
Adherence to the Mediterranean Diet in a School Population in the Principality of Asturias (Spain): Relationship with Physical Activity and Body Weight

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
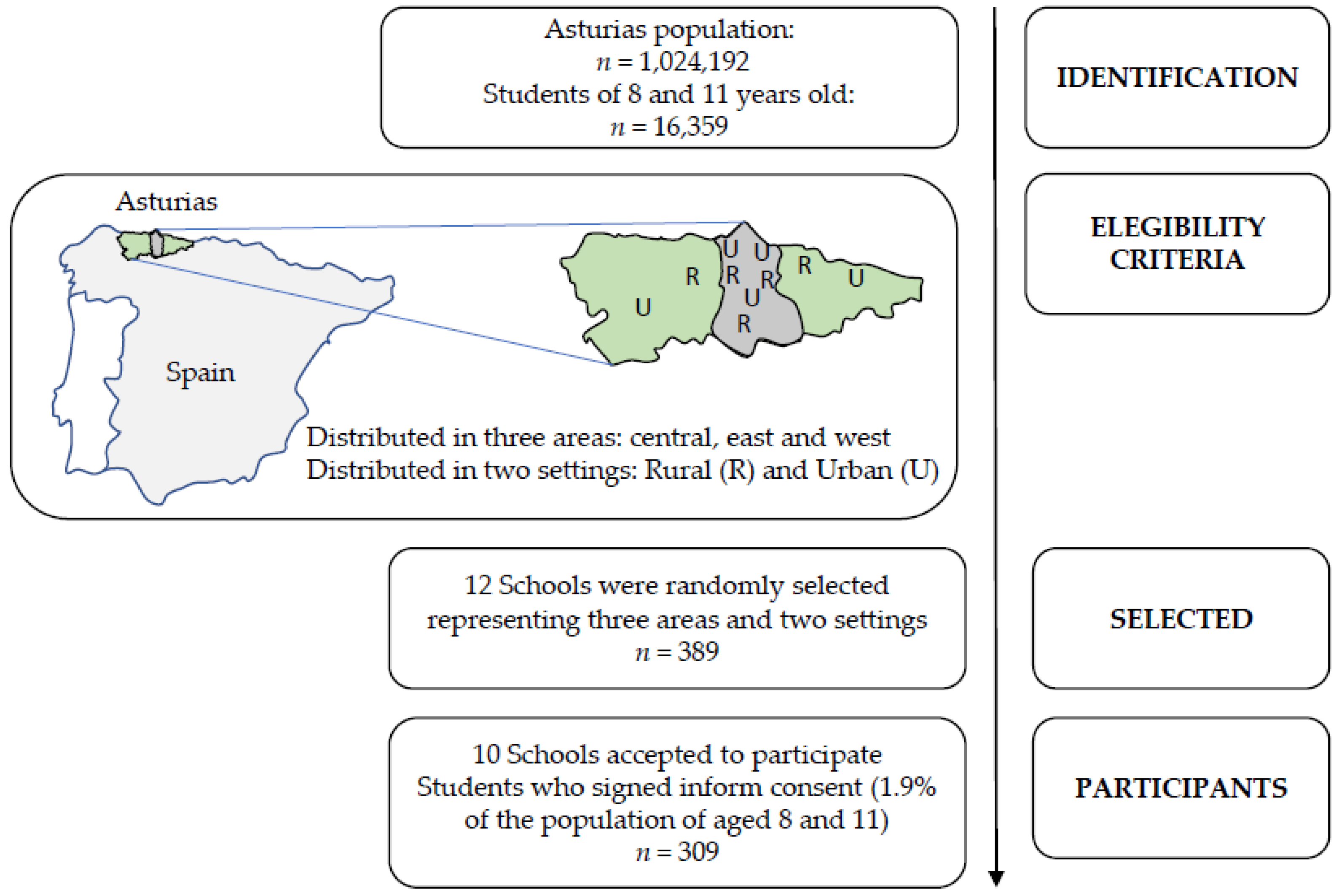
2.1. Participants and Sampling
2.2. Data Collection Instruments
2.3. Data Collection Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 August 2020).
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Report of the Commission on Ending Childhood Obesity. Available online: https://apps.who.int/iris/bitstream/handle/10665/204176/9789241510066_eng.pdf (accessed on 12 August 2020).
