
Persistent Moderate-to-Weak Mediterranean Diet Adherence and Low Scoring for Plant-Based Foods across Several Southern European Countries: Are We Overlooking the Mediterranean Diet Recommendations?

 ,
,  ,
,  ,
,  , , , , ,
, , , , , 
 , , , , and
, , , , and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Ethics and Recruitment
2.2. MeDiWeB Questionnaire
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
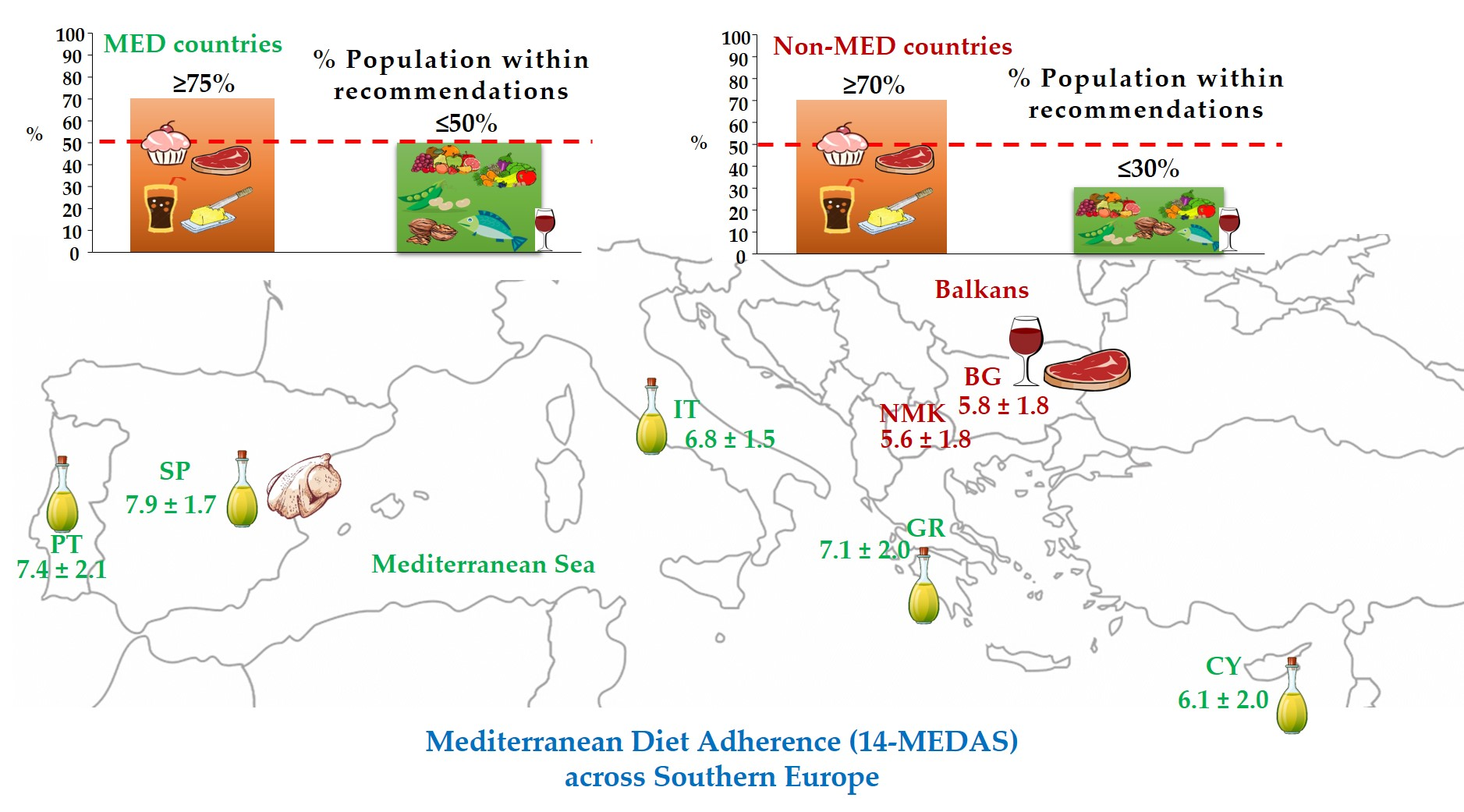
3.2. Analysis of the 14-MEDAS Score across Countries
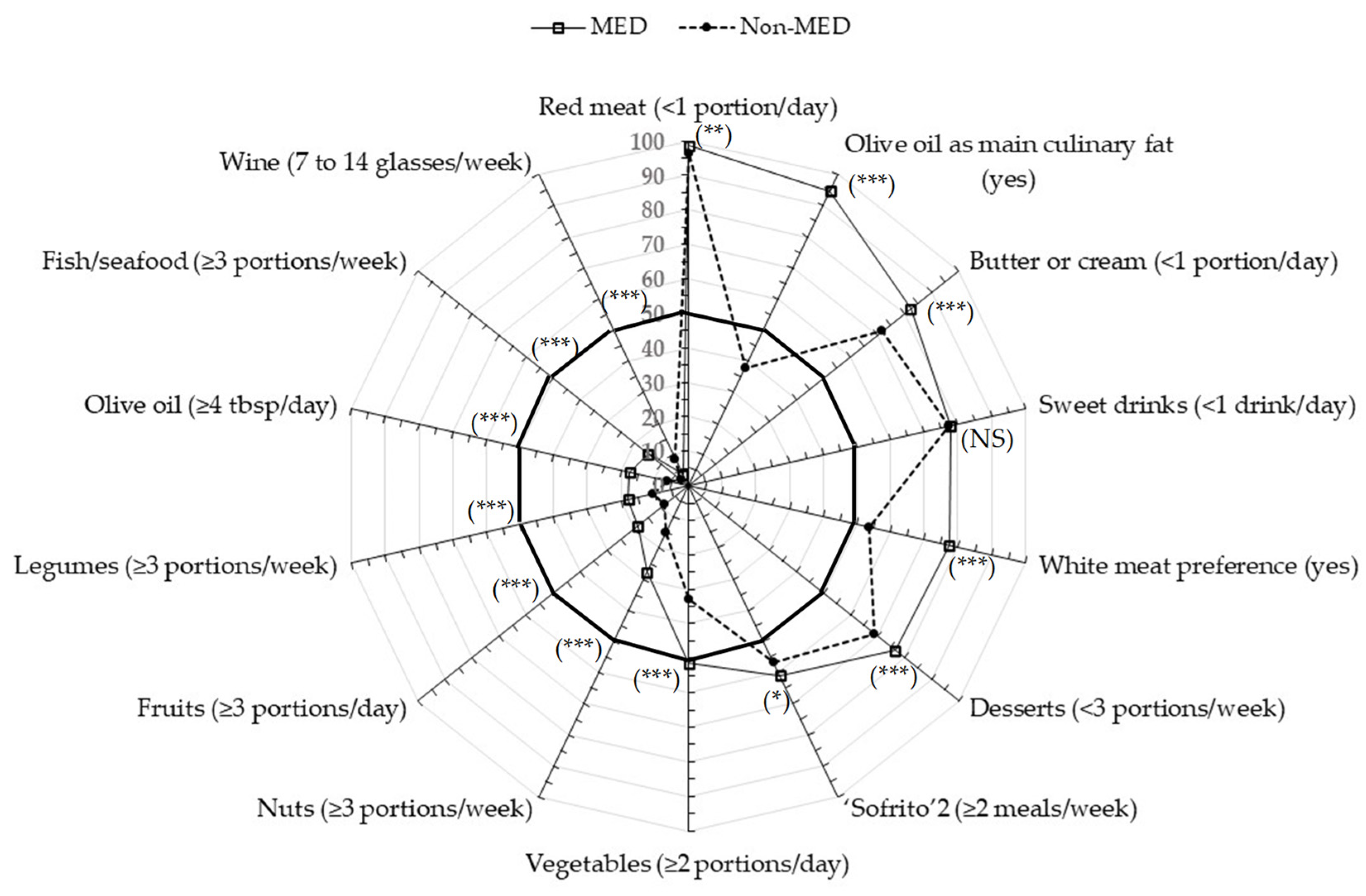
3.3. Comparison across Countries of the 14-Food Items Included in the 14-MEDAS Score
3.4. Additional Food-Related Questions Included in the MeDiWeB Questionnaire
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lăcătusu, C.M.; Grigorescu, E.D.; Floria, M.; Onofriescu, A.; Mihai, B.M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public Health 2019, 16, 942. [Google Scholar] [CrossRef] [Green Version]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [Green Version]
- AAVV. Sustainable Diet and Biodiversity; Food and Agriculture Organization of the United Nations (FAO): Roma, Italy, 2012; p. 309. [Google Scholar]
- Blas, A.; Garrido, A.; Unver, O.; Willaarts, B. A comparison of the Mediterranean diet and current food consumption patterns in Spain from a nutritional and water perspective. Sci. Total Environ. 2019, 664, 1020–1029. [Google Scholar] [CrossRef]
- Vanham, D.; Del Pozo, S.; Pekcan, A.G.; Keinan-Boker, L.; Trichopoulou, A.; Gawlik, B.M. Water consumption related to different diets in Mediterranean cities. Sci. Total Environ. 2016, 573, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Pairotti, M.B.; Cerutti, A.K.; Martini, F.; Vesce, E.; Padovan, D.; Beltramo, R. Energy consumption and GHG emission of the Mediterranean diet: A systemic assessment using a hybrid LCA-IO method. J. Clean. Prod. 2015, 103, 507–516. [Google Scholar] [CrossRef]
- Dernini, S.; Berry, E.M. Mediterranean Diet: From a Healthy Diet to a Sustainable Dietary Pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition-barriers to and opportunities for healthier eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.L.; Siani, A.; Fogliano, V.; Geleijnse, J.M.; Giacco, R.; Giampaoli, S.; Iacoviello, L.; Kromhout, D.; Lionetti, L.; Naska, A.; et al. The Mediterranean diet from past to future: Key concepts from the second “Ancel Keys” International Seminar. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 717–732. [Google Scholar] [CrossRef]
