
Vitamin D Supplementation and Cancer Mortality: Narrative Review of Observational Studies and Clinical Trials

 , , , , ,
, , , , ,  , , ,
, , ,
Abstract
:1. Introduction
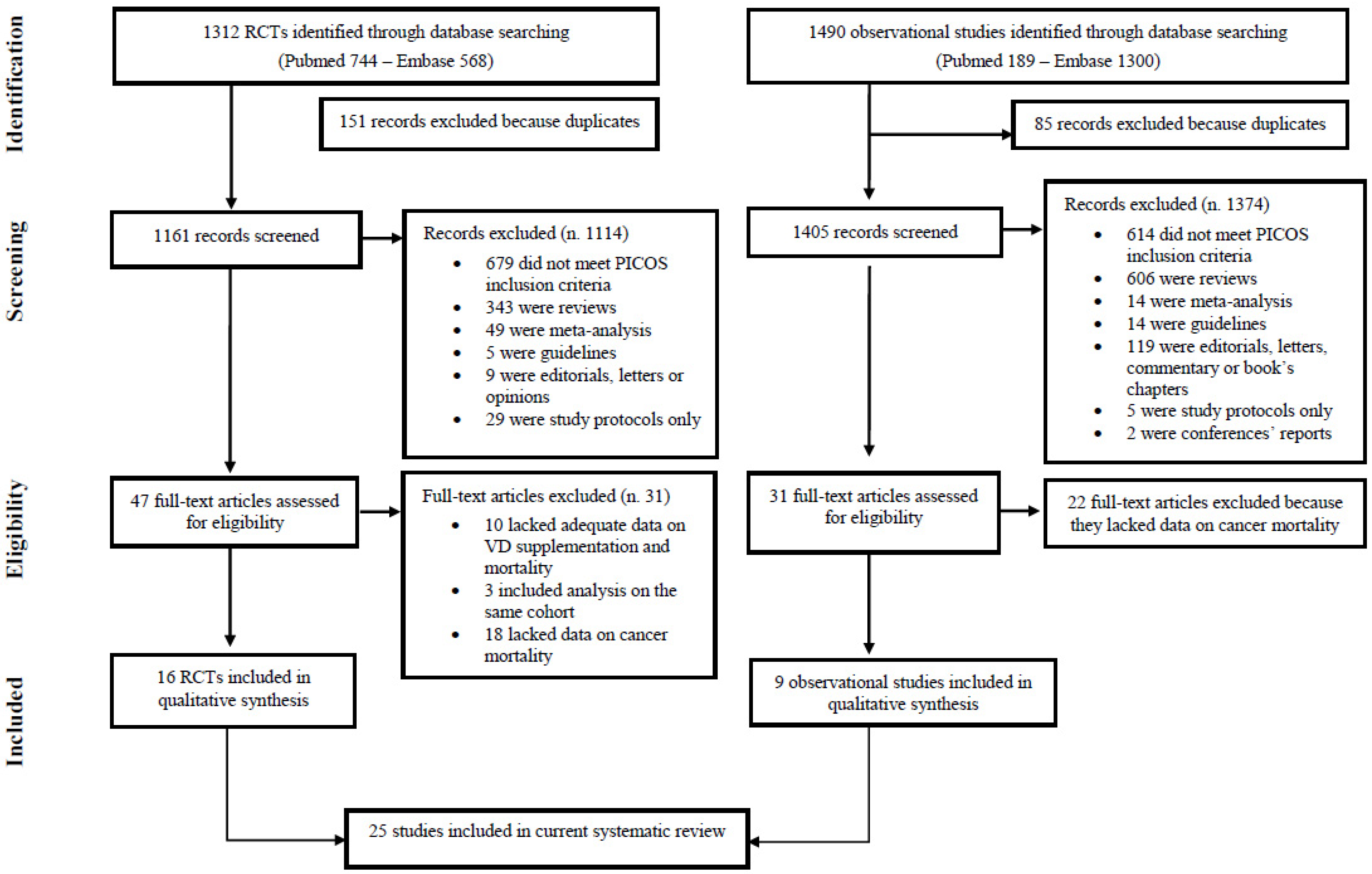
2. Materials and Methods
Data Extraction
3. Results
General Characteristics of Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, S.; Miller, D.; Li, W. Non-Musculoskeletal Benefits of Vitamin D beyond the Musculoskeletal System. Int. J. Mol. Sci. 2021, 22, 2128. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Vitamin, D. Sunlight and Cancer Connection. Anti-Cancer Agents Med. Chem. 2013, 13, 70–82. [Google Scholar] [CrossRef]
- Garland, C.F.; Garland, F.C.; Gorham, E.D.; Lipkin, M.; Newmark, H.; Mohr, S.B.; Holick, M.F. The role of vitamin D in cancer prevention. Am. J. Public Health 2006, 96, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Kunutsor, S.; Vitezova, A.; Oliver-Williams, C.; Chowdhury, S.; Jong, J.K.-D.; Khan, H.; Baena, C.P.; Prabhakaran, D.; Hoshen, M.B.; et al. Vitamin D and risk of cause specific death: Systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ 2014, 348, g1903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J. Vitamin D and Cardiovascular Disease. Annu. Rev. Med. 2016, 67, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.M. Vitamin D and cancer: Effects of 1,25(OH)2D3 and its analogs on growth control and tumorigenesis. Front. Biosci. 2001, 6, D820–D848. [Google Scholar] [CrossRef] [Green Version]
- Sluyter, J.D.; E Manson, J.; Scragg, R. Vitamin D and Clinical Cancer Outcomes: A Review of Meta-Analyses. JBMR Plus 2021, 5, e10420. [Google Scholar] [CrossRef]
- Manson, J.E.; Bassuk, S.S.; Lee, I.-M.; Cook, N.R.; Albert, M.A.; Gordon, D.; Zaharris, E.; MacFadyen, J.G.; Danielson, E.; Lin, J.; et al. The VITamin D and OmegA-3 TriaL (VITAL): Rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp. Clin. Trials 2012, 33, 159–171. [Google Scholar] [CrossRef] [Green Version]
- Avenell, A.; MacLennan, G.S.; Jenkinson, D.J.; McPherson, G.C.; McDonald, A.M.; Pant, P.R.; Grant, A.M.; Campbell, M.K.; Anderson, F.H.; Cooper, C.; et al. Long-Term Follow-Up for Mortality and Cancer in a Randomized Placebo-Controlled Trial of Vitamin D3and/or Calcium (RECORD Trial). J. Clin. Endocrinol. Metab. 2012, 97, 614–622. [Google Scholar] [CrossRef] [Green Version]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Scragg, R.; Khaw, K.-T.; Toop, L.; Sluyter, J.; Lawes, C.M.M.; Waayer, D.; Giovannucci, E.; Camargo, C.A. Monthly High-Dose Vitamin D Supplementation and Cancer Risk: A Post Hoc Analysis of the Vitamin D Assessment Randomized Clinical Trial. JAMA Oncol. 2018, 4, e182178. [Google Scholar] [CrossRef] [Green Version]
- Autier, P.; Gandini, S. Vitamin D supplementation and total mortality: A meta-analysis of randomized controlled trials. Arch. Intern. Med. 2007, 167, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.; Vale, C.; Haire, R.; Coyle, C.; Langley, R. Repurposing Vitamin D as an Anticancer Drug. Clin. Oncol. 2016, 28, 36–41. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.E.; Brennan, S.E.; Ryan, R.E.; Thomson, H.J.; Johnston, R.V.; Thomas, J. Chapter 3: Defining the criteria for including studies and how they will be grouped for the synthesis. In Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021. [Google Scholar] [CrossRef]
