
Behaviour Change Techniques in Weight Gain Prevention Interventions in Adults of Reproductive Age: Meta-Analysis and Meta-Regression

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Data Sources and Searches
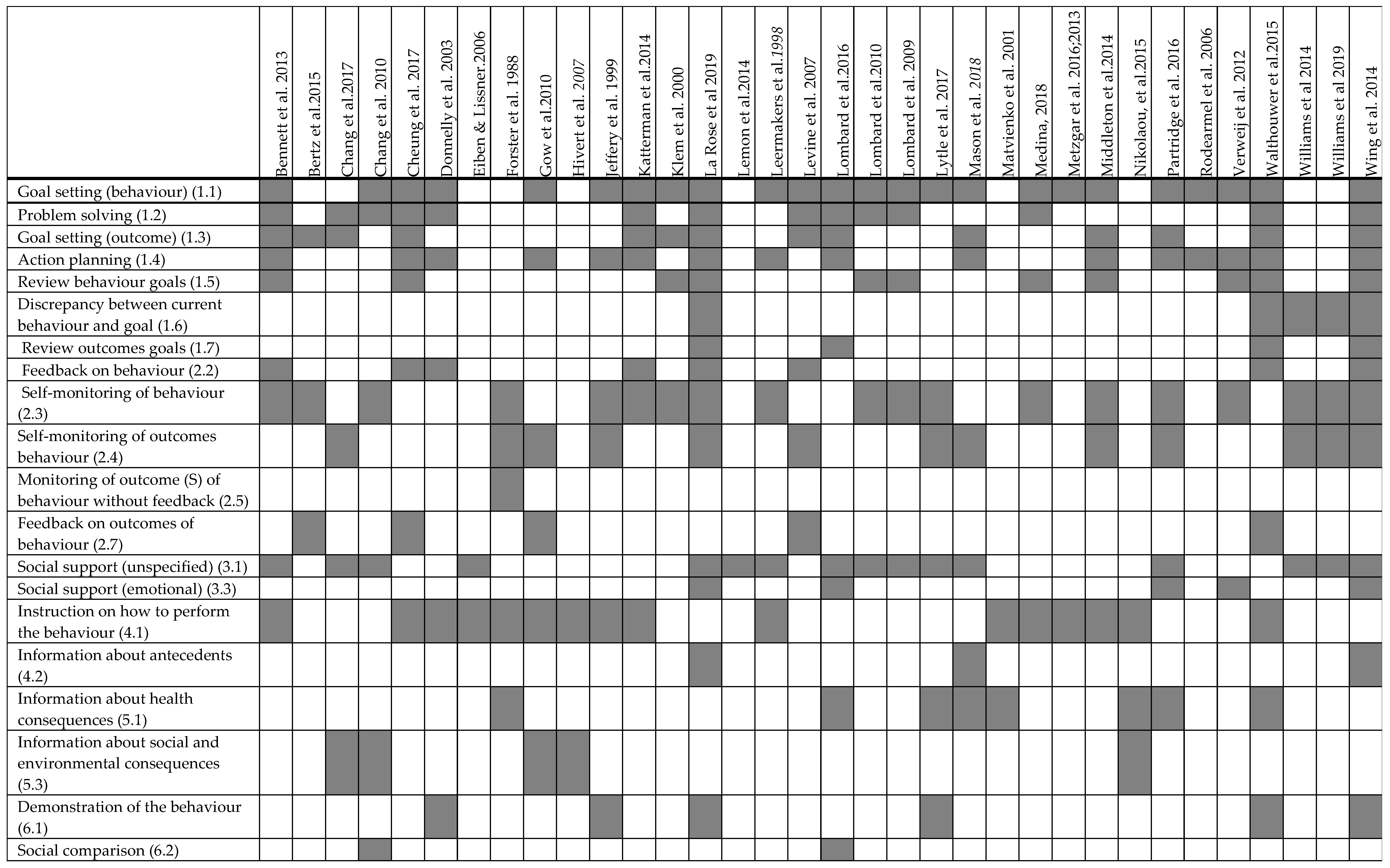
2.3. BCTs Coding
2.4. Data Synthesis and Analysis
2.5. Analysis of BCTs: Meta-Regression and Percentage Effectiveness Ratio
3. Results
3.1. Study Selection and Intervention Efficacy Overview
3.2. BCT Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Kimokoti, R.W.; Newby, P.; Gona, P.; Zhu, L.; McKeon-O’Malley, C.; Guzman, J.P.; D’Agostino, R.B.; Millen, B.E. Patterns of weight change and progression to overweight and obesity differ in men and women: Implications for research and interventions. Public Health Nutr. 2013, 16, 1463–1475. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, C.E.; Jacobs, D.R., Jr.; McCreath, H.; Kiefe, C.I.; Schreiner, P.J.; Smith, D.E.; Williams, O.D. Weight gain continues in the 1990s: 10-year trends in weight and overweight from the CARDIA study. Am. J. Epidemiol. 2000, 151, 1172–1181. [Google Scholar] [CrossRef]
- Brown, W.J.; Kabir, E.; Clark, B.K.; Gomersall, S.R. Maintaining a healthy BMI: Data from a 16-year study of young Australian women. Am. J. Prev. Med. 2016, 51, e165–e178. [Google Scholar] [CrossRef]
- Adamson, L.; Brown, W.; Byles, J.; Chojenta, C.; Dobson, A.; Fitzgerald, D.; Hockey, R.; Loxton, D.; Powers, J.; Spallek, M. Women’s Weight: Findings from the Australian Longitudinal Study on Women’s Health: Report Prepared for the Australian Government Department of Health and Ageing; Australian Government Department of Health and Ageing: Canberra, Australia, 2007.
- Gomersall, S.; Dobson, A.; Brown, W. Weight gain, overweight, and obesity: Determinants and health outcomes from the Australian Longitudinal Study on Women’s Health. Curr. Obes. Rep. 2014, 3, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truesdale, K.P.; Stevens, J.; Lewis, C.E.; Schreiner, P.J.; Loria, C.M.; Cai, J. Changes in risk factors for cardiovascular disease by baseline weight status in young adults who maintain or gain weight over 15 years: The CARDIA study. Int. J. Obes. 2006, 30, 1397–1407. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Manson, J.E.; Yuan, C.; Liang, M.H.; Grodstein, F.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA 2017, 318, 255–269. [Google Scholar] [CrossRef]
- Chen, C.; Ye, Y.; Zhang, Y.; Pan, X.-F.; Pan, A. Weight change across adulthood in relation to all cause and cause specific mortality: Prospective cohort study. BMJ 2019, 367, l5584. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.D.; Kahan, S. Maintenance of lost weight and long-term management of obesity. Med. Clin. 2018, 102, 183–197. [Google Scholar] [CrossRef]
