
Longitudinal Changes in the Concentration of Major Human Milk Proteins in the First Six Months of Lactation and Their Effects on Infant Growth

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Surveys
2.2. Human Milk Collection
2.3. Human Milk Measurements
2.4. Anthropometric Measurements
2.5. Statistics
3. Results
3.1. Subject Characteristics
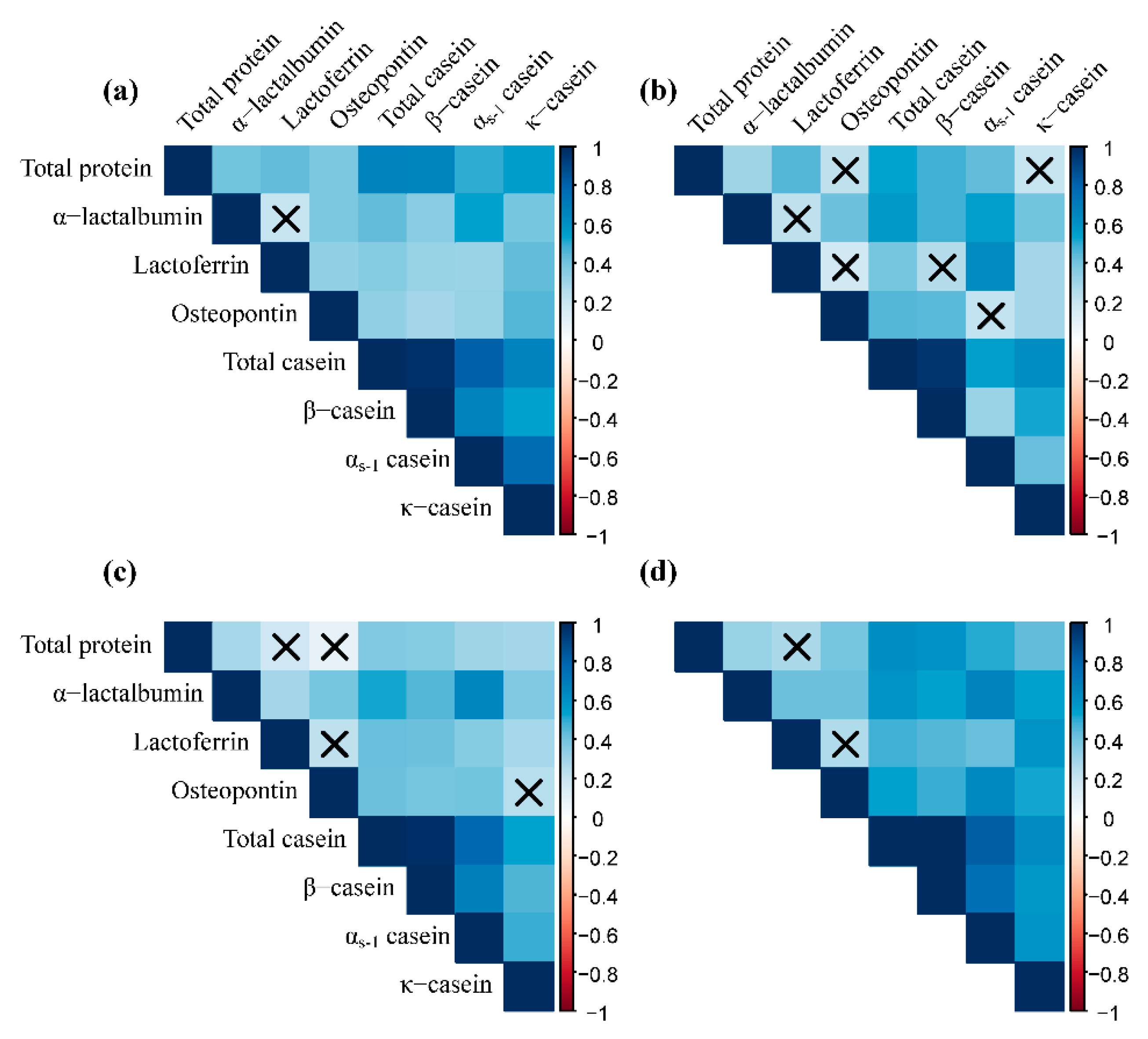
3.2. Contents of Protein Components in Human Milk