- Dubois, L.; Girard, M.; Bergeron, N. The choice of a diet quality indicator to evaluate the nutritional health of populations. Public Health Nutr. 2000, 3, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Conesa, M.T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef] [PubMed]
- León-Muñoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to the Mediterranean diet pattern has declined in Spanish adults. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef] [Green Version]
- Posta, A. Exploring adherence and attitude towards the Mediterranean diet in a Spanish population. DHS 2019, 2, 59–64. [Google Scholar] [CrossRef]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Andò, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: A cross-sectional web-based epidemiological study in Southern Italy. Int. J. Food Sci. Nutr. 2020, 71, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Dragà, D.; Misotti, A.M.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef]
- Bamia, C.; Martimianaki, G.; Kritikou, M.; Trichopoulou, A. Indexes for Assessing Adherence to a Mediterranean Diet from Data Measured through Brief Questionnaires: Issues Raised from the Analysis of a Greek Population Study. Curr. Dev. Nutr. 2017, 1, e000075. [Google Scholar] [CrossRef] [Green Version]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef]
- Kazaz, İ.; Angin, E.; Kabaran, S.; İyigün, G.; Kirmizigil, B.; Malkoç, M. Evaluation of the physical activity level, nutrition quality, and depression in patients with metabolic syndrome: Comparative study. Medicine 2018, 97, e0485. [Google Scholar] [CrossRef] [PubMed]
- Andrade, V.; Jorge, R.; Garcia-Conesa, M.T.; Philippou, E.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Maksimova, V.; Smilkov, K.; Ackova, D.G.; et al. Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients 2020, 12, 3837. [Google Scholar] [CrossRef]
- Cuschieri, S.; Libra, M. Adherence to the Mediterranean Diet in Maltese Adults. Int. J. Environ. Res. Public Health 2020, 18, 10. [Google Scholar] [CrossRef]
- El Rhazi, K.; Nejjari, C.; Romaguera, D.; Feart, C.; Obtel, M.; Zidouh, A.; Bekkali, R.; Gateau, P.B. Adherence to a Mediterranean diet in Morocco and its correlates: Cross-sectional analysis of a sample of the adult Moroccan population. BMC Public Health 2012, 12, 345. [Google Scholar] [CrossRef] [Green Version]
- Mohtadi, K.; Msaad, R.; Benalioua, N.; Jafri, A.; Meftah, H.; Elkardi, Y.; Lebrazi, H.; Kettani, A.; Derouiche, A.; Taki, H.; et al. Sociodemographic and Lifestyle Factors Associated with Adherence to Mediterranean Diet in Representative Adult Population in Casablanca City, Morocco: A Cross-Sectional Study. J. Nutr. Metab. 2020, 2020, 3105271. [Google Scholar] [CrossRef]
