
Development and Relative Validity of a Semiquantitative Food Frequency Questionnaire to Estimate Dietary Intake among a Multi-Ethnic Population in the Malaysian Cohort Project


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
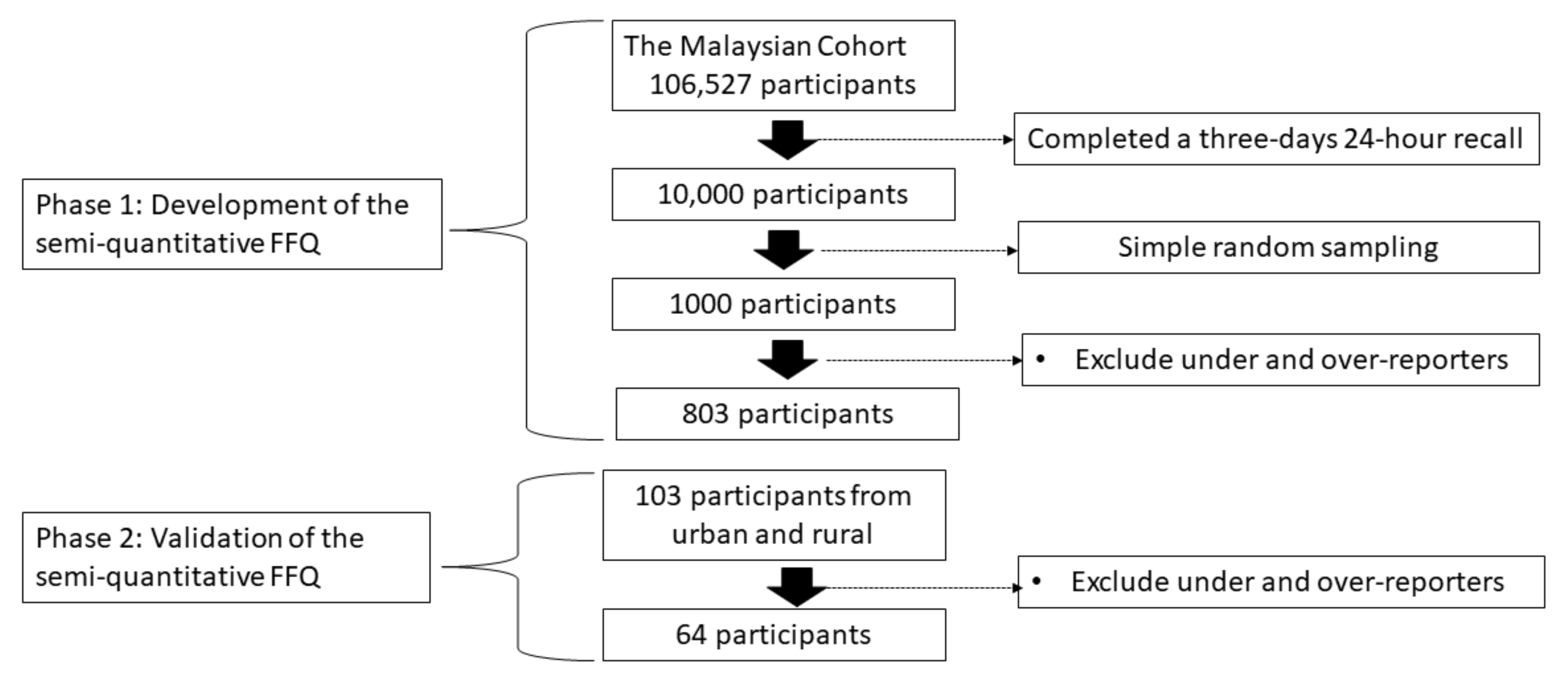
2.1. Study Sample
2.2. Data Collection
2.3. Development of the Food List
2.4. Development of Nutrient Database
2.5. Validation of Food Frequency Questionnaire (FFQ)
2.6. Nutrient Intake Analysis
2.7. Statistical Analysis
3. Results
3.1. The Characteristics of Study Population