- Beer, T.M.; Ryan, C.W.; Venner, P.M.; Petrylak, D.P.; Chatta, G.S.; Ruether, J.D.; Redfern, C.H.; Fehrenbacher, L.; Saleh, M.N.; Waterhouse, D.M.; et al. Double-Blinded Randomized Study of High-Dose Calcitriol Plus Docetaxel Compared With Placebo Plus Docetaxel in Androgen-Independent Prostate Cancer: A Report From the ASCENT Investigators. J. Clin. Oncol. 2007, 25, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Attia, S.; Eickhoff, J.; Wilding, G.; McNeel, D.; Blank, J.; Ahuja, H.; Jumonville, A.; Eastman, M.; Shevrin, D.; Glode, M.; et al. Randomized, double-blinded phase II evaluation of docetaxel with or without doxercalciferol in patients with metastatic, androgen-independent prostate cancer. Clin. Cancer Res. 2008, 14, 2437–2443. [Google Scholar] [CrossRef] [Green Version]
- Scher, H.I.; Jia, X.; Chi, K.; De Wit, R.; Berry, W.R.; Albers, P.; Henick, B.; Waterhouse, D.; Ruether, D.J.; Rosen, P.J.; et al. Randomized, Open-Label Phase III Trial of Docetaxel Plus High-Dose Calcitriol Versus Docetaxel Plus Prednisone for Patients With Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2011, 29, 2191–2198. [Google Scholar] [CrossRef]
- Akiba, T.; Morikawa, T.; Odaka, M.; Nakada, T.; Kamiya, N.; Yamashita, M.; Yabe, M.; Inagaki, T.; Asano, H.; Mori, S.; et al. Vitamin D Supplementation and Survival of Patients with Non–small Cell Lung Cancer: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Cancer Res. 2018, 24, 4089–4097. [Google Scholar] [CrossRef] [Green Version]
- Golubić, Z.A.; Barsic, I.; Librenjak, N.; Plestina, S. Vitamin D Supplementation and Survival in Metastatic Colorectal Cancer. Nutr. Cancer 2018, 70, 413–417. [Google Scholar] [CrossRef]
- Ng, K.; Nimeiri, H.S.; McCleary, N.J.; Abrams, T.A.; Yurgelun, M.B.; Cleary, J.M.; Rubinson, D.A.; Schrag, D.; Miksad, R.; Bullock, A.J.; et al. Effect of High-Dose vs Standard-Dose Vitamin D3 Supplementation on Progression-Free Survival Among Patients With Advanced or Metastatic Colorectal Cancer: The SUNSHINE Randomized Clinical Trial. JAMA 2019, 321, 1370–1379. [Google Scholar] [CrossRef] [Green Version]
- Urashima, M.; Ohdaira, H.; Akutsu, T.; Okada, S.; Yoshida, M.; Kitajima, M.; Suzuki, Y. Effect of Vitamin D Supplementation on Relapse-Free Survival Among Patients With Digestive Tract Cancers: The AMATERASU Randomized Clinical Trial. JAMA 2019, 321, 1361–1369. [Google Scholar] [CrossRef]
- Yonaga, H.; Okada, S.; Akutsu, T.; Ohdaira, H.; Suzuki, Y.; Urashima, M. Effect Modification of Vitamin D Supplementation by Histopathological Characteristics on Survival of Patients with Digestive Tract Cancer: Post Hoc Analysis of the AMATERASU Randomized Clinical Trial. Nutrition 2019, 11, 2547. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, D.P.; Doll, R.; Khaw, K.T. Papers Effect of four monthly oral vitamin D 3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: Randomised double blind controlled trial. BMJ 2003, 326, 469. [Google Scholar] [CrossRef] [Green Version]
- Wactawski-Wende, J.; Kotchen, J.M.; Anderson, G.L.; Assaf, A.R.; Brunner, R.L.; O’Sullivan, M.J.; Margolis, K.; Ockene, J.K.; Phillips, L.; Pottern, L.; et al. Calcium plus Vitamin D Supplementation and the Risk of Colorectal Cancer. N. Engl. J. Med. 2006, 354, 684–696. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, R.T.; Johnson, K.C.; Kooperberg, C.; Pettinger, M.; Wactawski-Wende, J.; Rohan, T.; Rossouw, J.; Lane, D.; O’Sullivan, M.J.; Yasmeen, S.; et al. Calcium Plus Vitamin D Supplementation and the Risk of Breast Cancer. J. Natl. Cancer Inst. 2008, 100, 1581–1591. [Google Scholar] [CrossRef] [Green Version]