- Abu-Saad, K.; Endevelt, R.; Goldsmith, R.; Shimony, T.; Nitsan, L.; Shahar, D.R.; Keinan-Boker, L.; Ziv, A.; Kalter-Leibovici, O. Adaptation and predictive utility of a Mediterranean diet screener score. Clin. Nutr. 2019, 38, 2928–2935. [Google Scholar] [CrossRef]
- Baydemir, C.; Ozgur, E.G.; Balci, S. Evaluation of adherence to Mediterranean diet in medical students at Kocaeli University, Turkey. J. Int. Med. Res. 2018, 46, 1585–1594. [Google Scholar] [CrossRef]
- Gómez Sánchez, M.; Gómez Sánchez, L.; Patino-Alonso, M.C.; Alonso-Domínguez, R.; Sánchez-Aguadero, N.; Lugones-Sánchez, C.; Rodríguez Sánchez, E.; García Ortiz, L.; Gómez-Marcos, M.A. Adherence to the Mediterranean Diet in Spanish Population and Its Relationship with Early Vascular Aging according to Sex and Age: EVA Study. Nutrients 2020, 12, 1025. [Google Scholar] [CrossRef] [Green Version]
- Inan-Eroglu, E.; Çetin, C.; Akyol Mutlu, A.; Ayaz, A.; Samur, G. Does adherence to mediterranean diet affect body mass index and dietary macronutrient intakes in adults? Clin. Nutr. ESPEN 2018, 37, S112. [Google Scholar] [CrossRef]
- Patino-Alonso, M.C.; Recio-Rodríguez, J.I.; Belio, J.F.M.; Colominas-Garrido, R.; Lema-Bartolomé, J.; Arranz, A.G.; Agudo-Conde, C.; Gomez-Marcos, M.A.; García-Ortiz, L. Factors Associated with Adherence to the Mediterranean Diet in the Adult Population. J. Acad. Nutr. Diet. 2014, 114, 583–589. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Martínez, J.A.; De Irala, J.; Martínez-González, M.A. Determinants of the adherence to an “a priori” defined Mediterranean dietary pattern. Eur. J. Nutr. 2002, 41, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprara, G. Mediterranean-Type Dietary Pattern and Physical Activity: The Winning Combination to Counteract the Rising Burden of Non-Communicable Diseases (NCDs). Nutrients 2021, 13, 429. [Google Scholar] [CrossRef] [PubMed]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Off. J. Eur. Union 2016. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 31 January 2019).
- Organization for Economic Co-operation and Development (OECD). In Guidelines on Measuring Subjective Well-Being; OECD Publishing: Paris, France, 2013. [CrossRef]
- World Health Organization (WHO). Obesity and Overweight. Available online: https://www.who.int/westernpacific/health-topics/obesity (accessed on 15 October 2020).
- World Health Organization (WHO). ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; (v. 3); WHO: Geneva, Switzerland, 2004; ISBN 92 4154654 9. Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 31 January 2019).
