
Translation of Two Healthy Eating and Active Living Support Programs for Parents of 2–6-Year-Old Children: Outcomes of the ‘Time for Healthy Habits’ Parallel Partially Randomised Preference Trial

 , , ,
, , , _Okely.png) , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
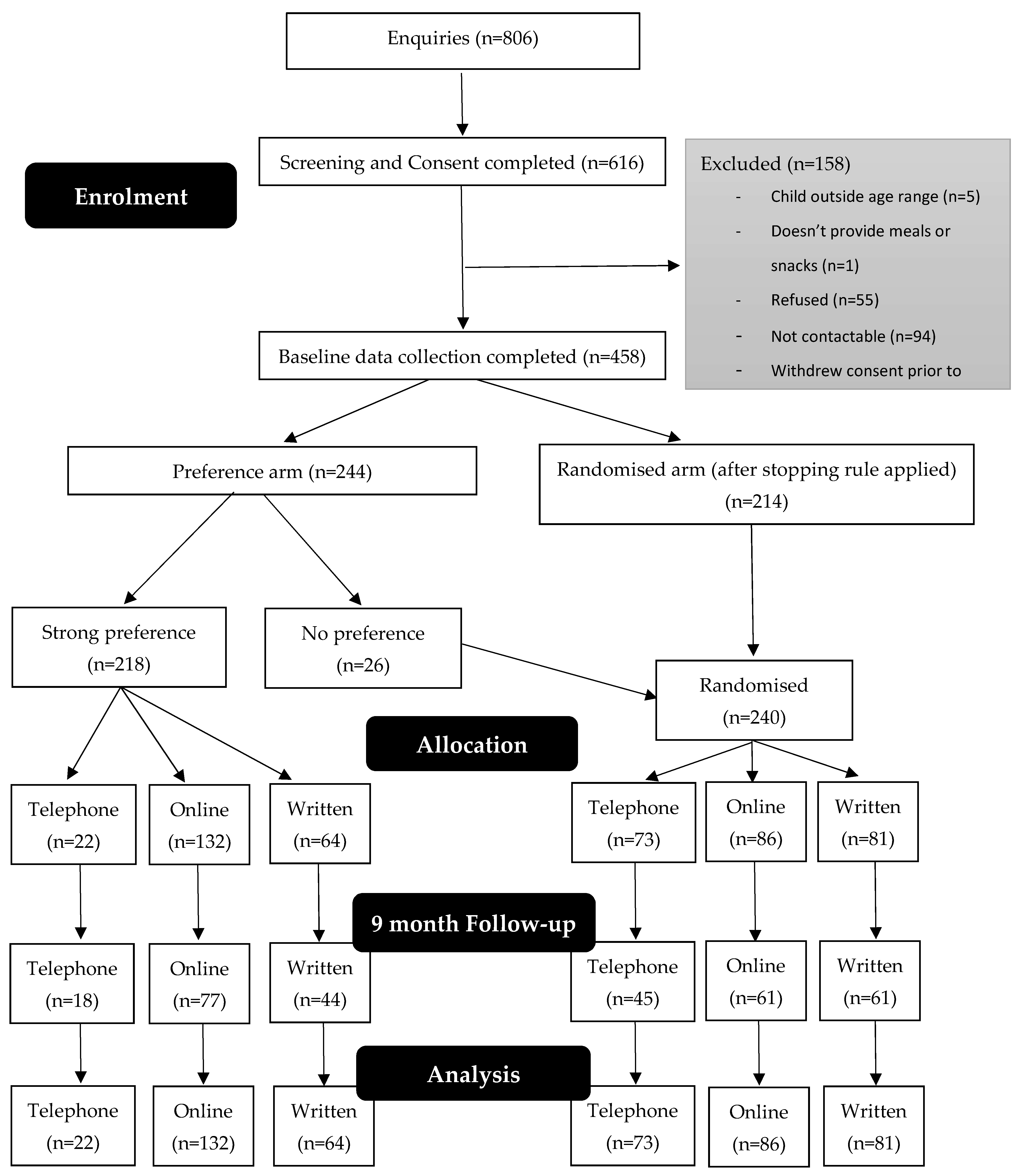
2.1. Study Design
2.2. Participant Recruitment and Eligibility Criteria
2.3. Randomisation and Blinding
2.4. Interventions
2.4.1. Healthy Habits Plus
2.4.2. Time2bHealthy
2.4.3. Active Control Group
2.5. Outcome Measures
2.5.1. Primary Outcome Measures
2.5.2. Secondary Outcome Measures
2.6. Power and Sample Size
2.7. Statistical Analyses
3. Results
3.1. Overview
3.2. Participant Characteristics
3.3. Primary Outcome
3.3.1. Primary Outcome Randomised Analyses
3.3.2. Primary Outcome Other Analyses
3.4. Secondary Outcomes
3.4.1. Secondary Outcome Randomised Analyses
3.4.2. Secondary Outcome Other Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Innes-Hughes, C.J.; Rissel, C.; Thomas, M.; Wolfenden, L. Reflections on the NSW Healthy Children Initiative: A comprehensive state-delivered childhood obesity prevention initiative. Public Health Res. Pract. 2019, 29, e2911908. [Google Scholar] [CrossRef] [Green Version]
- Summerbell, C.D.; Moore, H.J.; Vögele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Douthwaite, W.; Nixon, C.A.; Gibson, E.L. Evidence-based recommendations for the development of obesity prevention programs targeted at preschool children. Obes. Rev. 2012, 13, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Garnett, S.P.; Baur, L.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Effectiveness of Lifestyle Interventions in Child Obesity: Systematic Review with Meta-analysis. Pediatrics 2012, 130, e1647–e1671. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, Cd001871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, K.M.; Northern, J.J.; Lister, K.M.; Drummond, J.; O’Brien, W.H. A meta-analysis of family-behavioral weight-loss treatments for children. Clin. Psychol. Rev. 2007, 27, 240–249. [Google Scholar] [CrossRef]
- Grimes-Robison, C.; Evans, R.R. Benefits and barriers to medically supervised pediatric weight-management programs. J. Child Health Care 2008, 12, 329–343. [Google Scholar] [CrossRef] [PubMed]
- Fitch, A.; Fox, C.; Bauerly, K.; Gross, A.; Heim, C.; Judge-Dietz, J.; Kaufman, T.; Krych, E.; Kumar, S.; Landin, D.; et al. Prevention and Management of Obesity for Children and Adolescents; Institute for Clinical Systems Improvement: Bloomington, IN, USA, 2013. [Google Scholar]
- Golan, M.; Weizman, A. Familial approach to the treatment of childhood obesity: Conceptual mode. J. Nutr. Educ. 2001, 33, 102–107. [Google Scholar] [CrossRef]
