
Association between Chronotype and Nutritional, Clinical and Sociobehavioral Characteristics of Adults Assisted by a Public Health Care System in Brazil

 and
and
Abstract
:1. Introduction
2. Materials and Methods
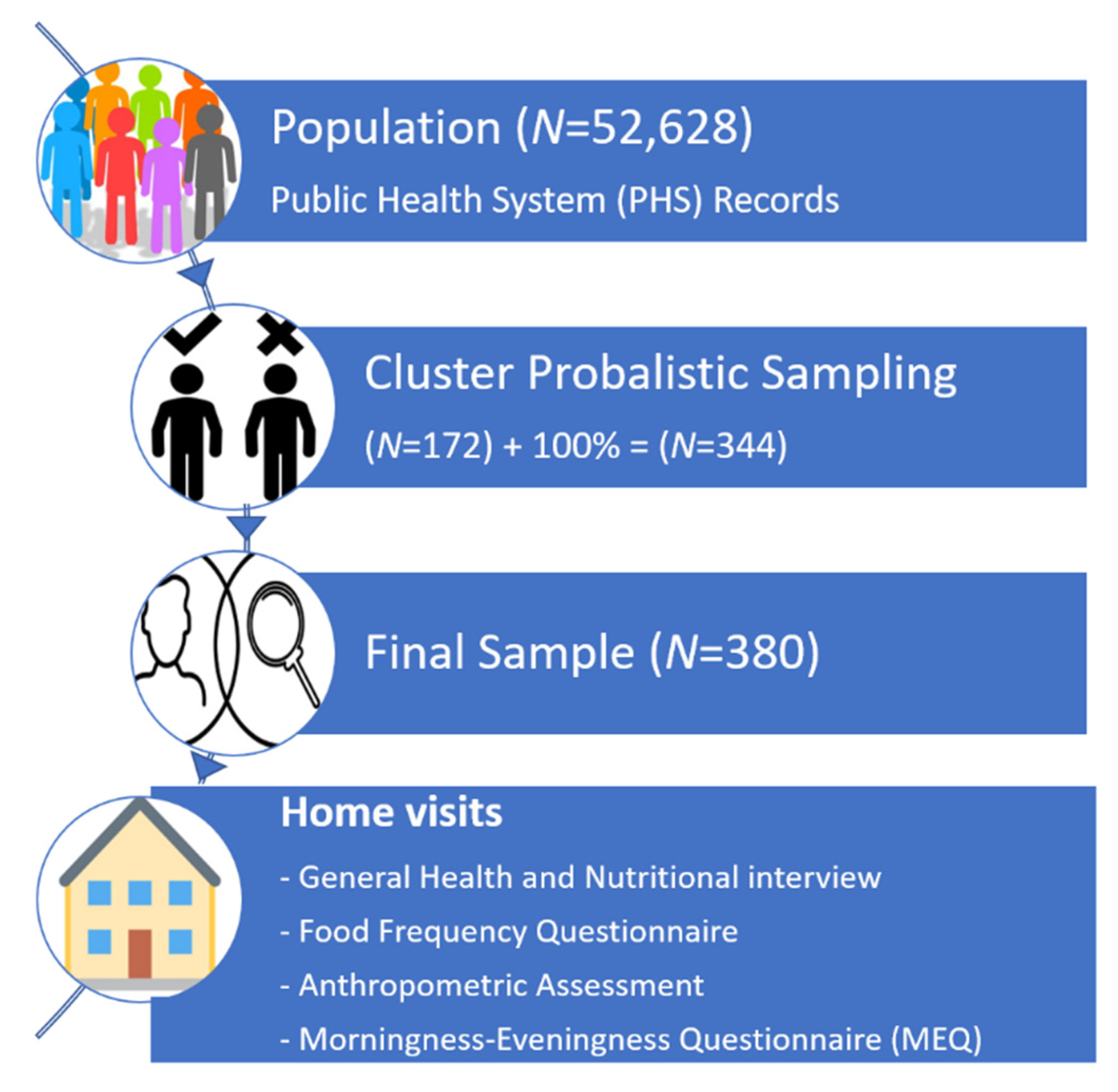
2.1. Study Design and Sampling
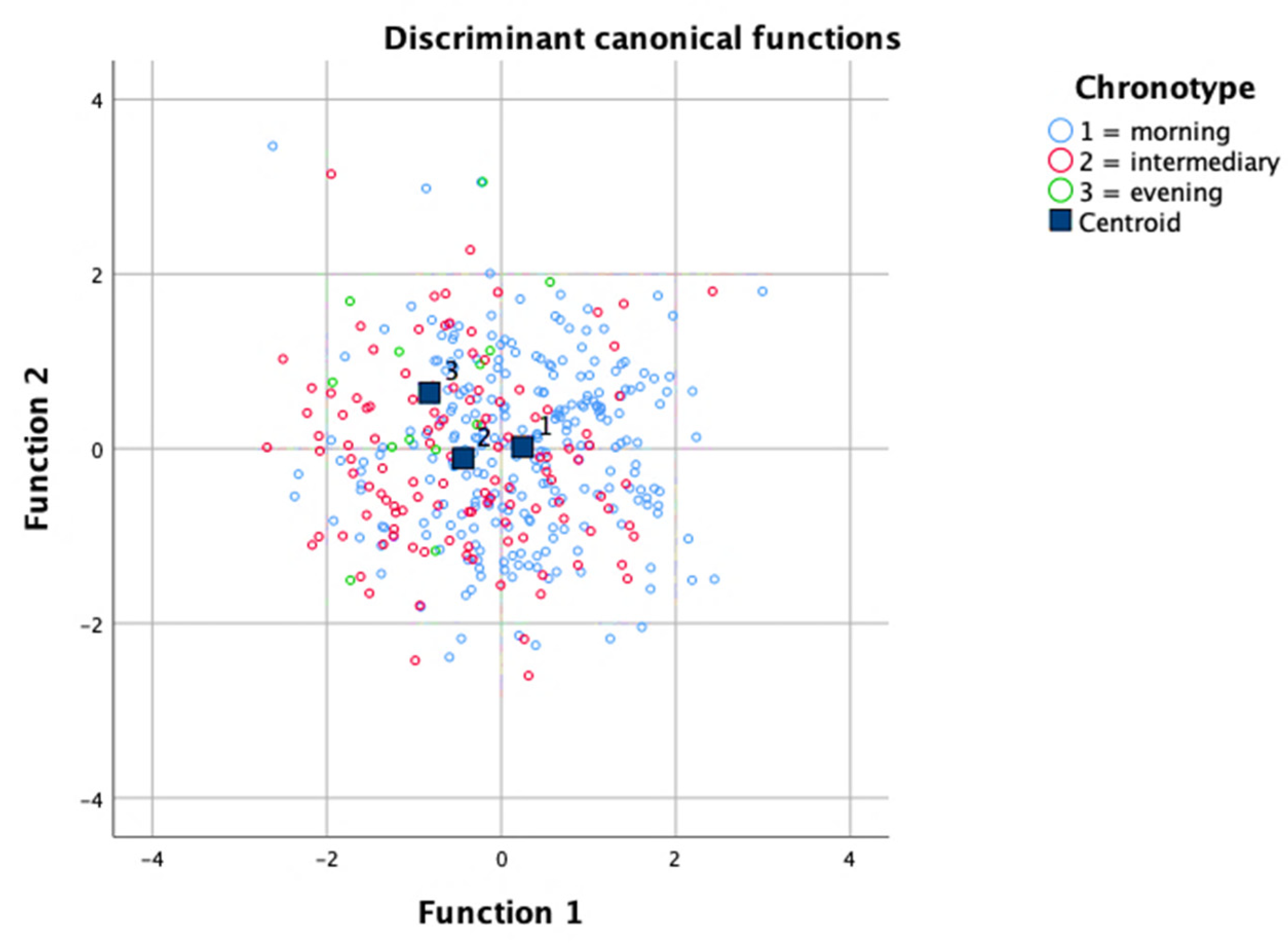
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almoosawi, S.; Vingeliene, S.; Gachon, F.; Voortman, T.; Palla, L.; Johnston, J.D.; Van Dam, R.M.; Darimont, C.; Karagounis, L.G. Chronotype: Implications for Epidemiologic Studies on Chrono-Nutrition and Cardiometabolic Health. Adv. Nutr. 2019, 10, 30–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitale, J.A.; Roveda, E.; Montaruli, A.; Galasso, L.; Weydahl, A.; Caumo, A.; Carandente, F. Chronotype influences activity circadian rhythm and sleep: Differences in sleep quality between weekdays and weekend. Chronobiol. Int. 2015, 32, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Allebrandt, K.V.; Roenneberg, T. The search for circadian clock components in humans: New perspectives for association studies. Braz. J. Med. Biol. Res. 2008, 41, 716–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Mat Ludin, A.F. The Association between Chronotype and Dietary Pattern among Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Horne, J.A.; Östberg, O. A Self Assessment Questionnaire to Determine Morningness Eveningness in Human Circadian Rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social jetlag: Misalignment of biological and social time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef]
- Foster, R.G.; Roenneberg, T. Review Human Responses to the Geophysical Daily, Annual and Lunar Cycles. Curr. Biol. 2008, 18, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Leonhard, C.; Randler, C. In sync with the family: Children and partners influence the sleep-wake circadian rhythm and social habits of women. Chronobiol. Int. 2009, 26, 510–525. [Google Scholar] [CrossRef]
- Dimitrov, A.; Veer, I.M.; Kleeblatt, J.; Seyfarth, F.; Roenneberg, T.; Ising, M.; Uhr, M.; Keck, M.E.; Kramer, A.; Berger, M.; et al. Chronotype is associated with psychological well-being depending on the composition of the study sample. J. Health Psychol. 2020, 25, 1236–1247. [Google Scholar] [CrossRef]