3.2. Energy Intake
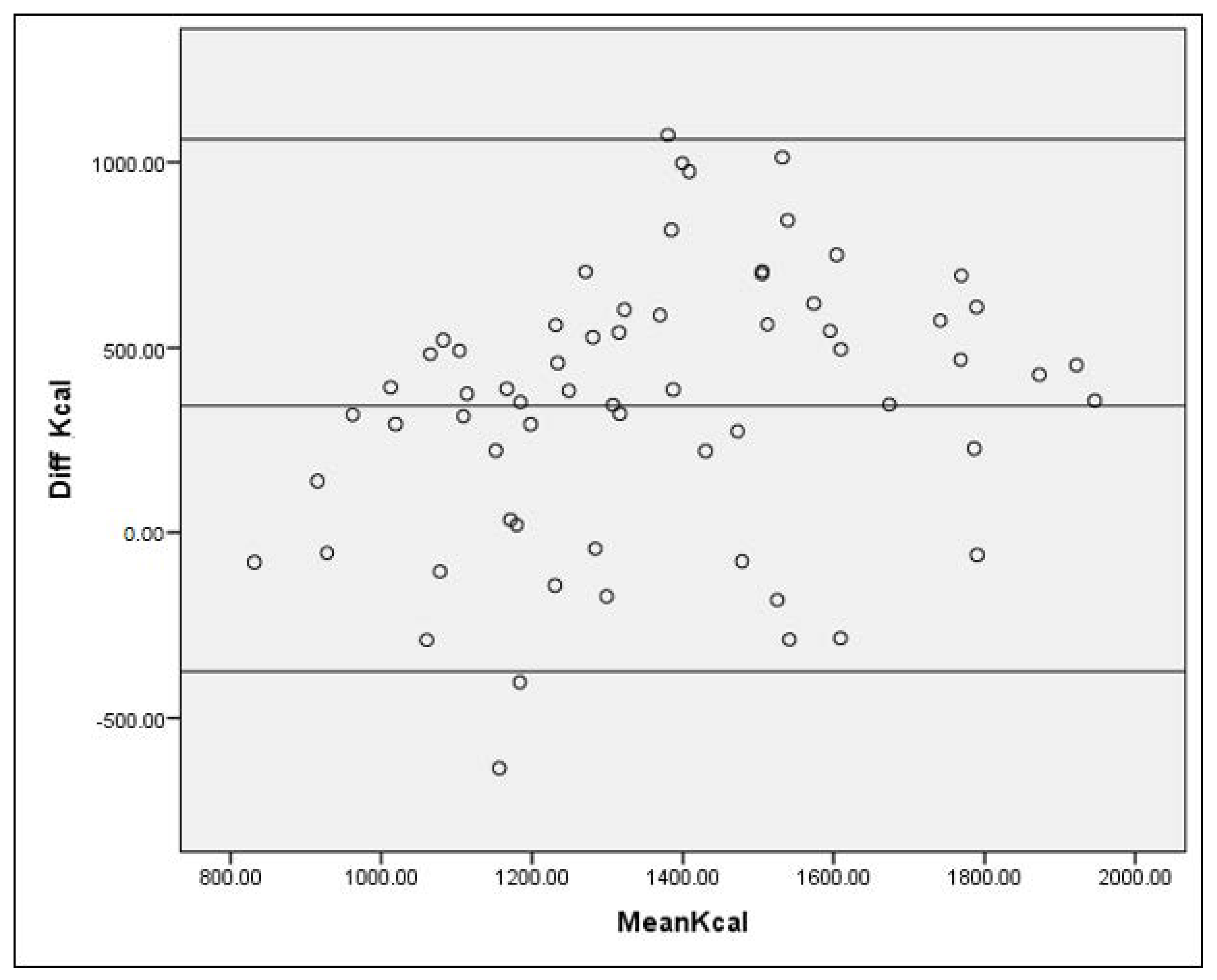
3.3. Comparison between Food Frequency Questionnaire and 24-h Diet Recall
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute for Public Health. National Health and Morbidity Survey 2015 (NHMS 2015). Vol. II: Non-Communicable Diseases, Risk Factors & Other Health Problems; Institute for Public Health: Kuala Lumpur, Malaysia, 2015. Available online: https://www.moh.gov.my/moh/resources/nhmsreport2015vol2.pdf (accessed on 24 January 2020).