- Wyse, R.J.; Wolfenden, L.; Campbell, E.; Campbell, K.J.; Wiggers, J.; Brennan, L.; Fletcher, A.; Bowman, J.; Heard, T.R. A cluster randomized controlled trial of a telephone-based parent intervention to increase preschoolers’ fruit and vegetable consumption. Am. J. Clin. Nutr. 2012, 96, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Hammersley, M.L.; Okely, A.D.; Batterham, M.J.; Jones, R.A. An Internet-Based Childhood Obesity Prevention Program (Time2bHealthy) for Parents of Preschool-Aged Children: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e11964. [Google Scholar] [CrossRef] [Green Version]
- Rychetnik, L.; Bauman, A.; Laws, R.; King, L.; Rissel, C.; Nutbeam, D.; Colagiuri, S.; Caterson, I. Translating research for evidence-based public health: Key concepts and future directions. J. Epidemiol. Community Health 2012, 66, 1187–1192. [Google Scholar] [CrossRef]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ 2015, 350, h2147. [Google Scholar] [CrossRef] [Green Version]
- Bradley-Gilbride, J.; Bradley, C. Partially Randomized Preference Trial Design. In Encyclopedia of Research Design, Partially Randomized Preference Trial Design; Salkind, C., Ed.; Sage: California, CA, USA, 2010; Volume 2, pp. 1009–1015. [Google Scholar]
- Torgerson, D.J.; Sibbald, B. Understanding controlled trials. What is a patient preference trial? BMJ 1998, 316, 360. [Google Scholar] [CrossRef] [Green Version]
- Hammersley, M.L.; Wyse, R.J.; Jones, R.A.; Wolfenden, L.; Yoong, S.; Stacey, F.; Eckermann, S.; Okely, A.D.; Innes-Hughes, C.; Li, V.; et al. Translation of two healthy eating and active living support programs for parents of 2-6 year old children: A parallel partially randomised preference trial protocol (the ‘time for healthy habits’ trial). BMC Public Health 2020, 20, 636. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar]
- Magarey, A.; Golley, R.; Spurrier, N.; Goodwin, E.; Ong, F. Reliability and validity of the Children’s Dietary Questionnaire; a new tool to measure children’s dietary patterns. Int. J. Pediatr. Obes. 2009, 4, 257–265. [Google Scholar] [CrossRef]
- Centre for Epidemiology and Evidence. 2009–2010 Summary Report from the New South Wales Child Health Survey; NSW Ministry of Health: Sydney, Australia, 2012.
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- World Health Organization. WHO BMI-for-Age (2–5 Years) Percentiles Tables; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- NSW Ministry of Health. NSW Population Health Survey; Ministry of Health: Sydney, Australia, 2012.
- Barr, M.; Baker, D.; Gorringe, M.; Fitsche, L. NSW Population Health Survey: Description of Methods; NSW Department of Health: Sydney, Australia, 2008.
- Australian Bureau of Statistics. National Nutrition and Physical Activity Survey; Australian Bureau of Statistics: Canberra, Australia, 2011.