- Kantermann, T.; Sung, H.; Burgess, H.J. Comparing the Morningness-Eveningness Questionnaire and Munich ChronoType Questionnaire to the dim light melatonin onset. J. Biol. Rhythm. 2015, 30, 449–453. [Google Scholar] [CrossRef] [Green Version]
- Levandovski, R.; Sasso, E.; Hidalgo, M.P. Chronotype: A review of the advances, limits and applicability of the main instruments used in the literature to assess human phenotype. Trends Psychiatry Psychother. 2013, 35, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sridhar, G.R.; Sanjana, N.S.N. Sleep, circadian dysrhythmia, obesity and diabetes. World J. Diabetes 2016, 7, 515. [Google Scholar] [CrossRef]
- Glazer Baron, K.; Reid, K.J. Circadian Misalignment and Health. Int. Rev. Psychiatry 2014, 26, 139–154. [Google Scholar] [CrossRef] [Green Version]
- Prasai, M.J.; Pernicova, I.; Grant, P.J.; Scott, E.M. An endocrinologist’s guide to the clock. J. Clin. Endocrinol. Metab. 2011, 96, 913–922. [Google Scholar] [CrossRef] [Green Version]
- Forouzanfar, M.H.; Alexander, L.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Casey, D.; Coates, M.M.; Delwiche, K.; Estep, K.; Frostad, J.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [Green Version]
- Sacco, R.L.; Roth, G.A.; Reddy, K.S.; Arnett, D.K.; Bonita, R.; Gaziano, T.A.; Heidenreich, P.A.; Huffman, M.D.; Mayosi, B.M.; Mendis, S.; et al. The Heart of 25 by 25: Achieving the Goal of Reducing Global and Regional Premature Deaths from Cardiovascular Diseases and Stroke: A Modeling Study From the American Heart Association and World Heart Federation. Glob. Heart 2016, 11, 251. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Prim. 2015, 1, 1–22. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Knutson, K.L.; von Schantz, M. Associations between chronotype, morbidity and mortality in the UK Biobank cohort. Chronobiol. Int. 2018, 35, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, F.; Malone, S.K.; Grandner, M.A.; Lozano, A.; Perkett, M.; Hanlon, A. Interactive effects of sleep duration and morning/evening preference on cardiovascular risk factors. Eur. J. Public Health 2018, 28, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Buijs, F.N.; León-Mercado, L.; Guzmán-Ruiz, M.; Guerrero-Vargas, N.N.; Romo-Nava, F.; Buijs, R.M. The circadian system: A regulatory feedback network of periphery and brain. Physiology 2016, 31, 170–181. [Google Scholar] [CrossRef]