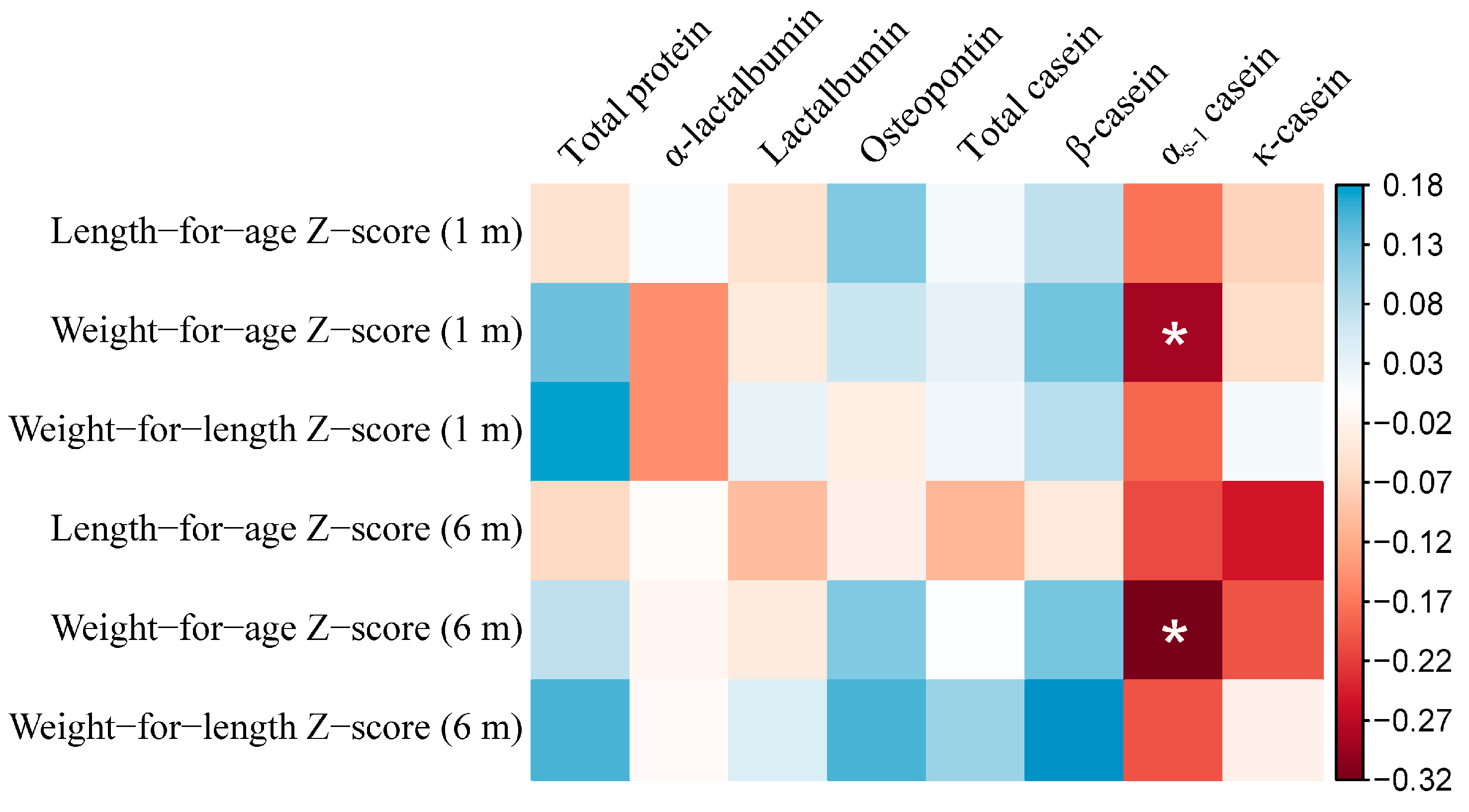
3.3. Concentrations of Human Milk Proteins and Growth of Infants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Strategy for Infant and Young Child Feeding; WHO Publications: Singapore, 2003. [Google Scholar]
- United Nations Children’s Fund. Breastfeeding. Available online: https://www.unicef.org/nutrition/index_24824.html (accessed on 1 January 2021).