- Bonuck, K.A.; Goodlin-Jones, B.L.; Schechter, C.; Owens, J. Modified Children’s sleep habits questionnaire for behavioral sleep problems: A validation study. Sleep Health 2017, 3, 136–141. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Australian 24-Hour Movement Guidelines for the Early Years (birth to 5 years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep; Australian Government Department of Health: Canberra, Australia, 2017.
- Mittal, R.; Harris, I.A.; Adie, S.; Naylor, J.M. Surgery for Type B Ankle Fracture Treatment: A Combined Randomised and Observational Study (CROSSBAT). BMJ Open 2017, 7, e013298. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Harrington, J.; Barlow, C.A.; Tookman, A.; Drake, R.; Barnes, K.; King, M. Advance care planning in advanced cancer: Can it be achieved? An exploratory randomized patient preference trial of a care planning discussion. Palliat. Support. Care 2011, 9, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.; Flach, C.; Leese, M.; Byford, S.; Killaspy, H.; Cole, L.; Lawlor, C.; Betts, J.; Sharac, J.; Cutting, P.; et al. Effectiveness and cost-effectiveness of admissions to women’s crisis houses compared with traditional psychiatric wards: Pilot patient-preference randomised controlled trial. Br. J. Psychiatry 2010, 53, s32–s40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, A.; Wolfenden, L.; Wyse, R.; Bowman, J.; McElduff, P.; Duncan, S. A randomised controlled trial and mediation analysis of the ‘Healthy Habits’, telephone-based dietary intervention for preschool children. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelalian, E.; Evans, E.W.; Rancourt, D.; Ranzenhofer, L.; Taylor, N.; Hart, C.; Seifer, R.; Klinepier, K.; Foster, G.D. JOIN for ME: Testing a Scalable Weight Control Intervention for Adolescents. Child Obes. 2020, 16, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Mihrshahi, S.; Gale, J.; Nguyen, B.; Baur, L.A.; O’Hara, B.J. Translational research: Are community-based child obesity treatment programs scalable? BMC Public Health 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croyden, D.L.; Vidgen, H.A.; Esdaile, E.; Hernandez, E.; Magarey, A.; Moores, C.J.; Daniels, L. A narrative account of implementation lessons learnt from the dissemination of an up-scaled state-wide child obesity management program in Australia: PEACH™ (Parenting, Eating and Activity for Child Health) Queensland. BMC Public Health 2018, 18, 347. [Google Scholar] [CrossRef] [PubMed]
- Nyström, C.D.; Sandin, S.; Henriksson, P.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Ortega, F.B.; Pomeroy, J.; Ruiz, J.R.; et al. Mobile-based intervention intended to stop obesity in preschool-aged children: The MINISTOP randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 1327–1335. [Google Scholar] [CrossRef] [Green Version]
- McCrabb, S.; Lane, C.; Hall, A.; Milat, A.; Bauman, A.; Sutherland, R.; Yoong, S.; Wolfenden, L. Scaling-up evidence-based obesity interventions: A systematic review assessing intervention adaptations and effectiveness and quantifying the scale-up penalty. Obes. Rev. 2019, 20, 964–982. [Google Scholar] [CrossRef]
- Sacher, P.M.; Kolotourou, M.; Poupakis, S.; Chadwick, P.; Radley, D.; Fagg, J. Addressing childhood obesity in low-income, ethnically diverse families: Outcomes and peer effects of MEND 7-13 when delivered at scale in US communities. Int. J. Obes. 2019, 43, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Bedi, N.; Chilvers, C.; Churchill, R.; Dewey, M.; Duggan, C.; Fielding, K.; Gretton, V.; Miller, P.; Harrison, G.; Lee, A.; et al. Assessing effectiveness of treatment of depression in primary care. Partially randomised preference trial. Br. J. Psychiatry 2000, 177, 312–318. [Google Scholar] [CrossRef]
- Majumdar, A.; Latthe, P.; Toozs-Hobson, P. Urodynamics prior to treatment as an intervention: A pilot study. Neurourol. Urodyn. Off. J. Int. Cont. Soc. 2010, 29, 522–526. [Google Scholar] [CrossRef]
- Hubacher, D.; Spector, H.; Monteith, C.; Chen, P.-L.; Hart, C. Rationale and enrollment results for a partially randomized patient preference trial to compare continuation rates of short-acting and long-acting reversible contraception. Contraception 2015, 91, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddock, G.; Berry, K.; Davies, G.; Dunn, G.; Harris, K.; Hartley, S.; Holland, F.; Kelly, J.; Law, H.; Morrison, A.P.; et al. Delivery of cognitive-behaviour therapy for psychosis: A service user preference trial. J. Ment. Health 2018, 27, 336–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Bueno, R.; López-Sánchez, G.F.; Casajús, J.A.; Calatayud, J.; Tully, M.A.; Smith, L. Potential health-related behaviors for pre-school and school-aged children during COVID-19 lockdown: A narrative review. Prev. Med. 2021, 143, 106349. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Jalaludin, B.B.; Morgan, G.G.; Hanigan, I.C.; Johnston, F.H. Bushfire smoke: Urgent need for a national health protection strategy. Med. J. Aust. 2020, 212, 349–353.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Medical Research Council of Australia. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children; National Health and Medical Research Council: Melbourne, Australia, 2013.
