
Metabolic Dysfunction-Associated Fatty Liver Disease Is Associated with the Risk of Incident Cardiovascular Disease: A Prospective Cohort Study in Xinjiang

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Biochemical Analysis
2.4. Questionnaire Survey
2.5. Key Definitions
2.6. Diagnosis of CVD
3. Statistical Analysis
4. Results
4.1. Baseline Characteristics
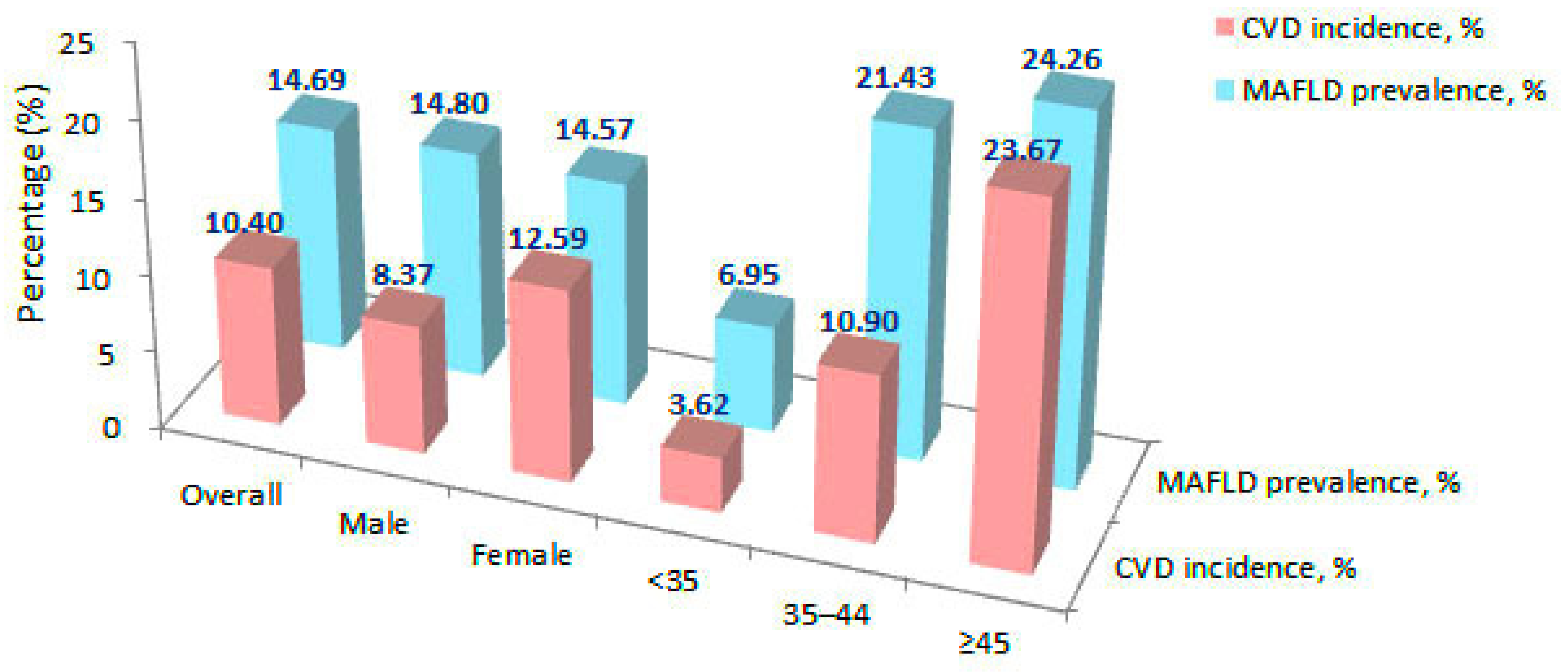
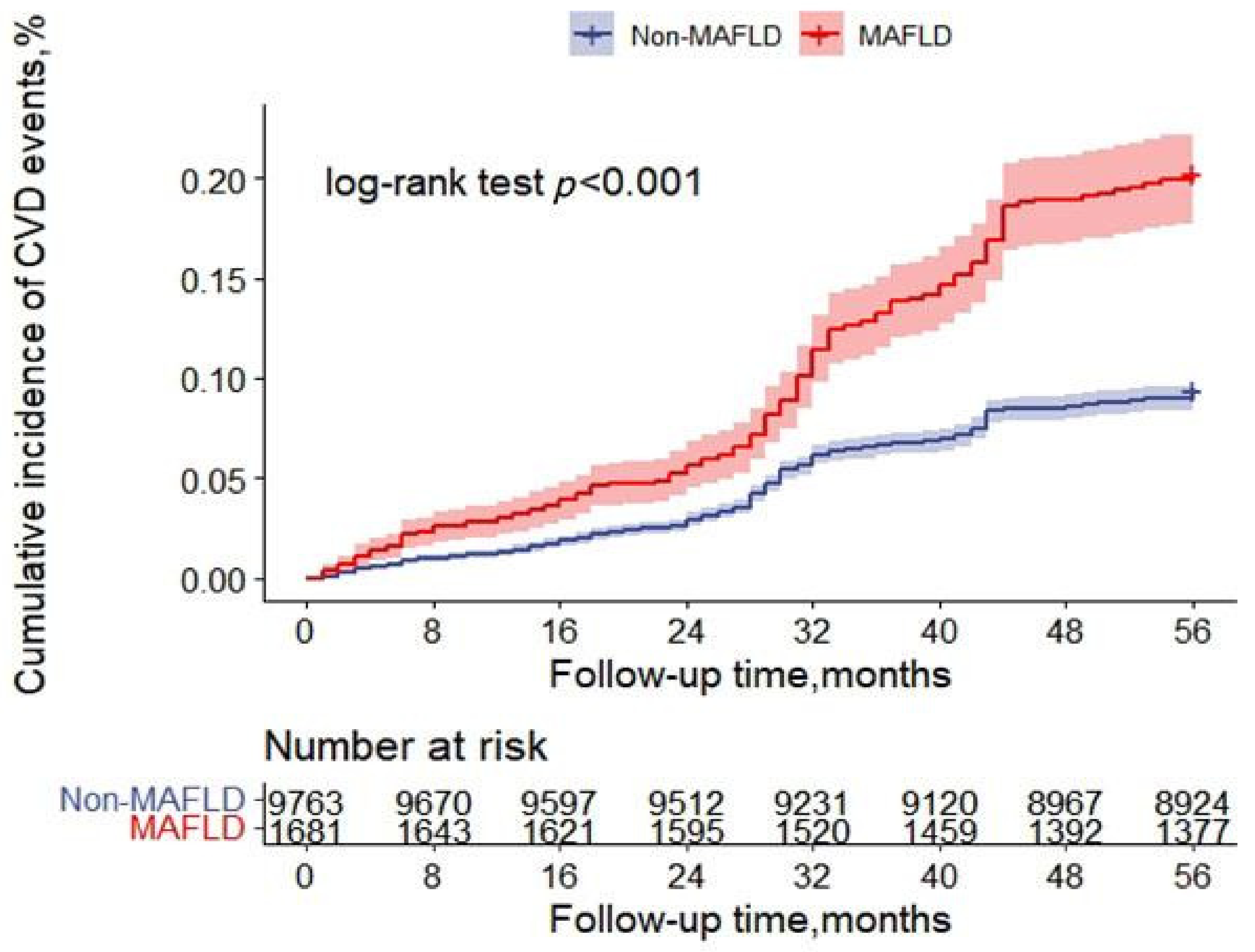
4.2. Incidence of CVD
4.3. CVD Univariate and Multivariate Analysis
4.4. Sensitivity Analysis
5. Discussion
6. Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: A Systematic Review and Meta-Analysis. Hepatology 2019, 70, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Pierantonelli, I.; Svegliati-Baroni, G. Nonalcoholic Fatty Liver Disease: Basic Pathogenetic Mechanisms in the Progression From NAFLD to NASH. Transplantation 2019, 103, e1–e13. [Google Scholar] [CrossRef]
- Lonardo, A.; Sookoian, S.; Pirola, C.J.; Targher, G. Non-alcoholic fatty liver disease and risk of cardiovascular disease. Metabolism 2016, 65, 1136–1150. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, N.; Bai, C.; Fang, Y.; Srishord, M.; McCullough, A.; Gramlich, T.; Younossi, Z.M. Long-term follow-up of patients with nonalcoholic fatty liver. Clin. Gastroenterol. Hepatol. 2009, 7, 234–238. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Lee, H.; Lee, Y.-H.; Kim, S.U.; Kim, H.C. Metabolic Dysfunction-Associated Fatty Liver Disease and Incident Cardiovascular Disease Risk: A Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2138–2147. [Google Scholar] [CrossRef]
- Yamamura, S.; Eslam, M.; Kawaguchi, T.; Tsutsumi, T.; Nakano, D.; Yoshinaga, S.; Takahashi, H.; Anzai, K.; George, J.; Torimura, T. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD. Liver Int. 2020, 40, 3018–3030. [Google Scholar] [CrossRef]
- Lim, S.; Kim, J.W.; Targher, G. Links between metabolic syndrome and metabolic dysfunction-associated fatty liver disease. Trends Endocrinol. Metab. 2021, 32, 500–514. [Google Scholar] [CrossRef]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020, 40, 2082–2089. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, H.; Liu, Y.; Hou, X.; Wei, L.; Bao, Y.; Yang, C.; Zong, G.; Wu, J.; Jia, W. Association of MAFLD with diabetes, chronic kidney disease, and cardiovascular disease: A 4.6-year cohort study in China. J. Clin. Endocrinol. Metab. 