
Impact of COVID-19 Pandemic on Serum Vitamin D Level among Infants and Toddlers: An Interrupted Time Series Analysis and before-and-after Comparison

 ,
,  , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcomes and Covariates
2.3. Data Analysis
2.4. Ethical Approval
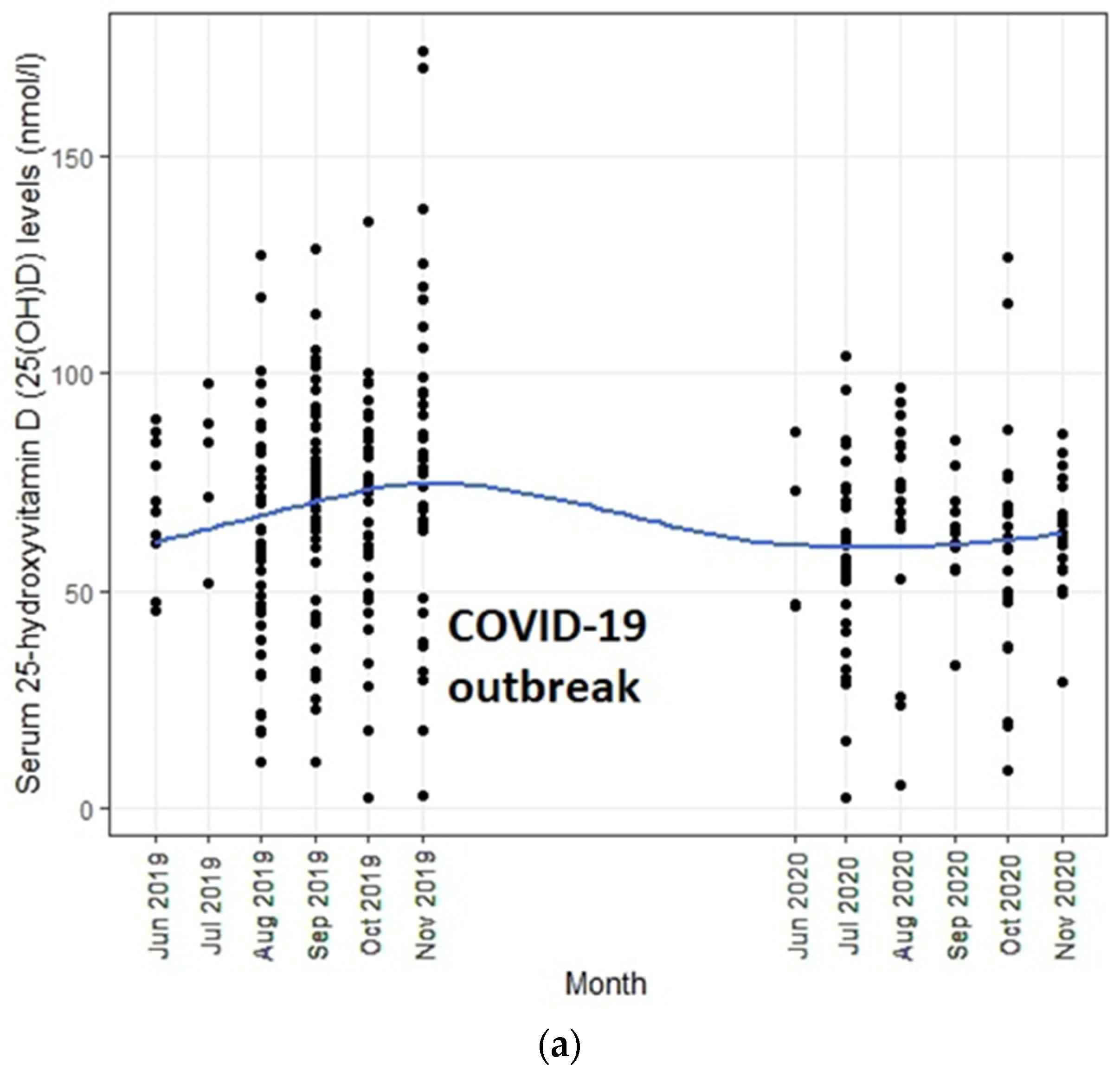
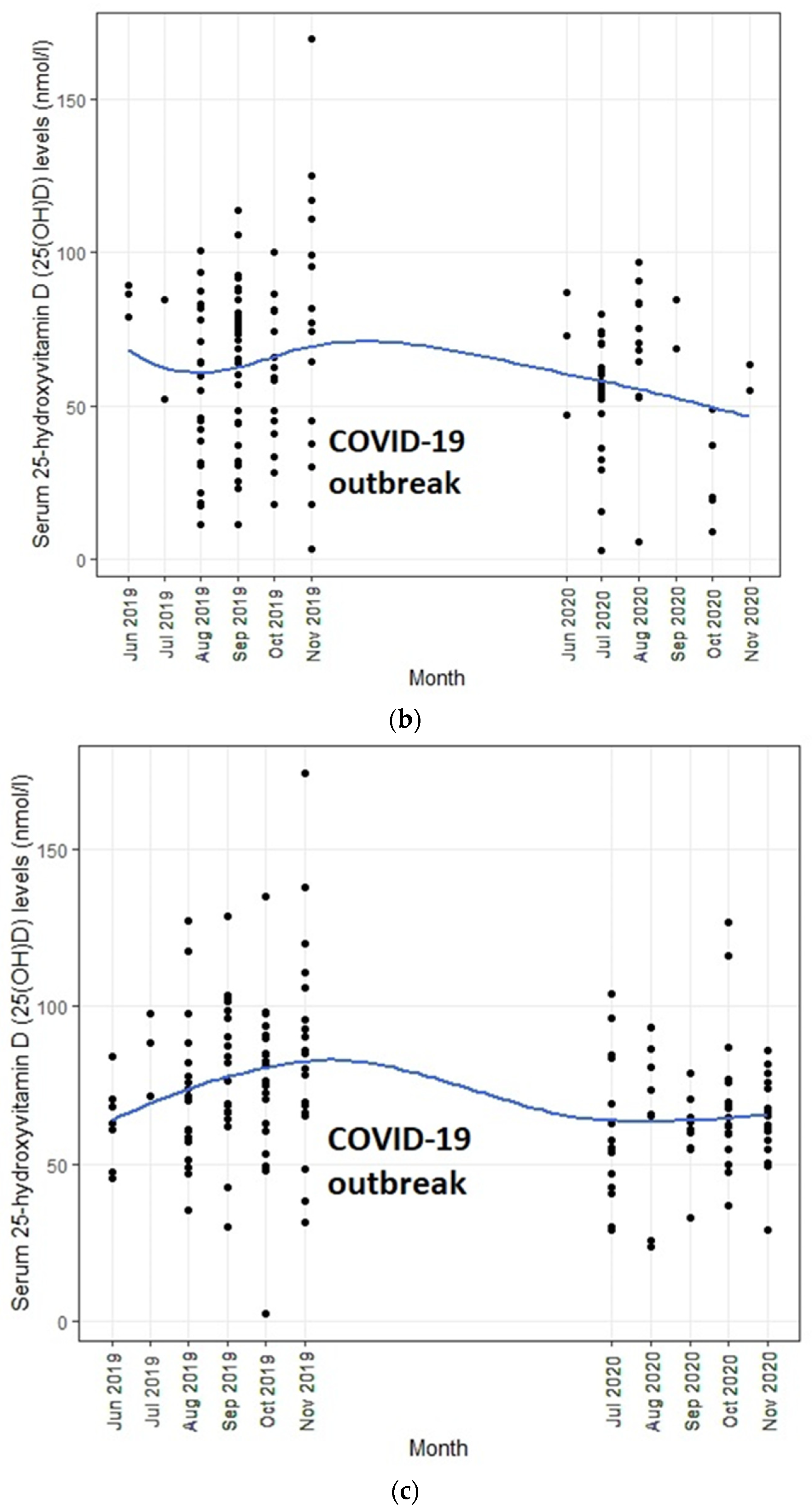
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| UV | Ultraviolet |
| 25(OH)D | 25-hydroxyvitamin D |
| COVID-19 | coronavirus disease 2019 |
| WHO | World Health Organization |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| ITS | Interrupted time series |
References
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus disease 2019 (COVID-19): A perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [Green Version]
- Hick, J.L.; Biddinger, P.D. Novel coronavirus and old lessons—Preparing the health system for the pandemic. N. Engl. J. Med. 2020, 382, e55. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cheung, E. China coronavirus: Death toll almost doubles in one day as Hong Kong reports its first two cases. South China Morning Post, 23 January 2020. [Google Scholar]
- Zuo, M.; Cheng, L.; Yan, A.; Yau, C. Hong Kong takes emergency measures as mystery ‘pneumonia’ infects dozens in China’s Wuhan city. South China Morning Post, 31 December 2019. [Google Scholar]
- Fong, M.W.; Gao, H.; Wong, J.Y.; Xiao, J.; Shiu, E.Y.; Ryu, S.; Cowling, B.J. Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings—Social distancing measures. Emerg. Infect. Dis. 2020, 26, 976. [Google Scholar] [CrossRef]
- Wong, S.-Y.; Kwong, R.-S.; Wu, T.C.; Chan, J.; Chu, M.; Lee, S.; Wong, H.; Lung, D. Risk of nosocomial transmission of coronavirus disease 2019: An experience in a general ward setting in Hong Kong. J. Hosp. Infect. 2020, 105, 119–127. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.; Tsang, T.K.; Li, J.C.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Nowson, C.A.; McGrath, J.J.; Ebeling, P.R.; Haikerwal, A.; Daly, R.M.; Sanders, K.M.; Seibel, M.J.; Mason, R.S. Vitamin D and health in adults in Australia and New Zealand: A position statement. Med. J. Aust. 2012, 196, 686–687. [Google Scholar] [CrossRef]