- Gemming, L.; Jiang, Y.; Swinburn, B.; Utter, J.; Mhurchu, C.N. Under-reporting remains a key limitation of self-reported dietary intake: An analysis of the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Clin. Nutr. 2014, 68, 259–264. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Randomised | Preference | All | |||||
|---|---|---|---|---|---|---|---|
| Control (n = 81) | Online (n = 86) | Telephone (n = 73) | Control (n = 64) | Online (n = 132) | Telephone (n = 22) | (n = 458) | |
| N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | |
| Child characteristics | |||||||
| Gender | |||||||
| -Female | 35 (43.2%) | 39 (45.3%) | 37 (50.7%) | 33 (51.6%) | 64 (48.5%) | 10 (45.5%) | 218 (47.6%) |
| -Male | 46 (56.8%) | 47 (54.7%) | 36 (49.3%) | 31 (48.4%) | 68 (51.5%) | 12 (54.5%) | 240 (52.4%) |
| Age, Mean (SD) | 3.25 (1.14) | 3.38 (1.14) | 3.23 (1.16) | 3.73 (1.23) | 3.30 (1.15) | 3.55 (1.06) | 3.37 (1.16) |
| Aboriginal or Torres Strait Islander origin | 3 (3.7%) | 4 (4.7%) | 1 (1.4%) | 3 (4.7%) | 3 (2.3%) | 1 (4.5%) | 15 (3.3%) |
| Parent characteristics | |||||||
| Gender | |||||||
| -Female | 79 (97.5%) | 83 (96.5%) | 69 (94.5%) | 62 (96.9%) | 126 (95.5%) | 22 (100.0%) | 441 (96.3%) |
| -Male | 2 (2.5%) | 3 (3.5%) | 4 (5.5%) | 2 (3.1%) | 6 (4.5%) | 0 (0.0%) | 17 (3.7%) |
| Age, Mean (SD) | 36.77 (5.09) | 36.58 (4.92) | 34.92 (4.52) | 35.84 (4.98) | 36.09 (4.84) | 37.18 (5.49) | 36.13 (4.92) |
| Aboriginal or Torres Strait Islander origin | 1 (1.2%) | 2 (2.3%) | 1 (1.4%) | 1 (1.6%) | 1 (0.8%) | 1 (4.5%) | 7 (1.5%) |
| University or other tertiary education | 53 (65.4%) | 64 (74.4%) | 57 (78.1%) | 40 (62.5%) | 88 (66.7%) | 20 (90.9%) | 322 (70.3%) |
| Employment status in last week | |||||||
| -Salary earner | 62 (76.5%) | 55 (64.0%) | 53 (72.6) | 45 (70.3%) | 95 (72.0%) | 17 (77.3%) | 327 (71.4%) |
| -Absent on paid leave | 8 (9.9%) | 5 (5.8%) | 3 (4.1%) | 6 (9.4%) | 14 (10.6%) | 2 (9.1%) | 38 (8.3%) |
| -Unpaid work | 5 (6.2%) | 11 (12.8%) | 2 (2.7%) | 2 (3.1%) | 9 (6.8%) | 0 (0.0%) | 29 (6.4%) |
| -Did not have a job | 6 (7.4%) | 15 (17.4%) | 15 (20.5%) | 11 (17.2%) | 13 (9.8%) | 3 (13.6%) | 63 (13.8%) |
| -Don’t know | 1 (0.8%) | 1 (0.2%) | |||||
| Annual household income before tax | |||||||
| Less than $80,000 | 14 (17.50%) | 15 (17.86%) | 15 (20.55%) | 18 (28.13%) | 20 (15.15%) | 4 (18.18%) | 86 (18.90%) |
| -$80,000 plus | 63 (78.75%) | 66 (78.57%) | 56 (76.71%) | 45 (70.31%) | 105 (79.55%) | 17 (7.27%) | 352 (77.36%) |
| -Don’t know | 3 (3.8%) | 3 (3.6%) | 2 (2.7%) | 1 (1.6%) | 7 (5.3%) | 1 (4.5%) | 17 (3.7%) |
| Hours in paid work last week | 22.54 (17.39) | 19.26 (13.53) | 28.30 (14.44) | 25.77 (15.11) | 24.14 (13.83) | 21.50 (12.45) | 23.70 (14.98) |
| Language other than English spoken at home | 13 (16.0%) | 14 (16.3%) | 16 (21.9%) | 10 (15.6%) | 23 (17.4%) | 5 (22.7%) | 81 (17.7%) |
| CDQ Total Score | CDQ Total Change Score | |||||
|---|---|---|---|---|---|---|
| Baseline Mean (SD) | Complete Case †: Mean Difference vs. Control (95% CI) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | Complete Case †: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | Reference | 14.51 (5.51) | Reference | Reference | Reference |
| Online | 0.14 (−1.12, 1.40) | 15.68 (3.87) | 0.77 (−0.63, 2.16) | 0.14 (−1.12, 1.40) | 0.14 (–1.12, 1.40) | |