- Lobstein, T.; Frelut, M.-L. Prevalence of overweight among children in Europe. Obes. Rev. 2003, 4, 195–200. [Google Scholar] [CrossRef]
- Majem, L.S.; Barba, L.R.; Bartrina, J.A.; Rodrigo, C.P.; Santana, P.S.; Quintana, L.P. Obesidad infantil y juvenil en España. Resultados del Estudio enKid (1998–2000). Med. Clínic. 2003, 121, 725–732. [Google Scholar] [CrossRef]
- Aurrecoechea, B.D.; Echenique, M.S.; Alonso, M.Á.O.; Candás, J.I.P.; Osinaga, J.D. Estado nutricional de la población infantil en Asturias (Estudio ESNUPI-AS): Delgadez, sobrepeso, obesidad y talla baja. Pediatría Atención Primaria 2015, 17, e21–e31. [Google Scholar] [CrossRef] [Green Version]
- Leech, R.M.; McNaughton, A.S.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- Ambrosini, G.L. Childhood dietary patterns and later obesity: A review of the evidence. Proc. Nutr. Soc. 2014, 73, 137–146. [Google Scholar] [CrossRef]
- Muntaner-Mas, A.; Vidal-Conti, J.; Cantallops, J.; Borràs, P.A.; Palou, P. Obesity and physical activity patterns among Balearic Islands children and adolescents: A cross-sectional study. J. Hum. Sport Exerc. 2017, 12, 333–348. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Sánchez-Oliver, A.J.; Ries, F.; González-Jurado, J.A. Mediterranean Diet, Physical Fitness and Body Composition in Sevillian Adolescents: A Healthy Lifestyle. Nutrients 2019, 11, 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosi, A.; Calestani, M.V.; Parrino, L.; Milioli, G.; Palla, L.; Volta, E.; Brighenti, F.; Scazzina, F. Weight Status Is Related with Gender and Sleep Duration but Not with Dietary Habits and Physical Activity in Primary School Italian Children. Nutrients 2017, 9, 579. [Google Scholar] [CrossRef]
- Börnhorst, C.; Wijnhoven, A.T.M.; Kunešová, M.; Yngve, A.; Rito, I.A.; Lissner, L.; Duleva, V.; Petrauskiene, A.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Associations between sleep duration, screen time and food consumption frequencies. BMC Public Health 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graffe, M.I.M.; Pala, V.; De Henauw, S.; Eiben, G.; Hadjigeorgiou, C.; Iacoviello, L.; Intemann, T.; Jilani, H.; Molnar, D.; Russo, P.; et al. Dietary sources of free sugars in the diet of European children: The IDEFICS Study. Eur. J. Nutr. 2019, 59, 979–989. [Google Scholar] [CrossRef]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Morenga, L.T.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondaki, K.; Grammatikaki, E.; Jiménez-Pavón, D.; De Henauw, S.; González-Gross, M.; Sjöström, M.; Gottrand, F.; Molnar, D.A.; Moreno, L.; Kafatos, A.; et al. Daily sugar-sweetened beverage consumption and insulin resistance in European adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr. 2012, 16, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Brouns, F. WHO Guideline: “Sugars intake for adults and children” raises some question marks. Agro Food Ind. HiTech. 2015, 26, 34–36. [Google Scholar]
- Rosi, A.; Paolella, G.; Biasini, B.; Scazzina, F.; Alicante, P.; De Blasio, F.; Russo, M.D.; Rendina, D.; Tabacchi, G.; Cairella, G.; et al. Dietary habits of adolescents living in North America, Europe or Oceania: A review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean Diet. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 544–560. [Google Scholar] [CrossRef]
