
Southwest Harvest for Health: An Adapted Mentored Vegetable Gardening Intervention for Cancer Survivors

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Harvest for Health Gardening Intervention
2.3. Primary Outcomes and Measures: Feasibility and Acceptability
2.4. Secondary Outcomes and Measures: Health and Lifestyle Outcomes
2.5. Other Outcomes and Measures
2.6. Data Analysis
3. Results
3.1. Feasibility
3.2. Adherence
3.3. Acceptability
3.4. Secondary Outcomes
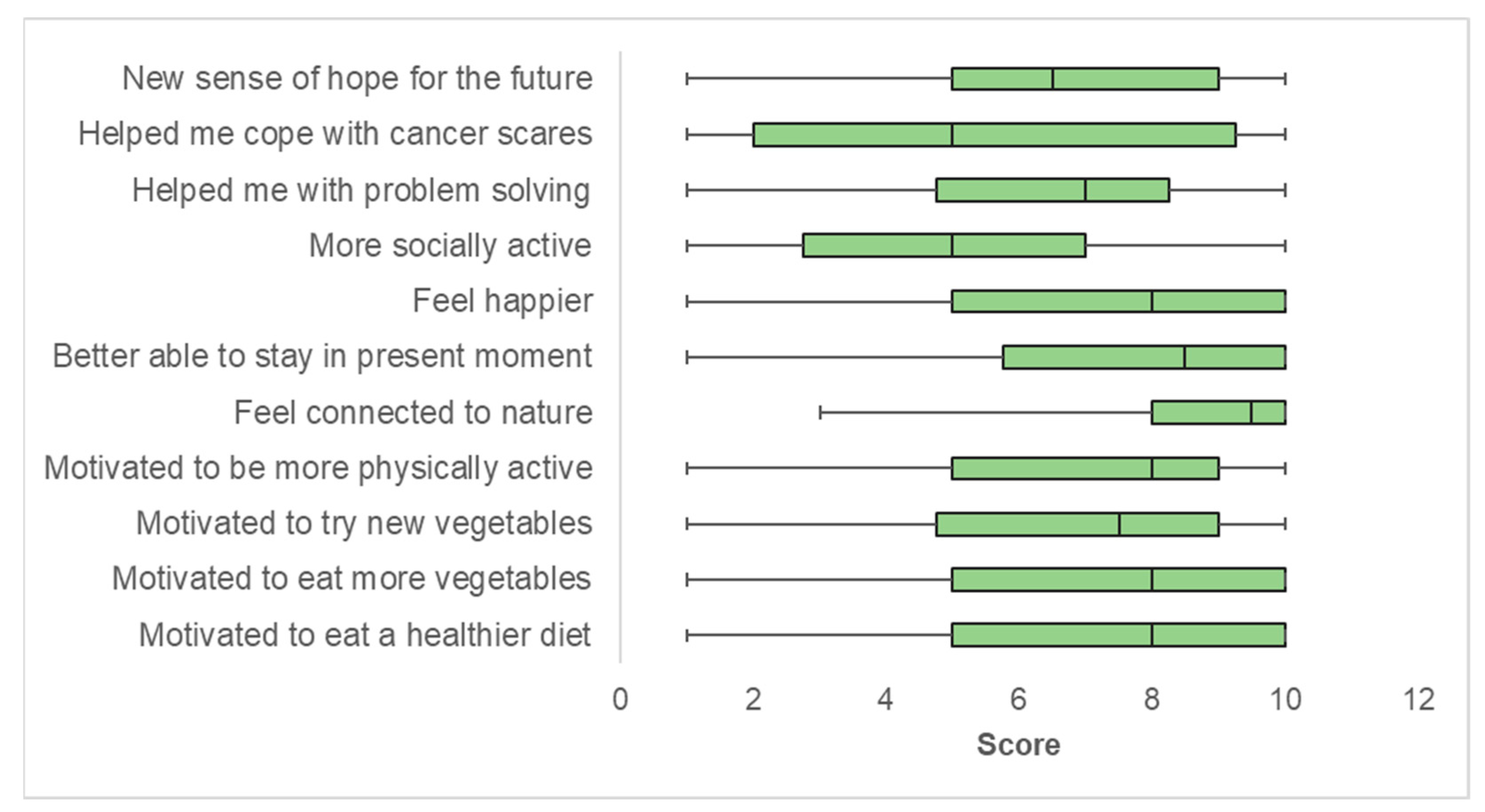
3.5. Other Outcomes
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Avis, N.E.; Deimling, G.T. Cancer survivorship and aging. Cancer 2008, 113, 3519–3529. [Google Scholar] [CrossRef]
- Hewitt, M.; Rowland, J.H.; Yancik, R. Cancer survivors in the United States: Age, health, and disability. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Morgans, A.K.; Fan, K.H.; Koyama, T.; Albertsen, P.C.; Goodman, M.; Hamilton, A.S.; Hoffman, R.M.; Stanford, J.L.; Stroup, A.M.; Resnick, M.J.; et al. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J. Urol. 2015, 193, 1226–1231. [Google Scholar] [CrossRef]
- Singh, S.; Earle, C.C.; Bae, S.J.; Fischer, H.D.; Yun, L.; Austin, P.C.; Rochon, P.A.; Anderson, G.M.; Lipscombe, L. Incidence of Diabetes in Colorectal Cancer Survivors. J. Natl. Cancer Inst. 2016, 108, djv402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armenian, S.H.; Xu, L.; Ky, B.; Sun, C.; Farol, L.T.; Pal, S.K.; Douglas, P.S.; Bhatia, S.; Chao, C. Cardiovascular Disease Among Survivors of Adult-Onset Cancer: A Community-Based Retrospective Cohort Study. J. Clin. Oncol. 2016, 34, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.E.; Stanway, S.; Lyon, A.R.; Dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: A population-based cohort study using multiple linked UK electronic health records databases. Lancet 2019, 394, 1041–1054. [Google Scholar] [CrossRef] [Green Version]
- Schoormans, D.; Vissers, P.A.J.; van Herk-Sukel, M.P.P.; Denollet, J.; Pedersen, S.S.; Dalton, S.O.; Rottmann, N.; van de Poll-Franse, L. Incidence of cardiovascular disease up to 13 year after cancer diagnosis: A matched cohort study among 32,757 cancer survivors. Cancer Med. 2018, 7, 4952–4963. [Google Scholar] [CrossRef]
- Overholser, L.S.; Callaway, C. Preventive Health in Cancer Survivors: What Should We Be Recommending? J. Natl. Compr. Cancer Netw. 2018, 16, 1251–1258. [Google Scholar] [CrossRef]
