
Nutritional Intake, White Matter Integrity, and Neurodevelopment in Extremely Preterm Born Infants

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
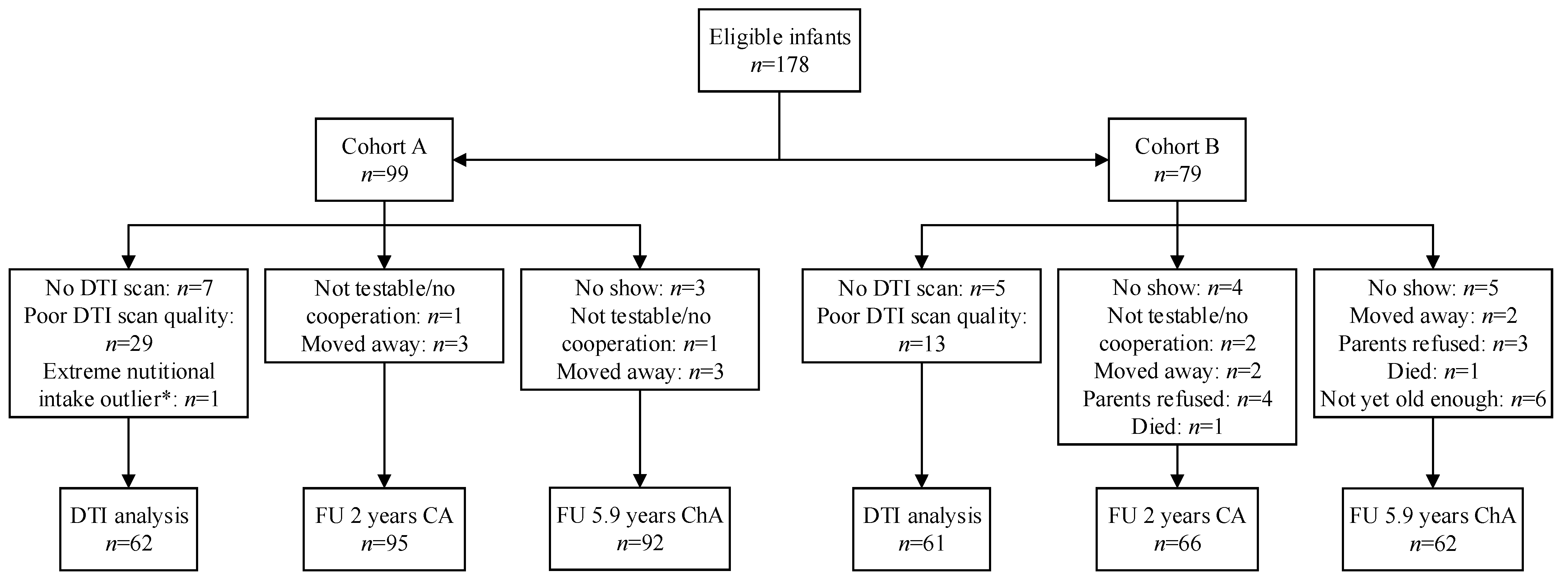
2.1. Patient Population
2.2. Data Collection and Nutritional Regimens
2.3. MRI Acquisition and Processing
2.4. Neurodevelopmental Outcome Measurements
2.5. Statistical Analysis
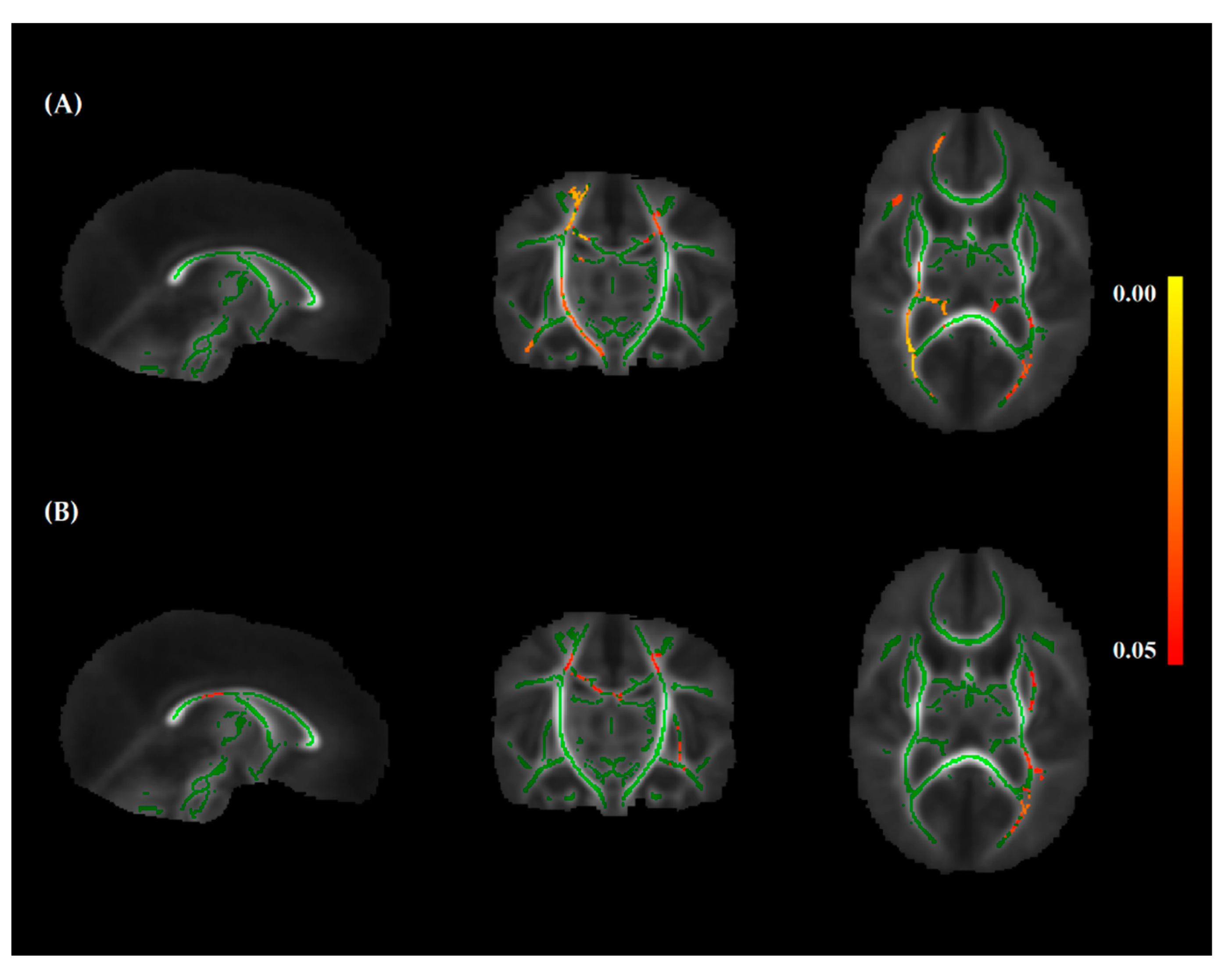
2.5.1. White Matter Integrity
2.5.2. Neurodevelopmental Outcome
3. Results
3.1. Patient Population
3.2. Nutritional Details
3.3. Nutritional Intake and White Matter Integrity
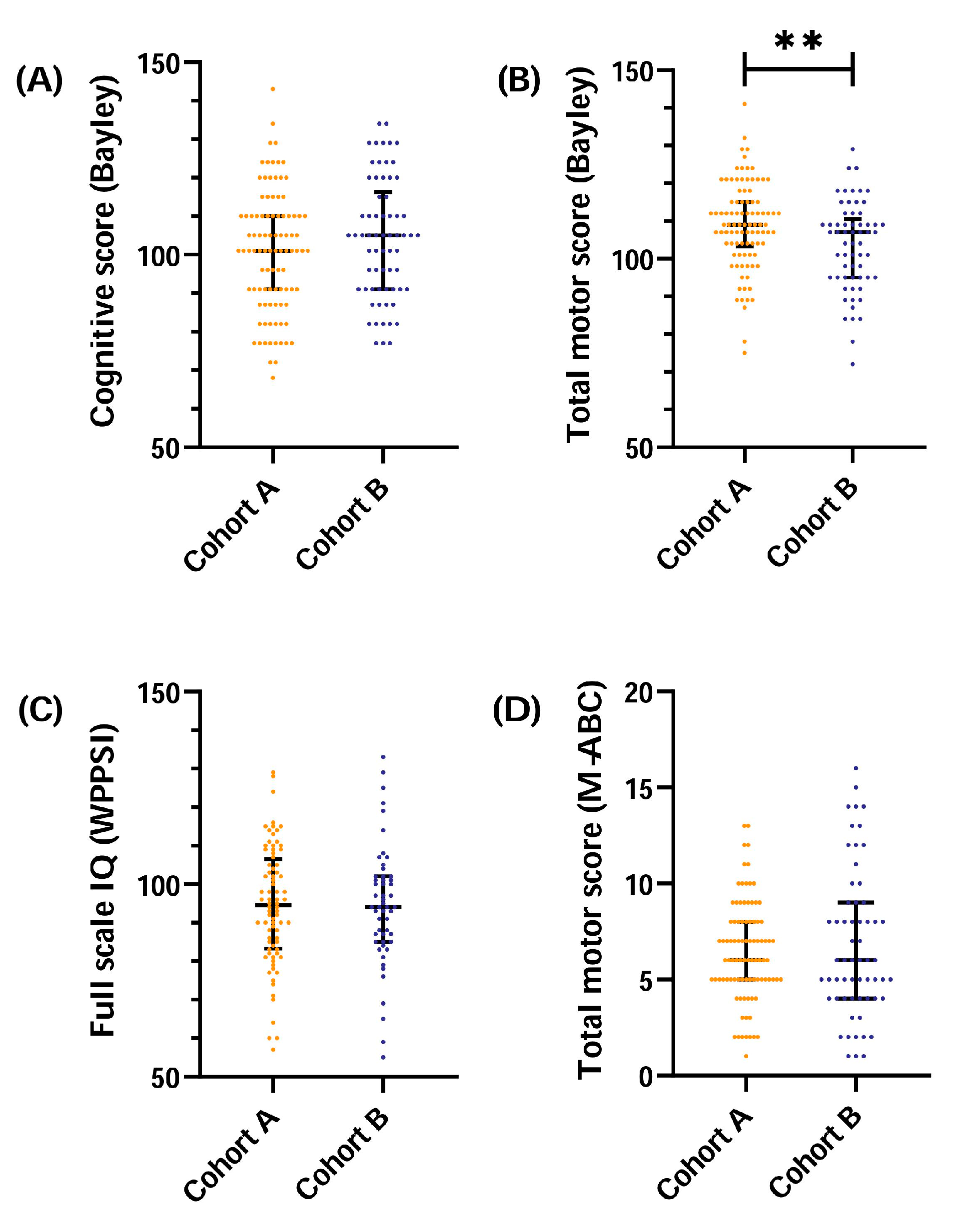
3.4. Nutritional Intake and Neurodevelopmental Outcome at 2 Years CA and 5.9 Years Chronological Age
4. Discussion
4.1. Protein Intake and White Matter Integrity
4.2. Protein Intake and Neurodevelopmental Outcome
4.3. Clinical Relevance
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vinall, J.; Grunau, R.E.; Brant, R.; Chau, V.; Poskitt, K.J.; Synnes, A.R.; Miller, S.P. Slower postnatal growth is associated with delayed cerebral cortical maturation in preterm newborns. Sci. Transl. Med. 2013, 5, 168ra8. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.A.; Matthews, L.G.; Cherkerzian, S.; Palmer, C.; Drouin, K.; Pepin, H.L.; Ellard, D.; Inder, T.E.; Ramel, S.E.; Belfort, M.B. Associations of Growth and Body Composition with Brain Size in Preterm Infants. J. Pediatr. 2019, 214, 20–26.e2. [Google Scholar] [CrossRef] [PubMed]
- Coviello, C.; Keunen, K.; Kersbergen, K.J.; Groenendaal, F.; Leemans, A.; Peels, B.; Isgum, I.; Viergever, M.A.; de Vries, L.S.; Buonocore, G.; et al. Effects of early nutrition and growth on brain volumes, white matter microstructure, and neurodevelopmental outcome in preterm newborns. Pediatr. Res. 2018, 83, 102–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belfort, M.B.; Rifas-Shiman, S.L.; Sullivan, T.; Collins, C.T.; McPhee, A.J.; Ryan, P.; Kleinman, K.P.; Gillman, M.W.; Gibson, R.A.; Makrides, M. Infant growth before and after term: Effects on neurodevelopment in preterm infants. Pediatrics 2011, 128, e899–e906. [Google Scholar] [CrossRef]