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [Green Version]
- Grissom, R.J.; Kim, J.J. Effect Sizes for Research: Univariate and Multivariate Applications; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Cena, H.; Calder, P. Defining a healthy diet: Evidence for a role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maderuelo-Fernandez, J.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Pérez-Arechaederra, D.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; García-Ortiz, L. Effectiveness of interventions applicable to primary health care settings to promote Mediterranean diet or healthy eating adherence in adults: A systematic review. Prev. Med. 2015, 76, S39–S55. [Google Scholar] [CrossRef]
- Moreno-Agostino, D.; Caballero, F.F.; Martin-Maria, N.; Tyrovolas, S.; Lopez-Garcia, P.; Rodriguez-Artalejo, F.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Mediterranean diet and wellbeing: Evidence from a nationwide survey. Psychol. Health 2019, 34, 321–335. [Google Scholar] [CrossRef]
- Pano, O.; Sayon-Orea, C.; Gea, A.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.A.; Martinez, J.A. Nutritional Determinants of Quality of Life in a Mediterranean Cohort: The SUN Study. Int. J. Environ. Res. Public Health 2020, 17, 3897. [Google Scholar] [CrossRef]
- Gregorio, M.J.; Rodrigues, A.M.; Salvador, C.; Dias, S.S.; de Sousa, R.D.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Lopes, C.; Martinez-Gonzalez, M.A.; et al. Validation of the Telephone-Administered Version of the Mediterranean Diet Adherence Screener (MEDAS) Questionnaire. Nutrients 2020, 12, 1511. [Google Scholar] [CrossRef]
- Ferreira-Pêgo, C.; Rodrigues, J.; Costa, A.; Sousa, B. Adherence to the mediterranean diet in portuguese university students. Biomed. Biopharm. Res. 2019, 16, 41–49. [Google Scholar] [CrossRef]
- Amato, M.; Bonomi, A.; Laguzzi, F.; Veglia, F.; Tremoli, E.; Werba, J.P.; Giroli, M.G. Overall dietary variety and adherence to the Mediterranean diet show additive protective effects against coronary heart disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1315–1321. [Google Scholar] [CrossRef]
- Cavaliere, A.; De Marchi, E.; Banterle, A. Exploring the Adherence to the Mediterranean Diet and Its Relationship with Individual Lifestyle: The Role of Healthy Behaviors, Pro-Environmental Behaviors, Income, and Education. Nutrients 2018, 10, 141. [Google Scholar] [CrossRef] [Green Version]
- Mattioli, A.V.; Pennella, S.; Pedrazzi, P.; Rosi, C.; Farinetti, A. Gender differences in adherence to Mediterranean diet and risk of atrial fibrillation. JHC 2015, 1, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Pelucchi, C.; Galeone, C.; Negri, E.; La Vecchia, C. Trends in adherence to the Mediterranean diet in an Italian population between 1991 and 2006. Eur. J. Clin. Nutr. 2010, 64, 1052–1056. [Google Scholar] [CrossRef] [Green Version]
- Dalamaga, M.; Muscogiuri, G.; Paganitsa, G.; Parvouleskou, G.; Syriou, V.; Karagkoynis, P.; Stratigou, T.; Vallianou, N.; Christodoulatos, G.S.; Karampela, I.; et al. Adherence to the Mediterranean diet is an independent predictor of circulating vitamin D levels in normal weight and non-smoker adults: An observational cross-sectional study. Int. J. Food Sci. Nutr. 2021, 1–13. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Skoumas, I.; Stefanadis, C.; Study, A. Five-year incidence of cardiovascular disease and its predictors in Greece: The ATTICA study. Vasc. Med. 2008, 13, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Kolokotroni, O.; Mosquera, M.; Quattrocchi, A.; Heraclides, A.; Demetriou, C.; Elena, P. Lifestyle Habits of Adults During The COVID-19 Pandemic Lockdown in Cyprus: Evidence From a Cross-Sectional Study. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Benhammou, S.; Heras-González, L.; Ibáñez-Peinado, D.; Barceló, C.; Hamdan, M.; Rivas, A.; Mariscal-Arcas, M.; Olea-Serrano, F.; Monteagudo, C. Comparison of Mediterranean diet compliance between European and non-European populations in the Mediterranean basin. Appetite 2016, 107, 521–526. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- Kolcic, I.; Relja, A.; Gelemanovic, A.; Miljkovic, A.; Boban, K.; Hayward, C.; Rudan, I.; Polasek, O. Mediterranean diet in the southern Croatia—Does it still exist? Croat. Med. J. 2016, 57, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Kristela, J.; Brunilda, S.; Inva, Z.; Jerina, J.; Fatjona, K. Eating Patterns and Adherence to the Mediterranean Diet: A Cross-Sectional Study in Albania. ESJ 2020, 16, 11. [Google Scholar] [CrossRef]
- Food and Agriculture Organization (FAO). New Food Balances. In FAOSTAT; 2018; Available online: http://www.fao.org/faostat/en/#data/FBS (accessed on 22 February 2021).