2022, 107, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.Q.; Wei, B.; Song, Y.P.; Guo, H.; Zhang, X.H.; Wang, X.P.; Yan, Y.Z.; Ma, J.L.; Wang, K.; Keerman, M.; et al. Metabolically healthy obesity and unhealthy normal weight rural adults in Xinjiang: Prevalence and the associated factors. BMC Public Health 2021, 21, 1940. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; He, Y.; Wang, Z.; Hu, Y. Status and characteristic of dietary intake of 12 minority nationalities in China. Wei Sheng Yan Jiu 2007, 36, 539–541. [Google Scholar]
- Ma, Y.C.; Zuo, L.; Chen, J.H.; Luo, Q.; Yu, X.Q.; Li, Y.; Xu, J.S.; Huang, S.M.; Wang, L.N.; Huang, W.; et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 2937–2944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Executive summary: Standards of medical care in diabetes—2012. Diabetes Care 2012, 35 (Suppl. 1), S4–S10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Writing Group of 2018 Chinese Guidelines for the Management of Hypertension. 2018 Chinese guidelines for the management of hypertension. Chin. J. Cardiovasc. Med. 2019, 24, 24–56. [Google Scholar]
- Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000; Volume 894, p. i-253.
- Guangdong Provincial Co-operation Group for Diabetes Epidemiological Study. Waist/height ratio: An effective index for abdominal obesity predicting diabetes and hypertension. Chin. J. Endocrinol. Metab. 2004, 20, 272–275. [Google Scholar]
- China Joint Committee on Revision of Guidelines for Prevention and Treatment of Dyslipidemia in Adults. Guidelines for the Prevention and Treatment of Dyslipidemia in Adults in China (Revised Edition in 2016). Chin. Circ. J. 2016, 31, 937–953. [Google Scholar]
- Azemati, B.; Kelishadi, R.; Ahadi, Z.; Shafiee, G.; Taheri, M.; Ziaodini, H.; Qorbani, M.; Heshmat, R. Association between junk food consumption and cardiometabolic risk factors in a national sample of Iranian children and adolescents population: The CASPIAN-V study. Eat. Weight Disord. 2020, 25, 329–335. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Cigarette smoking among adults—United States, 1992, and changes in definition of smoking. JAMA 1994, 272, 14–16. [Google Scholar] [CrossRef]