- Brunner, R.L.; Wactawski-Wende, J.; Caan, B.; Cochrane, B.B.; Chlebowski, R.T.; Gass, M.L.S.; Jacobs, E.T.; Lacroix, A.Z.; Lane, D.; Larson, J.; et al. The Effect of Calcium plus Vitamin D on Risk for Invasive Cancer: Results of the Women’s Health Initiative (WHI) Calcium Plus Vitamin D Randomized Clinical Trial. Nutr. Cancer 2011, 63, 827–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammann, E.M.; Drake, M.T.; Ms, B.H.; Wallace, R.B.; Johnson, K.C.; Desai, P.; Lin, E.M.; Link, B. Incidence of hematologic malignancy and cause-specific mortality in the Women’s Health Initiative randomized controlled trial of calcium and vitamin D supplementation. Cancer 2017, 123, 4168–4177. [Google Scholar] [CrossRef] [PubMed]
- Holm, M.; Olsen, A.; Kroman, N.; Tjønneland, A. Lifestyle influences on the association between pre-diagnostic hormone replacement therapy and breast cancer prognosis—Results from The Danish ‘Diet, Cancer and Health’ prospective cohort. Maturitas 2014, 79, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Yokosawa, E.B.; Arthur, A.E.; Mph, K.M.R.; Wolf, G.T.; Rozek, L.S.; Mondul, A.M. Vitamin D intake and survival and recurrence in head and neck cancer patients. Laryngoscope 2018, 128, E371–E376. [Google Scholar] [CrossRef]
- Zeichner, S.B.; Koru-Sengul, T.; Shah, N.; Liu, Q.; Markward, N.J.; Montero, A.J.; Glück, S.; Silva, O.; Ahn, E.R. Improved Clinical Outcomes Associated With Vitamin D Supplementation During Adjuvant Chemotherapy in Patients With HER2+ Nonmetastatic Breast Cancer. Clin. Breast Cancer 2015, 15, e1–e11. [Google Scholar] [CrossRef]
- Mulpur, B.H.; Nabors, L.B.; Thompson, R.C.; Olson, J.J.; LaRocca, R.V.; Thompson, Z.; Egan, K.M. Complementary therapy and survival in glioblastoma. Neuro-Oncol. Pract. 2015, 2, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, C.; Wang, J.; Huang, X.; Cheng, Y. Longitudinal, observational study on associations between postoperative nutritional vitamin D supplementation and clinical outcomes in esophageal cancer patients undergoing esophagectomy. Sci. Rep. 2016, 6, 38962. [Google Scholar] [CrossRef] [Green Version]
- Jeffreys, M.; Redaniel, M.T.; Martin, R.M. The effect of pre-diagnostic vitamin D supplementation on cancer survival in women: A cohort study within the UK Clinical Practice Research Datalink. BMC Cancer 2015, 15, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Madden, J.M.; Murphy, L.; Zgaga, L.; Bennett, K. De novo vitamin D supplement use post-diagnosis is associated with breast cancer survival. Breast Cancer Res. Treat. 2018, 172, 179–190. [Google Scholar] [CrossRef]
- Poole, E.M.; Shu, X.; Caan, B.; Flatt, S.W.; Holmes, M.D.; Lu, W.; Kwan, M.L.; Nechuta, S.; Pierce, J.P.; Chen, W.Y. Postdiagnosis supplement use and breast cancer prognosis in the After Breast Cancer Pooling Project. Breast Cancer Res. Treat. 2013, 139, 529–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, C.; Xun, P.; He, K. Vitamin D supplementation and quality of life following diagnosis in stage II colorectal cancer patients: A 24-month prospective study. Support. Care Cancer 2016, 24, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Sato, K.; Hollis, B.W.; Zhang, S.; Niedzwiecki, D.; Ou, F.-S.; Chang, I.-W.; O’Neil, B.H.; Innocenti, F.; Lenz, H.-J.; et al. Plasma 25-Hydroxyvitamin D Levels and Survival in Patients with Advanced or Metastatic Colorectal Cancer: Findings from CALGB/SWOG 80405 (Alliance). Clin. Cancer Res. 2019, 25, 7497–7505. [Google Scholar] [CrossRef] [Green Version]