- Kostova, S.; Atanasov, B.; Marinova, D. Consumption of animal products in Bulgaria: The case for change. In Handbook of Research on Social Marketing and Its Influence on Animal Origin Food Product Consumption; IGI Global: Hershey, PA, USA, 2018; pp. 283–297. [Google Scholar]
- El Ansari, W.; Stock, C.; Mikolajczyk, R.T. Relationships between food consumption and living arrangements among university students in four European countries—A cross-sectional study. Nutr. J. 2012, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Karamanos, B.; Thanopoulou, A.; Angelico, F.; Assaad-Khalil, S.; Barbato, A.; Del Ben, M.; Dimitrijevic-Sreckovic, V.; Djordjevic, P.; Gallotti, C.; Katsilambros, N.; et al. Nutritional habits in the Mediterranean Basin. The macronutrient composition of diet and its relation with the traditional Mediterranean diet. Multi-centre study of the Mediterranean Group for the Study of Diabetes (MGSD). Eur. J. Clin. Nutr. 2002, 56, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Spiroski, I.; Nikolic, M.; Kochubovski, M.; Gurinovic, M.; Ristovska, G.; Kadvan, A. Energy, macronutrients and dietary fibre intake among adults in North Macedonia. Cent. Eur. J. Public Health 2020, 28, 24–32. [Google Scholar] [CrossRef]
- Ivanova, L.; Dimitrov, P.; Ovcharova, D.; Dellava, J.; Hoffman, D.J. Economic transition and household food consumption: A study of Bulgaria from 1985 to 2002. Econ. Hum. Biol. 2006, 4, 383–397. [Google Scholar] [CrossRef]
- Pocol, C.B.; Marinescu, V.; Amuza, A.; Cadar, R.-L.; Rodideal, A.A. Sustainable vs. Unsustainable Food Consumption Behaviour: A Study among Students from Romania, Bulgaria and Moldova. Sustainability 2020, 12, 4699. [Google Scholar] [CrossRef]
- Darfour-Oduro, S.A.; Buchner, D.M.; Andrade, J.E.; Grigsby-Toussaint, D.S. A comparative study of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci. Rep. 2018, 8, 1623. [Google Scholar] [CrossRef] [Green Version]
- European Market Observatory for Fisheries and Aquaculture Products (EUMOFA). Retail Consumption; European Commission Publishing: Brussels, Belgium, 2018; Available online: https://www.eumofa.eu/data (accessed on 22 February 2021).
- Nikolai, V. Wine as a signifier of kinship in Bulgarian folklore epics. Acta Ethnogr. Hung. 2013, 58, 389–396. [Google Scholar] [CrossRef]
- Angelova, M.; Pastarmadzhieva, D.; Dimitrova, D.; Georgiev, P. Innovative Practices in Wine Industry: Opportunities for Competitiveness Enhancement in Bulgaria. In Proceedings of the 2019 International Conference on Creative Business for Smart and Sustainable Growth (CREBUS), Sandanski, Bulgaria, 18–21 March 2019; pp. 1–6. [Google Scholar]
- Hernández-Galiot, A.; Goñi, I. Adherence to the Mediterranean diet pattern, cognitive status and depressive symptoms in an elderly non-institutionalized population. Nutr. Hosp. 2017, 34, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Stefanadis, C. Association between the prevalence of obesity and adherence to the Mediterranean diet: The ATTICA study. Nutrition 2006, 22, 449–456. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Fiore, V.; Rosta, G.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Agodi, A. Determinants of Adherence to the Mediterranean Diet: Findings from a Cross-Sectional Study in Women from Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 2963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrigley, C.W. Wheat: An Overview of the Grain That Provides ‘Our Daily Bread’. In Encyclopedia of Food Grains, 2nd ed.; Wrigley, C., Corke, H., Seetharaman, K., Faubion, J., Eds.; Academic Press: Oxford, UK, 2016; pp. 105–116. [Google Scholar]
- Kelly, S.A.; Summerbell, C.D.; Brynes, A.; Whittaker, V.; Frost, G. Wholegrain cereals for coronary heart disease. Cochrane Database Syst. Rev. 2007, 2, Cd005051. [Google Scholar] [CrossRef]
- Kelly, S.A.; Hartley, L.; Loveman, E.; Colquitt, J.L.; Jones, H.M.; Al-Khudairy, L.; Clar, C.; Germanò, R.; Lunn, H.R.; Frost, G.; et al. Whole grain cereals for the primary or secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 8, Cd005051. [Google Scholar] [CrossRef] [Green Version]