- Denlinger, C.S.; Ligibel, J.A.; Are, M.; Baker, K.S.; Demark-Wahnefried, W.; Dizon, D.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A.; et al. Survivorship: Healthy lifestyles, version 2.2014. J. Natl. Compr. Cancer Netw. 2014, 12, 1222–1237. [Google Scholar] [CrossRef] [Green Version]
- Cancer.Net. What Is Survivorship? Available online: https://www.cancer.net/survivorship/what-survivorship#:~:text=A%20person%20who%20has%20had,reasons%20for%20this%20may%20vary (accessed on 3 July 2021).
- Jacob, M.E.; Yee, L.M.; Diehr, P.H.; Arnold, A.M.; Thielke, S.M.; Chaves, P.H.; Gobbo, L.D.; Hirsch, C.; Siscovick, D.; Newman, A.B. Can a Healthy Lifestyle Compress the Disabled Period in Older Adults? J. Am. Geriatr. Soc. 2016, 64, 1952–1961. [Google Scholar] [CrossRef]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of Healthy Lifestyle Factors on Life Expectancies in the US Population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Patel, A.V.; Kushi, L.H.; Patel, R.; Willett, W.C.; Doyle, C.; Thun, M.J.; Gapstur, S.M. Following cancer prevention guidelines reduces risk of cancer, cardiovascular disease, and all-cause mortality. Cancer Epidemiol. Biomarkers Prev. 2011, 20, 1089–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C.; Lancet Physical Activity Series Working, G. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Morey, M.C.; Snyder, D.C.; Sloane, R.; Cohen, H.J.; Peterson, B.; Hartman, T.J.; Miller, P.; Mitchell, D.C.; Demark-Wahnefried, W. Effects of home-based diet and exercise on functional outcomes among older, overweight long-term cancer survivors: RENEW: A randomized controlled trial. JAMA 2009, 301, 1883–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demark-Wahnefried, W.; Rogers, L.Q.; Alfano, C.M.; Thomson, C.A.; Courneya, K.S.; Meyerhardt, J.A.; Stout, N.L.; Kvale, E.; Ganzer, H.; Ligibel, J.A. Practical clinical interventions for diet, physical activity, and weight control in cancer survivors. CA Cancer J. Clin. 2015, 65, 167–189. [Google Scholar] [CrossRef]
- Basen-Engquist, K.; Alfano, C.M.; Maitin-Shepard, M.; Thomson, C.A.; Stein, K.; Syrjala, K.L.; Fallon, E.; Pinto, B.M.; Schmitz, K.H.; Zucker, D.S.; et al. Moving Research into Practice: Physical Activity, Nutrition, and Weight Management for Cancer Patients and Survivors. NAM Perspectives; Discussion Paper; National Academy of Medicine: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C.; Lancet Physical Activity Series 2 Executive, C. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef] [Green Version]
- USDA National Institute of Food and Agriculture: Cooperative Extension System. Available online: https://nifa.usda.gov/cooperative-extension-system (accessed on 3 July 2021).
