
Markers of Intestinal Permeability Are Rapidly Improved by Alcohol Withdrawal in Patients with Alcohol-Related Liver Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Measures
2.3. Markers of Intestinal Permeability
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Controls and ALD Patients
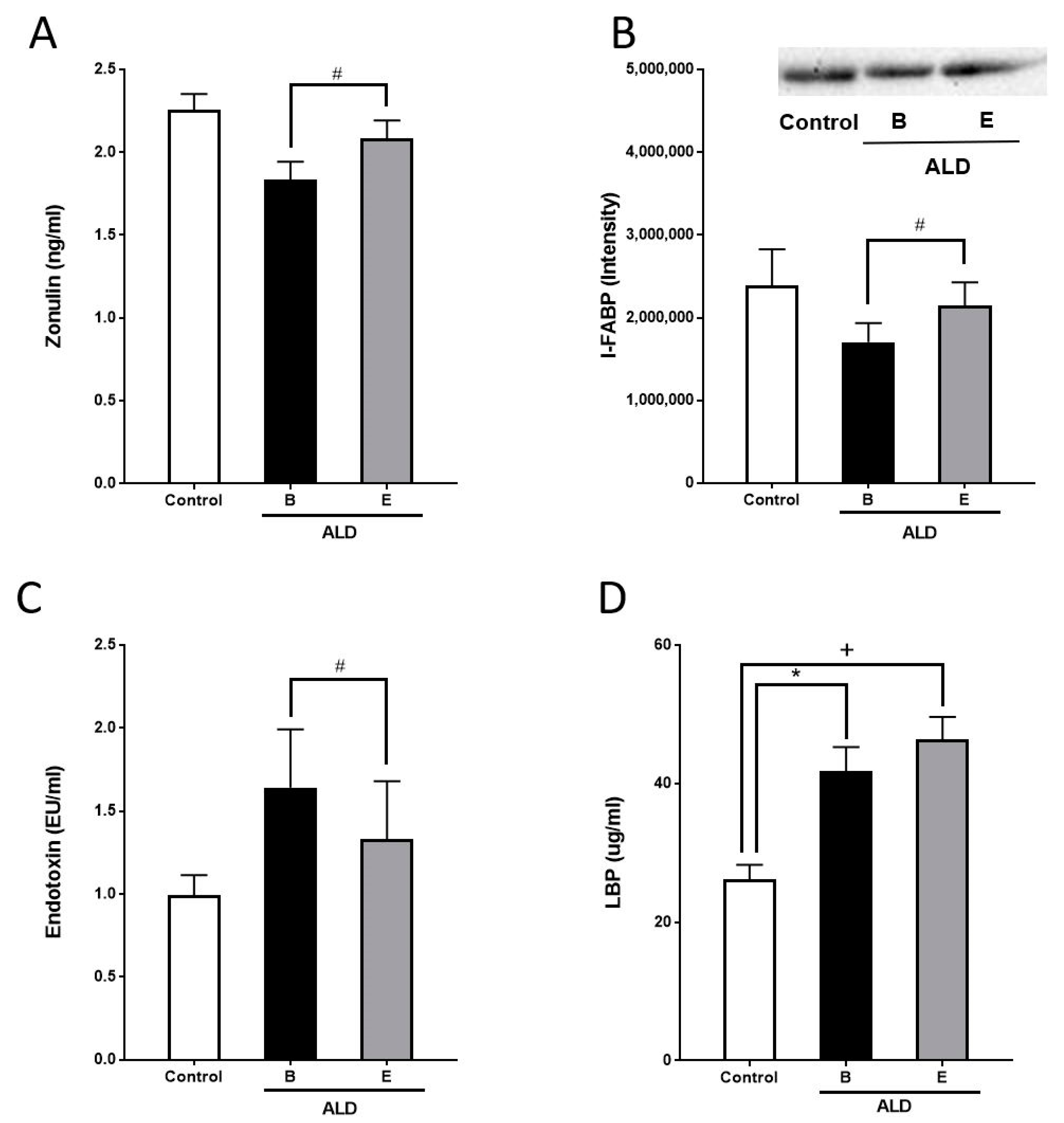
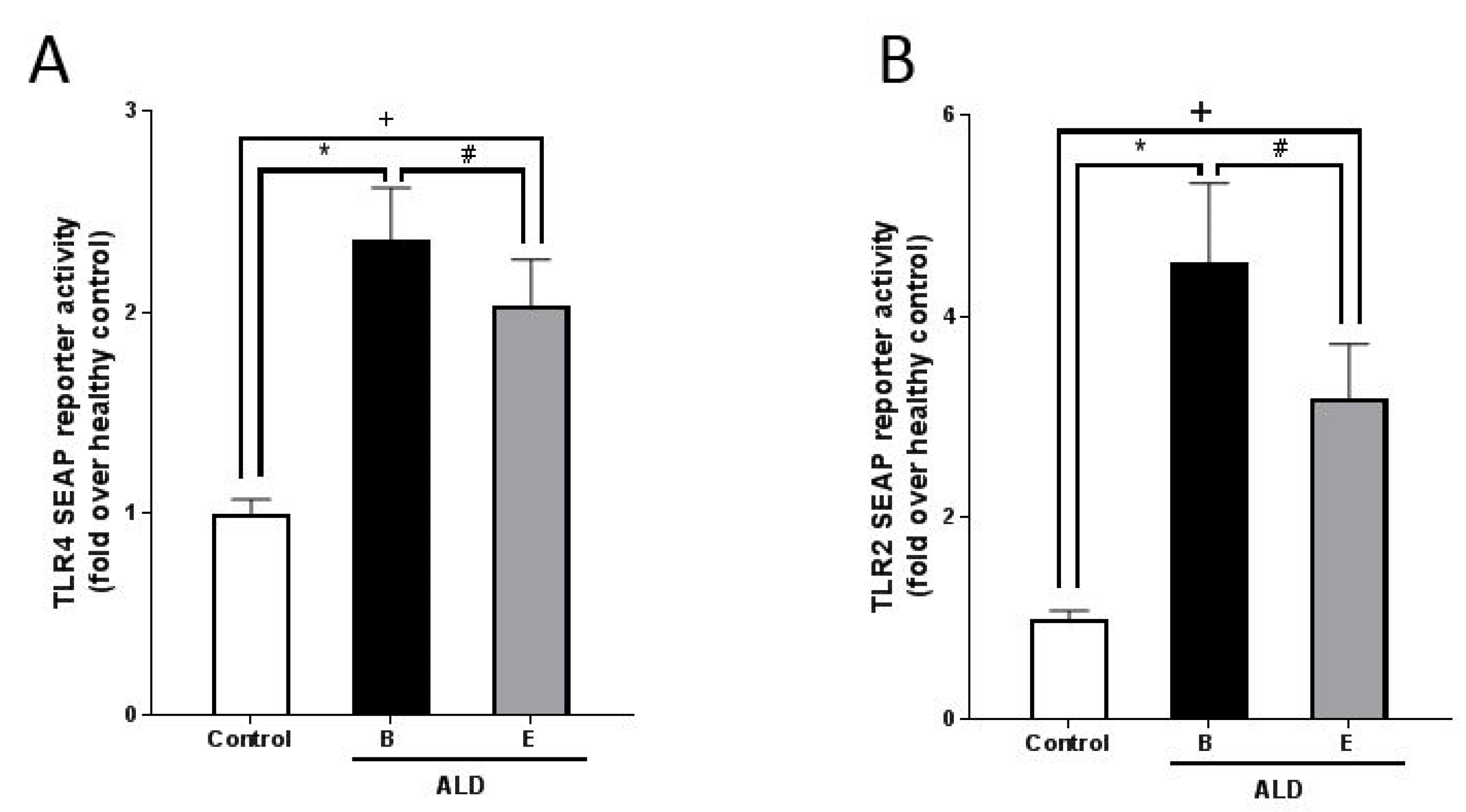
3.2. Markers of Intestinal Permeability in ALD Patients before and after Alcohol Withdrawal
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- WHO. Global Status Report on Alcohol and Health 2018; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Seitz, H.K.; Bataller, R.; Cortez-Pinto, H.; Gao, B.; Gual, A.; Lackner, C.; Mathurin, P.; Mueller, S.; Szabo, G.; Tsukamoto, H. Alcoholic liver disease. Nat. Rev. Dis. Primers 2018, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.E.; Smart, R.G.; Govoni, R. The epidemiology of alcoholic liver disease. Alcohol Res. Health 2003, 27, 209–219. [Google Scholar] [PubMed]
- Hartmann, P.; Seebauer, C.T.; Schnabl, B. Alcoholic liver disease: The gut microbiome and liver cross talk. Alcohol Clin. Exp. Res. 2015, 39, 763–775. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yang, F.; Lu, H.; Wang, B.; Chen, Y.; Lei, D.; Wang, Y.; Zhu, B.; Li, L. Characterization of fecal microbial communities in patients with liver cirrhosis. Hepatology 2011, 54, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Rivera, C.A.; Bradford, B.U.; Seabra, V.; Thurman, R.G. Role of endotoxin in the hypermetabolic state after acute ethanol exposure. Am. J. Physiol. 1998, 275 Pt 1, G1252–G1258. [Google Scholar] [CrossRef]
- Yuki, T.; Thurman, R.G. The swift increase in alcohol metabolism. Time course for the increase in hepatic oxygen uptake and the involvement of glycolysis. Biochem. J. 1980, 186, 119–126. [Google Scholar] [CrossRef]
