
Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment and Mediterranean Diet Score Construction
2.3. Assessment of Frailty Index (FI)
2.4. Measurement of Main Covariates
2.5. Statistical Analysis
3. Results
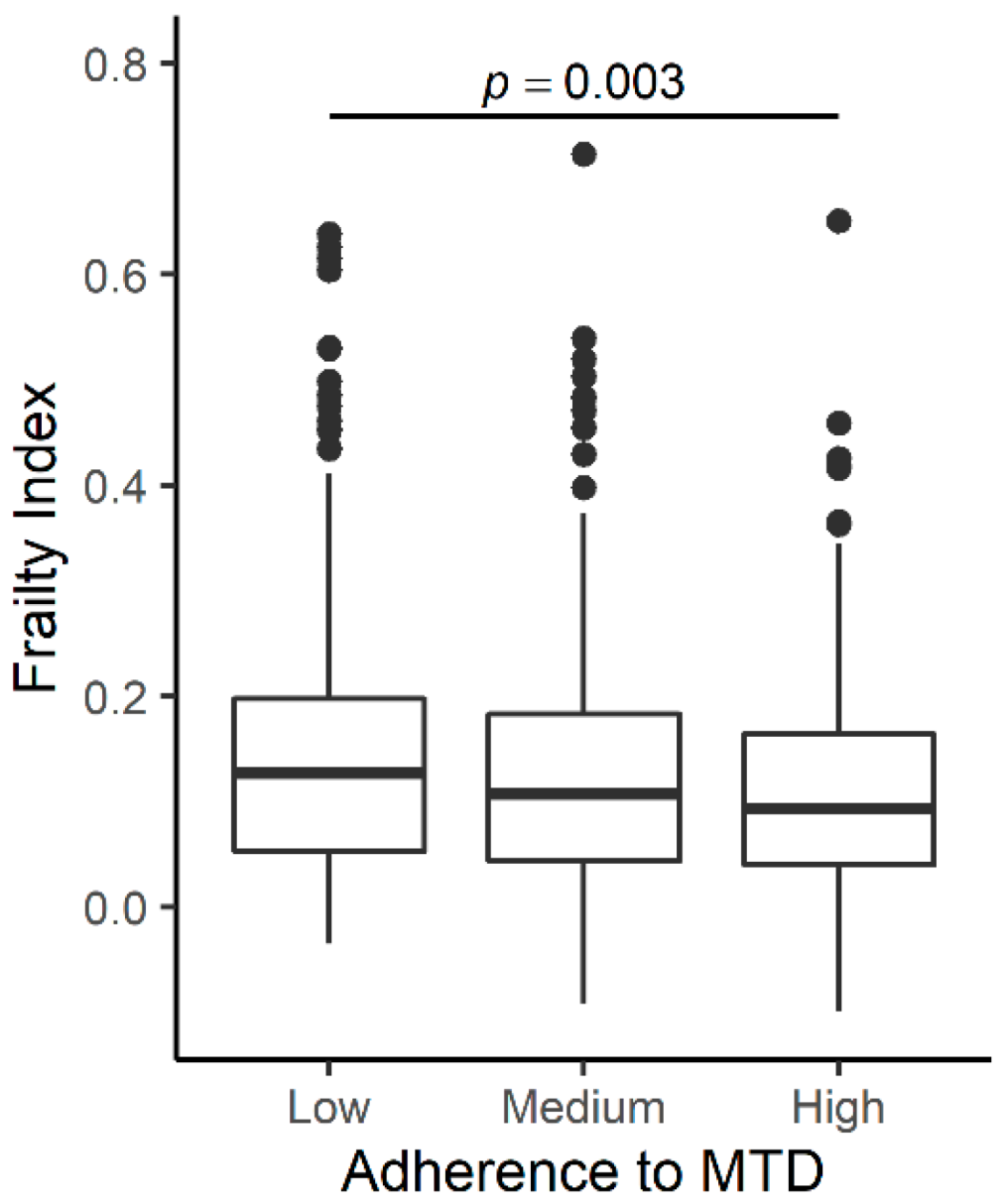
3.1. Association of Mediterranean-Type Diet with FI at Baseline
3.2. Association of the Mediterranean-Type Diet with the Trajectory of FI
3.3. Association of the Mediterranean-Type Diet with the Trajectory of FI by Baseline FI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of Deficits as a Proxy Measure of Aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Hoogendijk, E.O.; Stenholm, S.; Ferrucci, L.; Bandinelli, S.; Inzitari, M.; Cesari, M. Operationalization of a frailty index among older adults in the InCHIANTI study: Predictive ability for all-cause and cardiovascular disease mortality. Aging Clin. Exp. Res. 2020, 32, 1025–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.D.; Alipour-Haris, G.; Pahor, M.; Manini, T.M. Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study. J. Clin. Med. 2020, 9, 3757. [Google Scholar] [CrossRef]
- Fan, J.; Yu, C.; Guo, Y.; Bian, Z.; Sun, Z.; Yang, L.; Chen, Y.; Du, H.; Li, Z.; Lei, Y.; et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: A prospective cohort study. Lancet Public Health 2020, 5, e650–e660. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Colpo, M.; Ferrucci, L.; Bandinelli, S. Adherence to a Mediterranean Diet Protects from Cognitive Decline in the Invecchiare in Chianti Study of Aging. Nutrients 2018, 10, 2007. [Google Scholar] [CrossRef] [Green Version]
- Milaneschi, Y.; Bandinelli, S.; Corsi, A.M.; Lauretani, F.; Paolisso, G.; Dominguez, L.J.; Semba, R.D.; Tanaka, T.; Abbatecola, A.M.; Talegawkar, S.A.; et al. Mediterranean diet and mobility decline in older persons. Exp. Gerontol. 2011, 46, 303–308. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, P.; Wang, Y.; Buchman, A.S.; Bennett, D.A.; Morris, M.C. Dietary Patterns and Self-reported Incident Disability in Older Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 74, 1331–1337. [Google Scholar] [CrossRef]
- Kyprianidou, M.; Panagiotakos, D.; Faka, A.; Kambanaros, M.; Makris, K.C.; Christophi, C.A. Adherence to the Mediterranean diet in Cyprus and its relationship to multi-morbidity: An epidemiological study. Public Health Nutr. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Eleftheriou, D.; Benetou, V.; Trichopoulou, A.; La Vecchia, C.; Bamia, C. Mediterranean diet and its components in relation to all-cause mortality: Meta-analysis. Br. J. Nutr. 2018, 120, 1081–1097. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Bandinelli, S.; Bandeen-Roche, K.; Chen, P.; Milaneschi, Y.; Tanaka, T.; Semba, R.D.; Guralnik, J.M.; Ferrucci, L. A Higher Adherence to a Mediterranean-Style Diet Is Inversely Associated with the Development of Frailty in Community-Dwelling Elderly Men and Women. J. Nutr. 2012, 142, 2161–2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrucci, L.; Bandinelli, S.; Benvenuti, E.; Di Iorio, A.; Macchi, C.; Harris, T.B.; Guralnik, J.M. Subsystems Contributing to the Decline in Ability to Walk: Bridging the Gap Between Epidemiology and Geriatric Practice in the InCHIANTI Study. J. Am. Geriatr. Soc. 2000, 48, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Bartali, B.; Turrini, A.; Salvini, S.; Lauretani, F.; Russo, C.R.; Corsi, A.M.; Bandinelli, S.; D’Amicis, A.; Palli, D.; Guralnik, J.M.; et al. Dietary intake estimated using different methods in two Italian older populations. Arch. Gerontol. Geriatr. 2004, 38, 51–60. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbri, E.; An, Y.; Zoli, M.; Simonsick, E.M.; Guralnik, J.M.; Bandinelli, S.; Boyd, C.M.; Ferrucci, L. Aging and the Burden of Multimorbidity: Associations With Inflammatory and Anabolic Hormonal Biomarkers. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2015, 70, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.A.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontology 1969, 9, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Beekman, A.T.F.; Deeg, D.J.H.; Van Limbeek, J.; Braam, A.W.; De Vries, M.Z.; Van Tilburg, W. Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): Results from a community-based sample of older subjects in The Netherlands. Psychol. Med. 1997, 27, 231–235. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Wareham, N.J.; Jakes, R.W.; Rennie, K.L.; Mitchell, J.; Hennings, S.; Day, N.E. Validity and repeatability of the EPIC-Norfolk Physical Activity Questionnaire. Int. J. Epidemiol. 2002, 31, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Ferrucci, L.; Cherubini, A.; Bandinelli, S.; Bartali, B.; Corsi, A.; Lauretani, F.; Martin, A.; Andres-Lacueva, C.; Senin, U.; Guralnik, J.M. Relationship of Plasma Polyunsaturated Fatty Acids to Circulating Inflammatory Markers. J. Clin. Endocrinol. Metab. 2006, 91, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Dorgan, J.F.; Boakye, N.E.; Fears, T.R.; Schleicher, R.L.; Helsel, W.; Anderson, C.; Robinson, J.; Guin, J.D.; Lessin, S.; Ratnasinghe, L.D.; et al. Serum carotenoids and alpha-tocopherol and risk of nonmelanoma skin cancer. Cancer Epidemiol. Biomark. Prev. 2004, 13, 1276–1282. [Google Scholar]