| Phone | −0.09 (−1.46, 1.27) | 16.79 (4.17) | 0.76 (−0.83, 2.35) | −0.09 (−1.46, 1.27) | –0.09 (–1.46, 1.27) | |
| Preference only (n = 218) | Written | Reference | 15.75 (3.69) | Reference | Reference | Reference |
| Online | 0.28 (−1.14, 1.70) | 16.36 (4.74) | 0.13 (−1.46, 1.73) | 0.28 (−1.14, 1.70) | 0.28 (–1.14, 1.70) | |
| Phone | −0.68 (−2.77, 1.42) | 14.59 (5.22) | −0.46 (−3.10, 2.19) | −0.68 (−2.77, 1.42) | –0.68 (–2.77, 1.42) | |
| All (n = 458) | Written | Reference | 15.02 (4.85) | Reference | Reference | Reference |
| Online | 0.17 (−0.75, 1.10) | 16.06 (4.79) | 0.40 (−0.62, 1.42) | 0.17 (−0.75, 1.10) | 0.17 (–0.75, 1.10) | |
| Phone | −0.22 (−1.36, 0.92) | 16.16 (4.55) | 0.31 (−1.00, 1.63) | −0.22 (−1.36, 0.92) | –0.22 (–1.36, 0.92) | |
| Fruit Serves per Day | ||||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | |||
| Randomised only (n = 240) | Written | 2.20 (1.02) | 2.23 (0.94) | Reference | Reference | |
| Online | 2.32 (1.20) | 2.21 (1.10) | 0.03 (−0.31, 0.38) | −0.14 (−0.45, 0.16) | ||
| Phone | 2.22 (0.99) | 2.36 (1.05) | 0.06 (−0.34, 0.45) | 0.03 (−0.32, 0.38) | ||
| Preference only (n = 218) | Written | 2.23 (1.11) | 2.57 (0.90) | Reference | Reference | |
| Online | 2.28 (1.16) | 2.36 (1.00) | −0.13 (−0.52, 0.27) | −0.26 (−0.55, 0.02) | ||
| Phone | 2.33 (1.11) | 2.11 (0.96) | −0.38 (−1.02, 0.28) | −0.44 (−0.92, 0.04) | ||
| All (n = 458) | Written | 2.21 (1.06) | 2.29 (1.03) | Reference | Reference | |
| Online | 2.29 (1.17) | 2.93 (1.04) | −0.11 (−0.43, 0.22) | −0.17 (−0.36, 0.03) | ||
| Phone | 2.25 (1.01) | 2.29 (1.03) | −0.05 (−0.30, 0.21) | −0.13 (−0.42, 0.16) | ||
| Vegetable Serves per Day | ||||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | |||
| Randomised only (n = 240) | Written | 1.56 (0.93) | 1.90 (1.08) | Reference | Reference | |
| Online | 1.68 (1.05) | 1.93 (1.06) | −0.14 (−0.52, 0.24) | −0.14 (−0.48, 0.20) | ||
| Phone | 1.81 (0.85) | 2.30 (1.16) | 0.10 (−0.32, 0.53) | 0.20 (−0.21, 0.60) | ||
| Preference only (n = 218) | Written | 1.61 (0.97) | 1.82 (1.14) | Reference | Reference | |
| Online | 1.74 (0.98) | 2.11 (1.15) | 0.17 (−0.26, 0.61) | −0.03 (−0.39, 0.34) | ||
| Phone | 1.46 (1.01) | 1.96 (1.45) | 0.10 (−0.61, 0.81) | 0.08 (−0.44, 0.58) | ||
| All (n = 458) | Written | 1.59 (0.93) | 1.86 (1.10) | Reference | Reference | |
| Online | 1.71 (1.01) | 2.03 (1.11) | 0.003 (−0.28, 0.28) | −0.09 (−0.35, 0.18) | ||
| Phone | 1.72 (0.90) | 2.20 (1.25) | 0.11 (−0.25, 0.46) | 0.19 (−0.13, 0.50) | ||
| Meeting Fruit and Vegetable Guidelines | ||||||
| Baseline N (%) | Follow-Up N (%) | Complete Case †: Odds vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Odds vs. Control (95% CI) | |||
| Randomised only (n = 240) | Written | 46/81 (56.8) | 38/62 (61.3) | Reference | Reference | |
| Online | 53/86 (61.6) | 46/61 (75.4) | 1.53 (0.50, 4.66) | 2.04 (0.78, 5.39) | ||
| Phone | 50/73 (68.5) | 36/45 (80.0) | 1.58 (0.43, 5.86) | 2.61 (0.87, 7.79) | ||
| Preference only (n = 218) | Written | 41/64 (64.1) | 30/44 (68.2) | Reference | Reference | |
| Online | 88/132 (66.7) | 58/77 (75.3) | 1.54 (0.44, 5.40) | 1.94 (0.75, 5.04) | ||
| Phone | 11/22 (50.0) | 10/18 (55.6) | 0.75 (0.10, 5.768) | 0.96 (0.21, 4.45) | ||
| All (n = 458) | Written | 87/145 (60.0) | 68/106 (64.2) | Reference | Reference | |