- Hahm, B.-J.; Jo, B.; Dhabhar, F.S.; Palesh, O.; Aldridge-Gerry, A.; Bajestan, S.N.; Neri, E.; Nouriani, B.; Spiegel, D.; Zeitzer, J.M. Bedtime misalignment and progression of breast cancer. Chronobiol. Int. 2014, 31, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating Night Shifts and Risk of Breast Cancer in Women Participating in the Nurses’ Health Study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, P.M.; Hasler, B.P.; Kamarck, T.W.; Muldoon, M.F.; Manuck, S.B. Social Jetlag, Chronotype, and Cardiometabolic Risk. J. Clin. Endocrinol. Metab. 2015, 100, 4612–4620. [Google Scholar] [CrossRef]
- Boege, H.L.; Bhatti, M.Z.; St-Onge, M.-P. Circadian rhythms and meal timing: Impact on energy balance and body weight. Curr. Opin. Biotechnol. 2021, 70, 1–6. [Google Scholar] [CrossRef]
- Challet, E. The circadian regulation of food intake. Nat. Rev. Endocrinol. 2019, 15, 393–405. [Google Scholar] [CrossRef]
- Armstrong, S. A chronometric approach to the study of feeding behavior. Neurosci. Biobehav. Rev. 1980, 4, 27–53. [Google Scholar] [CrossRef]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L. The relationship between breakfast skipping, chronotype, and glycemic control in type 2 diabetes. Chronobiol. Int. 2014, 31, 64–71. [Google Scholar] [CrossRef]
- Meule, A.; Roeser, K.; Randler, C.; Kübler, A. Skipping breakfast: Morningness-eveningness preference is differentially related to state and trait food cravings. Eat. Weight Disord. 2012, 17, 304–308. [Google Scholar] [CrossRef]
- Dashti, H.S.; Scheer, F.A.J.L.; Jacques, P.F.; Lamon-Fava, S.; Ordovás, J.M. Short Sleep Duration and Dietary Intake: Epidemiologic Evidence, Mechanisms, and Health Implications. Adv. Nutr. 2015, 6, 648–659. [Google Scholar] [CrossRef]
- World Bank. World Bank Country and Lending Groups–World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 24 March 2021).