- Jamal, R.; Syed Zakaria, S.Z.; Kamaruddin, M.A.; Abd Jalal, N.; Ismail, N.; Mohd Kamil, N.; Abdullah, N.; Baharudin, N.; Hussin, N.H.; Othman, H.; et al. Cohort Profile: The Malaysian Cohort (TMC) project: A prospective study of non-communicable diseases in a multi-ethnic population. Int. J. Epidemiol. 2015, 44, 423–431. [Google Scholar] [CrossRef]
- Sulaiman, S.; Shahril, M.R.; Shaharudin, S.H.; Md Isa, N.; Syed Hussain, S.N.A. Semi-Quantitative Food Frequency Questionnaire for Assessment of Energy, Total Fat, Fatty Acids, and Vitamin A, C and E Intake among Malaysian Women: Comparison with Three Days 24-Hour Diet Recalls. J. Sains Kesihat. Malays. 2008, 6, 75–91. [Google Scholar]
- Satija, A.; Yu, E.; Willett, W.C.; Hu, F.B. Understanding Nutritional Epidemiology and Its Role in Policy. Adv. Nutr. 2015, 6, 5–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, Y.; Bertoia, M.L.; Lenart, E.B.; Stampfer, M.J.; Willett, W.C.; Speizer, F.E.; Chavarro, J.E. Origin, Methods, and Evolution of the Three Nurses’ Health Studies. Am. J. Public Health 2016, 106, 1573–1581. [Google Scholar] [CrossRef]
- Cade, J.E.; Burley, V.J.; Alwan, N.A.; Hutchinson, J.; Hancock, N.; Morris, M.A.; Threapleton, D.E.; Greenwood, D.C. Cohort Profile: The UK Women’s Cohort Study (UKWCS). Int. J. Epidemiol. 2017, 46, e11. [Google Scholar] [CrossRef]
- Gonzalez, C.A. The European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2006, 9, 124–126. [Google Scholar] [CrossRef] [Green Version]
- Dao, M.C.; Subar, A.F.; Warthon-Medina, M.; Cade, J.E.; Burrows, T.; Golley, R.K.; Forouhi, N.G.; Pearce, M.; Holmes, B.A. Dietary assessment toolkits: An overview. Public Health Nutr. 2019, 22, 404–418. [Google Scholar] [CrossRef] [Green Version]
- Khairunnisa, M. The Development of Food Frequency Questionnaire and Assessment of 15-Year-Old Malaysian Adolescent Dietary Intake. Ph.D. Thesis, University of Malaya, Kuala Lumpur, Malaysia, 2018. [Google Scholar]
- Fatihah, F.; Ng, B.; Hazwanie, H.; Norimah, A.; Nik Shanita, S.; Ruzita, A.; Poh, B. Development and validation of a food frequency questionnaire for dietary intake assessment among multi-ethic primary school-aged children. Singap. Med. J. 2015, 56, 687–694. [Google Scholar] [CrossRef] [Green Version]
- Zaleha, M.I.; Khadijah, S.; Bukhary, I.B.N.; Khor, G.L.; Zaleha, A.M.; Haslinda, H.; Hana, Y.N.S.; Hasanain Faisal, G. Development and Validation of a Food Frequency Questionnaire for Vitamin D intake among Urban Pregnant Women in Malaysia. Malays. J. Nutr. 2015, 21, 179–190. [Google Scholar]
- Shahar, S.; Hui Lin, C.; Haron, H. Development and Validation of Food Frequency Questionnaire (FFQ) for Estimation of the Dietary Polyphenol Intake among Elderly Individuals in Klang Valley. J. Sains Kesihat. Malays. 2014, 12. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.K.; Shahar, S.; Yusoff, N.A.M.; Chin, A.-V. Validation of a food frequency questionnaire in assessing the omega-3 polyunsaturated fatty acids intake for Malays and Chinese elderly in Malaysia. Sains Malays. 2013, 42, 1625–1632. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Tee, E.S.; Noor, M.I.; Azudin, M.N.; Idris, K. Nutrient Composition of Malaysian Foods, 4th ed.; Institute for Medical Research: Kuala Lumpur, Malaysia, 1997.