- American Horticultural Society Master Gardeners. Available online: https://ahsgardening.org/gardening-resources/master-gardeners (accessed on 15 January 2019).
- USDA National Institute of Food and Agriculture: Horticulture Programs. Available online: https://nifa.usda.gov/program/horticulture-programs (accessed on 15 January 2019).
- Blair, C.K.; Madan-Swain, A.; Locher, J.L.; Desmond, R.A.; de Los Santos, J.; Affuso, O.; Glover, T.; Smith, K.; Carley, J.; Lipsitz, M.; et al. Harvest for health gardening intervention feasibility study in cancer survivors. Acta Oncol. 2013, 52, 1110–1118. [Google Scholar] [CrossRef] [Green Version]
- Bail, J.R.; Fruge, A.D.; Cases, M.G.; De Los Santos, J.F.; Locher, J.L.; Smith, K.P.; Cantor, A.B.; Cohen, H.J.; Demark-Wahnefried, W. A home-based mentored vegetable gardening intervention demonstrates feasibility and improvements in physical activity and performance among breast cancer survivors. Cancer 2018, 124, 3427–3435. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Cases, M.G.; Cantor, A.B.; Fruge, A.D.; Smith, K.P.; Locher, J.; Cohen, H.J.; Tsuruta, Y.; Daniel, M.; Kala, R.; et al. Pilot Randomized Controlled Trial of a Home Vegetable Gardening Intervention among Older Cancer Survivors Shows Feasibility, Satisfaction, and Promise in Improving Vegetable and Fruit Consumption, Reassurance of Worth, and the Trajectory of Central Adiposity. J. Acad. Nutr. Diet 2018, 118, 689–704. [Google Scholar] [CrossRef]
- Blair, C.K.; Harding, E.M.; Adsul, P.; Moran, S.; Guest, D.; Clough, K.; Sussman, A.L.; Duff, D.; Cook, L.S.; Rodman, J.; et al. Southwest Harvest for Health: Adapting a mentored vegetable gardening intervention for cancer survivors in the southwest. Contemp. Clin. Trials Commun. 2021, 21, 100741. [Google Scholar] [CrossRef] [PubMed]
- Cases, M.G.; Fruge, A.D.; De Los Santos, J.F.; Locher, J.L.; Cantor, A.B.; Smith, K.P.; Glover, T.A.; Cohen, H.J.; Daniel, M.; Morrow, C.D.; et al. Detailed methods of two home-based vegetable gardening intervention trials to improve diet, physical activity, and quality of life in two different populations of cancer survivors. Contemp. Clin. Trials 2016, 50, 201–212. [Google Scholar] [CrossRef] [Green Version]
- New Mexico State University College of Agricultural, Consumer, and Environmental Sciences: Cooperative Extension Service. Available online: https://extension.nmsu.edu/index.html (accessed on 3 July 2021).
- New Mexico State University Extension & Outreach. Available online: https://www.nmsu.edu/extension_and_outreach/ (accessed on 3 July 2021).
- New Mexico State University College of Agricultural, Consumer and Environmental Sciences (ACS): Extension Master Gardener Program. Available online: https://aces.nmsu.edu/ces/mastergardeners/about-us.html (accessed on 3 July 2021).
- National Cancer Institute. Fruit & vegetable screeners in the Eating at America’s Table Study (EATS). Available online: https://epi.grants.cancer.gov/diet/screeners/fruitveg/ (accessed on 7 May 2021).