- Tangcharoensathien, V.; Mills, A.; Palu, T. Accelerating health equity: The key role of universal health coverage in the Sustainable Development Goals. BMC Med. 2015, 13, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, M.L.; Menzies, D.; Hone, T.; Dehghani, K.; Trajman, A. The impact of the Brazilian family health on selected primary care sensitive conditions: A systematic review. PLoS ONE 2017, 12, e0182336. [Google Scholar] [CrossRef]
- Gouveia, É.R.; Gouveia, B.R.; Marques, A.; Peralta, M.; França, C.; Lima, A.; Campos, A.; Jurema, J.; Kliegel, M.; Ihle, A. Predictors of metabolic syndrome in adults and older adults from amazonas, brazil. Int. J. Environ. Res. Public Health 2021, 18, 1303. [Google Scholar] [CrossRef]
- Abrantes, M.M.; Lamounier, J.A.; Colosimo, E.A. Overweight and obesity prevalence in Northeast and Southeast Regions of Brazil. Rev. Assoc. Med. Bras. 2003, 49, 162–166. [Google Scholar] [CrossRef] [Green Version]
- Soares, D.A.; Barreto, S.M. Sobrepeso e obesidade abdominal em adultos quilombolas, Bahia, Brasil TT-El sobrepeso y la obesidad abdominal en adultos quilombolas, Bahía, Brasil TT-Overweight and abdominal obesity in adults in a quilombo community in Bahia State, Brazil. Cad. Saude Publica 2014, 30, 341–354. [Google Scholar] [CrossRef] [Green Version]
- Fisberg, R.M.; Colucci, A.C.A.; Morimoto, J.M.; Marchioni, D.M.L. Food frequency questionnaire for adults from a population-based study. Rev. Saude Publica 2008, 42, 542–545. [Google Scholar] [CrossRef] [Green Version]
- Crispim, S.P.; Fisberg, R.M.; Almeida, C.C.B.; Nicolas, G.; Knaze, V.; Pereira, R.A.; Marchiori, D.M.L.; dos Santos, N.A.; Steluti, J.; Slimani, N. Manual Fotográfico de Quantificação Alimentar; Universidade Federal do Paraná: Curitiba, Brazil, 2017; ISBN 9788568566084. [Google Scholar]
- Costa, P.D.; Canaan, J.C.R.; Midori Castelo, P.; Campideli Fonseca, D.; Márcia Pereira-Dourado, S.; Mendonça Murata, R.; Pardi, V.; José Pereira, L. Influence of Micronutrient Intake, Sociodemographic, and Behavioral Factors on Periodontal Status of Adults Assisted by a Public Health Care System in Brazil: A Cross-Sectional Multivariate Analysis. Nutrients 2021, 13, 973. [Google Scholar] [CrossRef] [PubMed]
- Brazilian Food Composition Table-TACO. Available online: http://189.28.128.100/nutricao/docs/taco/tab_bras_de_comp_de_alim_doc.pdf (accessed on 9 April 2019).