- Energy and Nutrient Composition of Food. Available online: https://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 24 January 2020).
- United States Department of Agriculture: Agricultural Research Service. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 24 January 2020).
- Abdul Manaf, Z.; Shahar, S.; Safii, N.S.; Haron, H. Atlas of Food Exchanges & Portion Sizes, 3rd ed.; MDC: Kuala Lumpur, Malaysia, 2015; ISBN 9679677014587. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Lombard, M.J.; Steyn, N.P.; Charlton, K.E.; Senekal, M. Application and interpretation of multiple statistical tests to evaluate validity of dietary intake assessment methods. Nutr. J. 2015, 14, 40. [Google Scholar] [CrossRef] [Green Version]
- Norimah, A.K.; Safiah, M.; Jamal, K.; Haslinda, S.; Zuhaida, H.; Rohida, S.; Fatimah, S.; Norazlin, S.; Poh, B.K.; Kandiah, M.; et al. Food Consumption Patterns: Findings from the Malaysian Adult Nutrition Survey (MANS). Malays. J. Nutr. 2008, 14, 25–39. [Google Scholar]
- Jayawardena, R.; Swaminathan, S.; Byrne, N.M.; Soares, M.J.; Katulanda, P.; Hills, A.P. Development of a food frequency questionnaire for Sri Lankan adults. Nutr. J. 2012, 11, 63. [Google Scholar] [CrossRef] [Green Version]
- Nöthlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Fitting Portion Sizes in a Self-Administered Food Frequency Questionnaire. J. Nutr. 2007, 137, 2781–2786. [Google Scholar] [CrossRef]
- Abdullah, N.-F.; Teo, P.; Foo, L. Ethnic Differences in the Food Intake Patterns and Its Associated Factors of Adolescents in Kelantan, Malaysia. Nutrients 2016, 8, 551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haftenberger, M.; Heuer, T.; Heidemann, C.; Kube, F.; Krems, C.; Mensink, G.B. Relative validation of a food frequency questionnaire for national health and nutrition monitoring. Nutr. J. 2010, 9, 36. [Google Scholar] [CrossRef] [Green Version]
- Marques-Vidal, P.; Ross, A.; Wynn, E.; Rezzi, S.; Paccaud, F.; Decarli, B. Reproducibility and relative validity of a food-frequency questionnaire for French-speaking Swiss adults. Food Nutr. Res. 2011, 55. [Google Scholar] [CrossRef]
- Liu, X.; Wang, X.; Lin, S.; Song, Q.; Lao, X.; Yu, I.T.-S. Reproducibility and Validity of a Food Frequency Questionnaire for Assessing Dietary Consumption via the Dietary Pattern Method in a Chinese Rural Population. PLoS ONE 2015, 10, e0134627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streppel, M.T.; de Vries, J.H.; Meijboom, S.; Beekman, M.; de Craen, A.J.; Slagboom, P.E.; Feskens, E.J. Relative validity of the food frequency questionnaire used to assess dietary intake in the Leiden Longevity Study. Nutr. J. 2013, 12, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picó, C.; Serra, F.; Rodríguez, A.M.; Keijer, J.; Palou, A. Biomarkers of Nutrition and Health: New Tools for New Approaches. Nutrients 2019, 11, 1092. [Google Scholar] [CrossRef] [Green Version]