- National Cancer Institute. Scoring the All-Day Screener. Available online: https://epi.grants.cancer.gov/diet/screeners/fruitveg/scoring/allday.html (accessed on 7 May 2021).
- Chastin, S.F.; Granat, M.H. Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2010, 31, 82–86. [Google Scholar] [CrossRef]
- Grant, P.M.; Ryan, C.G.; Tigbe, W.W.; Granat, M.H. The validation of a novel activity monitor in the measurement of posture and motion during everyday activities. Br. J. Sports Med. 2006, 40, 992–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozey-Keadle, S.; Libertine, A.; Lyden, K.; Staudenmayer, J.; Freedson, P.S. Validation of wearable monitors for assessing sedentary behavior. Med. Sci. Sports Exerc. 2011, 43, 1561–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellers, C.; Dall, P.; Grant, M.; Stansfield, B. Validity and reliability of the activPAL3 for measuring posture and stepping in adults and young people. Gait Posture 2016, 43, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Amireault, S.; Godin, G. The Godin-Shephard leisure-time physical activity questionnaire: Validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept. Mot. Skills 2015, 120, 604–622. [Google Scholar] [CrossRef]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. Validation of the Godin-Shephard Leisure-Time Physical Activity Questionnaire classification coding system using accelerometer assessment among breast cancer survivors. J. Cancer Surviv. 2015, 9, 532–540. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Norman, G.J.; Wagner, N.; Patrick, K.; Calfas, K.J.; Sallis, J.F. Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. J. Phys. Act. Health 2010, 7, 697–705. [Google Scholar] [CrossRef] [PubMed]
- PROMIS: Patient-Reported Outcomes Measurement Information System. Available online: http://www.healthmeasures.net/explore-measurement-systems/promis/intro-to-promis (accessed on 3 July 2021).
- Cella, D.; Choi, S.W.; Condon, D.M.; Schalet, B.; Hays, R.D.; Rothrock, N.E.; Yount, S.; Cook, K.F.; Gershon, R.C.; Amtmann, D.; et al. PROMIS((R)) Adult Health Profiles: Efficient Short-Form Measures of Seven Health Domains. Value Health 2019, 22, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Cook, K.F.; Jensen, S.E.; Schalet, B.D.; Beaumont, J.L.; Amtmann, D.; Czajkowski, S.; Dewalt, D.A.; Fries, J.F.; Pilkonis, P.A.; Reeve, B.B.; et al. PROMIS measures of pain, fatigue, negative affect, physical function, and social function demonstrate clinical validity across a range of chronic conditions. J. Clin. Epidemiol. 2016, 73, 89–102. [Google Scholar] [CrossRef] [Green Version]
- Schalet, B.D.; Hays, R.D.; Jensen, S.E.; Beaumont, J.L.; Fries, J.F.; Cella, D. Validity of PROMIS physical function measures in diverse clinical samples. J. Clin. Epidemiol. 2016, 73, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalet, B.D.; Pilkonis, P.A.; Yu, L.; Dodds, N.; Johnston, K.L.; Yount, S.; Riley, W.; Cella, D. Clinical validity of PROMIS Depression, Anxiety, and Anger across diverse clinical samples. J Clin Epidemiol. 2016, 73, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutrona, C.E.; Russell, D. The provisions of social relationships and adaptation stress. In Advances in Personal Relationships; Jones, W.H., Perlman, D., Eds.; JAI Press: Greenwich, CT, USA, 1987; Volume 1, pp. 37–67. [Google Scholar]