- Szabo, G. Gut-Liver Axis in Alcoholic Liver Disease. Gastroenterology 2015, 148, 30–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, S.; Cani, P.D.; Neyrinck, A.M.; Starkel, P.; Jamar, F.; Mikolajczak, M.; Delzenne, N.M.; de Timary, P. Role of intestinal permeability and inflammation in the biological and behavioral control of alcohol-dependent subjects. Brain Behav. Immun. 2012, 26, 911–918. [Google Scholar] [CrossRef]
- De Ledinghen, V.; Vergniol, J.; Capdepont, M.; Chermak, F.; Hiriart, J.B.; Cassinotto, C.; Merrouche, W.; Foucher, J.; le Brigitte, B. Controlled attenuation parameter (CAP) for the diagnosis of steatosis: A prospective study of 5323 examinations. J. Hepatol. 2014, 60, 1026–1031. [Google Scholar] [CrossRef]
- Mueller, S.; Nahon, P.; Rausch, V.; Peccerella, T.; Silva, I.; Yagmur, E.; Straub, B.K.; Lackner, C.; Seitz, H.K.; Rufat, P.A.; et al. Caspase-cleaved keratin-18 fragments increase during alcohol withdrawal and predict liver-related death in patients with alcoholic liver disease. Hepatology 2017, 66, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Mueller, S. Liver Elastography: Clinical Use and Interpretation; Springer International Publishing: Basel, Switzerland, 2020. [Google Scholar]
- Mueller, S.; Seitz, H.K.; Rausch, V. Non-invasive diagnosis of alcoholic liver disease. World J. Gastroenterol. 2014, 20, 14626–14641. [Google Scholar] [CrossRef]
- Thiele, M.; Rausch, V.; Fluhr, G.; Kjaergaard, M.; Piecha, F.; Mueller, J.; Straub, B.K.; Lupsor-Platon, M.; De-Ledinghen, V.; Seitz, H.K.; et al. Controlled attenuation parameter and alcoholic hepatic steatosis: Diagnostic accuracy and role of alcohol detoxification. J. Hepatol. 2018, 68, 1025–1032. [Google Scholar] [CrossRef] [Green Version]
- Sellmann, C.; Baumann, A.; Brandt, A.; Jin, C.J.; Nier, A.; Bergheim, I. Oral Supplementation of Glutamine Attenuates the Progression of Nonalcoholic Steatohepatitis in C57BL/6J Mice. J. Nutr. 2017, 147, 2041–2049. [Google Scholar] [CrossRef] [Green Version]