- Frondas-Chauty, A.; Simon, L.; Branger, B.; Gascoin, G.; Flamant, C.; Ancel, P.Y.; Darmaun, D.; Roze, J.C. Early growth and neurodevelopmental outcome in very preterm infants: Impact of gender. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F366–F372. [Google Scholar] [CrossRef] [PubMed]
- Guellec, I.; Lapillonne, A.; Marret, S.; Picaud, J.C.; Mitanchez, D.; Charkaluk, M.L.; Fresson, J.; Arnaud, C.; Flamant, C.; Cambonie, G.; et al. Effect of Intra- and Extrauterine Growth on Long-Term Neurologic Outcomes of Very Preterm Infants. J. Pediatr. 2016, 175, 93–99.e1. [Google Scholar] [CrossRef]
- Ottolini, K.M.; Andescavage, N.; Keller, S.; Limperopoulos, C. Nutrition and the developing brain: The road to optimizing early neurodevelopment: A systematic review. Pediatr. Res. 2020, 87, 194–201. [Google Scholar] [CrossRef]
- Schneider, J.; Fischer Fumeaux, C.J.; Duerden, E.G.; Guo, T.; Foong, J.; Graz, M.B.; Hagmann, P.; Chakravarty, M.M.; Huppi, P.S.; Beauport, L.; et al. Nutrient Intake in the First Two Weeks of Life and Brain Growth in Preterm Neonates. Pediatrics 2018, 141, e20172169. [Google Scholar] [CrossRef] [Green Version]
- Beauport, L.; Schneider, J.; Faouzi, M.; Hagmann, P.; Huppi, P.S.; Tolsa, J.F.; Truttmann, A.C.; Fischer Fumeaux, C.J. Impact of Early Nutritional Intake on Preterm Brain: A Magnetic Resonance Imaging Study. J. Pediatr. 2017, 181, 29–36.e1. [Google Scholar] [CrossRef] [Green Version]
- van Beek, P.E.; Claessens, N.H.P.; Makropoulos, A.; Groenendaal, F.; de Vries, L.S.; Counsell, S.J.; Benders, M. Increase in Brain Volumes after Implementation of a Nutrition Regimen in Infants Born Extremely Preterm. J. Pediatr. 2020, 223, 57–63.e5. [Google Scholar] [CrossRef]