- Sowell, A.L.; Huff, D.L.; Yeager, P.R.; Caudill, S.P.; Gunter, E.W. Retinol, alpha-tocopherol, lutein/zeaxanthin, beta-cryptoxanthin, lycopene, alpha-carotene, trans-beta-carotene, and four retinyl esters in serum determined simultaneously by reversed-phase HPLC with multiwavelength detection. Clin. Chem. 1994, 40, 411–416. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Morley, J.E. A Comparison of Four Frailty Models. J. Am. Geriatr. Soc. 2014, 62, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Gambassi, G.; van Kan, G.A.; Vellas, B. The frailty phenotype and the frailty index: Different instruments for different purposes. Age Ageing 2014, 43, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Alaghehband, F.R.; Erkkilä, A.T.; Rikkonen, T.; Sirola, J.; Kröger, H.; Isanejad, M. Association of Baltic Sea and Mediterranean diets with frailty phenotype in older women, Kuopio OSTPRE-FPS study. Eur. J. Nutr. 2021, 60, 821–831. [Google Scholar] [CrossRef]
- Kwan, R.Y.; Cheung, D.S.; Lo, S.K.; Ho, L.Y.; Katigbak, C.; Chao, Y.-Y.; Liu, J.Y. Frailty and its association with the Mediterranean diet, life-space, and social participation in community-dwelling older people. Geriatr. Nurs. 2019, 40, 320–326. [Google Scholar] [CrossRef]
- Ntanasi, E.; Yannakoulia, M.; Kosmidis, M.-H.; Anastasiou, C.A.; Dardiotis, E.; Hadjigeorgiou, G.; Sakka, P.; Scarmeas, N. Adherence to Mediterranean Diet and Frailty. J. Am. Med. Dir. Assoc. 2018, 19, 315–322.e2. [Google Scholar] [CrossRef]
- Kojima, G.; Avgerinou, C.; Iliffe, S.; Walters, K. Adherence to Mediterranean Diet Reduces Incident Frailty Risk: Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2018, 66, 783–788. [Google Scholar] [CrossRef] [PubMed]
- De Haas, S.C.M.; De Jonge, E.A.L.; Voortman, T.; Graaff, J.S.-D.; Franco, O.H.; Ikram, M.A.; Rivadeneira, F.; Jong, J.C.K.-D.; Schoufour, J.D. Dietary patterns and changes in frailty status: The Rotterdam study. Eur. J. Nutr. 2017, 57, 2365–2375. [Google Scholar] [CrossRef] [Green Version]
- Bach-Faig, A.; Geleva, D.; Carrasco, J.; Ribas-Barba, L.; Serra-Majem, L. Evaluating associations between Mediterranean diet adherence indexes and biomarkers of diet and disease. Public Health Nutr. 2006, 9, 1110–1117. [Google Scholar] [CrossRef]
- Panagiotakos, D.; Kalogeropoulos, N.; Pitsavos, C.; Roussinou, G.; Palliou, K.; Chrysohoou, C.; Stefanadis, C. Validation of the MedDietScore via the determination of plasma fatty acids. Int. J. Food Sci. Nutr. 2009, 60 (Suppl. 5), 168–180. [Google Scholar] [CrossRef]