- Foscolou, A.; D’Cunha, N.M.; Naumovski, N.; Tyrovolas, S.; Chrysohoou, C.; Rallidis, L.; Matalas, A.L.; Sidossis, L.S.; Panagiotakos, D. The Association between Whole Grain Products Consumption and Successful Aging: A Combined Analysis of MEDIS and ATTICA Epidemiological Studies. Nutrients 2019, 11, 1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Hu, E.A.; Rebholz, C.M. Ultra-processed food intake and mortality in the USA: Results from the Third National Health and Nutrition Examination Survey (NHANES III, 1988–1994). Public Health Nutr. 2019, 22, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Elwood, P.C.; Pickering, J.E.; Fehily, A.M. Milk and dairy consumption, diabetes and the metabolic syndrome: The Caerphilly prospective study. J. Epidemiol. Community Health 2007, 61, 695–698. [Google Scholar] [CrossRef]
- Fumeron, F.; Lamri, A.; Abi Khalil, C.; Jaziri, R.; Porchay-Balderelli, I.; Lantieri, O.; Vol, S.; Balkau, B.; Marre, M.; Data from the Epidemiological Study on the Insulin Resistance Syndrome (DESIR) Study Group. Dairy consumption and the incidence of hyperglycemia and the metabolic syndrome: Results from a french prospective study, Data from the Epidemiological Study on the Insulin Resistance Syndrome (DESIR). Diabetes Care 2011, 34, 813–817. [Google Scholar] [CrossRef] [Green Version]
- Louie, J.C.; Flood, V.M.; Rangan, A.M.; Burlutsky, G.; Gill, T.P.; Gopinath, B.; Mitchell, P. Higher regular fat dairy consumption is associated with lower incidence of metabolic syndrome but not type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 816–821. [Google Scholar] [CrossRef] [Green Version]
- Babio, N.; Becerra-Tomás, N.; Martínez-González, M.; Corella, D.; Estruch, R.; Ros, E.; Sayón-Orea, C.; Fitó, M.; Serra-Majem, L.; Arós, F.; et al. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [CrossRef] [Green Version]
- Petrova, P.; Ivanov, I.; Tsigoriyna, L.; Valcheva, N.; Vasileva, E.; Parvanova-Mancheva, T.; Arsov, A.; Petrov, K. Traditional Bulgarian Dairy Products: Ethnic Foods with Health Benefits. Microorganisms 2021, 9, 480. [Google Scholar] [CrossRef]
- Chan, J.; Knutsen, S.F.; Blix, G.G.; Lee, J.W.; Fraser, G.E. Water, other fluids, and fatal coronary heart disease: The Adventist Health Study. Am. J. Epidemiol. 2002, 155, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Jan, K.M.; Chien, S.; Bigger, J.T., Jr. Observations on blood viscosity changes after acute myocardial infarction. Circulation 1975, 51, 1079–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, R.; Fezeu, L.; Bouby, N.; Balkau, B.; Lantieri, O.; Alhenc-Gelas, F.; Marre, M.; Bankir, L.; Group, D.E.S.I.R.S. Low water intake and risk for new-onset hyperglycemia. Diabetes Care 2011, 34, 2551–2554. [Google Scholar] [CrossRef] [Green Version]
- Vij, V.A.; Joshi, A.S. Effect of ‘water induced thermogenesis’ on body weight, body mass index and body composition of overweight subjects. J. Clin. Diagn. Res. 2013, 7, 1894–1896. [Google Scholar] [CrossRef]
- Paz-Graniel, I.; Babio, N.; Serra-Majem, L.; Vioque, J.; Zomeno, M.D.; Corella, D.; Diaz-Lopez, A.; Pinto, X.; Bueno-Cavanillas, A.; Tur, J.A.; et al. Fluid and total water intake in a senior mediterranean population at high cardiovascular risk: Demographic and lifestyle determinants in the PREDIMED-Plus study. Eur. J. Nutr. 2020, 59, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for water. EFSA J. 2010, 8, 1459. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; Ngo de la Cruz, J.; Bach-Faig, A.; Donini, L.M.; Medina, F.X.; Belahsen, R.; et al. Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on environmental concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef]
- Edelstein, S.L.; Barrett-Connor, E.L.; Wingard, D.L.; Cohn, B.A. Increased meal frequency associated with decreased cholesterol concentrations; Rancho Bernardo, CA, 1984–1987. Am. J. Clin. Nutr. 1992, 55, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Poscia, A.; Teleman, A.A.; Azzolini, E.; de Waure, C.; Maged, D.; Virdis, A.; Ricciardi, W.; Di Pietro, M.L. Eating episode frequency and fruit and vegetable consumption among Italian university students. Ann. Ist. Super. Sanita 2017, 53, 199–204. [Google Scholar] [CrossRef]