- Sun, K.; Ren, M.; Liu, D.; Wang, C.; Yang, C.; Yan, L. Alcohol consumption and risk of metabolic syndrome: A meta-analysis of prospective studies. Clin. Nutr. 2014, 33, 596–602. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Koehler, E.M.; Schouten, J.N.; Hansen, B.E.; Hofman, A.; Stricker, B.H.; Janssen, H.L. External validation of the fatty liver index for identifying nonalcoholic fatty liver disease in a population-based study. Clin. Gastroenterol. Hepatol. 2013, 11, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.L.; Wu, W.C.; Fang, K.C.; Wang, Y.C.; Huo, T.I.; Huang, Y.H.; Yang, H.I.; Su, C.W.; Lin, H.C.; Lee, F.Y.; et al. External validation of fatty liver index for identifying ultrasonographic fatty liver in a large-scale cross-sectional study in Taiwan. PLoS ONE 2015, 10, e0120443. [Google Scholar]
- Lai, X. Associations of Serum Uric Acid, Bilirubin and Their Change with Risk of Incident Cardiovascular Disease in a Prospective Cohort Study. Ph.D. Thesis, Huazhong University of Science and Technology, Wuhan, China, 2019. [Google Scholar]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [Green Version]
- Yoneda, M.; Yamamoto, T.; Honda, Y.; Imajo, K.; Ogawa, Y.; Kessoku, T.; Kobayashi, T.; Nogami, A.; Higurashi, T.; Kato, S.; et al. Risk of cardiovascular disease in patients with fatty liver disease as defined from the metabolic dysfunction associated fatty liver disease or nonalcoholic fatty liver disease point of view: A retrospective nationwide claims database study in Japan. J. Gastroenterol. 2021, 56, 1022–1032. [Google Scholar] [CrossRef]
- Xu, S.; Huang, W.; Qian, J.; Jin, L. Analysis of genomic admixture in Uyghur and its implication in mapping strategy. Am. J. Hum. Genet. 2008, 82, 883–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Jin, L. A genome-wide analysis of admixture in Uyghurs and a high-density admixture map for disease-gene discovery. Am. J. Hum. Genet. 2008, 83, 322–336. [Google Scholar] [CrossRef] [Green Version]
- Lear, S.A.; Humphries, K.H.; Kohli, S.; Chockalingam, A.; Frohlich, J.J.; Birmingham, C.L. Visceral adipose tissue accumulation differs according to ethnic background: Results of the Multicultural Community Health Assessment Trial (M-CHAT). Am. J. Clin. Nutr. 2007, 86, 353–359. [Google Scholar] [CrossRef]
- Tchernof, A.; Despres, J.P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Pais, R.; Giral, P.; Khan, J.F.; Rosenbaum, D.; Housset, C.; Poynard, T.; Ratziu, V.; Group, L.S. Fatty liver is an independent predictor of early carotid atherosclerosis. J. Hepatol. 2016, 65, 95–102. [Google Scholar] [CrossRef]
- Stepanova, M.; Younossi, Z.M. Independent association between nonalcoholic fatty liver disease and cardiovascular disease in the US population. Clin. Gastroenterol. Hepatol. 2012, 10, 646–650. [Google Scholar] [CrossRef]