| Online | 141/218 (64.7) | 104/138 (75.4) | 1.59 (0.71, 3.57) | 1.82 (0.93, 3.53) | ||
| Phone | 61/95 (64.2) | 46/63 (73.0) | 1.28 (0.45, 3.63) | 1.94 (0.84, 4.52) | ||
| Non-Core CDQ Score | |||||
|---|---|---|---|---|---|
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 2.60 (1.01) | 2.47 (1.18) | Reference | Reference |
| Online | 2.43 (1.18) | 2.35 (1.23) | −0.18 (−0.56, 0.20) | −0.05 (−0.13, 0.03) | |
| Phone | 2.20 (1.04) | 1.95 (0.89) | −0.33 (−0.75, 0.10) | −0.26 (−0.35, −0.17) * | |
| Preference only (n = 218) | Written | 2.42 (1.13) | 2.48 (1.15) | Reference | Reference |
| Online | 2.29 (1.05) | 2.32 (0.97) | 0.06 (−0.31, 0.43) | −0.09 (−0.17, −0.01) * | |
| Phone | 2.04 (0.89) | 1.83 (0.94) | −0.41 (−1.10, 0.21) | −0.41 (−0.54, −0.28) * | |
| All (n = 458) | Written | 2.55 (1.04) | 2.47 (1.16) | Reference | Reference |
| Online | 2.41 (1.20) | 2.33 (1.09) | −0.08 (−0.34, 0.18) | −0.05 (−0.29, 0.18) | |
| Phone | 2.13 (1.03) | 1.91 (0.90) | −0.35 (−0.68, −0.02) * | −0.30 (−0.57, −0.03) * | |
| BMI Percentile (WHO) | |||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 0.65 (0.33) | 0.60 (0.32) | Reference | Reference |
| Online | 0.59 (0.31) | 0.60 (0.30) | 0.04 (−0.12, 0.19) | 0.03 (−0.07, 0.13) | |
| Phone | 0.64 (0.34) | 0.64 (0.31) | 0.03 (−0.14, 0.20) | 0.00 (−0.13, 0.13) | |
| Preference only (n = 218) | Written | 0.59 (0.34) | 0.58 (0.32) | Reference | Reference |
| Online | 0.64 (0.31) | 0.55 (0.30) | −0.10 (−0.30, 0.08) | −0.004 (−0.14, 0.13) | |
| Phone | 0.64 (0.35) | 0.58 (0.25) | 0.04 (−0.20, 0.28) | 0.02 (−0.20, 0.23) | |
| All (n = 458) | Written | 0.62 (0.33) | 0.59 (0.31) | Reference | Reference |
| Online | 0.62 (0.31) | 0.57 (0.30) | −0.02 (−0.13, 0.09) | 0.004 (−0.08, 0.09) | |
| Phone | 0.64 (0.34) | 0.62 (0.29) | 0.04 (−0.10, 0.18) | 0.01 (−0.12, 0.14) | |
| Total Physical Activity (Minutes) on Previous Day | |||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 317.85 (174.24) | 291.33 (134.22) | Reference | Reference |
| Online | 281.49 (171.31) | 226.00 (113.53) | −38.33 (−89.46, 12.81) | −20.89 (−64.91, 23.14) | |
| Phone | 322.92 (149.83) | 257.42 (142.54) | 20.13 (−37.92, 78.18) | 30.70 (−19.93, 81.32) | |
| Preference only (n = 218) | Written | 287.67 (149.40) | 275.45 (162.30) | Reference | Reference |
| Online | 310.00 (169.10) | 259.00 (142.31) | −22.72 (−87.02, 41.59) | −24.54 (−78.50, 29.41) | |
| Phone | 293.18 (198.12) | 255.00 (177.41) | −61.15 (−166.06, 43.77) | −17.77 (−94.90, 59.35) | |
| All (n = 458) | Written | 304.01 (163.86) | 264.91 (150.57) | Reference | Reference |
| Online | 298.86 (170.14) | 244.33 (130.88) | −31.04 (−70.31, 8.23) | −18.48 (−55.07, 18.10) | |
| Phone | 315.86 (161.75) | 280.95 (147.27) | −2.95 (−53.68, 47.78) | 13.71 (−31.79, 59.20) | |
| Moderate to Vigorous Physical Activity (Minutes) on Previous Day | |||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 128.28 (95.70) | 116.80 (82.76) | Reference | Reference |
| Online | 131.22 (98.55) | 108.39 (78.18) | −12.02 (−40.92, 16.87) | −6.51 (−34.82, 21.80) | |
| Phone | 151.27 (107.74) | 134.33 (79.11) | 2.47 (−29.94, 34.88) | 11.41 (−17.57, 40.39) | |
| Preference only (n = 218) | Written | 124.52 (79.99) | 122.84 (81.13) | Reference | Reference |