- Lönnerdal, B. Bioactive Proteins in Human Milk: Health, Nutrition, and Implications for Infant Formulas. J. Pediatr. 2016, 173, S4–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Short-Term Effects of Breastfeeding: A Systematic Review on the Benefits of Breastfeeding on Diarrhoea and Pneumonia Mortality; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]
- Horta, B.L.; De Mola, C.L.; Victora, C.G. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef]
- Young, B.E. Chapter 2—Breastfeeding and Human Milk: Short and Long-Term Health Benefits to the Recipient Infant. In Early Nutrition and Long-Term Health; Saavedra, J.M., Dattilo, A.M., Eds.; Woodhead Publishing: Amsterdam, The Netherlands, 2017; pp. 25–53. [Google Scholar] [CrossRef]
- Lönnerdal, B. Infant formula and infant nutrition: Bioactive proteins of human milk and implications for composition of infant formulas. Am. J. Clin. Nutr. 2014, 99, 712S–717S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, M.V.; Larnkjær, A.; Mølgaard, C.; Michaelsen, K.F. Breastfeeding, Breast Milk Composition, and Growth Outcomes. Nestle Nutr. Inst. Workshop Ser. 2018, 89, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Rodenas, C.L.; De Castro, C.A.; Jenni, R.; Thakkar, S.K.; Beauport, L.; Tolsa, J.-F.; Fischer-Fumeaux, C.J.; Affolter, M. Temporal changes of major protein concentrations in preterm and term human milk. A prospective cohort study. Clin. Nutr. 2019, 38, 1844–1852. [Google Scholar] [CrossRef]
- Haschke, F.; Haiden, N.; Thakkar, S.K. Nutritive and Bioactive Proteins in Breastmilk. Ann. Nutr. Metab. 2016, 69, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Beck, K.L.; Weber, D.; Phinney, B.S.; Smilowitz, J.T.; Hinde, K.; Lönnerdal, B.; Korf, I.; Lemay, D.G. Comparative Proteomics of Human and Macaque Milk Reveals Species-Specific Nutrition during Postnatal Development. J. Proteome Res. 2015, 14, 2143–2157. [Google Scholar] [CrossRef]
- Prentice, A. Constituents of Human Milk. Food Nutr. Bull. 1996, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Affolter, M.; Garcia-Rodenas, C.L.; Vinyes-Pares, G.; Jenni, R.; Roggero, I.; Avanti-Nigro, O.; De Castro, C.A.; Zhao, A.; Zhang, Y.; Wang, P.; et al. Temporal Changes of Protein Composition in Breast Milk of Chinese Urban Mothers and Impact of Caesarean Section Delivery. Nutrients 2016, 8, 504. [Google Scholar] [CrossRef] [Green Version]
- Sandström, O.; Lönnerdal, B.; Graverholt, G.; Hernell, O. Effects of α-lactalbumin–enriched formula containing different concentrations of glycomacropeptide on infant nutrition. Am. J. Clin. Nutr. 2008, 87, 921–928. [Google Scholar] [CrossRef]
- Fleddermann, M.; Demmelmair, H.; Grote, V.; Nikolic, T.; Trisic, B.; Koletzko, B. Infant formula composition affects energetic efficiency for growth: The BeMIM study, a randomized controlled trial. Clin. Nutr. 2014, 33, 588–595. [Google Scholar] [CrossRef] [Green Version]
- Dupont, C.; Rivero, M.; Grillon, C.; Belaroussi, N.; Kalindjian, A.; Marin, V. α-Lactalbumin-enriched and probiotic-supplemented infant formula in infants with colic: Growth and gastrointestinal tolerance. Eur. J. Clin. Nutr. 2010, 64, 765–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rai, D.; Adelman, A.S.; Zhuang, W.; Rai, G.P.; Boettcher, J.; Lönnerdal, B. Longitudinal Changes in Lactoferrin Concentrations in Human Milk: A Global Systematic Review. Crit. Rev. Food Sci. Nutr. 2014, 54, 1539–1547. [Google Scholar] [CrossRef]