- Kennel, K.A.; Drake, M.T. Vitamin D in the cancer patient. Curr. Opin. Support. Palliat. Care 2013, 7, 272–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkan, A.; Köksoy, E.B. Vitamin D deficiency in cancer patients and predictors for screening (D-ONC study). Curr. Probl. Cancer 2019, 43, 421–428. [Google Scholar] [CrossRef]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: Systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hyppönen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A sys-tematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Zhang, H.; Wu, H.; Li, H.; Liu, L.; Guo, J.; Li, C.; Shih, D.Q.; Zhang, X. Protective role of 1,25(OH)2vitamin D3 in the mucosal injury and epithelial barrier disruption in DSS-induced acute colitis in mice. BMC Gastroenterol. 2012, 12, 57. [Google Scholar] [CrossRef] [Green Version]
- Skrajnowska, D.; Bobrowska-Korczak, B. Potential Molecular Mechanisms of the Anti-cancer Activity of Vitamin D. Anticancer. Res. 2019, 39, 3353–3363. [Google Scholar] [CrossRef] [PubMed]
- Shan, N.L.; Wahler, J.; Lee, H.J.; Bak, M.J.; Das Gupta, S.; Maehr, H.; Suh, N. Vitamin D compounds inhibit cancer stem-like cells and induce differentiation in triple negative breast cancer. J. Steroid Biochem. Mol. Biol. 2017, 173, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Supnick, H.T.; Bunaciu, R.P.; Yen, A. The c-Raf modulator RRD-251 enhances nuclear c-Raf/GSK-3/VDR axis signaling and augments 1,25-dihydroxyvitamin D3-induced differentiation of HL-60 myeloblastic leukemia cells. Oncotarget 2018, 9, 9808–9824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Um, C.Y.; Fedirko, V.; Rutherford, R.E.; Seabrook, M.E.; Barry, E.L.; Baron, J.A.; Bostick, R.M. Effects of supplemental vitamin D and calcium on markers of proliferation, differentiation, and apoptosis in the normal colorectal mucosa of colorectal adenoma patients. PLoS ONE 2018, 13, e0208762. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Hendrix, S.L.; Langer, R.D.; Stefanick, M.L.; Gass, M.; Lane, D.; Rodabough, R.J.; Gilligan, M.A.; Cyr, M.G.; Thomson, C.A.; et al. Influence of Estrogen Plus Progestin on Breast Cancer and Mammography in Healthy Postmenopausal Women. JAMA 2003, 289, 3243–3253. [Google Scholar] [CrossRef] [Green Version]
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.A.; Bellerba, F.; Corso, F.; Gandini, S. Vitamin D Receptor Polymorphisms and Cancer. Adv. Exp. Med. Biol. 2020, 1268, 53–114. [Google Scholar] [CrossRef] [PubMed]
- Borella, E.; Nesher, G.; Israeli, E.; Shoenfeld, Y. Vitamin D: A new anti-infective agent? Ann. N. Y. Acad. Sci. 2014, 1317, 76–83. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; Goodall, E.C.; et al. Vitamin D supplementation to prevent acute respiratory infections: Individual participant data meta-analysis. Health Technol. Assess. 2019, 23, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus statement from 2nd International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| (a) Main Characteristics of RCTs in Cancer Patients | |||||||
|---|---|---|---|---|---|---|---|
| First Author, Publication Year, Study Name | Cancer Site | Country | Participants | Sex | Age | Inclusion Criteria | Primary and Secondary Outcomes |
| Beer, 2007 [15] ASCENT | Prostate | US | 250 | Males | Range 45–92 | Progressive metastatic androgen-independent prostate cancer—serum PSA 5.0 ng/mL, serum testosterone level 50 ng/dL, Eastern Cooperative Oncology Group performance status 2, life expectancy 3 months, age 18 yrs. | PSA reduction, OS, PSA, tumour, and clinical PFS, TRR measurable disease, skeletal morbidity-free survival, as well as safety and tolerability of the study treatment. |