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M.; Bronkowska, M.; Dlugosz, A.; Loboda, D.; Wyka, J. Reproducibility of a Questionnaire for Dietary Habits, Lifestyle and Nutrition Knowledge Assessment (KomPAN) in Polish Adolescents and Adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Demographics | Categories | Development | Validation | ||||
|---|---|---|---|---|---|---|---|
| Men | Women | Total | Men | Women | Total | ||
| (n = 329) | (n = 474) | (n = 803) | (n = 25) | (n = 39) | (n = 64) | ||
| Age, mean (SD) years | 50.5 (7.9) | 48.3 (7.4) | 49.2 (7.7) | 58.6 (6.6) | 54.8 (6.0) | 56.3 (6.5) | |
| Age group, n (%) (years) | 40 to 49 | 147 (44.7) | 262 (55.3) | 409 (50.9) | 3 (12.0) | 8 (20.5) | 11 (17.2) |
| 50 to 59 | 134 (40.7) | 175 (36.9) | 309 (38.5) | 11 (44.0) | 22 (56.4) | 33 (51.6) | |
| 60 and above | 48 (14.6) | 37 (7.8) | 85 (10.6) | 11 (44.0) | 9 (23.1) | 20 (31.3) | |
| BMI, mean (SD) kg/m2 | 25.5 (4.0) | 25.8 (4.9) | 25.5 (4.0) | 25.7 (3.7) | 26.0 (4.3) | 25.9 (4.0) | |
| BMI classification, n (%) | Underweight | 13 (4.0) | 20 (4.2) | 13 (4.0) | 1 (4.0) | 1 (2.6) | 2 (3.1) |
| Normal weight | 139 (42.2) | 197 (41.6) | 139 (42.2) | 9 (36.0) | 16 (41.0) | 25 (39.1) | |
| Overweight | 139 (42.2) | 184 (38.8) | 139 (42.2) | 12 (48.0) | 14 (35.9) | 26 (40.6) | |
| Obese | 38 (11.6) | 73 (15.4) | 38 (11.6) | 3 (12.0) | 8 (20.5) | 11 (17.2) | |
| Ethnicity, n (%) | Malay | 178 (54.1) | 176 (37.1) | 178 (54.1) | 17(68.0) | 18 (46.2) | 35 (54.7) |
| Chinese | 79 (24.0) | 180 (38.0) | 79 (24.0) | 7 (28.0) | 18 (46.2) | 25 (39.1) | |
| Indian | 38 (11.6) | 84 (17.7) | 38 (11.6) | 1 (4.0) | 3 (7.7) | 4 (6.2) | |
| Others | 34 (10.3) | 34 (7.2) | 34 (10.3) | ||||
| Place of residence, n (%) | Rural | 158 (48.0) | 231 (48.7) | 158 (48.0) | 17 (68.0) | 16 (41.0) | 33 (51.6) |
| Urban | 171 (52.0) | 243 (51.3) | 171 (52.0) | 8 (32.0) | 23 (59.0) | 31 (48.4) | |
| Education level, n (%) | No schooling | 5 (1.5) | 10 (2.1) | 15 (1.9) | 1 (4.0) | 2 (5.1) | 3 (4.7) |
| Primary | 87 (26.4) | 127 (26.8) | 214 (26.7) | 16 (64.0) | 14 (35.9) | 30 (46.9) | |
| Secondary | 140 (42.6) | 213 (44.9) | 353 (44.0) | 6 (24.0) | 15 (38.5) | 21 (32.8) | |
| Tertiary | 97 (29.5) | 124 (26.2) | 221 (27.5) | 2 (24.0) | 8 (20.5) | 10 (15.6) | |
| Household income (USD), n (%) | <USD 241 | 0 (0) | 2 (5.10) | 2 (3.10) | |||
| USD 241–481.77 | 7 (28.00) | 12 (30.80) | 19 (29.70) | ||||
| USD 482.01–722.77 | 11 (44.00) | 5 (12.80) | 16 (25.00) | ||||
| USD 723.01–963.78 | 2 (8.00) | 5 (12.80) | 7 (10.90) | ||||