- Yu, L.; Ke, H.-J.; Che, D.; Luo, S.-L.; Guo, Y.; Wu, J.-L. Effect of Pandemic-Related Confinement on Vitamin D Status Among Children Aged 0–6 Years in Guangzhou, China: A Cross-Sectional Study. Risk Manag. Healthc. Policy 2020, 13, 2669. [Google Scholar] [CrossRef]
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [CrossRef] [Green Version]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Yousfi, N.; Bragazzi, N.L.; Briki, W.; Zmijewski, P.; Chamari, K. The COVID-19 pandemic: How to maintain a healthy immune system during the lockdown–a multidisciplinary approach with special focus on athletes. Biol. Sport 2020, 37, 211. [Google Scholar] [CrossRef]
- Wagner, C.L.; Greer, F.R. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics 2008, 122, 1142–1152. [Google Scholar] [CrossRef] [Green Version]
- Nowson, C.A.; Margerison, C. Vitamin D intake and vitamin D status of Australians. Med. J. Aust. 2002, 177, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.; Tam, W.; Chan, M.; Chan, R.; Li, A. Vitamin D deficiency among healthy infants in Hong Kong: A pilot study. Hong Kong Med. J. 2018, 24, 32–35. [Google Scholar]
- Allen, K.J.; Koplin, J.J.; Ponsonby, A.-L.; Gurrin, L.C.; Wake, M.; Vuillermin, P.; Martin, P.; Matheson, M.; Lowe, A.; Robinson, M. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef]
- Wang, S.S.; Hon, K.L.; Kong, A.P.S.; Pong, H.N.H.; Wong, G.W.K.; Leung, T.F. Vitamin D deficiency is associated with diagnosis and severity of childhood atopic dermatitis. Pediatr. Allergy Immunol. 2014, 25, 30–35. [Google Scholar] [CrossRef]
- Holick, M.F. Resurrection of vitamin D deficiency and rickets. J. Clin. Investig. 2006, 116, 2062–2072. [Google Scholar] [CrossRef] [Green Version]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2016, 46, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Yetley, E.A.; Pfeiffer, C.M.; Schleicher, R.L.; Phinney, K.W.; Lacher, D.A.; Christakos, S.; Eckfeldt, J.H.; Fleet, J.C.; Howard, G.; Hoofnagle, A.N.; et al. Vitamin D Roundtable on the NHANES Monitoring of Serum 25D: Assay Challenges Options for Resolving Them. NHANES Monitoring of Serum 25-Hydroxyvitamin D: A Roundtable Summary. J. Nutr. 2010, 140, 2030S–2045S. [Google Scholar] [CrossRef] [Green Version]
- Leung, Y.K.; Cheng, Y.Y.; Ginn, E.W.L. Technical Note (Local) No. 80—Solar Ultraviolet Index in Hong Kong, 1999–2003; Hong Kong Observatory: Hong Kong, China, 2004. [Google Scholar]