- Food and Agriculture Organization (FAO). Food-Based Dietary Guidelines; FAO Publishing: Rome, Italy, 2021; Available online: http://www.fao.org/nutrition/education/fooddietary-guidelines/home/en/ (accessed on 22 February 2021).
- Fernández-Lázaro, C.I.; Ruiz-Canela, M.; Martínez-González, M. Deep dive to the secrets of the PREDIMED trial. Curr. Opin. Lipidol. 2021, 32, 62–69. [Google Scholar] [CrossRef]
- Berry, E.M. Sustainable Food Systems and the Mediterranean Diet. Nutrients 2019, 11, 2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trajkovska Petkoska, A.; Trajkovska-Broach, A. Mediterranean diet: A nutrient-packed diet and a healthy lifestyle for a sustainable world. J. Sci. Food Agric. 2020. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| SP | IT | PT 1 | GR | CY | MED | BG | NMK | Non-MED | |
|---|---|---|---|---|---|---|---|---|---|
| Total N (%) | 486 (21.9) | 505 (22.8) | 488 (22.0) | 296 (13.4) | 442 (20.0) | 2217 | 492 (53.0) | 436 (47.0) | 928 |
| Sex | |||||||||
| Women; N (%) | 276 (56.8) | 315 (62.4) | 349 (72.0) | 230 (77.7) | 317 (72.0) | 1487 (67.2) | 340 (69.1) | 323 (74.1) | 663 (71.4) |
| Men; N (%) | 210 (43.2) | 190 (37.6) | 136 (28.0) | 66 (22.3) | 123 (28.0) | 725 (32.8) | 152 (30.9) | 113 (25.9) | 265 (28.6) |
| Age (years) | |||||||||
| Median (IQR) | 49.0 (18.0) | 36.0 (25) | 34.0 (23.8) | 33.0 (12.0) | 37 (16) | 38.0 (23.0) | 42.0 (17.0) | 24.0 (14.0) | 35.0 (22.0) |
| Mean ± SD | 45.7 ± 12.8 | 38.1 ± 14.2 | 36.5 ± 13.6 | 34.8 ± 8.9 | 38.1 ± 12.1 | 39.0 ± 13.3 | 43.0 ± 12.8 | 29.2 ± 10.5 | 36.7 ± 13.6 |
| (N) | (485) | (505) | (488) | (293) | (442) | (2213) | (492) | (434) | (926) |
| Range (years) | 18–74 | 18–80 | 18–75 | 18–66 | 19–75 | 18–80 | 18–90 | 18–74 | 18–90 |
| 18–24 (years) N (%) | 46 (9.5) | 118 (23.4) | 124 (25.4) | 26 (8.9) | 64 (14.5) | 378 (17.1) | 30 (6.1) | 221 (50.9) | 251 (27.1) |
| 25–44 (years) N (%) | 143 (29.5) | 215 (42.6) | 215 (44.1) | 228 (77.8) | 262 (59.3) | 1063 (48.0) | 250 (50.8) | 157 (36.2) | 407 (44.0) |
| 45–64 (years) N (%) | 281 (57.9) | 150 (29.7) | 141 (28.9) | 38 (13.0) | 104 (23.5) | 714 (32.3) | 186 (37.8) | 53 (12.2) | 239 (25.8) |
| ≥65 (years) N (%) | 15 (3.1) | 22 (4.4) | 8 (1.6) | 1 (0.3) | 12 (2.7) | 58 (2.6) | 26 (5.3) | 3 (0.7) | 29 (3.1) |
| BMI (kg/m2) | |||||||||
| Median (IQR) | 24.2 (4.4) | 23.5 (4.9) | 23.4 (5.2) | 24.6 (6.6) | 23.8 (6.2) | 23.8 (5.3) | 24.2 (6.6) | 23.3 (5.3) | 23.7 (6.2) |
| Mean ± SD | 24.7 ± 3.9 | 21.1 ± 4.1 | 24.2 ± 4.6 | 25.6 ± 5.5 | 24.6 ± 4.7 | 24.6 ± 4.5 | 25.2 ± 5.7 | 23.8 ± 4.1 | 24.6 ± 5.1 |
| (N) | (481) | (501) | (474) | (293) | (440) | (2189) | (491) | (422) | (913) |
| 2 Underweight (<18.5 kg/m2) N (%) | 9 (1.9) | 22 (4.4) | 17 (3.6) | 9 (3.1) | 21 (4.8) | 78 (3.6) | 24 (4.9) | 21 (5.0) | 45 (4.9) |
| Normal weight (18.5–24.9 kg/m2) N (%) | 276 (57.4) | 307 (61.3) | 296 (62.4) | 145 (49.5) | 254 (57.7) | 1278 (58.4) | 256 (52.2) | 262 (62.1) | 518 (56.7) |
| Overweight (25.0–29.9 kg/m2) N (%) | 150 (31.2) | 134 (26.7) | 109 (23.0) | 85 (29.0) | 100 (22.7) | 578 (26.4) | 126 (25.6) | 111 (26.3) | 237 (26.0) |
| Obesity (≥30 kg/m2) N (%) | 46 (9.6) | 38 (7.6) | 52 (11.0) | 54 (18.4) | 65 (14.8) | 255 (11.6) | 85 (17.3) | 28 (6.6) | 113 (12.3) |
| (Overweight + obesity) N (%) | 196 (40.8) | 172 (34.3) | 161 (34.0) | 139 (47.4) | 165 (37.5) | 833 (38.0) | 211 (42.9) | 139 (32.9) | 350 (38.3) |
| Disease status | |||||||||
| Non declared pathology N (%) | 317 (66.6) | 423 (83.8) | 342 (74.7) | 220 (74.6) | 336 (76.0) | 1638 (75.3) | 401 (83.9) | 364 (86.1) | 765 (84.9) |
| Declared one pathology N (%) | 123 (25.8) | 71 (14.1) | 106 (23.1) | 66 (22.4) | 73 (16.5) | 438 (20.1) | 65 (13.6) | 53 (12.5) | 118 (13.1) |
| Declared multi-pathology N (%) | 36 (7.6) | 11 (2.2) | 10 (2.2) | 9 (3.1) | 33 (7.5) | 100 (4.6) | 12 (2.5) | 6 (1.4) | 18 (2.0) |
| 14-MEDAS Question (Score 1) | SP | IT | PT | GR | CY | BG | NMK | MED | Non-MED | p-Value (Chi-S) 1 | p-Value (Fisher) 2 | Effect Size 3 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Olive oil as main culinary fat (yes) | 98.3 | 97.0 | 96.5 | 96.6 | 84.6 | 43.7 | 31.8 | 94.7 | 38.0 | <0.001 | <0.001 | 0.62 (large) |
| 2. Olive oil (≥4 tbsp 4/day) | 16.5 | 21.4 | 9.4 | 28.3 | 15.2 | 9.2 | 3.1 | 17.4 | 6.4 | <0.001 | <0.001 | 0.14 (small) |