- Morrison, A.E.; Zaccardi, F.; Khunti, K.; Davies, M.J. Causality between non-alcoholic fatty liver disease and risk of cardiovascular disease and type 2 diabetes: A meta-analysis with bias analysis. Liver Int. 2019, 39, 557–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauridsen, B.K.; Stender, S.; Kristensen, T.S.; Kofoed, K.F.; Kober, L.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. Liver fat content, non-alcoholic fatty liver disease, and ischaemic heart disease: Mendelian randomization and meta-analysis of 279,013 individuals. Eur. Heart J. 2018, 39, 385–393. [Google Scholar] [CrossRef]
- Gutierrez-Cuevas, J.; Santos, A.; Armendariz-Borunda, J. Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases. Int. J. Mol. Sci. 2021, 22, 11629. [Google Scholar] [CrossRef] [PubMed]
- Masarone, M.; Rosato, V.; Aglitti, A.; Bucci, T.; Caruso, R.; Salvatore, T.; Sasso, F.C.; Tripodi, M.F.; Persico, M. Liver biopsy in type 2 diabetes mellitus: Steatohepatitis represents the sole feature of liver damage. PLoS ONE 2017, 12, e0178473. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef]
- Sasso, F.C.; Pafundi, P.C.; Caturano, A.; Galiero, R.; Vetrano, E.; Nevola, R.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Di Marco, V.; et al. Impact of direct acting antivirals (DAAs) on cardiovascular events in HCV cohort with pre-diabetes. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2345–2353. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced incidence of type 2 diabetes in patients with chronic hepatitis C virus infection cleared by direct-acting antiviral therapy: A prospective study. Diabetes Obes. Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef] [PubMed]
- Lechner, K.; McKenzie, A.L.; Krankel, N.; Von Schacky, C.; Worm, N.; Nixdorff, U.; Lechner, B.; Scherr, J.; Weingartner, O.; Krauss, R.M. High-Risk Atherosclerosis and Metabolic Phenotype: The Roles of Ectopic Adiposity, Atherogenic Dyslipidemia, and Inflammation. Metab. Syndr. Relat. Disord. 2020, 18, 176–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasper, P.; Martin, A.; Lang, S.; Kutting, F.; Goeser, T.; Demir, M.; Steffen, H.M. NAFLD and cardiovascular diseases: A clinical review. Clin. Res. Cardiol. 2021, 110, 921–937. [Google Scholar] [CrossRef] [PubMed]
- Galiero, R.; Caturano, A.; Vetrano, E.; Cesaro, A.; Rinaldi, L.; Salvatore, T.; Marfella, R.; Sardu, C.; Moscarella, E.; Gragnano, F.; et al. Pathophysiological mechanisms and clinical evidence of relationship between Nonalcoholic fatty liver disease (NAFLD) and cardiovascular disease. Rev. Cardiovasc. Med. 2021, 22, 755–768. [Google Scholar] [CrossRef]