- Vanicek, K.; Frei, T.; Litynska, Z.; Schmalwieser, A. UV-Index for the Public; Publication of the European Communities: Brussels, Belgium, 2000. [Google Scholar]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Durbin, J.; Watson, G.S. Testing for serial correlation in least squares regression: I. Biometrika 1950, 37, 409–428. [Google Scholar] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Inoue, M.; Binns, C.W. Introducing Solid Foods to Infants in the Asia Pacific Region. Nutrients 2014, 6, 276–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, H.; Xinghua, Z.; Yuesi, W. Variability in UVB radiation in Beijing, China. Photochem. Photobiol. 2013, 89, 745–750. [Google Scholar] [CrossRef]
- Griffin, G.; Hewison, M.; Hopkin, J.; Kenny, R.; Quinton, R.; Rhodes, J.; Subramanian, S.; Thickett, D. Vitamin D and COVID-19: Evidence and recommendations for supplementation. R. Soc. Open Sci. 2020, 7, 201912. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, J.Y.; Wei, R.; Hu, S.; Lin, T.; Lash, G.E.; Tan, M. Serum 25 hydroxyvitamin D status in 6-month-old infants in Guangzhou, China: A paired longitudinal follow up study. Matern. Child Nutr. 2020, 16, e12924. [Google Scholar] [CrossRef]
- Halicioglu, O.; Aksit, S.; Koc, F.; Akman, S.A.; Albudak, E.; Yaprak, I.; Coker, I.; Colak, A.; Ozturk, C.; Gulec, E.S. Vitamin D deficiency in pregnant women and their neonates in spring time in western Turkey. Paediatr. Perinat. Epidemiol. 2012, 26, 53–60. [Google Scholar] [CrossRef]
- Hawk, J. Safe, mild ultraviolet-B exposure: An essential human requirement for vitamin D and other vital bodily parameter adequacy: A review. Photodermatol. Photoimmunol. Photomed. 2020, 36, 417–423. [Google Scholar] [CrossRef]
- Tso, W.W.; Wong, R.S.; Tung, K.T.; Rao, N.; Fu, K.W.; Yam, J.C.; Chua, G.T.; Chen, E.Y.; Lee, T.M.; Chan, S.K. Vulnerability and resilience in children during the COVID-19 pandemic. Eur. Child Adolesc. Psychiatry 2020, 1–16. [Google Scholar] [CrossRef]
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O’Hare, D.; Schanler, R.J.; Eidelman, A.I. Breastfeeding and the use of human milk. Pediatrics 2005, 115, 496–506. [Google Scholar]