- Nordmo, M.; Danielsen, Y.S.; Nordmo, M. The challenge of keeping it off, a descriptive systematic review of high-quality, follow-up studies of obesity treatments. Obes. Rev. 2020, 21, e12949. [Google Scholar] [CrossRef]
- Proietto, J. Why is treating obesity so difficult? Justification for the role of bariatric surgery. Med. J. Aust. 2011, 195, 144–146. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Martin, J.C.; Awoke, M.A.; Misso, M.L.; Moran, L.J.; Harrison, C.L. Preventing weight gain in adults: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13280. [Google Scholar] [CrossRef] [PubMed]
- Davidson, K.W.; Goldstein, M.; Kaplan, R.M.; Kaufmann, P.G.; Knatterud, G.L.; Orleans, C.T.; Spring, B.; Trudeau, K.J.; Whitlock, E.P. Evidence-based behavioral medicine: What is it and how do we achieve it? Ann. Behav. Med. 2003, 26, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Johnston, M.; MacLennan, G.; Araújo-Soares, V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychol. Rev. 2012, 6, 7–32. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Hill, B.; Pirotta, S.; O’Reilly, S.; Moran, L. What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 237. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690. [Google Scholar] [CrossRef] [Green Version]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Hill, B.; Skouteris, H.; Fuller-Tyszkiewicz, M. Interventions designed to limit gestational weight gain: A systematic review of theory and meta-analysis of intervention components. Obes. Rev. 2013, 14, 435–450. [Google Scholar] [CrossRef]
- Ashton, L.M.; Sharkey, T.; Whatnall, M.C.; Williams, R.L.; Bezzina, A.; Aguiar, E.J.; Collins, C.E.; Hutchesson, M.J. Effectiveness of interventions and behaviour change techniques for improving dietary intake in young adults: A systematic review and meta-analysis of RCTs. Nutrients 2019, 11, 825. [Google Scholar] [CrossRef] [Green Version]
- Ashton, L.M.; Sharkey, T.; Whatnall, M.C.; Haslam, R.L.; Bezzina, A.; Aguiar, E.J.; Collins, C.E.; Hutchesson, M.J. Which behaviour change techniques within interventions to prevent weight gain and/or initiate weight loss improve adiposity outcomes in young adults? A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2020, 21, e13009. [Google Scholar] [CrossRef]
- Martin, J.; Chater, A.; Lorencatto, F. Effective behaviour change techniques in the prevention and management of childhood obesity. Int. J. Obes. 2013, 37, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Brandt, J.S.; Cruz Ithier, M.A.; Rosen, T.; Ashkinadze, E. Advanced paternal age, infertility, and reproductive risks: A review of the literature. Prenat. Diagn. 2019, 39, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Mann, L.; Bateson, D.; Black, K.I. Teenage pregnancy. Aust. J. Gen. Pract. 2020, 49, 310–316. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Bull, E.R.; McCleary, N.; Li, X.; Dombrowski, S.U.; Dusseldorp, E.; Johnston, M. Interventions to promote healthy eating, physical activity and smoking in low-income groups: A systematic review with meta-analysis of behavior change techniques and delivery/context. Int. J. Behav. Med. 2018, 25, 605–616. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Sheals, K.; Godinho, C.A. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [Green Version]
