.11) | 4.52 a,b,c,e | (0.09) | 4.09 b,c,e,f | (0.12) | 4.58 a,b,c,f,g | (0.06) | 4.25 a,b,c,e,g | (0.09) | 14.85 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claes, L.; Kiekens, G.; Boekaerts, E.; Depestele, L.; Dierckx, E.; Gijbels, S.; Schoevaerts, K.; Luyckx, K. Are Sensitivity to Punishment, Sensitivity to Reward and Effortful Control Transdiagnostic Mechanisms Underlying the Eating Disorder/Obesity Spectrum? Nutrients 2021, 13, 3327. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103327
Claes L, Kiekens G, Boekaerts E, Depestele L, Dierckx E, Gijbels S, Schoevaerts K, Luyckx K. Are Sensitivity to Punishment, Sensitivity to Reward and Effortful Control Transdiagnostic Mechanisms Underlying the Eating Disorder/Obesity Spectrum? Nutrients. 2021; 13(10):3327. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103327
Chicago/Turabian StyleClaes, Laurence, Glenn Kiekens, Els Boekaerts, Lies Depestele, Eva Dierckx, Sylvia Gijbels, Katrien Schoevaerts, and Koen Luyckx. 2021. "Are Sensitivity to Punishment, Sensitivity to Reward and Effortful Control Transdiagnostic Mechanisms Underlying the Eating Disorder/Obesity Spectrum?" Nutrients 13, no. 10: 3327. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103327