- Ziegler, E.E.; Hollis, B.W.; Nelson, S.E.; Jeter, J.M. Vitamin D deficiency in breastfed infants in Iowa. Pediatrics 2006, 118, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Dawodu, A.; Tsang, R.C. Maternal Vitamin D Status: Effect on Milk Vitamin D Content and Vitamin D Status of Breastfeeding Infants. Adv. Nutr. 2012, 3, 353–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisse, K.; Winkler, S.; Hirche, F.; Herberth, G.; Hinz, D.; Bauer, M.; Röder, S.; Rolle-Kampczyk, U.; von Bergen, M.; Olek, S.; et al. Maternal and newborn vitamin D status and its impact on food allergy development in the German LINA cohort study. Allergy 2013, 68, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Hoogenboezem, T.; Degenhart, H.; De Muinck Keizer-Schrama, S.; Bouillon, R.; Grose, W.; Hackeng, W.; Visser, H. Vitamin D metabolism in breast-fed infants and their mothers. Pediatr. Res. 1989, 25, 623–628. [Google Scholar] [CrossRef] [Green Version]
- Wagner, C.L.; Hulsey, T.C.; Fanning, D.; Ebeling, M.; Hollis, B.W. High-dose vitamin D3 supplementation in a cohort of breastfeeding mothers and their infants: A 6-month follow-up pilot study. Breastfeed. Med. 2006, 1, 59–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Overall (n = 303) | 2–6 Months (n = 140) | 7–24 Months (n = 163) | ||||
|---|---|---|---|---|---|---|
| Age (months), mean (SD) | 10.42 (6.37) | 4.54 (1.52) | 15.47 (4.24) | |||
| Gender, n(%) | ||||||
| Male | 147 (48.51) | 70 (50.00) | 77 (47.24) | |||
| Female | 156 (51.49) | 70 (50.00) | 86 (52.76) | |||
| Serum 25(OH)D level (nmol/L) | n | mean(SD) | n | mean(SD) | n | mean(SD) |
| Before the COVID-19 outbreak | 183 | 70.58 (28.53) | 93 | 64.17 (29.58) | 90 | 77.20 (25.94) |
| June 2019 | 10 | 69.51 (15.46) | 3 | 84.93 (5.46) | 7 | 62.90 (13.37) |
| July 2019 | 5 | 78.86 (17.71) | 2 | 68.15 (22.98) | 3 | 86.00 (13.12) |
| August 2019 | 44 | 61.02 (26.59) | 23 | 51.84 (27.13) | 21 | 71.08 (22.52) |
| September 2019 | 53 | 71.70 (24.68) | 34 | 66.97 (24.45) | 19 | 80.16 (23.35) |
| October 2019 | 36 | 68.60 (25.82) | 15 | 58.85 (23.32) | 21 | 75.57 (25.76) |
| November 2019 | 35 | 82.04 (38.43) | 16 | 76.54 (43.54) | 19 | 86.67 (34.06) |
| After the COVID-19 outbreak | 120 | 61.00 (20.85) | 47 | 55.60 (22.55) | 73 | 64.48 (19.04) |