- Lăcătușu, C.-M.; Grigorescu, E.-D.; Floria, M.; Onofriescu, A.; Mihai, B.-M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public Health 2019, 16, 942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Angelino, D.; Rosi, A.; Dall’Asta, M.; Bresciani, L.; Ferraris, C.; Guglielmetti, M.; Godos, J.; Del Bo’, C.; et al. Effects of Popular Diets on Anthropometric and Cardiometabolic Parameters: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 815–833. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean Diet and Risk of Coronary Heart Disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef]
- Romaguera, D.; Norat, T.; Mouw, T.; May, A.M.; Bamia, C.; Slimani, N.; Travier, N.; Besson, H.; Luan, J.; Wareham, N.; et al. Adherence to the Mediterranean Diet Is Associated with Lower Abdominal Adiposity in European Men and Women. J. Nutr. 2009, 139, 1728–1737. [Google Scholar] [CrossRef] [PubMed]
- Beunza, J.-J.; Toledo, E.; Hu, F.B.; Bes-Rastrollo, M.; Serrano-Martínez, M.; Sánchez-Villegas, A.; Martínez, J.A.; A Martínez-González, M. Adherence to the Mediterranean diet, long-term weight change, and incident overweight or obesity: The Seguimiento Universidad de Navarra (SUN) cohort. Am. J. Clin. Nutr. 2010, 92, 1484–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [Green Version]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Exclusive olive oil consumption was favorably associated with metabolic indices and lifestyle factors in schoolchildren. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; De La Cruz, J.N.; Bach-Faig, A.; Donini, L.M.; Medina, F.-X.; Belahsen, R.; et al. Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef]
- Fernandez, M.; Raheem, D.; Ramos, F.; Carrascosa, C.; Saraiva, A.; Raposo, A. Highlights of Current Dietary Guidelines in Five Continents. Int. J. Environ. Res. Public Health 2021, 18, 2814. [Google Scholar] [CrossRef]
- Grosso, G.; Galvano, F. Mediterranean diet adherence in children and adolescents in southern European countries. NFS J. 2016, 3, 13–19. [Google Scholar] [CrossRef] [Green Version]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11, 1306. [Google Scholar] [CrossRef] [Green Version]
- Garrido-Miguel, M.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Rodríguez-Artalejo, F.; Moreno, L.A.; Ruiz, J.R.; Ahrens, W.; Martínez-Vizcaíno, V. Prevalence and Trends of Overweight and Obesity in European Children From 1999 to 2016. JAMA Pediatrics 2019, 173, e192430. [Google Scholar] [CrossRef]
- Cabrera, S.G.; Fernández, N.H.; Hernández, C.R.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. Kidmed test. prevalence of low adherence to the mediterranean diet in children and young. a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Ojeda-Rodríguez, A.; Zazpe, I.; Morell-Azanza, L.; Chueca, M.J.; Azcona-Sanjulian, M.C.; Marti, A. Improved Diet Quality and Nutrient Adequacy in Children and Adolescents with Abdominal Obesity after a Lifestyle Intervention. Nutrients 2018, 10, 1500. [Google Scholar] [CrossRef] [Green Version]
- MARM. Análisis y Prospectiva-Serie AgrInfo no12. Subdirección General de Análisis, Prospectiva y Coordinación; Ministerio de Medio Ambiente y Medio Rural y Marino: San Marino, Spain, 2019.
- SADEI. Datos Básicos de Asturias 2017; Gobierno del Principado de Asturias: Oviedo, Spain, 2017.