- Willmott, T.J.; Pang, B.; Rundle-Thiele, S.; Badejo, A. Weight management in young adults: Systematic review of electronic health intervention components and outcomes. J. Med. Internet Res. 2019, 21, e10265. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; O’Reilly, S.; Behrens, H.; Skinner, T.; Ellis, I.; Dunbar, J.A. Effective strategies for weight loss in post-partum women: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 972–987. [Google Scholar] [CrossRef]
- Darling, K.E.; Sato, A.F. Systematic review and meta-analysis examining the effectiveness of mobile health technologies in using self-monitoring for pediatric weight management. Child. Obes. 2017, 13, 347–355. [Google Scholar] [CrossRef]
- Spring, B.; Champion, K.E.; Acabchuk, R.; Hennessy, E.A. Self-regulatory behaviour change techniques in interventions to promote healthy eating, physical activity, or weight loss: A meta-review. Health Psychol. Rev. 2020, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Hutchesson, M.J.; Rollo, M.E.; Krukowski, R.; Ells, L.; Harvey, J.; Morgan, P.J.; Callister, R.; Plotnikoff, R.; Collins, C.E. eH ealth interventions for the prevention and treatment of overweight and obesity in adults: A systematic review with meta-analysis. Obes. Rev. 2015, 16, 376–392. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Stewart, R.A.H.; Benatar, J.R. Intensity and duration of lifestyle interventions for long-term weight loss and association with mortality: A meta-analysis of randomised trials. BMJ Open 2019, 9, e029966. [Google Scholar] [CrossRef] [Green Version]
- Hills, A.P.; Byrne, N.M.; Lindstrom, R.; Hill, J.O. ‘Small Changes’ to Diet and Physical Activity Behaviors for Weight Management. Obes. Facts 2013, 6, 228–238. [Google Scholar] [CrossRef]
- Hall, K.D. What is the required energy deficit per unit weight loss? Int. J. Obes. 2008, 32, 573–576. [Google Scholar] [CrossRef] [Green Version]
- Williams, S.L.; French, D.P. What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behaviour—And are they the same? Health Educ. Res. 2011, 26, 308–322. [Google Scholar] [CrossRef]
- Lombard, C.; Harrison, C.; Kozica, S.; Zoungas, S.; Ranasinha, S.; Teede, H. Preventing weight gain in women in rural communities: A cluster randomised controlled trial. PLoS Med. 2016, 13, e1001941. [Google Scholar] [CrossRef]