- Shim, S.Y.; Ahn, H.M.; Cho, S.J.; Park, E.A. Early aggressive nutrition enhances language development in very low-birthweight infants. Pediatr. Int. 2014, 56, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.E.; Walden, R.V.; Gargus, R.A.; Tucker, R.; McKinley, L.; Mance, M.; Nye, J.; Vohr, B.R. First-week protein and energy intakes are associated with 18-month developmental outcomes in extremely low birth weight infants. Pediatrics 2009, 123, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Cester, E.A.; Bloomfield, F.H.; Taylor, J.; Smith, S.; Cormack, B.E. Do recommended protein intakes improve neurodevelopment in extremely preterm babies? Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F243–F247. [Google Scholar] [CrossRef]
- Barreault, S.; Bellanger, A.; Berneau, P.; de La Pintiere, A.; Lallemant, C.; Beuchee, A. Impact of early protein and energy intakes on neurodevelopment at 2 years of corrected age in very low birth weight infants: A single-center observational study. PLoS ONE 2019, 14, e0218887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormack, B.E.; Harding, J.E.; Miller, S.P.; Bloomfield, F.H. The Influence of Early Nutrition on Brain Growth and Neurodevelopment in Extremely Preterm Babies: A Narrative Review. Nutrients 2019, 11, 2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.H.; Johnson, M.J.; Leaf, A.A.; Vollmer, B. Nutrition and neurodevelopmental outcomes in preterm infants: A systematic review. Acta Paediatr. 2016, 105, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortensius, L.M.; van Elburg, R.M.; Nijboer, C.H.; Benders, M.; de Theije, C.G.M. Postnatal Nutrition to Improve Brain Development in the Preterm Infant: A Systematic Review From Bench to Bedside. Front. Physiol. 2019, 10, 961. [Google Scholar] [CrossRef]
- Dutch Perinatal Registry. Available online: www.perined.nl (accessed on 21 August 2018).