- Lönnerdal, B. Bioactive proteins in breast milk. J. Paediatr. Child Health 2013, 49, 1–7. [Google Scholar] [CrossRef]
- Goonatilleke, E.; Huang, J.; Xu, G.; Wu, L.; Smilowitz, J.T.; German, J.B.; Lebrilla, C.B. Human Milk Proteins and Their Glycosylation Exhibit Quantitative Dynamic Variations during Lactation. J. Nutr. 2019, 149, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Lönnerdal, B.; Kvistgaard, A.S.; Peerson, J.M.; Donovan, S.M.; Peng, Y.-M. Growth, Nutrition, and Cytokine Response of Breast-fed Infants and Infants Fed Formula with Added Bovine Osteopontin. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 650–657. [Google Scholar] [CrossRef]
- Donovan, S.M.; Monaco, M.H.; Drnevich, J.; Kvistgaard, A.S.; Hernell, O.; Lönnerdal, B. Bovine Osteopontin Modifies the Intestinal Transcriptome of Formula-Fed Infant Rhesus Monkeys to Be More Similar to Those That Were Breastfed. J. Nutr. 2014, 144, 1910–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, R.; Prell, C.; Lönnerdal, B. Milk osteopontin may promote brain development via up-regulating osteopontin expression in vivo. FASEB J. 2015, 29, 121–124. [Google Scholar]
- Si, J.; Wang, C.; Zhang, D.; Wang, B.; Hou, W.; Zhou, Y. Osteopontin in Bone Metabolism and Bone Diseases. Med. Sci. Monit. 2020, 26, e919159. [Google Scholar] [CrossRef]
- Bzikowska-Jura, A.; Sobieraj, P.; Szostak-Węgierek, D.; Wesołowska, A. Impact of Infant and Maternal Factors on Energy and Macronutrient Composition of Human Milk. Nutrients 2020, 12, 2591. [Google Scholar] [CrossRef]
- Ren, Q.; Sun, H.; Zhao, M.; Xu, Y.; Xie, Q.; Jiang, S.; Zhao, X.; Zhang, W. Longitudinal Changes in Crude Protein and Amino Acids in Human Milk in Chinese Population: A Systematic Review. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Jiang, R.; Chen, Q.; Wang, J.; Duan, Y.; Pang, X.; Jiang, S.; Bi, Y.; Zhang, H.; Lönnerdal, B.; et al. Concentration of Lactoferrin in Human Milk and Its Variation during Lactation in Different Chinese Populations. Nutrients 2018, 10, 1235. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.; Jin, Q.; Wang, X. Human milk fat substitutes: Past achievements and current trends. Prog. Lipid Res. 2019, 74, 69–86. [Google Scholar] [CrossRef]
- Eriksen, K.G.; Christensen, S.H.; Lind, M.V.; Michaelsen, K.F. Human milk composition and infant growth. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 200–206. [Google Scholar] [CrossRef]
- Hammond, J.B.; Kruger, N.J. The bradford method for protein quantitation. In New Protein Techniques; Humana Press: Clifton, NJ, USA, 1988; pp. 25–32. [Google Scholar]
- Chen, Q.; Zhang, J.; Ke, X.; Lai, S.; Li, D.; Yang, J.; Mo, W.; Ren, Y. Simultaneous quantification of α-lactalbumin and β-casein in human milk using ultra-performance liquid chromatography with tandem mass spectrometry based on their signature peptides and winged isotope internal standards. Biochim. Biophys. Acta. 2016, 1864, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Child Growth Standards. Available online: https://www.who.int/tools/child-growth-standards (accessed on 28 March 2021).
- Wei, T.; Simko, V. R Package “Corrplot”: Visualization of a Correlation Matrix (Version 0.84). 2017. Available online: https://github.com/taiyun/corrplot (accessed on 5 February 2021).
- Schumacher, D.; Borghi, E.; Polonsky, J.; Schumacher, M.D. Package ‘Anthro’. 2020. Available online: https://CRAN.R-project.org/package=anthro (accessed on 5 February 2021).