- Foster-Schubert, K.E.; Alfano, C.M.; Duggan, C.R.; Xiao, L.; Campbell, K.L.; Kong, A.; Bain, C.E.; Wang, C.Y.; Blackburn, G.L.; McTiernan, A. Effect of diet and exercise, alone or combined, on weight and body composition in overweight-to-obese postmenopausal women. Obesity 2012, 20, 1628–1638. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Lara, J.; Evans, E.H.; O’Brien, N.; Moynihan, P.J.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Sniehotta, F.F.; White, M.; Mathers, J.C. Association of behaviour change techniques with effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014, 12, 177. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.M.; Taylor, W.; Lavender, T. Behaviour change techniques to change the postnatal eating and physical activity behaviours of women who are obese: A qualitative study. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Tate, D.F.; Lytle, L.; Polzien, K.; Diamond, M.; Leonard, K.R.; Jakicic, J.M.; Johnson, K.C.; Olson, C.M.; Patrick, K.; Svetkey, L.P. Deconstructing weight management interventions for young adults: Looking inside the black box of the EARLY consortium trials. Obesity 2019, 27, 1085–1098. [Google Scholar] [CrossRef]
- Dusseldorp, E.; Van Genugten, L.; van Buuren, S.; Verheijden, M.W.; van Empelen, P. Combinations of techniques that effectively change health behavior: Evidence from Meta-CART analysis. Health Psychol. 2014, 33, 1530. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Dusseldorp, E.; Meulman, J.J. Meta-CART: A tool to identify interactions between moderators in meta-analysis. Br. J. Math. Stat. Psychol. 2017, 70, 118–136. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Behaviour Change Strategies | Weight (n = 29) | Energy Intake (n = 13) | Physical Activity (n = 17) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β (95%CI) | p Value | Adj. R2 (%) | β (95%CI) | p Value | Adj. R2 (%) | β (95%CI) | p Value | Adj. R2 (%) | |
| Total BCT | −0.03 (−0.10, 0.05) | 0.475 | 0 | −3.99 (−10.5, 2.48) | 0.202 | 21.6 | −0.04 (−0. 08, 0.01 | 0.107 | 30.12 |
| Behaviour strategies consistent with control theory | 0.46 (−0.48, 1.40) | 0.323 | 0 | −20.4 (−230.5, 189.8) | 0.835 | 0 | −0.26 (−0.90, 0.39) | 0.413 | 0 |
| Goal setting (behaviour) (1.1) | −0.06 (−0.78, 0.66) | 0.867 | 0 | −20.4 (−230.5, 189.8) | 0.835 | 0 | −0.26 (−0.90, 0.39) | 0.413 | 0 |
| Problem solving (1.2) | −0.18 (−0.91, 0.54) | 0.604 | 0 | −62.2 (−163.9, 39.0) | 0.203 | 24.2 | −0.04 (−0.41, 0.33) | 0.817 | 0 |
| Goal setting (outcome) (1.3) | −0.29 (−0.96, 0.38) | 0.383 | 10.6 | −24.2 (−124.5, 76.0) | 0.605 | 0.11 | −0.11 (−0.48, 0.26) | 0.647 | 0 |
| Action planning (1.4) | −0.09 (−0.78, 0.60) | 0.795 | 0 | −18.9 (−132.1, 94.2) | 0.720 | 0 | −0.06 (−0.47, 0.35) | 0.763 | 0 |
| Review behaviour goals (1.5) | −0.65 (−1.34, 0.08) | 0.079 | 27.5 | −90.6 (−164.6, −16.7) | 0.021 | 52.6 | −0.15 (−0.52, 0.22) | 0.405 | 0 |
| Discrepancy between current behaviour and goal (1.6) | −0.68 (−1.69, 0.33) | 0.179 | 15.4 | −60.4 (−135.2, 14.4) | 0.103 | 43.4 | NA | NA | NA |