| Attia, 2008 [16] | Prostate | US | 70 | Males | Range 52–85 | >18 yrs of age, histologic diagnosis of prostate adenocarcinoma, radiographic evidence of metastasis, chemotherapy naive | PSA reduction, PFS, OS, ORR and toxicity |
| Scher, 2011 [17] ASCENT | Prostate | US | 953 | Males | 70.9 VD and 70.4 control | Pathologically or cytologically proven adenocarcinoma of the prostate, metastatic disease and disease progression after medical or surgical castration (CRPC) | OS, thromboembolic event rates |
| Akiba, 2018 [18] | NSCLC | Japan | 155 | Males and females | 68 (SD 9) | NSCLC (stage IA to IIIA), aged 20 to 75 yrs at entry; diagnosed and operated at one of four Jikei University Hospitals; tumour totally resected; no major complications; followed-up for as long as possible | RFS, OS |
| Golubic, 2018 [19] | CRC metastatic | Croatia | 72 | Males and females | 69 (range 24–79) | CRC metastatic and 25(OH)D levels <75 nmol/L | OS, PFS |
| Ng, 2019 [20] SUNSHINE | CRC metastatic | US | 139 | Males and females | 56 (Range 47–65) | Pathologically confirmed, unresectable locally advanced or metastatic CRC, no prior treatment, no previous VD supplementation | PFS, ORR, OS and change in plasma 25(OH)D level |
| Urashima, 2019 [21] AMATERASU | Digestive tract | Japan | 417 | Males and females | 66 (Range 30–90) | Post-operative digestive tract cancer from the esophagus to the rectum, stages I to III, taking VD supplements or active VD; no history of urinary tract stones | RFS, OS, relapse, cancer-specific death, and no cancer death |
| Yonaga, 2019 [22] AMATERASU | Digestive tract | Japan | 400 | Males and females | Range 35–90 | Post-operative digestive tract cancer from the esophagus to the rectum, stages I to III, taking VD supplements; no history of urinary tract stones | RFS, OS, relapse, cancer-specific death, and no cancer death |
| (b) Main Characteristics of Population RCTs | |||||||
| First Author, Publication Year, Study Name | Health Status | Country | Participants | Sex | Age | Inclusion Criteria | Primary and Secondary Outcomes |
| Trivedi, 2003 [23] | General population | UK | 2686 | Males and females | VD group 74.8 (SD 4.6) and Placebo group 74.7 (SD 4.6) (range 65-85) | Fracture incidence | Fracture incidence and total mortality by cause. |
| Wactawski-Wende, 2006 [24] WHI | Postmenopausal women | US | 36,282 | Female | Range 50–79 | Postmenopausal women 50 to 79 yrs enrolled in the WHI randomized trials | Prevent hip fracture, CRC |
| Chlebowski, 2008 [25] WHI | Postmenopausal women | US | 36,282 | Female | Range 50–79 | Postmenopausal women 50 to 79 yrs enrolled in the WHI randomized trials | Hip fracture, breast and CRC |
| Brunner, 2011 [26] WHI | Postmenopausal women | US | 36,282 | Female | Range 50–79 | Postmenopausal women 50 to 79 yrs enrolled in the WHI randomized trials | Prevent other fractures, or CRC |
| Avenell, 2012 [9] RECORD | Elderly | UK | 5292 | Males and females | 77 (SD 6) | Fragility fracture within the last 10 yrs and aged at least 70 yrs | All-cause mortality, CVD mortality, cancer mortality, and cancer incidence |
| Ammann,2017 [27] WHI | Postmenopausal women | US | 34,763 | Female | Range 58-69 | Postmenopausal women 50 to 79 yrs enrolled in the WHI randomized trials | Hip fracture, breast and CRC |
| Scragg, 2018 [11] VIDA | Community adults | NZ | 5108 | Males and females | 65.9 (SD 8.3) (range 50–84) | 50 to 84 yrs; resident of Auckland, New Zealand, at the time of recruitment; and anticipated residence in New Zealand for the 4-yrs study period | Cancer incidence and cancer mortality (Primary aim: assess the effect of VD suppl. on incidence of CVD) |