- Ji, J. Epidemiological Study on the Risk Factors of Cardiovascular Disease in Chinese Adults. Ph.D. Thesis, Peking Union Medical College, Beijing, China, 2011. [Google Scholar]
- Ai, Y. The Background and Consequences of Inter-Ethnic Marriage: A Case Study of Uyghur Marriage and Inter-Ethnic Marriage in Urumqi City. Master’s Thesis, Minzu University of China, Beijing, China, 2011. [Google Scholar]
- Zhang, X.; Ma, R.; Guo, H.; Zhang, J. Prevalence and screening indicators of metabolic syndrome in in rural area of Xinjiang. J. Shihezi Univ. (Nat. Sci.) 2019, 37, 513–518. [Google Scholar]
- Wang, Y.; Zhang, L.; He, J.; Yan, Y. Relationship between blood pressure and obesity in adults of remote rural areas of Xinjiang. Chin. J. Hypertens. 2016, 24, 650–656. [Google Scholar]
- He, J.; Guo, H.; Ding, Y.; Liu, J.; Zhang, M.; Ma, R.; Zhang, J.; Li, S.; Sun, F.; Xu, S.; et al. Epidemiological study on overweight and obesity among rural adult residents in Hazakh, Uygur and Han populations in Xinjiang. Chin. J. Epidemiol. 2013, 34, 1164–1168. [Google Scholar]
- Li, C. Nested Case-Control Study on Risk Factors of Coronary Heart Disease in Rural Minority Population of Xinjiang. Master’s Thesis, Shihezi University, Shihezi, China, 2020. [Google Scholar]
- He, H.; Pa, L.; Pan, L.; Simayi, A.; Mu, H.; Abudurexiti, Y.; Tao, N.; Shan, G. Effect of BMI and Its Optimal Cut-Off Value in Identifying Hypertension in Uyghur and Han Chinese: A Biethnic Study from the China National Health Survey (CNHS). Int. J. Hypertens. 2018, 2018, 1508083. [Google Scholar] [CrossRef] [Green Version]
- Frayn, K.N. Visceral fat and insulin resistance: Causative a correlative. Br. J. Nutr. 2000, 83 (Suppl. 1), S71–S77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abate, N.; Garg, A.; Peshock, R.M.; Stray-Gundersen, J.; Grundy, S.M. Relationship of generalized and regional adiposity to insulin sensitivity in man. J. Clin. Investig. 1995, 96, 88–98. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.M. Subcutaneous and visceral adipose tissue: Structural and functional differences. Obes. Rev. 2010, 11, 11–18. [Google Scholar] [CrossRef]