| Review outcomes goals (1.7) | −0.38 (−1.43, 0.67) | 0.462 | 5.33 | −24.3 (−119.6, 71.1) | 0.587 | 0 | NA | NA | NA |
| Feedback on behaviour (2.2) | −0.73 (−1.43, −0.03) | 0.042 | 40.1 | −61.7 (−136.6, 13.1) | 0.097 | 43.9 | −0.05 (−0.47, 0.37) | 0.798 | 0 |
| Self-monitoring of behaviour (2.3) | −0.54 (−1.19, 0.11) | 0.103 | 20.6 | −20.9 (−117.6, 75.6) | 0.642 | 0 | 0.22 (−0.11, 0.57) | 0.174 | 21.12 |
| Self-monitoring of outcomes of behaviour (2.4) | 0.76 (0.16, 1.14) | 0.015 | 29.7 | 6.3 (−91.4, 103.9) | 0.890 | 0 | 0.09 (−0.32, 0.51) | 0.644 | 0 |
| Feedback on outcomes of behaviour (2.7) | 0.61 (−0.18, 0.14) | 0.123 | 25.6 | NA | NA | NA | −0.36 (−0.74, 0.01) | 0.053 | 34.2 |
| Social support (unspecified) (3.1) | −0.32 (−1.02, 0.38) | 0.350 | 8.2 | 26.2 (−61.7, 114.1) | 0.525 | 0 | 0.17 (−0.21, 0.56) | 0.358 | 0 |
| Social support (emotional) (3.3 | −0.65 (−1.55, 0.26) | 0.156 | 21.1 | NA | NA | NA | −0.15 (−0.62, 0.32) | 0.503 | 0 |
| Instruction on how to perform the behaviour (4.1) | 0.08 (−0.61, 0.78) | 0.813 | 0 | −33.9 (−119.5, 51.8) | 0.403 | 0 | 0.04 (−0.35, 0.44) | 0.811 | 0 |
| Information about health consequences (5.1) | 0.15 (−0.67, 0.98) | 0.709 | 0 | −21.9 (−114.2, 70.5) | 0.623 | 0 | −0.31(−0.70, 0.09) | 0.117 | 20.4 |
| Information about social and environmental consequences (5.3) | 0.71 (0.05, 1.37) | 0.037 | 23.9 | NA | NA | NA | −0.04 (−0.56, 0.44) | 0.865 | 0 |
| Demonstration of the behaviour (6.1) | 0.00 (−0.87, 0.87) | 0.998 | 0 | −59.7 (−140.3, 20.9) | 0.131 | 43.3 | −0.07 (−0.52, 0.38) | 0.750 | 0 |
| Behaviour practice/rehearsal (8.1) | 0.13 (−0.74, 1.01) | 0.758 | 0 | −0.81 (−102.2, 100.6) | 0.986 | 0 | −0.01 (−0.69, 0.68) | 0.982 | 0 |
| Behaviour substitution (8.2) | −0.54 (−1.33, 0.25) | 0.171 | 22.0 | NA | NA | NA | NA | NA | NA |
| Graded tasks (8.7) | −0.82 (−1.46, −0.17) | 0.015 | 50.3 | NA | NA | NA | 0.45 (−0.04, 0.94) | 0.070 | 32.72 |
| Credible source (9.1) | −0.24 (−0.96, 0.49) | 0.510 | 0 | 52.7 (−50.5, 155.9) | 0.285 | 14.2 | 0.09 (−0.28, 0.46) | 0.611 | 0 |
| Reward (outcome) (10.10) | NA | NA | NA | −60.3 (−135.2, 14.6) | 0.104 | 43.4 | NA | NA | NA |
| Reduce negative emotions (11.2) | 0.35 (−0.53, 1.23) | 0.421 | 0 | NA | NA | NA | 0.03 (−0.47, 0.53) | 0.894 | 0 |
| Adding objects to the environment (12.5) | −0.46 (−1.15, 0.23) | 0.185 | 15.4 | NA | NA | NA | 0.05 (−0.38, 0.48) | 0.754 | 0 |
| Behaviour Change Strategies | Weight (n = 29) | Energy Intake (n = 13) | Physical Activity (n = 17) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Effective | Non- Effective | Percentage of Effectiveness | Effective | Non- Effective | Percentage of Effectiveness | Effective | Non- Effective | Percentage of Effectiveness | |
| Goal setting (behaviour) (1.1) | 11 | 8 | 57.9 | 4 | 6 | 40.0 | 3 | 12 | 20.0 |