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Usinglme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Gu, F.; Ye, W.; Ren, Y.; Guo, S. Colostral and mature breast milk protein compositional determinants in Qingdao, Wuhan and Hohhot: Maternal food culture, vaginal delivery and neonatal gender. Asia Pac. J. Clin. Nutr. 2019, 28, 800–811. [Google Scholar]
- Jiang, J.J. Nutrients and Bioactive Factors and Metabolites in Human; Zhejiang University: Zhejiang, China, 2017. [Google Scholar]
- Wu, X.; Jackson, R.T.; Khan, S.A.; Ahuja, J.; Pehrsson, P.R. Human Milk Nutrient Composition in the United States: Current Knowledge, Challenges, and Research Needs. Curr. Dev. Nutr. 2018, 2, nzy025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. North Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fumeaux, C.J.F.; Garcia-Rodenas, C.L.; De Castro, C.A.; Courtet-Compondu, M.-C.; Thakkar, S.K.; Beauport, L.; Tolsa, J.-F.; Affolter, M. Longitudinal Analysis of Macronutrient Composition in Preterm and Term Human Milk: A Prospective Cohort Study. Nutrients 2019, 11, 1525. [Google Scholar] [CrossRef] [Green Version]
- Sahin, S.; Ozdemir, T.; Katipoglu, N.; Akcan, A.B.; Turkmen, M.K. Comparison of Changes in Breast Milk Macronutrient Content During the First Month in Preterm and Term Infants. Breastfeed. Med. 2020, 15, 56–62. [Google Scholar] [CrossRef]
- Jorgensen, J.M.; Young, R.; Ashorn, P.; Ashorn, U.; Chaima, D.; Davis, J.C.C.; Goonatilleke, E.; Kumwenda, C.; Lebrilla, C.B.; Maleta, K.; et al. Associations of human milk oligosaccharides and bioactive proteins with infant growth and development among Malawian mother-infant dyads. Am. J. Clin. Nutr. 2021, 113, 209–220. [Google Scholar] [CrossRef]
- Jiang, R.; Lönnerdal, B. Osteopontin in human milk and infant formula affects infant plasma osteopontin concentrations. Pediatr. Res. 2019, 85, 502–505. [Google Scholar] [CrossRef]
- Schack, L.; Lange, A.; Kelsen, J.; Agnholt, J.; Christensen, B.; Petersen, T.; Sørensen, E. Considerable variation in the concentration of osteopontin in human milk, bovine milk, and infant formulas. J. Dairy Sci. 2009, 92, 5378–5385. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.Y.; Dar, T.A.; Singh, L.R. Casein proteins: Structural and functional aspects. Milk Proteins–From Structure to Biological Properties and Health Aspects; InTech: Rijeka, Croatia, 2016; pp. 1–17. [Google Scholar]
- Khan, S.; Casadio, Y.S.; Lai, C.T.; Prime, D.K.; Hepworth, A.R.; Trengove, N.J.; Hartmann, P.E. Investigation of Short-term Variations in Casein and Whey Proteins in Breast Milk of Term Mothers. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 136–141. [Google Scholar] [CrossRef]
- Cuillière, M.L.; Trégoat, V.; Béné, M.C.; Faure, G.; Montagne, P. Changes in the κ-casein and β-casein concentrations in human milk during lactation. J. Clin. Lab. Anal. 1999, 13, 213–218. [Google Scholar] [CrossRef]
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; Van Tol, E.A.F.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luque, V.; Closa-Monasterolo, R.; Escribano, J.; Ferré, N. Early Programming by Protein Intake: The Effect of Protein on Adiposity Development and the Growth and Functionality of Vital Organs. Nutr. Metab. Insights 2015, 8, 49–56. [Google Scholar] [CrossRef]