- Statistics Netherlands. Education Level. Available online: https://www.cbs.nl/en-gb/news/2018/20/well-being-not-distributed-equally/education-level (accessed on 6 June 2018).
- Lafeber, H.N.; van Zoeren-Grobben, D.; van Beek, R.H.T.; Christmann, V. Werkboek Enterale en Parenterale Voeding bij Pasgeborenen; VU University Press: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23 (Suppl. 1), S208–S219. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- Andersson, J.L.R.; Jenkinson, M.; Smith, S. Non-linear optimisation. FMRIB technical report TR07JA. Practice 2007. Available online: www.fmrib.ox.ac.uk/analysis/techrep (accessed on 7 February 2021).
- Andersson, J.L.R.; Jenkinson, M.; Smith, S. Non-linear registration, aka Spatial normalisation FMRIB technical report TR07JA2. FMRIB Anal. Group Univ. Oxf. 2007, 2, e21. Available online: www.fmrib.ox.ac.uk/analysis/techrep (accessed on 7 February 2021).
- Winkler, A.M.; Ridgway, G.R.; Webster, M.A.; Smith, S.M.; Nichols, T.E. Permutation inference for the general linear model. Neuroimage 2014, 92, 381–397. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Nichols, T.E. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. Neuroimage 2009, 44, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Nichols, T.E.; Holmes, A.P. Nonparametric permutation tests for functional neuroimaging: A primer with examples. Hum. Brain Mapp. 2002, 15, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org (accessed on 6 July 2021).
- Terrin, G.; De Nardo, M.C.; Boscarino, G.; Di Chiara, M.; Cellitti, R.; Ciccarelli, S.; Gasparini, C.; Parisi, P.; Urna, M.; Ronchi, B.; et al. Early Protein Intake Influences Neonatal Brain Measurements in Preterms: An Observational Study. Front. Neurol. 2020, 11, 885. [Google Scholar] [CrossRef] [PubMed]
- Duerden, E.G.; Thompson, B.; Poppe, T.; Alsweiler, J.; Gamble, G.; Jiang, Y.; Leung, M.; Tottman, A.C.; Wouldes, T.; Miller, S.P.; et al. Early protein intake predicts functional connectivity and neurocognition in preterm born children. Sci. Rep. 2021, 11, 4085. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K. Nutrition and the developing brain: Nutrient priorities and measurement. Am. J. Clin. Nutr. 2007, 85, 614S–620S. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Burgess, L. High Protein Intake Does Not Prevent Low Plasma Levels of Conditionally Essential Amino Acids in Very Preterm Infants Receiving Parenteral Nutrition. JPEN J. Parenter. Enteral Nutr. 2017, 41, 455–462. [Google Scholar] [CrossRef]
- Yumani, D.F.; Lafeber, H.N.; van Weissenbruch, M.M. Dietary proteins and IGF I levels in preterm infants: Determinants of growth, body composition, and neurodevelopment. Pediatr. Res. 2015, 77, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [Green Version]
- Hay, W.W., Jr. Nutritional Support Strategies for the Preterm Infant in the Neonatal Intensive Care Unit. Pediatr. Gastroenterol. Hepatol. Nutr. 2018, 21, 234–247. [Google Scholar] [CrossRef]
- Hay, W.W.; Thureen, P. Protein for preterm infants: How much is needed? How much is enough? How much is too much? Pediatr. Neonatol. 2010, 51, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Jahn, O.; Tenzer, S.; Werner, H.B. Myelin proteomics: Molecular anatomy of an insulating sheath. Mol. Neurobiol. 