- Tajik, N.; Frech, M.; Schulz, O.; Schalter, F.; Lucas, S.; Azizov, V.; Durholz, K.; Steffen, F.; Omata, Y.; Rings, A.; et al. Targeting zonulin and intestinal epithelial barrier function to prevent onset of arthritis. Nat. Commun. 2020, 11, 1995. [Google Scholar] [CrossRef] [Green Version]
- Bode, C.; Kugler, V.; Bode, J.C. Endotoxemia in patients with alcoholic and non-alcoholic cirrhosis and in subjects with no evidence of chronic liver disease following acute alcohol excess. J. Hepatol. 1987, 4, 8–14. [Google Scholar] [CrossRef]
- Fukui, H.; Brauner, B.; Bode, J.C.; Bode, C. Plasma endotoxin concentrations in patients with alcoholic and non-alcoholic liver disease: Reevaluation with an improved chromogenic assay. J. Hepatol. 1991, 12, 162–169. [Google Scholar] [CrossRef]
- Dentener, M.A.; von Asmuth, E.J.; Francot, G.J.; Marra, M.N.; Buurman, W.A. Antagonistic effects of lipopolysaccharide binding protein and bactericidal/permeability-increasing protein on lipopolysaccharide-induced cytokine release by mononuclear phagocytes. Competition for binding to lipopolysaccharide. J. Immunol. 1993, 151, 4258–4265. [Google Scholar] [PubMed]
- Schumann, R.R. Old and new findings on lipopolysaccharide-binding protein: A soluble pattern-recognition molecule. Biochem. Soc. Trans. 2011, 39, 989–993. [Google Scholar] [CrossRef] [Green Version]
- Turunen, U.; Malkamaki, M.; Valtonen, V.V.; Larinkari, U.; Pikkarainen, P.; Salaspuro, M.P.; Makela, P.H. Endotoxin and liver diseases. High titres of enterobacterial common antigen antibodies in patients with alcoholic cirrhosis. Gut 1981, 22, 849–853. [Google Scholar]
- Lau, E.; Marques, C.; Pestana, D.; Santoalha, M.; Carvalho, D.; Freitas, P.; Calhau, C. The role of I-FABP as a biomarker of intestinal barrier dysfunction driven by gut microbiota changes in obesity. Nutr. Metab. Lond. 2016, 13, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Heo, J.S.; Baek, K.S.; Kim, S.Y.; Kim, J.H.; Baek, K.H.; Kim, K.E.; Sheen, Y.H. Zonulin level, a marker of intestinal permeability, is increased in association with liver enzymes in young adolescents. Clin. Chim. Acta 2018, 481, 218–224. [Google Scholar] [CrossRef] [PubMed]