- Koletzko, B.; Von Kries, R.; Monasterolo, R.C.; Subías, J.E.; Scaglioni, S.; Giovannini, M.; Beyer, J.; Demmelmair, H.; Anton, B.; Gruszfeld, D.; et al. Can infant feeding choices modulate later obesity risk? Am. J. Clin. Nutr. 2009, 89, 1502S–1508S. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, C.; Mølgaard, C.; Dalum, C.; Vaag, A.; Michaelsen, K.F. Differential effects of casein versus whey on fasting plasma levels of insulin, IGF-1 and IGF-1/IGFBP-3: Results from a randomized 7-day supplementation study in prepubertal boys. Eur. J. Clin. Nutr. 2009, 63, 1076–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolb, A.F.; Huber, R.C.; Lillico, S.G.; Carlisle, A.; Robinson, C.J.; Neil, C.; Petrie, L.; Sorensen, D.B.; Olsson, I.A.S.; Whitelaw, C.B.A. Milk Lacking α-Casein Leads to Permanent Reduction in Body Size in Mice. PLoS ONE 2011, 6, e21775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigourd, V.; Lopera, I.; Cata, F.; Benoit, G.; Jacquemet, B.; Lapillonne, A. Role of Daily Milk Volume and Period of Lactation in Nutrient Content of Human Milk: Results from a Prospective Study. Nutrients 2020, 12, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dizdar, E.A.; Sari, F.N.; Degirmencioglu, H.; Canpolat, F.E.; Oguz, S.S.; Uras, N.; Dilmen, U. Effect of mode of delivery on macronutrient content of breast milk. J. Matern. Neonatal Med. 2014, 27, 1099–1102. [Google Scholar] [CrossRef]
- Ozmen, E.B.; Okman, E.; Sari, F.N.; Keser, M.K.; Dizdar, E.A.; Tayman, C.; Oguz, S.S. Comparison of the Macronutrient Content of Colostrum: Locals with Refugees. Breastfeed. Med. 2020, 15, 453–457. [Google Scholar] [CrossRef]
- Nissen, E.; Uvnäs-Moberg, K.; Svensson, K.; Stock, S.; Widström, A.-M.; Winberg, J. Different patterns of oxytocin, prolactin but not cortisol release during breastfeeding in women delivered by Caesarean section or by the vaginal route. Early Hum. Dev. 1996, 45, 103–118. [Google Scholar] [CrossRef]
- Dewey, K.G.; Nommsen-Rivers, L.A.; Heinig, M.J.; Cohen, R.J. Risk Factors for Suboptimal Infant Breastfeeding Behavior, Delayed Onset of Lactation, and Excess Neonatal Weight Loss. Pediatrics 2003, 112, 607–619. [Google Scholar] [CrossRef]
- Duan, Y.F.; Jiang, S.; Wang, J.; Zhao, L.Y.; Pang, X.H.; Bi, Y.; Yin, S.A.; Yang, Z.Y. Dietary intake status of Chinese lactating women during the first month postpartum in 2013. Chin. J. Prev. Med. 2016, 50, 1043–1049. [Google Scholar] [CrossRef]
- Forsum, E.; Lönnerdal, B. Effect of protein intake on protein and nitrogen composition of breast milk. Am. J. Clin. Nutr. 1980, 33, 1809–1813. [Google Scholar] [CrossRef]
- Sanchez-Pozo, A.; Morales, J.L.; Izquierdo, A.; Martinez-Valverde, A.; Gil, A. Protein composition of human milk in relation to mothers’ weight and socioeconomic status. Hum. Nutr. Clin. Nutr. 1987, 41, 115–125. [Google Scholar]
- Huang, Z.; Hu, Y.-M. Dietary patterns and their association with breast milk macronutrient composition among lactating women. Int. Breastfeed. J. 2020, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-H.; Hsu, Y.-C.; Lin, M.-C.; Chen, C.-H.; Wang, T.-M. The association of macronutrients in human milk with the growth of preterm infants. PLoS ONE 2020, 15, e0230800. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Participants | Subgroup | p |