- Ben-Yacov, L.; Ainembabazi, P.; Stark, A.H.; Kizito, S.; Bahendeka, S. Prevalence and sex-specific patterns of metabolic syndrome in rural Uganda. BMJ Nutr. Prev. Health 2020, 3, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Overall | MAFLD | Non-MAFLD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n1 | CVD | Non-CVD | p1 | n2 | CVD | Non-CVD | p2 | ||
| n | 11,444 (100) | 1681 (14.69) | 308 (18.32) | 1373 (81.68) | 9763 (85.31) | 882 (9.03) | 8881 (90.96) | ||
| Age (years) a | 36.47 ± 13.38 | 42.85 ± 11.57 | 48.96 ± 11.16 | 41.47 ± 11.20 | <0.001 | 35.38 ± 13.36 | 47.25 ± 14.06 | 34.20 ± 12.70 | <0.001 |
| Sex | <0.001 | <0.001 | |||||||
| Male | 5940 (51.90) | 879 (52.29) | 124 (40.26) | 755 (54.99) | 5061 (51.84) | 373 (42.29) | 4688 (52.79) | ||
| Female | 5504 (48.10) | 802 (47.71) | 184 (59.74) | 618 (45.01) | 4702 (48.16) | 509 (57.71) | 4193 (47.21) | ||
| Marital status a | 0.296 | <0.001 | |||||||
| No | 2148 (18.77) | 154 (9.16) | 33 (10.71) | 121 (8.81) | 1994 (20.42) | 139 (15.76) | 1855 (20.89) | ||
| Yes | 9296 (81.23) | 1527 (90.84) | 275 (89.29) | 1252 (91.19) | 7769 (79.58) | 743 (84.24) | 7026 (79.11) | ||
| Education a | <0.001 | <0.001 | |||||||
| Illiteracy | 4334 (37.87) | 754 (44.85) | 171 (55.52) | 583 (42.46) | 3580 (36.67) | 496 (56.24) | 3084 (34.73) | ||
| Primary school | 3042 (26.58) | 458 (27.25) | 68 (22.08) | 390 (28.40) | 2584 (26.47) | 208 (23.58) | 2376 (26.75) | ||
| ≥Junior high school | 4068 (35.55) | 469 (27.90) | 69 (22.40) | 400 (29.13) | 3599 (36.86) | 178 (20.18) | 3421 (38.52) | ||
| Smoking | <0.001 | <0.001 | |||||||
| No | 9403(82.17) | 1383(82.27) | 279 (90.58) | 1104 (80.41) | 8020(82.15) | 770 (87.30) | 7250 (81.63) | ||
| Yes | 2041(17.83) | 298(17.73) | 29 (9.42) | 269 (19.59) | 1743(17.85) | 112 (12.70) | 1631 (18.37) | ||
| Drinking b | 0.001 | 0.372 | |||||||
| No | 10,841 (94.73) | 1571 (93.46) | 301 (97.73) | 1270 (92.50) | 9270 (94.95) | 843 (95.58) | 8427 (94.89) | ||
| Yes | 603 (5.27) | 110 (6.54) | 7 (2.27) | 103 (7.50) | 493 (5.05) | 39 (4.42) | 454 (5.11) | ||
| Overweight a | 5958 (52.06) | 1572 (93.52) | 297 (96.43) | 1275 (92.86) | 0.022 | 4386 (44.92) | 556 (63.04) | 3830 (43.13) | <0.001 |
| Abdominal obesity a | 8394 (73.35) | 1605 (63.36) | 295 (95.78) | 1310 (95.41) | 0.779 | 6789 (69.54) | 743 (84.24) | 6046 (68.08) | <0.001 |
| Obesity a | <0.001 | <0.001 | |||||||
| No | 9421 (82.32) | 703 (41.82) | 101 (32.79) | 602 (43.85) | 8718 (89.30) | 703 (79.71) | 8015 (90.25) | ||
| Obese class Ⅰ | 1574 (13.75) | 274 (16.30) | 124 (40.26) | 150 (10.92) | 1300 (13.32) | 543 (61.56) | 757 (8.52) | ||