2009, 40, 55–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socha, P.; Grote, V.; Gruszfeld, D.; Janas, R.; Demmelmair, H.; Closa-Monasterolo, R.; Subias, J.E.; Scaglioni, S.; Verduci, E.; Dain, E.; et al. Milk protein intake, the metabolic-endocrine response, and growth in infancy: Data from a randomized clinical trial. Am. J. Clin. Nutr. 2011, 94, 1776S–1784S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engstrom, E.; Niklasson, A.; Wikland, K.A.; Ewald, U.; Hellstrom, A. The role of maternal factors, postnatal nutrition, weight gain, and gender in regulation of serum IGF-I among preterm infants. Pediatr. Res. 2005, 57, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yumani, D.F.J.; Calor, A.K.; van Weissenbruch, M.M. The Course Of IGF-1 Levels and Nutrient Intake in Extremely and Very Preterm Infants During Hospitalisation. Nutrients 2020, 12, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen-Pupp, I.; Hovel, H.; Hellstrom, A.; Hellstrom-Westas, L.; Lofqvist, C.; Larsson, E.M.; Lazeyras, F.; Fellman, V.; Huppi, P.S.; Ley, D. Postnatal decrease in circulating insulin-like growth factor-I and low brain volumes in very preterm infants. J. Clin. Endocrinol. Metab. 2011, 96, 1129–1135. [Google Scholar] [CrossRef]
- Okuma, C.; Hernandez, M.I.; Rodriguez, P.; Flores, R.; Avila, A.; Cavada, G.; Kopplin, E.; Rossel, K.; Iniguez, G.; Mericq, V. Microstructural brain and multivoxel spectroscopy in very low birth weight infants related to insulin-like growth factor concentration and early growth. Horm. Res. Paediatr. 2013, 79, 197–207. [Google Scholar] [CrossRef]
- Wojnar, M.M.; Fan, J.; Li, Y.H.; Lang, C.H. Endotoxin-induced changes in IGF-I differ in rats provided enteral vs. parenteral nutrition. Am. J. Physiol. 1999, 276, E455–E464. [Google Scholar] [CrossRef]
- O’Leary, M.J.; Xue, A.; Scarlett, C.J.; Sevette, A.; Kee, A.J.; Smith, R.C. Parenteral versus enteral nutrition: Effect on serum cytokines and the hepatic expression of mRNA of suppressor of cytokine signaling proteins, insulin-like growth factor-1 and the growth hormone receptor in rodent sepsis. Crit. Care 2007, 11, R79. [Google Scholar] [CrossRef] [Green Version]
- Keunen, K.; van Elburg, R.M.; van Bel, F.; Benders, M.J. Impact of nutrition on brain development and its neuroprotective implications following preterm birth. Pediatr. Res. 2015, 77, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Tottman, A.C.; Alsweiler, J.M.; Bloomfield, F.H.; Gamble, G.D.; Jiang, Y.; Leung, M.; Poppe, T.; Thompson, B.; Wouldes, T.A.; Harding, J.E.; et al. Relationships Between Early Neonatal Nutrition and Neurodevelopment at School Age in Children Born Very Preterm. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 72–78. [Google Scholar] [CrossRef]
- Blanco, C.L.; Gong, A.K.; Schoolfield, J.; Green, B.K.; Daniels, W.; Liechty, E.A.; Ramamurthy, R. Impact of early and high amino acid supplementation on ELBW infants at 2 years. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 601–607. [Google Scholar] [CrossRef]
- Cormack, B.E.; Bloomfield, F.H.; Dezoete, A.; Kuschel, C.A. Does more protein in the first week of life change outcomes for very low birthweight babies? J. Paediatr. Child Health 2011, 47, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Biasini, A.; Monti, F.; Laguardia, M.C.; Stella, M.; Marvulli, L.; Neri, E. High protein intake in human/maternal milk fortification for ≤1250 gr infants: Intrahospital growth and neurodevelopmental outcome at two years. Acta Biomed. 2018, 88, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Al-Wassia, H.; Premji, S.S.; Sauve, R.S. Higher versus lower protein intake in formula-fed low birth weight infants. Cochrane Database Syst. Rev. 2020, 6, CD003959. [Google Scholar] [CrossRef] [Green Version]