- Féart, C.; Torrès, M.J.M.; Samieri, C.; Jutand, M.-A.; Peuchant, E.; Simopoulos, A.P.; Barberger-Gateau, P. Adherence to a Mediterranean diet and plasma fatty acids: Data from the Bordeaux sample of the Three-City study. Br. J. Nutr. 2011, 106, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Razquin, C.; Martinez, J.A.; Martinez-Gonzalez, M.A.; Mitjavila, M.T.; Estruch, R.; Marti, A. A 3 years follow-up of a Mediterranean diet rich in virgin olive oil is associated with high plasma antioxidant capacity and reduced body weight gain. Eur. J. Clin. Nutr. 2009, 63, 1387–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jö Nsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity commissioned by the ILSI Europe Metabolic Syndrome and Diabetes Task Force. Br. J. Nutr. 2011, 106, S1–S78. [Google Scholar] [CrossRef]
- Fitó, M.; Guxens, M.; Corella, D.; Sáez, G.; Estruch, R.; De La Torre, R.; Francés, F.; Cabezas, C.; López-Sabater, M.D.C.; Marrugat, J.; et al. Effect of a Traditional Mediterranean Diet on Lipoprotein Oxidation: A randomized controlled trial. Arch. Intern. Med. 2007, 167, 1195–1203. [Google Scholar] [CrossRef]
- Kipnis, V.; Subar, A.F.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Bingham, S.; Schoeller, D.A.; Schatzkin, A.; Carroll, R.J. Structure of Dietary Measurement Error: Results of the OPEN Biomarker Study. Am. J. Epidemiol. 2003, 158, 14–21, discussion 22–16. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All | Low Adherence | Medium Adherence | High Adherence | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean/n | (SD/%) | Mean/n | (SD/%) | Mean/n | (SD/%) | Mean/n | (SD/%) | p * | |
| n | 825 | 235 | 357 | 233 | |||||
| Age (y) | 73.5 | (6.4) | 75.1 | (7.0) | 73.6 | (6.5) | 71.9 | (5.2) | <0.001 |
| Sex (%Female) | 463 | (56.1) | 131 | (55.7) | 219 | (61.3) | 113 | (48.5) | 0.009 |
| Site (%Bagno a Ripoli) | 441 | (53.5) | 112 | (47.7) | 195 | (54.6) | 134 | (57.5) | 0.086 |
| Smoking (%Smoker) | 118 | (14.3) | 36 | (15.3) | 46 | (12.9) | 36 | (15.5) | 0.596 |
| IL6 (pg/mL) | 2.05 | (3.39) | 2.09 | (2.24) | 1.90 | (1.96) | 2.23 | (5.47) | 0.441 |
| CRP (ug/mL) | 4.59 | (7.39) | 5.40 | (10.73) | 3.89 | (4.45) | 4.87 | (6.83) | 0.035 |
| BMI (kg/m2) | 27.5 | (4.0) | 27.1 | (4.2) | 27.5 | (4.2) | 27.8 | (3.6) | 0.128 |
| Years of Education (y) | 5.58 | (3.31) | 5.53 | (3.67) | 5.45 | (3.10) | 5.85 | (3.23) | 0.311 |
| MMSE | 25.4 | (3.4) | 25.1 | (3.8) | 25.4 | (3.3) | 25.8 | (3.0) | 0.063 |
| Total energy intake (kcal/day) | 1942.7 | (566.1) | 1826.3 | (582.1) | 1917.9 | (571.8) | 2098.1 | (505.7) | <0.001 |
| Plasma α-tocopherol (µmol/L) | 30.4 | (8.3) | 29.4 | (8.3) | 30.9 | (8.3) | 30.8 | (8.2) | 0.081 |