- De Jong, W.J.; Cleveringa, A.M.; Greijdanus, B.; Meyer, P.; Heineman, E.; Hulscher, J.B. The effect of acute alcohol intoxication on gut wall integrity in healthy male volunteers; a randomized controlled trial. Alcohol 2015, 49, 65–70. [Google Scholar] [CrossRef]
- Donnadieu-Rigole, H.; Pansu, N.; Mura, T.; Pelletier, S.; Alarcon, R.; Gamon, L.; Perney, P.; Apparailly, F.; Lavigne, J.P.; Dunyach-Remy, C. Beneficial Effect of Alcohol Withdrawal on Gut Permeability and Microbial Translocation in Patients with Alcohol Use Disorder. Alcohol Clin. Exp. Res. 2018, 42, 32–40. [Google Scholar] [CrossRef]
- Derikx, J.P.; Blijlevens, N.M.; Donnelly, J.P.; Fujii, H.; Kanda, T.; van Bijnen, A.A.; Heineman, E.; Buurman, W.A. Loss of enterocyte mass is accompanied by diminished turnover of enterocytes after myeloablative therapy in haematopoietic stem-cell transplant recipients. Ann. Oncol. 2009, 20, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.E.; Yu, L.R.; Abdelmegeed, M.A.; Yoo, S.H.; Song, B.J. Apoptosis of enterocytes and nitration of junctional complex proteins promote alcohol-induced gut leakiness and liver injury. J. Hepatol. 2018, 69, 142–153. [Google Scholar] [CrossRef]
- Moreno, C.; Mueller, S.; Szabo, G. Non-invasive diagnosis and biomarkers in alcohol-related liver disease. J. Hepatol. 2019, 70, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Keshavarzian, A.; Holmes, E.W.; Patel, M.; Iber, F.; Fields, J.Z.; Pethkar, S. Leaky gut in alcoholic cirrhosis: A possible mechanism for alcohol-induced liver damage. Am. J. Gastroenterol. 1999, 94, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Parlesak, A.; Schafer, C.; Schutz, T.; Bode, J.C.; Bode, C. Increased intestinal permeability to macromolecules and endotoxemia in patients with chronic alcohol abuse in different stages of alcohol-induced liver disease. J. Hepatol. 2000, 32, 742–747. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Controls | ALD Patients |