- Grao-Cruces, A.; Nuviala, A.; Fernández-Martínez, A.; Porcel-Gálvez, A.M.; Moral-García, J.E.; Martínez-López, E.-J. Adherence to the Mediterranean diet in rural and urban adolescents of southern Spain, life satisfaction, anthropometry, and physical and sedentary activities. Nutr. Hosp. 2013, 28, 1129–1135. [Google Scholar] [PubMed]
- Guillamón, A.R.; López, P.J.C.; Cantó, E.G.; Soto, J.J.P.; Marcos, L.T. Dieta mediterránea, estado de peso y actividad física en escolares de la Región de Murcia. Clínic. Investig. Arterioscler. 2019, 31, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Idelson, P.I.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; Da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- Arcila-Agudelo, A.M.; Ferrer-Svoboda, C.; Torres-Fernàndez, T.; Farran-Codina, A. Determinants of Adherence to Healthy Eating Patterns in a Population of Children and Adolescents: Evidence on the Mediterranean Diet in the City of Mataró (Catalonia, Spain). Nutrients 2019, 11, 854. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.I.; Dinis, A.; Rascôa, C.; Maia, A.; Mendes, S.; Stein-Novais, C.; Lima, J. Mediterranean Diet Index (KIDMED) Adherence, Socioeconomic Determinants, and Nutritional Status of Portuguese Children: The Eat Mediterranean Program. Port. J. Public Health 2019, 36, 141–149. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [Green Version]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- R Core Team. The R Project for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 26 March 2021).
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the Mediterranean Diet among School Children and Adolescents Living in Northern Italy and Unhealthy Food Behaviors Associated to Overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Domínguez, R.; Pihu, M.; Gísladóttir, T.; Sánchez-Oliver, A.J.; Ries, F. Evaluation of Physical Fitness, Body Composition, and Adherence to Mediterranean Diet in Adolescents from Estonia: The AdolesHealth Study. Int. J. Environ. Res. Public Health 2019, 16, 4479. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Ries, F.; Gisladottir, T.; Domínguez, R.; Sánchez-Oliver, A.J. Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. Int. J. Environ. Res. Public Health 2018, 15, 2632. [Google Scholar] [CrossRef] [Green Version]
- Eurostat Population Statistics at Regional Level; Eurostat: Bruxelles, Belgium, 2020.
- Eurostat Statistics on Regional Population Projections. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Statistics_on_regional_population_projections&oldid=407822 (accessed on 7 December 2020).
- European Commission EU Action Plan on Childhood Obesity. Available online: https://ec.europa.eu/health/sites/health/files/nutrition_physical_activity/docs/childhoodobesity_actionplan_2014_2020_en.pdf (accessed on 7 December 2020).
- Ministerio de Servicios Sociales e Lgualdad. Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarro-llo Infantil y Obesidad en España. Available online: https://www.aesan.gob.es/AECOSAN/docs/documentos/nutricion/observatorio/Estudio_ALADINO_2015.pdf (accessed on 7 December 2020).