- Brasil. Health Ministry. Guidelines for the Collection and Analysis of Anthropometric Data in Health Services-Technical Standard for Food and Nuance Systems-SISVAN. 2011. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/orientacoes_coleta_analise_dados_antropometricos.pdf (accessed on 9 April 2019).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. In Report of a WHO Consultation; World Health Organization, 2000; p. 894. [Google Scholar]
- Benedito-Silva, A.A.; Menna-Barreto, L.; Marques, N.; Tenreiro, S. A self-assessment questionnaire for the determination of morningness-eveningness types in Brazil. Prog. Clin. Biol. Res. 1990, 341B, 89–98. [Google Scholar] [PubMed]
- Carrier, J.; Monk, T.H.; Buysse, D.J.; Kupfer, D.J. Sleep and morningness-eveningness in the “middle” years of life (20–59 y). J. Sleep Res. 1997, 6, 230–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Ma, J.; Yao, K.; Su, W.; Tan, B.; Wu, X.; Huang, X.; Li, T.; Yin, Y.; Tosini, G.; et al. Circadian rhythms and obesity: Timekeeping governs lipid metabolism. J. Pineal Res. 2020, 69, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Logan, R.W.; Ma, T.; Lewis, D.A.; Tseng, G.C.; Sibille, E.; McClung, C.A. Effects of aging on circadian patterns of gene expression in the human prefrontal cortex. Proc. Natl. Acad. Sci. USA 2016, 113, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofman, M.A.; Swaab, D.F. Living by the clock: The circadian pacemaker in older people. Ageing Res. Rev. 2006, 5, 33–51. [Google Scholar] [CrossRef] [PubMed]
- Archer, S.N.; Laing, E.E.; Möller-Levet, C.S.; van der Veen, D.R.; Bucca, G.; Lazar, A.S.; Santhi, N.; Slak, A.; Kabiljo, R.; von Schantz, M.; et al. Mistimed sleep disrupts circadian regulation of the human transcriptome. Proc. Natl. Acad. Sci. USA 2014, 111, E682–E691. [Google Scholar] [CrossRef] [Green Version]
- Randler, C. Gender differences in morningness-eveningness assessed by self-report questionnaires: A meta-analysis. Pers. Individ. Dif. 2007, 43, 1667–1675. [Google Scholar] [CrossRef]
- Preckel, F.; Lipnevich, A.A.; Schneider, S.; Roberts, R.D. Chronotype, cognitive abilities, and academic achievement: A meta-analytic investigation. Learn. Individ. Differ. 2011, 21, 483–492. [Google Scholar] [CrossRef]
- Duffy, J.F.; Cain, S.W.; Chang, A.M.; Phillips, A.J.K.; Münch, M.Y.; Gronfier, C.; Wyatt, J.K.; Dijk, D.J.; Wright, K.P.; Czeisler, C.A. Sex difference in the near-24-h intrinsic period of the human circadian timing system. Proc. Natl. Acad. Sci. USA 2011, 108, 15602–15608. [Google Scholar] [CrossRef] [Green Version]
- Adan, A.; Natale, V. Gender differences in morningness-eveningness preference. Chronobiol. Int. 2002, 19, 709–720. [Google Scholar] [CrossRef]
- Song, J.; Stough, C. The relationship between morningness–eveningness, time-of-day, speed of information processing, and intelligence. Pers. Individ. Dif. 2000, 29, 1179–1190. [Google Scholar] [CrossRef]
- Panev, A.S.; Tserne, T.A.; Polugrudov, A.S.; Bakutova, L.A.; Petrova, N.B.; Tatarinova, O.V.; Kolosova, O.N.; Borisenkov, M.F. Association of chronotype and social jetlag with human non-verbal intelligence. Chronobiol. Int. 2017, 34, 977–980. [Google Scholar] [CrossRef]
- Parsons, M.J.; Moffitt, T.E.; Gregory, A.M.; Goldman-Mellor, S.; Nolan, P.M.; Poulton, R.; Caspi, A. Social jetlag, obesity and metabolic disorder: Investigation in a cohort study. Int. J. Obes. 2015, 39, 842–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Didikoglu, A.; Maharani, A.; Payton, A.; Pendleton, N.; Canal, M.M. Longitudinal change of sleep timing: Association between chronotype and longevity in older adults. Chronobiol. Int. 2019, 36, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- IBGE. Instituto Brasileiro de Geografia e Estatística. In Pesquisa Nacional por Amostra de Domicílios Contínua—PNAD Contínua da Educação 2018; 2019; pp. 1–12. Available online: https://www.ibge.gov.br/estatisticas/sociais/habitacao/17270-pnad-continua.html (accessed on 24 February 2021).