|---|---|---|---|
| Number of participants | 105 | 51 | |
| Maternal age (years) | >0.999 | ||
| Below 30 | 58.1 | 56.9 | |
| 30 and above | 41.9 | 43.1 | |
| Education | 0.261 | ||
| Middle school and below | 38.1 | 49.0 | |
| College and above | 61.9 | 51.0 | |
| Per capita household income (RMB/month) | 0.587 | ||
| 4000 and below | 35.2 | 41.2 | |
| Above 4000 | 64.8 | 58.8 | |
| Pre-gestational body mass index (kg/m2) b | 0.807 | ||
| <20.7 | 46.7 | 43.1 | |
| ≥20.7 | 53.3 | 56.9 | |
| Delivery mode | 0.195 | ||
| Cesarean delivery | 25.7 | 37.3 | |
| Vaginal delivery | 74.3 | 62.7 | |
| Parity | 0.767 | ||
| First birth | 78.1 | 74.5 | |
| Others | 21.9 | 25.5 | |
| Infant gender | >0.999 | ||
| Female | 40.0 | 39.2 | |
| Male | 60.0 | 60.8 |
| 1–5 Days (t1) | 8–14 Days (t2) | 1 Month (t3) | 6 Months (t4) | p-Trend | p(t2 vs. t1) | p(t3 vs. t2) | p(t4 vs. t3) | |
|---|---|---|---|---|---|---|---|---|
| Number of samples (overall participants) | 103 | 105 | 105 | 98 | ||||
| Total protein (mg/100 mL) | 1666.2 (447.7) | 1545.2 (416.7) | 1368.3 (406.3) | 993.9 (335.0) | <0.001 | 0.013 | <0.001 | <0.001 |
| α-lactalbumin (mg/100 mL) | 327.9 (63.4) | 333.9 (58.5) | 310.9 (57.3) | 209.0 (52.6) | <0.001 | 0.326 | <0.001 | <0.001 |
| Number of samples (subgroup) | 49 | 51 | 51 | 46 | ||||
| Lactoferrin (mg/100 mL) b | 298.5 (154.1) | 189.5 (81.6) | 114.9 (45.4) | 70.4 (27.4) | <0.001 | <0.001 | <0.001 | <0.001 |
| Osteopontin (mg/100 mL) | 71.8 (30.3) | 58.6 (15.1) | 45.0 (14.8) | 23.6 (12.3) | <0.001 | 0.001 | <0.001 | <0.001 |
| Total casein (mg/100 mL) | 697.1 (191.0) | 632.2 (139.8) | 541.5 (122.7) | 373.9 (120.8) | <0.001 | 0.007 | <0.001 | <0.001 |
| β-casein (mg/100 mL) | 520.9 (147.8) | 484.4 (117.9) | 439.4 (103.3) | 315.4 (101.5) | <0.001 | 0.050 | 0.039 | <0.001 |
| αs-1 casein (mg/100 mL) | 125.4 (44.3) | 104.4 (35.6) | 69.2 (20.9) | 37.9 (19.4) | <0.001 | 0.001 | <0.001 | <0.001 |
| κ-casein (mg/100 mL) | 50.8 (15.9) | 43.4 (10.4) | 32.8 (7.9) | 20.6 (6.3) | <0.001 | <0.001 | <0.001 | <0.001 |
| One Month Postpartum | Six Months Postpartum | p | |
|---|---|---|---|
| Length-for-age Z-score | 0.38 (0.93) | 0.63 (1.31) | 0.036 |
| Weight-for-age Z-score | 0.47 (1.06) | 0.49 (1.17) | 0.841 |
| Weight-for-length Z-score | 0.16 (1.47) | 0.28 (1.16) | 0.453 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Zhao, A.; Lai, S.; Yuan, Q.; Jia, X.; Wang, P.; Zhang, Y. Longitudinal Changes in the Concentration of Major Human Milk Proteins in the First Six Months of Lactation and Their Effects on Infant Growth. Nutrients 2021, 13, 1476. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051476
Zhang J, Zhao A, Lai S, Yuan Q, Jia X, Wang P, Zhang Y. Longitudinal Changes in the Concentration of Major Human Milk Proteins in the First Six Months of Lactation and Their Effects on Infant Growth. Nutrients. 2021; 13(5):1476. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051476
Chicago/Turabian StyleZhang, Jian, Ai Zhao, Shiyun Lai, Qingbin Yuan, Xiaojiang Jia, Peiyu Wang, and Yumei Zhang. 2021. "Longitudinal Changes in the Concentration of Major Human Milk Proteins in the First Six Months of Lactation and Their Effects on Infant Growth" Nutrients 13, no. 5: 1476. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051476