| Plasma α-carotene (µmol/L) | 0.06 | (0.06) | 0.05 | (0.04) | 0.06 | (0.04) | 0.07 | (0.08) | 0.144 |
| Plasma β-carotene (µmol/L) | 0.43 | (0.26) | 0.39 | (0.24) | 0.45 | (0.28) | 0.44 | (0.25) | 0.021 |
| Plasma monosaturated fatty acid * | 33.0 | (3.7) | 32.5 | (3.8) | 33.0 | (3.7) | 33.4 | (3.8) | 0.055 |
| Frailty Index | 0.13 | (0.10) | 0.16 | (0.12) | 0.13 | (0.09) | 0.11 | (0.08) | <0.001 |
| Model without Interaction | Model with Interaction | |||||
|---|---|---|---|---|---|---|
| All participants | ||||||
| Adherence to MTD | Beta | SE | p | Beta | SE | p |
| Low | Reference | Reference | ||||
| Medium | −0.013 | 0.005 | 0.016 | −0.010 | 0.006 | 0.099 |
| High | −0.030 | 0.006 | <0.001 | −0.023 | 0.007 | <0.001 |
| Follow-up time | 0.013 | 0.001 | <0.001 | 0.016 | 0.002 | <0.001 |
| Low × Follow-up time | Reference | |||||
| Medium × Follow-up time | −0.003 | 0.002 | 0.249 | |||
| High × Follow-up time | −0.006 | 0.002 | 0.021 | |||
| Low frailty index at baseline | ||||||
| Adherence to MTD | Beta | SE | p | Beta | SE | p |
| Low | Reference | Reference | ||||
| Medium | −0.001 | 0.004 | 0.820 | 0.002 | 0.005 | 0.612 |
| High | −0.006 | 0.005 | 0.164 | −0.003 | 0.005 | 0.574 |
| Follow-up time | 0.009 | 0.001 | <0.001 | 0.012 | 0.002 | <0.001 |
| Low × Follow-up time | Reference | |||||
| Medium × Follow-up time | −0.004 | 0.002 | 0.040 | |||
| High × Follow-up time | −0.005 | 0.002 | 0.030 | |||
| High frailty index at baseline | ||||||
| Adherence to MTD | Beta | SE | p | Beta | SE | p |
| Low | Reference | Reference | ||||
| Medium | −0.010 | 0.009 | 0.248 | −0.010 | 0.010 | 0.295 |
| High | −0.021 | 0.011 | 0.057 | −0.016 | 0.012 | 0.186 |
| Follow-up time | 0.017 | 0.001 | <0.001 | 0.018 | 0.003 | <0.001 |
| Low × Follow-up time | Reference | |||||
| Medium × Follow-up time | 0.000 | 0.004 | 0.959 | |||
| High × Follow-up time | −0.004 | 0.004 | 0.363 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Bandinelli, S.; Ferrucci, L. Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults. Nutrients 2021, 13, 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041129
Tanaka T, Talegawkar SA, Jin Y, Bandinelli S, Ferrucci L. Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults. Nutrients. 2021; 13(4):1129. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041129
Chicago/Turabian StyleTanaka, Toshiko, Sameera A. Talegawkar, Yichen Jin, Stephania Bandinelli, and Luigi Ferrucci. 2021. "Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults" Nutrients 13, no. 4: 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041129