| Online | 136.22 (90.45) | 112.19 (76.39) | −8.86 (−42.79, 25.06) | −11.06 (−36.30, 14.17) | |
| Phone | 77.36 (60.230) | 72.78 (44.27) | −38.58 (−94.63, 17.47) | −30.20 (−71.79, 11.39) | |
| All (n = 458) | Written | 126.64 (88.91) | 119.33 (81.74) | Reference | Reference |
| Online | 134.30 (93.45) | 110.49 (76.92) | −10.28 (−31.70, 11.45) | −8.05 (−25.98, 9.88) | |
| Phone | 133.78 (103.24) | 116.75 (75.93) | −7.28 (−34.92, 20.36) | 1.25 (−22.62, 25.11) | |
| Screen Time (Minutes) on Previous Day | |||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 112.78 (84.04) | 106.45 (105.22) | Reference | Reference |
| Online | 103.60 (107.11) | 114.43 (82.21) | 32.18 (−3.40, 67.77) | 11.34 (−15.83, 38.51) | |
| Phone | 96.82 (81.69) | 88.00 (54.87) | −3.35 (−43.38, 36.69) | −7.83 (−39.00, 23.34) | |
| Preference only (n = 218) | Written | 102.50 (66.72) | 115.91 (90.18) | Reference | Reference |
| Online | 109.60 (80.08) | 119.61 (82.40) | 0.82 (−37.56, 39.20) | 9.51 (−22.36, 41.39) | |
| Phone | 102.62 (82.94) | 125.56 (111.14) | 36.41 (−26.63, 99.45) | 16.91 (−28.54, 62.37) | |
| All (n = 458) | Written | 108.24 (76.80) | 110.38 (98.92) | Reference | Reference |
| Online | 107.23 (91.51) | 117.32 (82.06) | 17.54 (−8.06, 43.14) | 13.29 (−7.13, 33.71) | |
| Phone | 98.13 (81.56) | 98.73 (76.23) | 4.13 (−28.83, 37.10) | −1.84 (−29.79, 26.10) | |
| Sleep (Hours) on Previous Day | |||||
| Baseline Mean (SD) | Follow-Up Mean (SD) | Complete Case †: Mean Difference vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Mean Difference vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 11.66 (1.13) | 11.23 (0.91) | Reference | Reference |
| Online | 11.32 (1.02) | 11.08 (0.86) | −0.01 (−0.36, 0.34) | −0.10 (−0.43, 0.23) | |
| Phone | 11.38 (1.19) | 11.03 (1.01) | 0.03 (−0.37, 0.43) | −0.10 (−0.43, 0.23) | |
| Preference only (n = 218) | Written | 11.46 (1.02) | 11.15 (0.96) | Reference | Reference |
| Online | 11.50 (1.08) | 10.88 (1.00) | −0.48 (−0.91, −0.05) * | −0.29 (−0.58, 0.18) | |
| Phone | 11.14 (1.44) | 11.14 (0.80) | 0.07 (−0.64, 0.78) | 0.15 (−0.38, 0.69) | |
| All (n = 458) | Written | 11.57 (1.09) | 11.20 (0.93) | Reference | Reference |
| Online | 11.43 (1.06) | 10.97 (0.95) | −0.24 (−0.51, 0.03) | −0.17 (−0.41, 0.07) | |
| Phone | 11.32 (1.25) | 11.06 (0.95) | −0.02 (−0.37, 0.33) | −0.05 (−0.35, 0.26) | |
| Meeting Physical Activity Guidelines | |||||
| Baseline N (%) | Follow-Up N (%) | Complete Case †: Odds vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Odds vs. control (95% CI) | ||
| Randomised only (n = 240) | Written | 62/79 (78.5) | 45/61 (73.8) | Reference | Reference |
| Online | 62/82 (75.6) | 41/59 (67.2) | 0.68 (0.25, 1.91) | 0.75 (0.29, 1.97) | |
| Phone | 62/72 (86.1) | 37/45 (82.2) | 2.06 (0.59, 7.20) | 1.24 (0.48, 3.24) | |
| Preference only (n = 218) | Written | 47/61 (77.0) | 35/44 (79.5) | Reference | Reference |
| Online | 105/131 (80.2) | 51/73 (66.2) | 0.38 (0.12, 1.24) | 0.46 (0.19, 1.08) | |
| Phone | 15/22 (68.2) | 11/18 (61.1) | 0.19 (0.03, 1.24) | 0.42 (0.11, 1.57) | |
| All (n = 458) | Written | 109/140 (77.9) | 80/105 (76.2) | Reference | Reference |
| Online | 167/213 (78.4) | 92/132 (69.7) | 0.58 (0.28, 1.20) | 0.66 (0.36, 1.21) | |
| Phone | 77/94 (81.9) | 48/63 (76.2) | 0.99 (0.38, 2.57) | 0.93 (0.45, 1.92) | |