| Manson, 2019 [10] VITAL | General population | US | 25,871 | Males and females | 67.1 (SD 7.1) | Men 50 yrs of age or older and women 55 yrs of age or older in the US | Cancer of any type and major CVE, site-specific cancers, cancer mortality, and additional CVE |
| (c) Main Characteristics of Observational Studies | |||||||
| First Author, Publication Year, Study Name | Health Status | Country | Participants | Sex | Age | Inclusion Criteria | Primary and Secondary Outcomes |
| Poole, 2013 [35] (ABCPP) | Breast | US and China | 12019 | Female | 58.0 (10.0) * | Breast cancer survivors, stage I–IV stage | BC recurrence, BC specific mortality, and all-cause mortality |
| Holm,2014 [28] (cohort study) | Breast | DK | 1064 | Female | 62 (range 50–64) | Breast cancer diagnosis | BC specific mortality |
| Zeichner, 2015 [30](retrospective study) | Breast | US | 246 | Female | >50 years (users 53.0 SD 12.1) | VD with trastuzumab-based chemotherapy for HER2-positive (HER2D) nonmetastatic breast cancer | DFS, OS |
| Jeffreys, 2015 [33] (cancer register) | Breast, CRC, lung, ovarian or uterine | UK | 21565 | Female | >55 years | First diagnosis of breast, colorectal, lung, ovarian or uterine cancer in postmenopausal women identified at least 5 years of CPRD data prior to diagnosis and 3+ to 1–2 (but no more) VD prescriptions | Cancer survival |
| Wang, 2016 [32] (Longitudinal study) | Esophageal | China | 303 | Males and females | non-users 64.9 (SD 7.6) users 61.7 (SD 7.6) | Esophageal cancer patients undergoing esophagectomy post-surgery | QoL and survival |
| Lewis, 2016 [36] (cancer register) | CRC | US | 453 | Males and females | 63.3 (SD 10.4) | Stage II CRC | VD supplementation and QoL |
| Mulpur, 2016 [31] (case-control) | Glioblastoma | US | 470 | Males and females | 59 (median) (range 18-89) | >18 age, recent diagnosis of primary (nonrecurrent) GBM and undergoing treatment at participating medical and oncology centers in the South Eastern US | Associations of CAM use and GBM outcome/mortality |
| Madden, 2018 [35] (cancer register) | Breast | Ireland | 5417 | Female | non-users 68 (59–74) users 66 (59–73) (range 50–80) | Aged 50-80 yrs, stage I-II breast cancer diagnosis and no VD use in yr prior to diagnosis | BC specific mortality |
| Yokosawa, 2018 [29] (cohort study) | HNC | US | 434 | Males and females | NR | HNC diagnosis, >18 yrs | Death from any cause, HNC-specific death and recurrence of disease. |
| (a) Details of RCTs in Cancer Patients (Statistically Significant Estimates Are in Bold) | ||||||||
|---|---|---|---|---|---|---|---|---|
| First Author, Publication Year, Study Name | Arms | Intervention Dose/Day | Comparator | Duration of Treatment/ Follow-Up | Cancer Deaths/ Treatment | Cancer Deaths/ Controls | Contrast | Estimates |
| Beer, 2007 [15] ASCENT | 2 | 45mcg DN-101 on day 1, 8 and 15 + therapy * | Placebo | Every 3 weeks/18.3 mths | NR | NR | VDS vs. placebo | OS HR = 0.67 (95% CI = 0.45–0.97) |
| Attia, 2008 [16] | 2 | 10 mcg Doxercalciferol Orally/days 1–28 ** | Placebo | Every 28 days/17.6 mths | 31 | 25 | VDS vs. placebo | OS Median 17.8 mths (95% CI = 14.9–23.6) vs. 16.4 mths (95% CI = 11.9-23.8) (P = 0.383) |
| Scher, 2011 [17] ASCENT | 2 | 45mcg DN-101 on day 1, 8 and 15 + therapy * | Placebo | Every 3 weeks/11.7 mths | 108 | 142 | VDS vs. placebo | OS Median 17.8 mths (95% CI = 16.0–19.5) vs. 20.2 mths (95% CI = 18.8–23.0) (log-rank P = 0.002). |