| Problem solving (1.2) | 6 | 4 | 60.0 | 4 | 3 | 57.1 | 2 | 6 | 25.0 |
| Goal setting (outcome) (1.3) | 8 | 3 | 72.7 | 3 | 2 | 60.0 | 1 | 5 | 16.7 |
| Action planning (1.4 | 8 | 4 | 66.7 | 3 | 4 | 42.9 | 2 | 9 | 18.2 |
| Review behaviour goals (1.5) | 4 | 3 | 57.1 | 4 | 2 | 66.7 | 2 | 4 | 33.3 |
| Discrepancy between current behaviour and goal (1.6) | 3 | 0 | 100 | 2 | 1 | 66.7 | NA | NA | NA |
| Review outcomes goals (1.7) | NA | NA | NA | 2 | 1 | 66.7 | NA | NA | NA |
| Feedback on behaviour (2.2) | 4 | 1 | 80.0 | 3 | 1 | 75.0 | 1 | 3 | 25.0 |
| Self-monitoring of behaviour (2.3) | 12 | 5 | 70.6 | 2 | 3 | 40.0 | 2 | 7 | 22.2 |
| Self-monitoring of outcomes of behaviour (2.4) | 7 | 5 | 58.3 | 1 | 2 | 33.3 | 1 | 3 | 25.0 |
| Feedback on outcomes of behaviour (2.7) | 1 | 2 | 33.3 | NA | NA | NA | 0 | 3 | 0 |
| Social support (unspecified) (3.1) | 11 | 2 | 84.6 | 1 | 3 | 25.0 | 2 | 4 | 33.3 |
| Social support (emotional) (3.3) | 3 | 1 | 75.0 | NA | NA | NA | 1 | 3 | 25.0 |
| Instruction on how to perform the behaviour (4.1) | 8 | 6 | 57.1 | 4 | 6 | 40.0 | 3 | 9 | 25.0 |
| Information about health consequences (5.1) | 6 | 1 | 85.7 | 2 | 1 | 66.7 | 0 | 3 | 0 |
| Information about social and environmental consequences (5.3) | 2 | 3 | 40.0 | NA | NA | NA | 0 | 3 | 0 |
| Demonstration of the behaviour (6.1) | 3 | 1 | 75.0 | 2 | 2 | 50.0 | 1 | 2 | 33.3 |
| Behaviour practice/rehearsal (8.1) | 2 | 2 | 50.0 | 2 | 1 | 66.7 | NA | NA | NA |
| Behaviour substitution (8.2) | 4 | 1 | 80.0 | NA | NA | NA | NA | NA | NA |
| Graded tasks (8.7) | 5 | 0 | 100 | NA | NA | NA | 1 | 2 | 33.3 |
| Credible source (9.1) | 8 | 4 | 66.7 | 0 | 5 | 0 | 3 | 5 | 37.5 |
| Reward (outcome) (10.10) | NA | NA | NA | 3 | 0 | 100 | NA | NA | NA |
| Reduce negative emotions (11.2) | 2 | 5 | 28.6 | NA | NA | NA | 0 | 4 | 0 |
| Adding objects to the environment (12.5) | 4 | 2 | 66.7 | NA | NA | NA | 0 | 4 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awoke, M.A.; Harrison, C.L.; Martin, J.; Misso, M.L.; Lim, S.; Moran, L.J. Behaviour Change Techniques in Weight Gain Prevention Interventions in Adults of Reproductive Age: Meta-Analysis and Meta-Regression. Nutrients 2022, 14, 209. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010209
Awoke MA, Harrison CL, Martin J, Misso ML, Lim S, Moran LJ. Behaviour Change Techniques in Weight Gain Prevention Interventions in Adults of Reproductive Age: Meta-Analysis and Meta-Regression. Nutrients. 2022; 14(1):209. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010209
Chicago/Turabian StyleAwoke, Mamaru Ayenew, Cheryce L. Harrison, Julie Martin, Marie L. Misso, Siew Lim, and Lisa J. Moran. 2022. "Behaviour Change Techniques in Weight Gain Prevention Interventions in Adults of Reproductive Age: Meta-Analysis and Meta-Regression" Nutrients 14, no. 1: 209. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010209