| USD 964.02–1204.78 | 4 (16.00) | 3 (7.70) | 7 (10.90) | ||||
| USD 1205.03–1686.79 | 0 (0) | 4 (10.30) | 4 (6.30) | ||||
| USD 1687.04–2409.81 | 1 (4.00) | 5 (12.80) | 6 (9.40) | ||||
| >USD 2410.05 | 0 (0) | 3 (7.70) | 3 (4.70) | ||||
| Parameters | Men | Women | Total | p-Value 1 |
|---|---|---|---|---|
| (n = 329) | (n = 474) | (n = 803) | ||
| Energy (kcal/day) | 1741 (437) | 1589 (339) | 1651 (389) | <0.01 |
| Carbohydrates (g/day) | 224.9 (68.2) | 199.9 (52.7) | 210.2 (60.8) | <0.01 |
| % from energy | 52.0 (10.1) | 50.6 (10.0) | 51.2 (10.1) | |
| Protein (g) | 77.2 (36.6) | 72.8 (25.9) | 74.6 (30.8) | 0.06 |
| % from energy | 17.7 (6.7) | 18.3 (5.1) | 18.1 (5.8) | |
| Total fat (g) | 60.8 (29.1) | 55.6 (20.9) | 57.7 (24.8) | 0.01 |
| % from energy | 31.1 (11.8) | 31.1 (7.7) | 31.1 (9.6) | |
| Calcium (mg) | 484.9 (235.9) | 474.7 (266.5) | 478.9 (254.3) | 0.58 |
| Phosphorus (mg) | 1006.1 (535.5) | 919.3 (421.6) | 954.9 (473.2) | 0.14 |
| Iron (mg) | 15.6 (8.7) | 14.3 (6.2) | 14.9 (7.3) | 0.02 |
| Sodium (mg) | 3217.3 (2063.2) | 3132.3 (2180.3) | 3167.2 (2132.2) | 0.58 |
| Potassium (mg) | 1512.3 (969.8) | 1400.1 (650.0) | 1446.1 (798.1) | 0.07 |
| Zinc (mg) | 5.2 (4.3) | 5.5 (5.0) | 5.4 (4.72) | 0.4 |
| Vitamin A (µg) | 722.0 (883.3) | 597.9 (1715.2) | 648.7 (1434.5) | 0.23 |
| Vitamin B1 (mg) | 0.8 (0.5) | 0.8 ± 0.4 | 0.8 (0.4) | 0.22 |
| Vitamin B2 (mg) | 1.3 (0.9) | 1.2 (0.6) | 1.2 (0.7) | 0.04 |
| Vitamin B3 (mg) | 9.2 (5.4) | 8.7 (4.8) | 8.9 (5.1) | 0.11 |
| Vitamin C (mg) | 115.9 (342.0) | 156.1 (252.2) | 139.6 (292.7) | 0.47 |
| Food Categories | Total Food Items and Mixed Dishes 1 | Grouping of Food Items 2 | Contribution of 90% 3 | Inclusion of Foods 4 | Final Food Items 5 |
|---|---|---|---|---|---|
| Cereal | 104 | 26 | 26 | 7 | 33 |
| Meat | 68 | 16 | 15 | 5 | 20 |
| Fish and shellfish | 143 | 15 | 15 | 5 | 20 |
| Egg | 10 | 3 | 3 | 0 | 3 |
| Vegetables | 128 | 20 | 19 | 2 | 21 |
| Tuber and starch | 11 | 4 | 3 | 1 | 4 |
| Soy products | 17 | 3 | 3 | 2 | 5 |
| Beans and legumes | 13 | 3 | 3 | 1 | 4 |
| Fruits | 30 | 18 | 17 | 3 | 20 |
| Milk and milk products | 17 | 6 | 4 | 5 | 9 |
| Fast foods | 16 | 7 | 6 | 7 | 13 |
| Beverages | 71 | 16 | 16 | 2 | 18 |
| Alcoholic beverages | 0 | 0 | 0 | 3 | 3 |
| Traditional snacks and confectionaries | 104 | 9 | 9 | 4 | 13 |
| Condiments and gravies | 21 | 7 | 6 | 0 | 6 |
| Spreads | 8 | 6 | 4 | 3 | 7 |
| Sweetener | 2 | 2 | 2 | 2 | 4 |
| Total | 763 | 161 | 151 | 52 | 203 |
| Nutrient (Unit) | FFQ | 3DR | p-Value 1 | S.C.C., rs | I.C.C. | S.Q. (%) | S.A.Q. (%) | O.Q. (%) | Q.W.K. |
|---|---|---|---|---|---|---|---|---|---|
| Median (I.Q.R.) | Median (I.Q.R.) | ||||||||