- Blair, C.K.; Harding, E.; Wiggins, C.; Kang, H.; Schwartz, M.; Tarnower, A.; Du, R.; Kinney, A.Y. A Home-Based Mobile Health Intervention to Replace Sedentary Time with Light Physical Activity in Older Cancer Survivors: Randomized Controlled Pilot Trial. JMIR Cancer 2021, 7, e18819. [Google Scholar] [CrossRef]
- Campbell, M.K.; McLerran, D.; Turner-McGrievy, G.; Feng, Z.; Havas, S.; Sorensen, G.; Buller, D.; Beresford, S.A.; Nebeling, L. Mediation of adult fruit and vegetable consumption in the National 5 A Day for Better Health community studies. Ann. Behav. Med. 2008, 35, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Grajek, M.; Dzialach, E.; Buczkowska, M.; Gorski, M.; Nowara, E. Feelings Related to the COVID-19 Pandemic Among Patients Treated in the Oncology Clinics (Poland). Front. Psychol. 2021, 12, 647196. [Google Scholar] [CrossRef]
- Cox, B.D.; Whichelow, M.J.; Prevost, A.T. Seasonal consumption of salad vegetables and fresh fruit in relation to the development of cardiovascular disease and cancer. Public Health Nutr. 2000, 3, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Locke, E.; Coronado, G.D.; Thompson, B.; Kuniyuki, A. Seasonal variation in fruit and vegetable consumption in a rural agricultural community. J. Am. Diet Assoc. 2009, 109, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepeda, M.; Koolhaas, C.M.; van Rooij, F.J.A.; Tiemeier, H.; Guxens, M.; Franco, O.H.; Schoufour, J.D. Seasonality of physical activity, sedentary behavior, and sleep in a middle-aged and elderly population: The Rotterdam study. Maturitas 2018, 110, 41–50. [Google Scholar] [CrossRef]
- Tucker, P.; Gilliland, J. The effect of season and weather on physical activity: A systematic review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef] [PubMed]
- Turrisi, T.B.; Bittel, K.M.; West, A.B.; Hojjatinia, S.; Hojjatinia, S.; Mama, S.K.; Lagoa, C.M.; Conroy, D.E. Seasons, weather, and device-measured movement behaviors: A scoping review from 2006 to 2020. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Median (IQR) or Frequency (%) |
|---|---|
| Age (range 50 to 83) | 68 (64, 72) |
| Sex | |
| Female | 21 (70%) |
| Male | 9 (30%) |
| Race-ethnicity | |
| Non-Hispanic White | 22 (73%) |
| Hispanic White | 6 (20%) |
| Other | 2 (7%) |
| Education | |
| No college degree | 13 (43%) |
| College degree | 17 (57% |
| Cancer type | |
| Breast | 11 (37%) |
| Prostate | 6 (20%) |
| Lung | 4 (13%) |
| Other a | 9 (30%) |
| Treatment received b | |
| Surgery | 23 (77%) |
| Radiation | 22 (73%) |
| Chemotherapy | 10 (33%) |
| Hormone therapy | 12 (40%) |
| Other | 2 (7%) |
| Years since cancer diagnosis (range 1 to 17) | 5 (2, 8) |
| Self-reported general health | |
| Excellent | 2 (7%) |
| Very good | 5 (17%) |
| Good | 18 (60%) |
| Fair | 5 (17%) |
| Poor | 0 (0%) |
| Number of comorbidities (range 0 to 8) | 3 (2, 4) |
| BMI (kg/m2) | 28.8 (24.4, 32.1) |
| Pre−Intervention (Pre-COVID−19) Median (IQR) | Mid-Intervention (during COVID-19) Median (IQR) | Post-Intervention (during COVID−19) Median (IQR) | Pre-Mid Median Difference (IQR) p-Value a | Pre-Post Median Difference (IQR) p-Value a | |
|---|---|---|---|---|---|
| Lifestyle Behaviors | |||||
| V and F (servings per day) | 3.8 (2.5, 6.3) | 5.5 (3.6, 7.2) | 5.3 (3.7, 6.3) | 0.9 (−0.3, 2.2) p = 0.006 | 1.2 (−0.4, 2.2) p = 0.03 |
| Physical activity a | |||||
| Self−Report (Minutes per day) | |||||