| Meeting Screen Time Guidelines | |||||
| Baseline N (%) | Follow-Up N (%) | Complete Case †: Odds vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Odds vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 35/81 (43.2) | 29/62 (46.8) | Reference | Reference |
| Online | 43/86 (50.0) | 22/61 (36.1) | 0.25 (0.09, 0.69)* | 0.43 (0.17, 1.05) | |
| Phone | 41/72 (56.9) | 25/45 (55.6) | 0.82 (0.28, 2.41) | 1.31 (0.58, 2.99) | |
| Preference only (n = 218) | Written | 30/64 (46.9) | 20/44 (45.5) | Reference | Reference |
| Online | 62/132 (47.0) | 33/77 (42.9) | 1.02 (0.39, 2.7) | 0.73 (0.32, 1.68) | |
| Phone | 10/21 (47.6) | 10/18 (55.6) | 1.11 (0.23, 5.47) | 1.40 (0.44, 0.47) | |
| All (n = 458) | Written | 65/145 (44.8) | 49/106 (46.2) | Reference | Reference |
| Online | 105/218 (48.2) | 55/138 (39.9) | 0.56 (0.29, 1.09) | 0.60 (0.32, 1.11) | |
| Phone | 51/93 (54.8) | 35/63 (55.6) | 1.02 (0.44, 2.38) | 1.34 (0.67, 2.70) | |
| Meeting Sleep Guidelines | |||||
| Baseline N (%) | Follow-Up N (%) | Complete Case †: Odds vs. Control Adjusted (95% CI) | Multiple Imputation ‡: Odds vs. Control (95% CI) | ||
| Randomised only (n = 240) | Written | 70/81 (86.4) | 53/62 (85.5) | Reference | Reference |
| Online | 73/86 (84.9) | 55/61 (90.2) | 2.12 (0.46, 9.67) | 1.66 (0.52, 5.31) | |
| Phone | 58/73 (79.5) | 33/45 (73.3) | 0.89 (0.22, 3.60) | 0.64 (0.24, 1.73) | |
| Preference only (n = 218) | Written | 54/64 (84.4) | 37/42 (88.1) | Reference | Reference |
| Online | 114/132 (86.4) | 62/77 (80.5) | 0.37 (0.08, 1.79) | 0.64 (0.24, 1.84) | |
| Phone | 16/22 (72.7) | 14/18 (77.8) | 1.82 (0.14, 23.12) | 0.64 (0.12, 3.32) | |
| All (n = 458) | Written | 124/145 (85.5) | 90/104 (86.5) | Reference | Reference |
| Online | 187/218 (85.8) | 117/138 (84.8) | 0.78 (0.30, 2.04) | 0.90 (0.44, 1.86) | |
| Phone | 74/95 (77.9) | 47/63 (74.6) | 0.99 (0.31, 3.17) | 0.60 (0.26, 1.34) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammersley, M.L.; Wyse, R.J.; Jones, R.A.; Stacey, F.; Okely, A.D.; Wolfenden, L.; Batterham, M.J.; Yoong, S.; Eckermann, S.; Green, A.; et al. Translation of Two Healthy Eating and Active Living Support Programs for Parents of 2–6-Year-Old Children: Outcomes of the ‘Time for Healthy Habits’ Parallel Partially Randomised Preference Trial. Nutrients 2021, 13, 3348. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103348
Hammersley ML, Wyse RJ, Jones RA, Stacey F, Okely AD, Wolfenden L, Batterham MJ, Yoong S, Eckermann S, Green A, et al. Translation of Two Healthy Eating and Active Living Support Programs for Parents of 2–6-Year-Old Children: Outcomes of the ‘Time for Healthy Habits’ Parallel Partially Randomised Preference Trial. Nutrients. 2021; 13(10):3348. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103348
Chicago/Turabian StyleHammersley, Megan L., Rebecca J. Wyse, Rachel A. Jones, Fiona Stacey, Anthony D. Okely, Luke Wolfenden, Marijka J. Batterham, Serene Yoong, Simon Eckermann, Amanda Green, and et al. 2021. "Translation of Two Healthy Eating and Active Living Support Programs for Parents of 2–6-Year-Old Children: Outcomes of the ‘Time for Healthy Habits’ Parallel Partially Randomised Preference Trial" Nutrients 13, no. 10: 3348. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103348