| June 2020 | 4 | 63.35 (19.82) | 4 | 63.35 (19.81) | 0 | 0.00 (0.00) |
| July 2020 | 38 | 56.85 (21.08) | 22 | 52.51 (19.16) | 16 | 62.83 (22.73) |
| August 2020 | 19 | 66.28 (24.88) | 11 | 67.65 (24.96) | 8 | 64.39 (26.34) |
| September 2020 | 13 | 63.33 (12.47) | 2 | 76.59 (11.47) | 11 | 60.92 (11.48) |
| October 2020 | 25 | 60.49 (26.27) | 5 | 26.81 (15.87) | 20 | 68.91 (21.10) |
| November 2020 | 21 | 62.46 (12.72) | 3 | 57.83 (4.94) | 18 | 63.23 (13.53) |
| Before the COVID-19 Outbreak (June to November 2019) | After the COVID-19 Outbreak (June to November 2020) | |||||
|---|---|---|---|---|---|---|
| Within-Group | Within-Group | Between-Group a | ||||
| β (95%CI) | p-Value | β (95%CI) | p-Value | β (95%CI) | p-Value | |
| Overall (n = 303) | ||||||
| Unadjusted | 3.36 (0.28, 6.44) | 0.033 | 0.78 (−1.60, 3.16) | 0.519 | −9.57 (−15.53, −3.62) | 0.002 |
| Adjusted for age and sex | 3.30 (0.28, 6.32) | 0.032 | −0.63 (−3.25, 1.98) | 0.631 | −11.16 (−17.07, −5.26) | <0.001 |
| Additional adjustment for UV | 3.03 (−3.51, 9.58) | 0.361 | −5.91 (−13.78, 1.97) | 0.140 | −10.55 (−16.64, −4.45) | <0.001 |
| Additional adjustment for UV and month | - | - | - | - | −10.79 (−16.89, −4.69) | <0.001 |
| 2–6 months (n = 140) | ||||||
| Unadjusted | 2.93 (−2.11, 7.96) | 0.251 | −2.58 (−7.49, 2.33) | 0.296 | −8.57 (−18.28, 1.14) | 0.083 |
| Adjusted for age and sex | 2.85 (−2.17, 7.86) | 0.263 | −3.25 (−8.21, 1.70) | 0.193 | −9.35 (−19.23, 0.52) | 0.063 |
| Additional adjustment for UV | 1.88 (−8.53, 12.29) | 0.720 | −13.39 (−23.99, −2.80) | 0.015 | −7.24 (−18.79, 4.31) | 0.217 |
| Additional adjustment for UV and month | - | - | - | - | −7.21 (−18.81, 4.39) | 0.221 |
| 7–24 months (n = 163) | ||||||
| Unadjusted | 3.66 (−0.003, 7.33) | 0.050 | 0.61 (−2.41, 3.62) | 0.690 | −12.72 (−19.91, −5.53) | <0.001 |
| Adjusted for age and sex | 3.88 (0.22, 7.53) | 0.038 | −0.40 (−3.55, 2.74) | 0.798 | −12.83 (−20.00, −5.65) | <0.001 |
| Additional adjustment for UV | 4.13 (−4.36, 12.61) | 0.336 | 3.55 (−8.71, 15.80) | 0.565 | −12.75 (−19.94, −5.56) | <0.001 |
| Additional adjustment for UV and month | - | - | - | - | −13.34 (−20.45, −6.22) | <0.001 |
| Model 1 | Model 2 a | Model 3 b | ||||
|---|---|---|---|---|---|---|
| β (95%CI) | p-Value | β (95%CI) | p-Value | β (95%CI) | p-Value | |