| 3. Vegetables (≥2 portions/day) | 54.3 | 41.0 | 53.1 | 56.8 | 54.9 | 43.9 | 21.3 | 51.5 | 33.1 | <0.001 | <0.001 | 0.17 (small) |
| 4. Fruits (≥3 portions/day) | 25.0 | 8.7 | 23.8 | 16.8 | 18.9 | 9.1 | 8.1 | 18.8 | 8.6 | <0.001 | <0.001 | 0.13 (small) |
| 5. Red meat (<1 portion/day) | 99.2 | 98.6 | 95.5 | 100.0 | 99.5 | 95.3 | 97.7 | 98.4 | 96.4 | <0.001 | 0.001 | 0.06 (small) |
| 6. Butter or cream (<1 portion/day) | 91.9 | 95.0 | 67.8 | 77.1 | 76.8 | 68.9 | 75.0 | 82.3 | 71.8 | <0.001 | <0.001 | 0.12 (small) |
| 7. Sweet drinks (<1 drink/day) | 88.2 | 77.2 | 82.6 | 67.8 | 68.3 | 84.5 | 69.9 | 77.8 | 77.5 | <0.001 | NS | 0.003 (NS) |
| 8. Wine (7 to 14 glasses/week) | 2.5 | 5.8 | 4.3 | 2.1 | 2.7 | 15.0 | 1.4 | 3.6 | 8.6 | <0.001 | <0.001 | 0.10 (small) |
| 9. Legumes (≥3 portions/week) | 20.2 | 14.3 | 23.0 | 6.9 | 20.4 | 7.0 | 14.5 | 17.8 | 10.6 | <0.001 | <0.001 | 0.09 (small) |
| 10. Fish/seafood (≥3 portions/week) | 19.4 | 6.5 | 35.0 | 2.1 | 5.2 | 3.0 | 1.9 | 14.8 | 2.5 | <0.001 | <0.001 | 0.18 (small) |
| 11. Desserts (<3 portions/week) | 81.6 | 71.7 | 72.5 | 73.5 | 82.9 | 78.5 | 58.0 | 76.5 | 68.8 | <0.001 | <0.001 | 0.08 (small) |
| 12. Nuts (≥3 portions/week) | 36.6 | 10.3 | 29.7 | 42.3 | 26.1 | 12.3 | 18.4 | 27.8 | 15.2 | <0.001 | <0.001 | 0.13 (small) |
| 13. White meat preference (yes) | 84.6 | 68.8 | 76.8 | 73.7 | 82.4 | 49.7 | 58.0 | 77.4 | 53.7 | <0.001 | <0.001 | 0.24 (small) |
| 14. “Sofrito” 5 (≥2 meals/week) | 75.5 | 63.4 | 68.0 | 67.7 | 30.3 | 55.4 | 58.1 | 61.1 | 56.7 | <0.001 | <0.05 | 0.04 (small) |
| Question (Within MD Recommendations) | SP | IT | PT | GR | CY | BG | NMK | MED | Non-MED | p-Value (Chi-S) 2 | p-Value (Fisher) 3 | Effect Size 4 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Milk and derived products (one or two/day) 1 | 85.2 | 73.5 | 60.8 | 70.2 | 61.3 | 59.1 | 62.4 | 70.4 | 60.7 | <0.001 | <0.001 | 0.18 (small) |
| Preference for low fat milk, yogurt, or cheese (yes) 1 | 68.0 | 66.6 | 46.8 | 62.4 | 77.1 | 31.3 | 39.9 | 64.2 | 35.4 | <0.001 | <0.001 | 0.26 (median) |
| Preference for whole grain (yes)1 | 55.3 | 65.2 | 68.7 | 66.5 | 79.2 | 49.5 | 73.2 | 67.3 | 59.6 | <0.001 | <0.001 | 0.07 (small) |
| Water (one to two liters/day) 1 | 59.1 | 47.9 | 59.1 | 49.0 | 61.3 | 53.3 | 67.3 | 57.7 | 56.3 | <0.001 | NS | 0.03 (small) |
| Caffeinated drinks (one to three/day) | 64.8 | 68.6 | 58.2 | 60.4 | 58.1 | 62.6 | 56.3 | 60.1 | 63.8 | <0.001 | NS | 0.04 (small) |
| Herbal teas (one to three/day) | 35.2 | 23.9 | 28.0 | 18.5 | 34.1 | 45.3 | 22.8 | 26.0 | 40.0 | <0.001 | <0.001 | 0.18 (small) |
| Number of meals (per day) | 3.9 ± 0.9 5 4.0 (2.0) 6 | 3.7 ± 1.0 4.0 (1.0) | 4.2 ± 1.0 4.0 (1.0) | 4.1 ± 1.0 4.0 (2.0) | 4.0 ± 1.2 4.0 (2.0) | 3.2 ± 1.0 3.0 (1.0) | 2.9 ± 0.9 3.0 (1.0) | 4.0 ± 1.0 4.0 (2.0) | 3.1 ± 0.9 3.0 (2.0) | <0.001 7 | <0.001 8 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quarta, S.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; Jorge, R.; Andrade, V.; Philippou, E.; Zisimou, C.; Maksimova, V.; et al. Persistent Moderate-to-Weak Mediterranean Diet Adherence and Low Scoring for Plant-Based Foods across Several Southern European Countries: Are We Overlooking the Mediterranean Diet Recommendations? Nutrients 2021, 13, 1432. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051432
Quarta S, Massaro M, Chervenkov M, Ivanova T, Dimitrova D, Jorge R, Andrade V, Philippou E, Zisimou C, Maksimova V, et al. Persistent Moderate-to-Weak Mediterranean Diet Adherence and Low Scoring for Plant-Based Foods across Several Southern European Countries: Are We Overlooking the Mediterranean Diet Recommendations? Nutrients. 2021; 13(5):1432. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051432
Chicago/Turabian StyleQuarta, Stefano, Marika Massaro, Mihail Chervenkov, Teodora Ivanova, Dessislava Dimitrova, Rui Jorge, Vanda Andrade, Elena Philippou, Constantinos Zisimou, Viktorija Maksimova, and et al. 2021. "Persistent Moderate-to-Weak Mediterranean Diet Adherence and Low Scoring for Plant-Based Foods across Several Southern European Countries: Are We Overlooking the Mediterranean Diet Recommendations?" Nutrients 13, no. 5: 1432. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051432