| Energy (kcal) | 1495 (1148–1615) | 1152 (959–1385) | <0.001 ** | .364 ** | 0.53 ** | 40.6 | 70.3 | 7.8 | 0.25 (0.01 to 0.49) |
| Carbohydrates (g) | 201 (177.2–246.5) | 167.9 (131.0–190.5) | <0.001 ** | .456 ** | 0.59 ** | 34.4 | 68.8 | 3.1 | 0.45 (0.24 to 0.66) |
| Protein (g) | 56.9 (47.7–71.1) | 48.4 (38.8–62.7) | 0.003 ** | .329 ** | 0.52 ** | 42.2 | 81.3 | 4.7 | 0.30 (0.09 to 0.51) |
| Fat (g) | 50.2 (39.7–59.3) | 34.9 (26.6–44.5) | <0.001 ** | .316 * | 0.44 * | 42.2 | 70.3 | 3.1 | 0.35 (0.13 to 0.57) |
| Calcium (mg) | 453.2 (323.2–545.7) | 363.4 (274.8–474.8) | 0.010 * | .312 * | −0.01 | 28.1 | 73.4 | 4.7 | 0.30 (0.09 to 0.51) |
| Phosphorus (mg) | 834.5 (697.3–1004.8) | 631 (508.2–829.0) | <0.001 ** | .301 * | 0.48 ** | 34.4 | 71.9 | 6.3 | 0.28 (0.05 to 0.50) |
| Iron (mg) | 12.32 (8.6–15.3) | 10.2 (7.5–13.9) | 0.1 | 0.425 ** | 0.38 * | 42.2 | 79.7 | 6.3 | 0.40 (0.18 to 0.62) |
| Sodium (mg) | 1520.2 (1230.7–1968.3) | 1618.9 (1240.0–2307.0) | 0.07 | 0.291 * | 0.48 ** | 28.1 | 75 | 6.3 | 0.29 (0.07 to 0.51) |
| Potassium (mg) | 1325.5 (988.1–1783.3) | 1099 (840.8–1406.3) | 0.002 ** | 0.326 ** | 0.523 ** | 37.5 | 76.6 | 4.7 | 0.38 (0.16 to 0.59) |
| Vitamin A (µg) | 665.5 (349.8–617.0) | 495.2 (349.8–617.0) | <0.001 ** | 0.303 * | 0.50 ** | 29.7 | 71.9 | 4.7 | 0.29 (0.07 to 0.50) |
| Vitamin C (mg) | 92.1 (53.8–145.7) | 57.1 (33.7–117.8) | 0.01 * | 0.239 | 0.40 * | 29.7 | 62.5 | 4.7 | 0.18 (−0.05 to 0.40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahar, S.; Shahril, M.R.; Abdullah, N.; Borhanuddin, B.; Kamaruddin, M.A.; Yusuf, N.A.M.; Dauni, A.; Rosli, H.; Zainuddin, N.S.; Jamal, R. Development and Relative Validity of a Semiquantitative Food Frequency Questionnaire to Estimate Dietary Intake among a Multi-Ethnic Population in the Malaysian Cohort Project. Nutrients 2021, 13, 1163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041163
Shahar S, Shahril MR, Abdullah N, Borhanuddin B, Kamaruddin MA, Yusuf NAM, Dauni A, Rosli H, Zainuddin NS, Jamal R. Development and Relative Validity of a Semiquantitative Food Frequency Questionnaire to Estimate Dietary Intake among a Multi-Ethnic Population in the Malaysian Cohort Project. Nutrients. 2021; 13(4):1163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041163
Chicago/Turabian StyleShahar, Suzana, Mohd Razif Shahril, Noraidatulakma Abdullah, Boekhtiar Borhanuddin, Mohd Arman Kamaruddin, Nurul Ain Md Yusuf, Andri Dauni, Hanisah Rosli, Nurzetty Sofia Zainuddin, and Rahman Jamal. 2021. "Development and Relative Validity of a Semiquantitative Food Frequency Questionnaire to Estimate Dietary Intake among a Multi-Ethnic Population in the Malaysian Cohort Project" Nutrients 13, no. 4: 1163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041163