- Alam, M.F.; Tomasi, E.; Lima, M.S.; Areas, R.; Menna-Barreto, L. Characterization and distribution of chronotypes in southern Brazil: Gender and season of birth differences. J. Bras. Psiquiatr. 2008, 57, 83–90. [Google Scholar] [CrossRef]
- von Schantz, M.; Taporoski, T.P.; Horimoto, A.R.; Duarte, N.E.; Vallada, H.; Krieger, J.E.; Pedrazzoli, M.; Negrão, A.B.; Pereira, A.C. Distribution and heritability of diurnal preference (chronotype) in a rural Brazilian family-based cohort, the Baependi study. Sci Rep. 2015, 5, 9214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, D.F.; Curtis, A.M.; Cheng, Y.; Westgate, E.J.; Rudic, R.D.; Paschos, G.; Morris, J.; Ouyang, M.; Thomas, S.A.; FitzGerald, G.A. Peripheral circadian clock rhythmicity is retained in the absence of adrenergic signaling. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, N.; Maemura, K. Circadian clock and cardiovascular disease. J. Cardiol. 2011, 57, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crnko, S.; Du Pré, B.C.; Sluijter, J.P.G.; Van Laake, L.W. Circadian rhythms and the molecular clock in cardiovascular biology and disease. Nat. Rev. Cardiol. 2019, 16, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Takeda, N.; Maemura, K.; Horie, S.; Oishi, K.; Imai, Y.; Harada, T.; Saito, T.; Shiga, T.; Amiya, E.; Manabe, I.; et al. Thrombomodulin is a clock-controlled gene in vascular endothelial cells. J. Biol. Chem. 2007, 282, 32561–32567. [Google Scholar] [CrossRef] [Green Version]
- Ohkura, N.; Oishi, K.; Fukushima, N.; Kasamatsu, M.; Atsumi, G.I.; Ishida, N.; Horie, S.; Matsuda, J. Circadian clock molecules CLOCK and CRYs modulate fibrinolytic activity by regulating the PAI-1 gene expression. J. Thromb. Haemost. 2006, 4, 2478–2485. [Google Scholar] [CrossRef]
- Merikanto, I.; Lahti, T.; Puolijoki, H.; Vanhala, M.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Kronholm, E.; Partonen, T. Associations of Chronotype and Sleep with Cardiovascular Diseases and Type 2 Diabetes. Chronobiol. Int. 2013, 30, 470–477. [Google Scholar] [CrossRef]
- Makarem, N.; Paul, J.; Giardina, E.-G.V.; Liao, M.; Aggarwal, B. Evening chronotype is associated with poor cardiovascular health and adverse health behaviors in a diverse population of women. Chronobiol. Int. 2020, 37, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social jetlag and obesity. Curr. Biol. 2012, 22, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Gangwisch, J.E. Epidemiological evidence for the links between sleep, circadian rhythms and metabolism. Obes. Rev. 2009, 10, 37–45. [Google Scholar] [CrossRef]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Kronholm, E.; Tapanainen, H.; Kontto, J.; Männistö, S. Chronotype differences in timing of energy and macronutrient intakes: A population-based study in adults. Obesity 2017, 25, 608–615. [Google Scholar] [CrossRef] [Green Version]
- Kreier, F.; Yilmaz, A.; Kalsbeek, A.; Romijn, J.A.; Sauerwein, H.P.; Fliers, E.; Buijs, R.M. Hypothesis: Shifting the Equilibrium from Activity to Food Leads to Autonomic Unbalance and the Metabolic Syndrome. Diabetes 2003, 52, 2652–2656. [Google Scholar] [CrossRef] [Green Version]
- Meier, A.H.; Cincotta, A.H. Circadian rhythms regulate the expression of the thrifty genotype/phenotype. Diabetes Rev. 1996, 4, 464–487. [Google Scholar]
- Doherty, R.; Madigan, S.; Warrington, G.; Ellis, J. Sleep and nutrition interactions: Implications for athletes. Nutrients 2019, 11, 822. [Google Scholar] [CrossRef] [Green Version]
- Greco, J.A.; Oosterman, J.E.; Belsham, D.D. Differential effects of omega-3 fatty acid docosahexaenoic acid and palmitate on the circadian transcriptional profile of clock genes in immortalized hypothalamic neurons. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R1049–R1060. [Google Scholar] [CrossRef] [Green Version]
- Ailhaud, G.; Massiera, F.; Weill, P.; Legrand, P.; Alessandri, J.; Guesnet, P. Temporal changes in dietary fats: Role of n−6 polyunsaturated fatty acids in excessive adipose tissue development and relationship to obesity. Prog. Lipid Res. 2006, 45, 203–236. [Google Scholar] [CrossRef]
- IBGE. Brazilian Institute of Geography and Statistics. Family Budget Research–POF 2017–2018. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101742.pdf (accessed on 12 March 2021).