- Osborn, D.A.; Schindler, T.; Jones, L.J.; Sinn, J.K.; Bolisetty, S. Higher versus lower amino acid intake in parenteral nutrition for newborn infants. Cochrane Database Syst. Rev. 2018, 3, CD005949. [Google Scholar] [CrossRef] [PubMed]
- Embleton, N.D.; van den Akker, C.H.P. Protein intakes to optimize outcomes for preterm infants. Semin. Perinatol. 2019, 43, 151154. [Google Scholar] [CrossRef]
- Girault, J.B.; Cornea, E.; Goldman, B.D.; Knickmeyer, R.C.; Styner, M.; Gilmore, J.H. White matter microstructural development and cognitive ability in the first 2 years of life. Hum. Brain Mapp. 2019, 40, 1195–1210. [Google Scholar] [CrossRef] [Green Version]
- van Kooij, B.J.; van Pul, C.; Benders, M.J.; van Haastert, I.C.; de Vries, L.S.; Groenendaal, F. Fiber tracking at term displays gender differences regarding cognitive and motor outcome at 2 years of age in preterm infants. Pediatr. Res. 2011, 70, 626–632. [Google Scholar] [CrossRef] [Green Version]
- van Kooij, B.J.; de Vries, L.S.; Ball, G.; van Haastert, I.C.; Benders, M.J.; Groenendaal, F.; Counsell, S.J. Neonatal tract-based spatial statistics findings and outcome in preterm infants. AJNR Am. J. Neuroradiol. 2012, 33, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Blesa, M.S.G.; Anblagan, D.; Telford, E.J.; Quigley, A.J.; Sparrow, S.; Serag, A.; Semple, S.I.; Blastin, M.; Boardman, J.P. Early breast milk exposure modifies brain connectivity in preterm infants. Neuroimage 2019, 184, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Chetta, K.E.; Schulz, E.V.; Wagner, C.L. Outcomes improved with human milk intake in preterm and full-term infants. Semin. Perinatol. 2021, 45, 151384. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| DTI Analysis (n = 123) | 2 Years Corrected Age (n = 161) | 5.9 Years Chronological Age (n = 154) | |
|---|---|---|---|
| Male (%) | 57 (46) | 75 (47) | 72 (47) |
| Gestational age (weeks) (median (Q1; Q3)) | 26 + 3 (25 + 6; 27 + 2) | 26 + 3 (25 + 6; 27 + 1) | 26 + 3 (25 + 6; 27 + 2) |
| Birth weight (g) (median (Q1; Q3)) | 880 (784; 1000) | 870 (750; 995) | 870 (750; 1000) |
| Birth weight Z-score (mean (SD)) | 0.39 (0.88) | 0.30 (0.91) | 0.28 (0.90) |
| SGA (<10th percentile) (%) | 5 (4) | 8 (5) | 8 (5) |
| Multiplicity (%) | 36 (29) | 52 (32) | 52 (34) |
| Apgar 5 min (median (Q1; Q3)) | 8 (7; 8) | 8 (7; 9) | 8 (7; 9) |
| Days parental nutrition (median (Q1; Q3)) | 13 (10; 17) | 12 (10; 17) | 12 (10; 17) |
| >7 days of ventilation (%) | 62 (50) | 83 (52) | 79 (51) |
| Abdominal surgery (%) | 10 (8) | 14 (9) | 14 (9) |
| Severe brain injury (%) | 14 (11) | 17 (11) | 15 (10) |
| Sepsis (%) | 48 (39) | 62 (39) | 59 (38) |
| DTI Analysis | 2 Years Corrected Age | 5.9 Years Chronological Age | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Cohort A (n = 63) | Cohort B (n = 60) | p-Value | Cohort A (n = 95) | Cohort B (n = 66) | p-Value | Cohort A (n = 92) | Cohort B (n = 62) | p-Value | |
| Total | |||||||||
| Protein (g/kg) | 75 (72; 82) | 97 (93; 99) | <0.001 # | 74 (71; 81) | 96 (93; 99) | <0.001 # | 74 (71; 80) | 97 (94; 99) | <0.001 # |
| Lipids (g/kg) | 135 (121; 148) | 136 (124; 144) | 0.71 | 137 (120; 148) | 134 (123; 144) | 0.55 | 136 (119; 148) | 135 (124; 144) | 0.87 |
| Calories (kcal/kg) | 2924 (2710; 3157) | 3075 (2895; 3181) | 0.02 * | 2924 (2707; 3149) | 3038 (2864; 3177) | 0.07 | 2924 (2699; 3155) | 3055 (2906; 3177) | 0.03 * |
| Daily | |||||||||
| Protein (g/kg) | 2.7 (2.6; 2.9) | 3.5 (3.3; 3.5) | <0.001 # | 2.7 (2.5; 2.9) | 3.4 (3.3; 3.5) | <0.001 # | 2.7 (2.5; 2.8) | 3.5 (3.3; 3.5) | <0.001 # |