| Light intensity | 11.3 (2.1, 17.1) | 4.3 (0, 25.7) | 5.3 (0, 25.7) | −1.4 (−10, 4.3) p = 0.39 | −0.7 (−10, 6.3) p = 0.66 |
| Moderate intensity | 0 (0, 7.1) | 0 (0, 8.6) | 0 (0, 12.9) | 0 (0, 0) p = 0.28 | 0 (0, 2.9) p = 0.19 |
| Device−based Measures | |||||
| Steps per day | 6781 (5523, 8633) | 6403 (4796, 7854) | 5831 (4287, 8038) | −792 (−1631, 464) p = 0.02 | −478 (−1832, 312) p = 0.05 |
| Minutes per day: | |||||
| Standing | 256.4 (201.5, 286.0) | 248.1 (181.5, 324.1) | 250.3 (180.6, 314.8) | 0.5 (−26.8, 29.0) p = 0.82 | 5.8 (−44.3, 49.1) p = 0.49 |
| Light intensity | 39.6 (30.7, 51.2) | 38.3 (29.2, 48.8) | 37.3 (26.8, 47.6) | −0.1 (−5.8, 3.0) p−0.46 | −1.1 (−10.6, 3.4) p = 0.20 |
| Moderate intensity | 49.5 (38.5, 70.6) | 49.3 (36.9, 64.4) | 45.8 (30.4, 64.3) | −6.1 (−15.1, 4.0) p = 0.01 | −4.2 (−13.8, 3.7) p = 0.06 |
| Sedentary behavior | |||||
| Self-Report (Minutes per day) | 517.8 (379.2, 623.4) | 469.2 (355.8, 591.6) | 507.0 (379.2, 618.0) | −54.0 (−114.0, 6.0) p = 0.06 | 12.0 (−114.0, 90) p = 0.87 |
| Device-based Measure (Minutes per day) | 440.5 (361.4, 505.8) | 457.2 (366.9, 529.0) | 457.8 (405.2, 510.3) | 27.7 (−40.8, 51.1) p = 0.50 | 14.8 (−35.8, 54.6) p = 0.63 |
| HRQOL b | |||||
| Physical | |||||
| Physical function | 47.0 (42.9, 53.1) | 44.8 (33.9, 52.4) | 45.6 (39.3, 52.8) | −0.1 (−4.9, 2.0) p = 0.50 | 0.0 (−7.0, 4.3) p = 0.39 |
| Fatigue | 50.5 (45.6, 58.2) | 50.7 (46.9, 59.2) | 49.8 (43.0, 57.5) | 1.1 (−2.1, 3.7) p = 0.41 | −0.9 (−5.7, 1.5) p = 0.28 |
| Pain | 55.4 (40.7, 58.3) | 54.4 (50.3, 57.5) | 50.6 (40.7, 58.7) | 0.0 (−2.4, 0.3) p = 0.57 | 0.0 (−7.1, 0.5) p = 0.09 |
| Sleep disturbance | 50.4 (48.7, 53.2) | 51.3 (50.2, 53.5) | 52.0 (49.3, 52.9) | −0.7 (−2.3, 3.5) p = 0.76 | −0.4 (−1.7, 2.4) p = 0.92 |
| Sleep impairment | 49.1 (40.2, 56.6) | 50.8 (39.9, 55.5) | 48.8 (40.6, 52.9) | 0.7 (−2.1, 4.9) p = 0.46 | −0.2 (−6.0, 5.1) p = 0.71 |
| Mental | |||||
| Anxiety | 49.3 (37.1, 53.5) | 50.9 (37.1, 56.5) | 47.8 (38.3, 56.3) | (−1.2, 3.0) p = 0.41 | 0.0 (−3.6, 3.0) p = 0.85 |
| Depression | 47.2 (38.2, 54.2) | 44.5 (38.2, 53.4) | 49.9 (38.2, 54.2) | 0.0 (−1.5, 3.6) p = 0.50 | 0.0 (−1.7, 4.8) p = 0.32 |
| Social | |||||
| Satisfaction with social roles and activities c | 50.5 (45.3, 58.0) | 51.7 (42.7, 58.0) | 51.3 (46.6, 65.4) | −1.6 (−5.6, 6.0) p = 0.77 | 3.3 (−1.4, 10.9) p = 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blair, C.K.; Adsul, P.; Guest, D.D.; Sussman, A.L.; Cook, L.S.; Harding, E.M.; Rodman, J.; Duff, D.; Burgess, E.; Quezada, K.; et al. Southwest Harvest for Health: An Adapted Mentored Vegetable Gardening Intervention for Cancer Survivors. Nutrients 2021, 13, 2319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072319
Blair CK, Adsul P, Guest DD, Sussman AL, Cook LS, Harding EM, Rodman J, Duff D, Burgess E, Quezada K, et al. Southwest Harvest for Health: An Adapted Mentored Vegetable Gardening Intervention for Cancer Survivors. Nutrients. 2021; 13(7):2319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072319
Chicago/Turabian StyleBlair, Cindy K., Prajakta Adsul, Dolores D. Guest, Andrew L. Sussman, Linda S. Cook, Elizabeth M. Harding, Joseph Rodman, Dorothy Duff, Ellen Burgess, Karen Quezada, and et al. 2021. "Southwest Harvest for Health: An Adapted Mentored Vegetable Gardening Intervention for Cancer Survivors" Nutrients 13, no. 7: 2319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072319