| Akiba, 2018 [18] | 2 | 1200 IU VD3/d | Placebo | 12 months/3.3 yrs | 40 | 24 | VDS vs. placebo | OS HR = 1.22 (95% CI = 0.54–2.79) |
| Golubic, 2018 [19] | 2 | 2000 IU/d + Standard chemotherapy | Placebo | 2 years/46 mths | NR | NR | VDS vs. placebo | OS HR = 1.01 (95% CI = 0.39–2.61) |
| Ng, 2019 [20] SUNSHINE | 2 | 8000 IU VD3/d followed by 4000 IU VD3/d *** | 400 IU/d Standard dose | 14 cycle/22.9 mths | 45 | 54 | High VDS vs. standard dose | OS Median 24.3 mths (95% CI = 19.0–33.2) vs. 24.3 mths (95% CI = 20.3–32.4) (log rank P = 0.43) OS HR = 0.64 (95% CI = 0–0.90) |
| Urashima, 2019 [21] AMATERASU | 2 | 2000 IU VD/d | Placebo | 3.5 yrs (median) | 27 | 16 | VDS vs. placebo | Cancer-specific death HR = 1.09 (95% CI = 0.58–2.01) |
| Yonaga, 2019 [22] AMATERASU | 2 | 2000 IU VD/d | Placebo | 3.5 years (median) | Well D AC: 19 Moderately D AC: 15 Poorly D AC: 3 Signet-ring CC: 1 SCC: 7 | Well D AC: 13 Moderately D AC: 9 Poorly D AC: 8 Signet-ring CC: 4 SCC: 3 | VDS vs. placebo | Well D AC OS HR = 0.82 (95%CI = 0.40–1.65) Moderately D AC OS HR = 1.31 (95%CI = 0.57–2.99) Poorly D AC OS HR = 0.25 (95%CI = 0.07–0.94) Signet-ring CC OS HR = 0.30 (95%CI = 0.03–2.65) SCC - OS HR = 1.39 (95%CI = 0.35–5.49) |
| (b) Details of Population RCTs (In Bold Statistical Significant Estimates) | ||||||||
| First Author, Publication Year, Study Name | Arms | Intervention Dose/Day | Comparator | Duration of Treatment/ Follow-Up | Cancer Deaths/ Treatment | Cancer Deaths/ Controls | Contrast | Estimates |
| Trivedi, 2003 [23] | 2 | 100 000 IU cholecalciferol | Placebo | Every 4 months for 5 yrs/5yrs | 63 | 72 | VDS vs. placebo | Cancer mortality RR = 0.86 (95% CI = 0.61–1.20) |
| Wactawski-Wende, 2006 [24] WHI | 2 | Calcium elemental 1000 mg + 400 IU VD3/d (two doses) | Placebo | 7.0 ± 1.4 yrs | 34 | 41 | VDS vs. no VDS | CRC mortality HR = 0.82 (95% CI = 0.52–1.29) |
| Chlebowski, 2008 [25] WHI | 2 | Calcium elemental 1000 mg + 400 IU VD3/d (two doses) | Placebo | 7 yrs | 23 | 23 | VDS vs. no VDS | Breast cancer mortality HR = 0.99 (95% CI = 0.55–1.76) |
| Brunner, 2011 [26] WHI | 2 | Calcium elemental 1000 mg + 400 IU VD3/d (two doses) | Placebo | 7.0 ± 1.4 yrs | 315 | 347 | VDS vs. no VDS | Cancer mortality HR = 0.90 (95% CI = 0.77–1.05) |
| Avenell, 2012 [9] RECORD | 4 | 800 IU VD3/day + 1000 mg Calcium/d | Placebo | 3 yrs/ 6.2 yrs (median) | 151 | 178 | VDS vs. no VDS | Cancer mortality HR = 0.85 (95% CI= 0.68–1.06) |
| Ammann,2017 [27] WHI | 2 | Calcium elemental 1000 mg + 400 IU VD3/d (two doses) | Placebo | 7 yrs | NR | NR | Calcium/VDS vs. placebo | Hematologic cancer-specific mortality HR = 0.77 (95% CI = 0.53–1.11) |
| Scragg, 2018 [11] VIDA | 2 | 200,000 IU VD3 (initial bolus) followed by 100 000 IU/mths | Placebo | 3 yrs/ 3.3 yrs (median) | 44 | 45 | NR | Cancer mortality HR = 0.97 (95% CI = 0.64–1.47) |
| Manson, 2019 [10] VITAL | 2 | 2000 IU VD3 + ω3 = 1 g/d | Placebo | 5 yrs/5.3 yrs (median) | 154 | 187 | NR | Cancer mortality HR = 0.83 (95% CI = 0.67–1.02) |
| (c) Details of Observational Studies in Cancer Patients (In Bold Statistical Significant Estimates) | ||||||||
| First Author, Publication Year, Study Name | Arms | Intervention Dose/Day | Comparator | Duration of Treatment/ Follow-Up | Cancer Deaths/ Treatment | Cancer Deaths/ Controls | Contrast | Estimates |
| Poole, 2013 [35] (ABCPP) | 2 | Regular VD use at least 1-yr post diagnosis | No VDS | 2.2 yrs (0.7) ^ | 41 | 808 | Users vs. non-users | BC mortality HR = 0.97 (95% CI = 0.68–1.38) |