| Lipids (g/kg) | 4.8 (4.3; 5.3) | 4.9 (4.4; 5.2) | 0.71 | 4.9 (4.3; 5.3) | 4.8 (4.4; 5.1) | 0.55 | 4.9 (4.3; 5.3) | 4.8 (4.4; 5.1) | 0.87 |
| Calories (kcal/kg) | 104 (97; 113) | 110 (103; 114) | 0.02 * | 104 (97; 112) | 108 (102; 113) | 0.07 | 104 (96; 113) | 109 (104; 113) | 0.03 * |
| % enteral | |||||||||
| Protein | 72% (61%; 80%) | 70% (59%; 76%) | 0.33 | 73% (60%; 82%) | 69% (59%; 76%) | 0.05 * | 72% (59%; 82%) | 69% (59%; 76%) | 0.12 |
| Lipids | 92% (87%; 95%) | 90% (84%; 93%) | 0.06 | 92% (87%; 95%) | 90% (84%; 93%) | 0.01 * | 92% (87%; 95%) | 90% (85%; 93%) | 0.02 * |
| Calories | 83% (75%; 89%) | 83% (72%; 87%) | 0.65 | 84% (74%; 89%) | 82% (73%; 87%) | 0.15 | 83% (74%; 89%) | 82% (74%; 87%) | 0.31 |
| Protein/energy ratio | |||||||||
| Protein (g)/100 kcal | 2.6 (2.4; 2.9) | 3.2 (3.1; 3.3) | <0.001 * | 2.6 (2.4; 2.9) | 3.2 (3.1; 3.3) | <0.001 * | 2.6 (2.4; 2.9) | 3.2 (3.1; 3.3) | <0.001 * |
| Cohort A | Cohort B | p-Value | |
|---|---|---|---|
| 2 years corrected age | |||
| Cognition | n = 95 | n = 66 | |
| Cognitive score | 101 (16) | 104 (16) | 0.20 |
| Motor | n = 94 | n = 61 | |
| Total motor score | 109 (12) | 103 (12) | 0.005 ** |
| Fine motor score | 13 (2.2) | 11 (2.6) | 0.002 ** |
| Gross motor score | 8.1 (2.7) | 7.5 (2.5) | 0.12 |
| 5.9 years chronological age | |||
| Cognition | n = 80 | n = 53 | |
| Full scale IQ | 94 (15) | 94 (16) | 0.99 |
| Verbal IQ | 98 (18) | 97 (14) | 0.88 |
| Performance IQ | 96 (13) | 97 (15) | 0.72 |
| Processing speed | 90 (16) | 88 (15) | 0.46 |
| Motor | n = 91 | n = 60 | |
| Total motor score | 6.4 (2.6) | 6.8 (3.9) | 0.92 |
| Manual dexterity | 6.7 (2.5) | 7.2 (3.3) | 0.26 |
| Aiming and catching | 7.7 (2.7) | 7.9 (3.7) | 0.73 |
| Balance | 7.9 (2.9) | 7.9 (3.3) | 0.92 |
| Cognition 2 Years CA | Motor 2 Years CA | Cognition 5.9 Years ChA | Motor 5.9 Years ChA | |
|---|---|---|---|---|
| Nutritional cohort (ref = cohort A) | 2.6 (−2.3 to 7.4) | −5.2 (−8.9 to −1.5) ** | 0.2 (−5.5 to 5.5) | 0.4 (−0.6 to 1.5) |
| Gestational age (days) | 0.1 (−0.2 to 0.5) | 0.2 (−0.1 to 0.5) | −0.1 (−0.5 to 0.3) | 0.0 (−0.1 to 0.1) |
| Gender (ref = male) | 2.6 (−2.2 to 7.3) | 1.1 (−2.6 to 4.7) | 1.7 (−3.5 to 6.9) | 1.5 (0.5 to 2.5) ** |
| Birth weight Z-score | 2.0 (−0.7 to 4.7) | 2.8 (0.8 to 4.9) ** | −0.9 (−3.9 to 2.1) | 0.1 (−0.5 to 0.7) |
| Severe illness (ref = no) | 1.4 (−3.7 to 6.5) | −2.4 (−6.3 to 1.4) | 0.0 (−5.6 to 5.6) | −1.3 (−2.4 to −0.2) * |
| Maternal education (ref = low) | ||||
| middle | 3.3 (−3.2 to 9.7) | 1.0 (−3.8 to 5.9) | 10 (2.6 to 17.5) ** | 0.2 (−0.6 to 2.3) |
| high | 11.9 (5.1 to 18.6) ** | 2.9 (−2.1 to 8.0) | 13.4 (5.8 to 21.1) ** | 0.8 (−0.6 to 2.3) |
| Severe brain injury (ref = no) | −0.7 (−8.3 to 6.9) | −2.3 (−8.2 to 3.5) | 9.1 (0.3 to 17.9) * | −0.4 (−2.1 to 1.3) |
| Cognition 2 Years CA | Motor 2 Years CA | Cognition 5.9 Years ChA | Motor 5.9 Years ChA | |
|---|---|---|---|---|
| Daily protein intake (grams/kg) | −2.7 (−8.1 to 2.7) | −6.7 (−10.8 to −2.7) ** | −1.0 (−6.9 to 4.9) | −0.6 (−1.8 to 0.5) |
| Gestational age (days) | 0.1 (−0.2 to 0.5) | 0.2 (−0.1 to 0.4) | −0.1 (−0.5 to 0.3) | 0.0 (−0.1 to 0.1) |
| Gender (ref = male) | 2.3 (−2.5 to 7.0) | 1.0 (−2.6 to 4.6) | 1.6 (−3.6 to 6.8) | 1.4 (0.4 to 2.4) ** |
| Birth weight Z-score | 1.9 (−0.8 to 4.6) | 2.7 (0.7 to 4.7) * | −0.9 (−3.9 to 2.1) | 0.1 (−0.5 to 0.6) |
| Severe illness (ref = no) | 1.3 (−3.8 to 6.5) | −3.1 (−6.9 to 0.8) | −0.2 (−5.9 to 5.5) | −1.3 (−2.4 to −0.2) * |
| Maternal education (ref = low) | ||||