- Chacón-Cuberos, R.; Zurita-Ortega, F.; Martínez-Martínez, A.; Olmedo-Moreno, E.M.; Castro-Sánchez, M. Adherence to the Mediterranean Diet Is Related to Healthy Habits, Learning Processes, and Academic Achievement in Adolescents: A Cross-Sectional Study. Nutrients 2018, 10, 1566. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, R.; Cervelló, E.; García, T.; Santos, F.; Iglesias, D. Estudio de las relaciones entre motivación, práctica deportiva extraescolar y hábitos alimenticios y de descanso en estudiantes de Educación Física. Int. J. Clin. Health Psychol. 2007, 7, 385–401. [Google Scholar]
- Cuberos, R.C.; Molina, J.J.M.; Zagalaz, J.C.; Sánchez, M.L.Z.; Sánchez, M.C.; Ortega, F.Z. Actividad física, dieta mediterránea, capacidad aeróbica y clima motivacional hacia el deporte en escolares de la provincia de Granada: Un modelo de ecuaciones estructurales. Nutr. Hosp. 2018, 35, 774–781. [Google Scholar] [CrossRef]
- Guillamón, A.R.; López, P.J.C.; Cantó, E.G.; Soto, J.J.P.; Marcos, L.T.; López, P.J.T. Mediterranean diet, weight status and physical activity in schoolchildren of the Region of Murcia. Clínic. Investig. Arterioscler. 2019, 31, 1–7. [Google Scholar] [CrossRef]
- Wang, Y. Epidemiology of childhood obesity—Methodological aspects and guidelines: What is new? Int. J. Obes. 2004, 28, S21–S28. [Google Scholar] [CrossRef] [Green Version]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [Green Version]
- Carrillo, H.A.; Ramírez-Vélez, R. Adherence to the Mediterranean diet in a sample of Colombian schoolchildren: An evaluation of the psychometric properties of the KIDMED questionnaire]. Nutr. Hosp. 2019, 37, 73–79. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Third Grade | Sixth Grade | Total Sample | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Females (n = 65) | Males (n = 73) | Total (n = 138) | Females (n = 86) | Males (n = 85) | Total (n = 171) | Females (n = 151) | Males (n = 158) | Total (n = 309) | |
| Child characteristics | |||||||||
| Age (years), mean (SD) | 8.3 (0.5) | 8.3 (0.5) | 8.3 (0.5) | 11.4 (0.6) | 11.5 (0.6) | 11.4 (0.6) | 10.1 (1.7) | 10.0 (1.7) | 10 (1.7) |
| Weight (kg), mean (SD) | 32.2 (8.4) | 32.7 (6.3) | 32.4 (7.3) | 45.3 (10.7) | 45.6 (12.0) | 45.5 (11.3) | 39.6 (11.7) | 39.6 (11.7) | 39.6 (11.7) |
| Height (cm), mean (SD) | 133.9 (6.4) | 135.7 (6.4) | 134.8 (6.4) | 150.1 (8.7) | 149.8 (9.6) | 149.9 (9.1) | 143 (11.2) | 143.2 (10.9) | 143.1 (11) |
| BMI (kg/m2), mean (SD) | 17.8 (3.6) | 17.7 (2.7) | 17.7 (3.1) | 20.1 (4.0) | 20.1 (3.5) | 20.1 (3.7) | 19.1 (4.0) | 19.0 (3.4) | 19 (3.7) |
| BMI Categories, n (%) 1 | |||||||||
| Underweight | 6 (9.2) | 5 (6.9) | 11 (8.0) | 10 (11.8) | 4 (4.8) | 14 (8.3) | 16 (10.7) | 9 (5.7) | 25 (8.1) |
| Normal-weight | 41 (63.1) | 49 (67.1) | 90 (65.2) | 49 (57.7) | 51 (60.7) | 100 (59.2) | 90 (60.0) | 100 (63.7) | 190 (61.9) |