| Holm,2014 [28] (cohort study) | 2 | VD use previous 12 months: low mcg (200 IU)/d); medium (5–10 mcg (400 IU)/d); high (>10 mcg (400 IU)/d). | No VDS | 6.3 yrs | 60 | 45 | for an increase in one category of the variable | BC mortality HR = 1.47 (95% CI = 1.07–2.00) |
| Zeichner, 2015 [30](retrospective study) | 2 | VD use during chemotherapy: <10,000 UI/week or >10,000 UI/week | No VD users | 29.5 mths | NR | NR | Users vs. non-users | OS HR = 0.31 (95% CI = 0.11–0.89) |
| Jeffreys, 2015 [33] (cancer register) | 2 | Any suppl 5 yrs prior to cancer diagnosis | No VDS | 30.4 mths | 314 | 1789 | Any vs. No suppl | BC survival HR = 0.78 (95% CI = 0.70–0.88) |
| 252 | 1474 | CRC survival HR = 0.90 (95% CI = 0.78–1.04) | ||||||
| 443 | 2313 | LC survival HR = 1.06 (95% CI = 0.96–1.17) | ||||||
| 134 | 1017 | GC survival HR = 0.89 (95% CI = 0.73–1.07) | ||||||
| ≥3 prescriptions 5 yrs prior to cancer diagnois | 1–2 prescriptions | 228 | 86 | ≥3 prescriptions vs. 1–2 prescriptions | BC survival HR = 1.02 (95% CI = 0.79–1.32) | |||
| 191 | 61 | CRC survival HR = 0.81 (95% CI = 0.59–1.11) | ||||||
| 323 | 120 | LC survival HR = 0.86 (95% CI = 0.70–1.07) | ||||||
| 98 | 36 | GC survival HR = 0.84 (95% CI = 0.59–1.30) | ||||||
| Wang, 2016 [32] (Longitudinal study) | 2 | Regular VD use after esophagectomy, during treatment and recovery phases: 200-400 IU/day | No VD users | 24-mths after surgery | NR | NR | Users vs. non-users | OS HR = 0.80 (95% CI = 0.51–1.24) |
| Lewis, 2016 [36] (cancer register) | 2 | Regular VD use 12 months prior to cancer diagnosis | No VD users | 24 months | NR | NR | Users vs. non-users | OS HR = 0.77 (95% CI = 0.37, 1.58) |
| Mulpur, 2016 [31] (case-control) | 2 | Regular VD use 5 yrs prior to cancer diagnosis | No VD users | 1.3 wks to 5.3 yrs | 373 | NR | Users vs. non-users | OS HR = 0.72 (95% CI = 0.52–0.99) |
| Madden, 2018 [35] (cancer register) | 2 | De novo VD use post diagnosis | No VD users | NR | 208 | 598 | Users vs. non-users Users (initiation < 180d) vs. non-users Users (initiation ≥ 180d) vs. non-users | BC survival HR = 0.80 (95% CI = 0.64–0.99) BC survival HR = 0.51 (95% CI = 0.34–0.74) BC survival HR = 0.91 (95% CI = 0.70–1.18) |
| Yokosawa, 2018 [29] (cohort study) | 3 | Past use of VD: 0; 0-400 UI/day; ≥400 UI/day | Level of VDS | NR | 32 | 28 | Use of ≥400 UI vs. 0 UI | HNC survival HR = 1.11 (95% CI = 0.65–1.90) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gnagnarella, P.; Muzio, V.; Caini, S.; Raimondi, S.; Martinoli, C.; Chiocca, S.; Miccolo, C.; Bossi, P.; Cortinovis, D.; Chiaradonna, F.; et al. Vitamin D Supplementation and Cancer Mortality: Narrative Review of Observational Studies and Clinical Trials. Nutrients 2021, 13, 3285. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093285
Gnagnarella P, Muzio V, Caini S, Raimondi S, Martinoli C, Chiocca S, Miccolo C, Bossi P, Cortinovis D, Chiaradonna F, et al. Vitamin D Supplementation and Cancer Mortality: Narrative Review of Observational Studies and Clinical Trials. Nutrients. 2021; 13(9):3285. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093285
Chicago/Turabian StyleGnagnarella, Patrizia, Valeria Muzio, Saverio Caini, Sara Raimondi, Chiara Martinoli, Susanna Chiocca, Claudia Miccolo, Paolo Bossi, Diego Cortinovis, Ferdinando Chiaradonna, and et al. 2021. "Vitamin D Supplementation and Cancer Mortality: Narrative Review of Observational Studies and Clinical Trials" Nutrients 13, no. 9: 3285. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093285