| Overall (n = 303) | ||||||
| Time | 3.36 (0.58, 6.15) | 0.018 | 3.31 (0.59, 6.03) | 0.017 | 1.67 (−2.45, 5.80) | 0.425 |
| COVID-19 | −26.00 (−53.01, 1.01) | 0.059 | −12.67 (−39.93, 14.59) | 0.361 | 26.08 (−52.26, 104.42) | 0.513 |
| Time since COVID-19 | −2.59 (−6.60, 1.43) | 0.206 | −4.24 (−8.26, −0.22) | 0.039 | −6.32 (−11.95, −0.69) | 0.028 |
| 2–6 months (n = 140) | ||||||
| Time | 2.93 (−1.73, 7.58) | 0.216 | 2.96 (−1.67, 7.61) | 0.208 | −0.67 (−7.31, 5.96) | 0.841 |
| COVID-19 | 3.13 (−45.60, 51.86) | 0.899 | −0.24 (−48.86, 48.38) | 0.992 | 78.04 (−35.20, 191.27) | 0.175 |
| Time since COVID-19 | −5.50 (−12.99, 1.99) | 0.149 | −5.25 (−12.76, 2.26) | 0.169 | −9.02 (−17.98, −0.06) | 0.048 |
| 7–24 months (n = 163) | ||||||
| Time | 3.66 (0.39, 6.93) | 0.028 | 3.85 (0.63, 7.08) | 0.020 | 5.16 (−0.18, 10.49) | 0.058 |
| COVID-19 | −28.84 (−63.80, 6.12) | 0.105 | −23.87 (−59.06, 11.32) | 0.182 | −57.56 (−172.98, 57.87) | 0.326 |
| Time since COVID-19 | −3.06 (−7.89, 1.78) | 0.214 | −3.85 (−8.71, 1.00) | 0.119 | −1.91 (−9.91, 6.09) | 0.638 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, R.S.; Tung, K.T.S.; So, H.-K.; Wong, W.H.S.; Wong, S.Y.; Tsang, H.W.; Tung, J.Y.L.; Chua, G.T.; Ho, M.H.K.; Wong, I.C.K.; et al. Impact of COVID-19 Pandemic on Serum Vitamin D Level among Infants and Toddlers: An Interrupted Time Series Analysis and before-and-after Comparison. Nutrients 2021, 13, 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041270
Wong RS, Tung KTS, So H-K, Wong WHS, Wong SY, Tsang HW, Tung JYL, Chua GT, Ho MHK, Wong ICK, et al. Impact of COVID-19 Pandemic on Serum Vitamin D Level among Infants and Toddlers: An Interrupted Time Series Analysis and before-and-after Comparison. Nutrients. 2021; 13(4):1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041270
Chicago/Turabian StyleWong, Rosa S., Keith T. S. Tung, Hung-Kwan So, Wilfred H. S. Wong, Siew Yan Wong, Hing Wai Tsang, Joanna Y. L. Tung, Gilbert T. Chua, Marco H. K. Ho, Ian C. K. Wong, and et al. 2021. "Impact of COVID-19 Pandemic on Serum Vitamin D Level among Infants and Toddlers: An Interrupted Time Series Analysis and before-and-after Comparison" Nutrients 13, no. 4: 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041270