| Overweight | 12 (18.5) | 14 (19.2) | 26 (18.8) | 21 (24.7) | 24 (28.6) | 45 (26.6) | 33 (22.0) | 38 (24.2) | 71 (23.1) |
| Obesity | 6 (9.2) | 5 (6.9) | 11 (8.0) | 5 (5.9) | 5 (6.0) | 10 (5.9) | 11 (7.3) | 10 (6.4) | 21 (6.8) |
| Parents characteristic | |||||||||
| Maternal age (years), mean (SD) | 39.6 (5.0) | 40.8 (5.2) | 40.2 (5.1) | 42.6 (5.0) | 42.9 (5.2) | 42.7 (5.1) | 41.3 (5.2) | 41.9 (5.3) | 41.6 (5.3) |
| Paternal age (years), mean (SD) | 42.6 (5.1) | 43 (5.1) | 42.8 (5.1) | 45.1 (5.3) | 45.4 (5.5) | 45.3 (5.4) | 44.0 (5.3) | 44.3 (5.4) | 44.2 (5.4) |
| Maternal education, n (%) 1 | |||||||||
| Primary | 8 (18.2) | 7 (13.7) | 15 (15.8) | 14 (17.5) | 14 (20.0) | 28 (18.7) | 22 (17.7) | 21 (17.4) | 43 (17.6) |
| Secondary/University | 36 (81.8) | 44 (86.3) | 80 (84.2) | 66 (82.5) | 56 (80.0) | 122 (81.3) | 102 (82.3) | 100 (82.6) | 202 (82.4) |
| Paternal education, n (%) 1 | |||||||||
| Primary | 8 (19.1) | 11 (21.6) | 19 (20.4) | 18 (23.7) | 15 (21.4) | 33 (22.6) | 26 (22.0) | 26 (21.5) | 52 (21.8) |
| Secondary/University | 34 (81.0) | 40 (78.4) | 74 (79.6) | 58 (76.3) | 55 (78.6) | 113 (77.4) | 92 (78.0) | 95 (78.5) | 187 (78.2) |
| Lifestyle behaviors | |||||||||
| Exercise practice outside school (days/week), mean (SD) | 3.5 (1.9) | 4.1 (1.7) | 3.8 (1.8) | 3.5 (1.8) | 4.2 (2) | 3.8 (1.9) | 3.5 (1.8) | 4.1 (1.8) | 3.8 (1.9) |
| Attendance at the school canteen (days/week), mean (SD) | 2.6 (2.4) | 2.3 (2.4) | 2.4 (2.4) | 1.4 (2.2) | 1.6 (2.2) | 1.5 (2.2) | 1.9 (2.3) | 1.9 (2.3) | 1.9 (2.3) |
| Sleeping habits (h/weekday), mean (SD) | 9.9 (0.9) | 9.8 (0.9) | 9.8 (0.9) | 9.3 (0.9) | 9.3 (1.0) | 9.3 (1.0) | 9.5 (1.0) | 9.5 (1.0) | 9.5 (1.0) |
| BMI Categories | Weekly Days Exercise Practice Outside School | Weekly Days Attendance at the School Canteen | Sleep Time on Weekdays | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| KIDMED Score Categories | 1.11 (0.66, 1.86) | 0.7 | 1.17 (1.02, 1.33) | 0.02 | 1.09 (0.98, 1.21) | 0.1 | 1.18 (0.91, 1.54) | 0.21 |
| KIDMED Items | ||||||||
| Consumes a fruit or fruit juice every day | 1.64 (0.72, 4.11) | 0.26 | 1.31 (1.10, 1.57) | <0.01 | 1.17 (1.03, 1.36) | 0.03 | 0.97 (0.71, 1.32) | 0.84 |
| Has a second piece of fruit every day | 1.47 (0.90, 2.43) | 0.13 | 1.10 (0.97, 1.25) | 0.14 | 1.09 (0.90, 1.22) | 0.09 | 1.15 (0.90, 1.48) | 0.26 |
| Has fresh or cooked vegetables regularly once a day | 1.04 (0.63, 1.73) | 0.9 | 1.07 (0.95, 1.22) | 0.28 | 1.10 (1.00, 1.22) | 0.06 | 1.58 (0.87, 2.85) | 0.13 |
| Has fresh or cooked vegetables more than once a day | 1.58 (0.87, 2.85) | 0.13 | 0.99 (0.87, 1.13) | 0.93 | 1.11 (1.00, 1.23) | 0.06 | 1.11 (0.84, 1.46) | 0.47 |
| Consumes fish regularly (at least 2–3/week) | 0.95 (0.53, 1.73) | 0.87 | 1.11 (0.95, 1.29) | 0.19 | 1.17 (1.03, 1.34) | 0.02 | 1.06 (0.78, 1.42) | 0.72 |