| middle | 3.8 (−2.7 to 10.3) | 1.8 (−3.0 to 6.6) | 10.3 (2.7 to 17.9) ** | 0.4 (−1.0 to 1.8) |
| high | 12.9 (6.2 to 19.6) # | 2.9 (−2.1 to 7.8) | 13.7 (6.0 to 21.4) ** | 1.1 (−0.4 to 2.5) |
| Severe brain injury (ref = no) | −0.8 (−8.4 to 6.9) | −2.5 (−8.3 to 3.2) | 9.0 (0.2 to 17.8) * | −0.5 (−2.2 to 1.3) |
| Cognition 2 Years CA | Motor 2 Years CA | Cognition 5.9 Years ChA | Motor 5.9 Years ChA | |
|---|---|---|---|---|
| Daily lipid intake (grams/kg) | 0.2 (−3.4 to 3.9) | 0.1 (−2.7 to 2.9) | −0.8 (−4.7 to 3.2) | 0.0 (−0.7 to 0.8) |
| Gestational age (days) | 0.1 (−0.2 to 0.5) | 0.2 (−0.1 to 0.5) | −0.1 (−0.5 to 0.3) | 0.0 (−0.1 to 0.1) |
| Gender (ref = male) | 2.5 (−2.4 to 7.3) | 1.3 (−2.4 to 5.1) | 1.6 (−3.6 to 6.8) | 1.5 (0.5 to 2.5) ** |
| Birth weight Z-score | 2.0 (−0.7 to 4.7) | 2.9 (0.8 to 5.0) ** | −0.9 (−3.9 to 2.1) | 0.1 (−0.5 to 0.6) |
| Severe illness (ref = no) | 1.7 (−4.1 to 7.5) | −2.4 (−6.9 to 2.1) | −0.5 (−6.8 to 5.7) | −1.3 (−2.5 to −0.1) * |
| Maternal education (ref = low) | ||||
| middle | 3.4 (−3.1 to 9.9) | 0.9 (−4.1 to 5.9) | 10.1 (2.7 to 17.6) ** | 0.3 (−1.1 to 1.6) |
| high | 12.4 (5.8 to 19.1) # | 1.7 (−3.4 to 6.8) | 13.5 (5.9 to 21.0) ** | 0.9 (−0.5 to 2.4) |
| Severe brain injury (ref = no) | −0.8 (−8.4 to 6.9) | −2.5 (−8.5 to 3.5) | 9.3 (0.4 to 18.1) * | −0.4 (−2.1 to 1.3) |
| Cognition 2 Years CA | Motor 2 Years CA | Cognition 5.9 Years ChA | Motor 5.9 Years ChA | |
|---|---|---|---|---|
| Daily caloric intake (kCal/kg) | 0.0 (−0.3 to 0.3) | −0.1 (−0.2 to 0.1) | −0.1 (−0.3 to 0.2) | 0.0 (−0.1 to 0.1) |
| Gestational age (days) | 0.1 (−0.2 to 0.5) | 0.2 (−0.1 to 0.5) | −0.1 (−0.5 to 0.3) | 0.0 (−0.1 to 0.1) |
| Gender (ref = male) | 2.4 (−2.4 to 7.2) | 1.3 (−2.5 to 5.0) | 1.6 (−3.6 to 6.8) | 1.5 (0.5 to 2.5) ** |
| Birth weight Z-score | 2.0 (−0.7 to 4.7) | 2.9 (0.8 to 5.0) ** | −0.9 (−3.9 to 2.1) | 0.1 (−0.5 to 0.7) |
| Severe illness (ref = no) | 1.5 (−4.2 to 7.3) | −3.0 (−7.5 to 1.4) | −0.8 (−7.0 to 5.4) | −1.2 (−2.5 to −0.0) * |
| Maternal education (ref = low) | ||||
| middle | 3.4 (−3.1 to 9.9) | 1.0 (−4.0 to 5.9) | 10.2 (2.7 to 17.6) ** | 0.3 (−0.5 to 2.4) |
| high | 12.4 (5.8 to 19.1) | 1.7 (−3.4 to 6.8) | 13.6 (6.0 to 21.1) ** | 0.9 (−0.5 to 2.4) |
| Severe brain injury (ref = no) | −0.7 (−8.4 to 7.0) | −2.4 (−8.4 to 3.6) | 9.2 (0.4 to 18.0) * | −0.4 (−2.2 to 1.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hortensius, L.M.; Janson, E.; van Beek, P.E.; Groenendaal, F.; Claessens, N.H.P.; Swanenburg de Veye, H.F.N.; Eijsermans, M.J.C.; Koopman-Esseboom, C.; Dudink, J.; van Elburg, R.M.; et al. Nutritional Intake, White Matter Integrity, and Neurodevelopment in Extremely Preterm Born Infants. Nutrients 2021, 13, 3409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103409
Hortensius LM, Janson E, van Beek PE, Groenendaal F, Claessens NHP, Swanenburg de Veye HFN, Eijsermans MJC, Koopman-Esseboom C, Dudink J, van Elburg RM, et al. Nutritional Intake, White Matter Integrity, and Neurodevelopment in Extremely Preterm Born Infants. Nutrients. 2021; 13(10):3409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103409
Chicago/Turabian StyleHortensius, Lisa M., Els Janson, Pauline E. van Beek, Floris Groenendaal, Nathalie H. P. Claessens, Henriette F. N. Swanenburg de Veye, Maria J. C. Eijsermans, Corine Koopman-Esseboom, Jeroen Dudink, Ruurd M. van Elburg, and et al. 2021. "Nutritional Intake, White Matter Integrity, and Neurodevelopment in Extremely Preterm Born Infants" Nutrients 13, no. 10: 3409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103409