- Muhlhausler, B.S.; Ailhaud, G.P. Omega-6 polyunsaturated fatty acids and the early origins of obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [Green Version]
- Kolbe, I.; Oster, H. Chronodisruption, metabolic homeostasis, and the regulation of inflammation in adipose tissues. Yale J. Biol. Med. 2019, 92, 317–325. [Google Scholar] [PubMed]
- Arango Duque, G.; Descoteaux, A. Macrophage Cytokines: Involvement in Immunity and Infectious Diseases. Front. Immunol. 2014, 5, 491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leproult, R.; Holmbäck, U.; Van Cauter, E. Circadian misalignment augments markers of insulin resistance and inflammation, independently of sleep loss. Diabetes 2014, 63, 1860–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peuhkuri, K.; Sihvola, N.; Korpela, R. Diet promotes sleep duration and quality. Nutr. Res. 2012, 32, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Sato-Mito, N.; Sasaki, S.; Murakami, K.; Okubo, H.; Takahashi, Y.; Shibata, S.; Yamada, K.; Sato, K. The midpoint of sleep is associated with dietary intake and dietary behavior among young Japanese women. Sleep Med. 2011, 12, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Froy, O. The relationship between nutrition and circadian rhythms in mammals. Front. Neuroendocrinol. 2007, 28, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Imaki, M.; Hatanaka, Y.; Ogawa, Y.; Yoshida, Y.; Tanada, S. An Epidemiological Study on Relationship between the Hours of Sleep and Life Style Factors in Japanese Factory Workers. J. Physiol. Anthropol. Appl. Human Sci. 2002, 21, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Toktaş, N.; Erman, K.A.; Mert, Z. Nutritional Habits According to Human Chronotype and Nutritional Status of Morningness and Eveningness. J. Educ. Train. Stud. 2018, 6, 61. [Google Scholar] [CrossRef]
- Sato-Mito, N.; Shibata, S.; Sasaki, S.; Sato, K. Dietary intake is associated with human chronotype as assessed by both morningnesseveningness score and preferred midpoint of sleep in young Japanese women. Int. J. Food Sci. Nutr. 2011, 62, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Kanerva, N.; Kronholm, E.; Partonen, T.; Ovaskainen, M.L.; Kaartinen, N.E.; Konttinen, H.; Broms, U.; Männistö, S. Tendency toward eveningness is associated with unhealthy dietary habits. Chronobiol. Int. 2012, 29, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Health Ministry. Primary Care Information and Management System (e-Gestor). Available online: https://egestorab.saude.gov.br/paginas/acessoPublico/relatorios/relatoriosPublicos.xhtml (accessed on 12 March 2021).
- Alves, C.G.; de Morais Neto, O.L. Trends in premature mortality due to chronic non-communicable diseases in Brazilian federal units. Cienc. Saude Colet. 2015, 20, 641–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Brasil. Health Ministry. NASF Guidelines: Family Health Support Center. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_do_nasf_nucleo.pdf (accessed on 12 March 2021).