| Goes >1/week to a fast-food restaurant | 0.95 (0.43, 1.95) | 0.88 | 0.93 (0.77, 1.12) | 0.47 | 0.97 (0.82, 1.12) | 0.66 | 1.13 (0.79, 1.64) | 0.50 |
| Likes pulses and eats >1/week | 0.59 (0.23, 1.60) | 0.28 | 1.09 (0.91, 1.33) | 0.36 | 1.02 (0.88, 1.19) | 0.76 | 1.28 (0.88, 1.87) | 0.19 |
| Consumes pasta/rice every day (5 or more per week) | 1.12 (0.61, 2.02) | 0.71 | 1.05 (0.92, 1.20) | 0.46 | 1.00 (0.90, 1.11) | 0.95 | 0.98 (0.76, 1.28) | 0.89 |
| Has cereals or grains (bread, etc.) for breakfast | 1.23 (0.60, 2.66) | 0.59 | 1.24 (1.03, 1.51) | 0.03 | 1.01 (0.87, 1.17) | 0.93 | 1.02 (0.71, 1.46) | 0.91 |
| Consumes nuts regularly (at least 2–3/week) | 1.43 (0.85, 2.41) | 0.18 | 0.97 (0.85, 1.10) | 0.58 | 1.04 (0.94, 1.16) | 0.44 | 1.15 (0.89, 1.49) | 0.30 |
| Uses olive oil at home | 0.68 (0.24, 2.03) | 0.48 | 1.19 (0.90, 1.61) | 0.23 | 1.03 (0.81, 1.34) | 0.81 | 1.14 (0.66, 1.93) | 0.62 |
| Skips breakfast | 1.03 (0.21, 4.15) | 0.97 | 0.89 (0.67, 1.17) | 0.42 | 1.06 (0.86, 1.31) | 0.55 | 0.65 (0.39, 1.11) | 0.11 |
| Has a dairy product for breakfast (yoghurt, milk, etc) | 4.03 (1.52, 12.97) | 0.01 | 0.93 (0.79, 1.11) | 0.42 | 1.06 (0.92, 1.23) | 0.41 | 1.30 (0.90, 1.88) | 0.16 |
| Has commercially baked goods or pastries for breakfast | 0.70 (0.39, 1.23) | 0.23 | 0.91 (0.79, 1.05) | 0.22 | 1.00 (0.89, 1.12) | 0.96 | 0.92 (0.69, 1.22) | 0.56 |
| Consumes two yoghurts and/or some cheese (40g) daily | 0.75 (0.41, 1.38) | 0.36 | 1.01 (0.89, 1.14) | 0.92 | 1.03 (0.93, 1.15) | 0.53 | 1.02 (0.80, 1.31) | 0.85 |
| Consumes sweets and candy several times every day | 0.96 (0.38, 2.25) | 0.92 | 0.98 (0.79, 1.22) | 0.87 | 1.09 (0.90, 1.31) | 0.37 | 0.83 (0.55, 1.27) | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Iglesias, R.; Álvarez-Pereira, S.; Tardón, A.; Fernández-García, B.; Iglesias-Gutiérrez, E. Adherence to the Mediterranean Diet in a School Population in the Principality of Asturias (Spain): Relationship with Physical Activity and Body Weight. Nutrients 2021, 13, 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051507
Fernández-Iglesias R, Álvarez-Pereira S, Tardón A, Fernández-García B, Iglesias-Gutiérrez E. Adherence to the Mediterranean Diet in a School Population in the Principality of Asturias (Spain): Relationship with Physical Activity and Body Weight. Nutrients. 2021; 13(5):1507. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051507
Chicago/Turabian StyleFernández-Iglesias, Rocío, Sonia Álvarez-Pereira, Adonina Tardón, Benjamín Fernández-García, and Eduardo Iglesias-Gutiérrez. 2021. "Adherence to the Mediterranean Diet in a School Population in the Principality of Asturias (Spain): Relationship with Physical Activity and Body Weight" Nutrients 13, no. 5: 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051507