|---|---|---|
| Gender (m/f) | (10/7) | (26/11) |
| Age (years) | 45.1 ± 2.3 | 49.0 ± 1.5 |
| BMI (kg/m2) | 22.7 ± 0.7 | 27.2 ± 1.09 a |
| High alcohol consumption (years) | n.a. | 29.7 ± 1.9 |
| Alcohol (g/d) (m/f) | - | 206.6 ± 25.0/156.0 ± 24.3 |
| Steatosis | - | |
| Grade 1 | 0 | 7 |
| Grade 2 | 0 | 19 |
| Grade 3 | 0 | 8 |
| unclassified | 0 | 3 |
| AST (U/L) | ||
| before | 21.1 ± 1.0 | 104.8 ± 14.7 a |
| after | - | 62.17 ± 4.8 a,b |
| ALT (U/L) | ||
| before | 19.5 ± 0.8 | 78.0 ± 9.3 a |
| after | - | 66.47 ± 7.3 a,b |
| gGT (U/L) | ||
| before | 17.5 ± 1.2 | 587.7 ± 132.7 a |
| after | - | 414.9 ± 94.6 a,b |
| Liver stiffness | ||
| Before (kPa) | - | 17.42 ± 3.68 |
| F0-F2 (n) | - | 24 |
| F3-F4 (n) | - | 12 |
| After (kPa) | - | 13.86 ± 2.92 b |
| F0-F2 (n) | - | 22 |
| F3-F4 (n) | - | 14 |
| CAP (dB/m) | ||
| before | - | 315.0 ± 7.7 |
| after | - | 274.9 ± 10.6 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, F.; Burger, K.; Staltner, R.; Brandt, A.; Mueller, S.; Bergheim, I. Markers of Intestinal Permeability Are Rapidly Improved by Alcohol Withdrawal in Patients with Alcohol-Related Liver Disease. Nutrients 2021, 13, 1659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051659
Jung F, Burger K, Staltner R, Brandt A, Mueller S, Bergheim I. Markers of Intestinal Permeability Are Rapidly Improved by Alcohol Withdrawal in Patients with Alcohol-Related Liver Disease. Nutrients. 2021; 13(5):1659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051659
Chicago/Turabian StyleJung, Finn, Katharina Burger, Raphaela Staltner, Annette Brandt, Sebastian Mueller, and Ina Bergheim. 2021. "Markers of Intestinal Permeability Are Rapidly Improved by Alcohol Withdrawal in Patients with Alcohol-Related Liver Disease" Nutrients 13, no. 5: 1659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051659