{kind=link}
{kind=link}
| Chronotype | Morning (n = 252) | Intermediate (n = 119) | Evening (n = 13) | |
|---|---|---|---|---|
| Clinical and sociobehavioral aspects | ||||
| Age (years) * | mean (SD) | 53.5 (0.7) | 46.5 (1.2) | 42.4 (2.7) |
| BMI (Kg/m2) | mean (SD) | 29.0 (0.4) | 29.3 (0.6) | 31.4 (2.5) |
| Sex (female) | % | 77 | 83 | 85 |
| Schooling * (>8 years) | % | 49 | 66 | 62 |
| Income (>2 min wage) | % | 36 | 36 | 9 |
| Physical activity (>3x a week) | % | 36.5 | 24 | 38.5 |
| Smoking habit (yes) | % | 21 | 21 | 31 |
| Alcohol consumption (≥2 times/week) | % | 10 | 12 | 15 |
| Chronic diseases | ||||
| Diabetes mellitus (yes) | % | 32 | 24 | 31 |
| Hypertension (yes) | % | 54 | 52 | 31 |
| Hypercholesterolemia (yes) | % | 26 | 22 | 7 |
| Hypertriglyceridemia (yes) | % | 2 | 2.5 | 0 |
| Hypothyroidism (yes) | % | 5 | 9 | 0 |
| Liver steatosis (yes) | % | 1 | 2.5 | 8 |
| Heart diseases (yes) * | % | 7.5 | 1 | 15 |
| Kidney disease (yes) | % | 0.5 | 1 | 0 |
| Circulatory system disease (yes) | % | 0.5 | 0 | 0 |
| Depression (yes) | % | 6 | 2.5 | 15 |
| Nutritional aspects | ||||
| Total energy intake (Kcal) | mean (SD) | 1522.3 (27.8) | 1633.6 (42.4) | 1649.0 (91.5) |
| Protein intake (g) | mean (SD) | 62.3 (1.3) | 66.8 (1.9) | 63.9 (3.9) |
| Lipid intake (g) | mean (SD) | 42.0 (1.0) | 46.1 (1.4) | 42.1 (3.6) |
| Carbohydrate intake (g) | mean (SD) | 222.9 (4.1) | 235.4 (6.7) | 248.2 (16.3) |
| Component | |||
|---|---|---|---|
| 1 | 2 | 3 | |
| omega-6 | 0.784 | ||
| omega-3 | 0.690 | 0.356 | |
| fiber | 0.334 | 0.833 | |
| calcium | 0.883 | ||
| magnesium | 0.722 | ||
| manganese | 0.319 | 0.765 | |
| phosphorus | 0.343 | 0.632 | |
| iron | 0.580 | 0.599 | |
| sodium | 0.720 | ||
| potassium | 0.656 | 0.361 | |
| copper | 0.732 | ||
| zinc | 0.631 | ||
| retinol | 0.900 | ||
| thiamine | 0.577 | ||
| riboflavin | 0.829 | ||
| pyridoxine | 0.719 | ||
| niacin | 0.716 | ||
| vitamin C | −0.389 | 0.718 | |
| Dependent Variable | Independent Variables | B | CI (95%) | t | Sig | F | Adj R2 | Durbin–Watson |
|---|---|---|---|---|---|---|---|---|
| constant | 59.73 | 50.42–69.04 | 12.62 | <0.0001 | 8.471 | 0.138 | 1.959 | |
| CT scores | age | 0.20 | 0.12–0.27 | 5.01 | <0.0001 | |||
| omega-6 | −1001.14 | −1944.95–−57.33 | −2.09 | 0.038 | ||||
| fiber | −431.96 | −743.55–−120.37 | −2.73 | 0.007 | ||||
| magnesium | 69.85 | 25.99–113.71 | 3.13 | 0.002 | ||||
| sodium | 6.37 | 0.82–11.92 | 2.26 | 0.025 | ||||
| zinc | −1337.11 | −2397.76–−276.47 | −2.48 | 0.014 | ||||
| retinol | −25.93 | −42.51–−9.35 | −3.08 | 0.002 | ||||
| pyridoxine | −8509.37 | −14,441.69–−2577.06 | −2.82 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reis-Canaan, J.C.; Canaan, M.M.; Costa, P.D.; Rodrigues-Juliatte, T.P.; Pereira, M.C.A.; Castelo, P.M.; Pardi, V.; M. Murata, R.; Pereira, L.J. Association between Chronotype and Nutritional, Clinical and Sociobehavioral Characteristics of Adults Assisted by a Public Health Care System in Brazil. Nutrients 2021, 13, 2260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072260
Reis-Canaan JC, Canaan MM, Costa PD, Rodrigues-Juliatte TP, Pereira MCA, Castelo PM, Pardi V, M. Murata R, Pereira LJ. Association between Chronotype and Nutritional, Clinical and Sociobehavioral Characteristics of Adults Assisted by a Public Health Care System in Brazil. Nutrients. 2021; 13(7):2260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072260
Chicago/Turabian StyleReis-Canaan, Juliana C., Marcelo M. Canaan, Patrícia D. Costa, Tamires P. Rodrigues-Juliatte, Michel C. A. Pereira, Paula M. Castelo, Vanessa Pardi, Ramiro M. Murata, and Luciano J. Pereira. 2021. "Association between Chronotype and Nutritional, Clinical and Sociobehavioral Characteristics of Adults Assisted by a Public Health Care System in Brazil" Nutrients 13, no. 7: 2260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072260