| Obese class Ⅱ | 367 (3.21) | 98 (5.83) | 71 (23.05) | 27 (1.97) | 269 (2.76) | 182 (20.63) | 87 (0.98) | ||
| Obese class Ⅲ | 82 (0.72) | 14 (0.83) | 12 (3.90) | 2 (0.15) | 68 (0.70) | 46 (5.22) | 22 (0.25) | ||
| T2DM a | 0.055 | <0.001 | |||||||
| No | 10,896 (95.21) | 1498 (89.11) | 265 (86.04) | 1233 (89.80) | 9398 (96.26) | 812 (92.06) | 8586 (96.68) | ||
| Yes | 548 (4.79) | 183 (10.89) | 43 (13.96) | 140 (10.20) | 365 (3.74) | 70 (7.94) | 295 (3.32) | ||
| FPG level a | 0.278 | 0.012 | |||||||
| ≤6.0 | 10,442 (91.24) | 1386 (82.45) | 248 (80.52) | 1138 (82.88) | 9056 (92.76) | 789 (89.46) | 8267 (93.09) | ||
| 6.1–6.9 | 495 (4.33) | 53 (3.15) | 19 (6.17) | 34 (2.48) | 442 (4.53) | 107 (12.13) | 335 (3.77) | ||
| ≥7.0 | 507 (4.43) | 100 (5.95) | 41 (13.31) | 59 (4.30) | 407 (4.17) | 128 (14.51) | 279 (3.14) | ||
| Dyslipidaemia a | 0.157 | <0.001 | |||||||
| No | 8099 (70.77) | 798 (47.47) | 135 (43.83) | 663 (48.29) | 7301 (74.78) | 580 (65.76) | 6721 (75.68) | ||
| Yes | 3345 (29.23) | 883 (52.53) | 173 (56.17) | 710 (51.71) | 2462 (25.22) | 302 (34.24) | 2160 (24.32) | ||
| High LDL a | 276 (2.41) | 59 (3.51) | 24 (7.79) | 35 (2.55) | 0.009 | 217 (2.22) | 58 (6.58) | 159 (1.79) | <0.001 |
| Low HDL a | 976 (8.53) | 187 (11.12) | 69 (22.40) | 118 (8.59) | 1.000 | 789 (8.08) | 164 (18.59) | 625 (7.04) | <0.001 |
| High TG a | 2124 (18.56) | 272 (16.18) | 119 (38.64) | 153 (11.14) | 1.000 | 1852 (18.97) | 541 (61.34) | 1311 (14.76) | 0.074 |
| High TC a | 874 (7.64) | 105 (6.25) | 38 (12.34) | 67 (4.88) | 0.068 | 769 (7.88) | 227 (25.74) | 542 (6.10) | 0.080 |
| Family history of CVD | 1416 (12.37) | 222 (13.21) | 23 (7.47) | 199 (14.49) | 0.001 | 1194 (12.23) | 113 (12.81) | 1081 (12.17) | 0.58 |
| Family history of T2DM a | 435 (3.80) | 101 (6.01) | 13 (4.22) | 88 (6.41) | 0.144 | 334 (3.42) | 38 (4.31) | 296 (3.33) | 0.129 |
| BMI (kg/m2) a | 25.78 ± 4.78 | 31.19 ± 4.94 | 32.13 ± 4.34 | 30.98 ± 5.04 | <0.001 | 24.85 ± 4.08 | 26.58 ± 4.16 | 24.68 ± 4.03 | <0.001 |
| WC (cm) a | 90.01 ± 13.16 | 101.91 ± 12.31 | 104.05 ± 12.66 | 101.44 ± 12.18 | <0.001 | 87.96 ± 12.17 | 92.16 ± 12.80 | 87.54 ± 12.03 | <0.001 |
| SBP (mm Hg) a | 126.59 ± 17.96 | 133.94 ± 19.30 | 142.14 ± 21.52 | 132.10 ± 18.28 | <0.001 | 125.32 ± 17.41 | 136.66 ± 22.71 | 124.19 ± 16.37 | <0.001 |
| DBP (mm Hg) a | 74.15 ± 11.96 | 78.59 ± 12.63 | 82.06 ± 13.12 | 77.81 ± 12.39 | <0.001 | 73.38 ± 11.67 | 78.14 ± 13.03 | 72.91 ± 11.42 | <0.001 |
| FPG (mmol/L) a | 4.92 ± 1.84 | 5.48 ± 2.77 | 5.66 ± 3.14 | 5.44 ± 2.68 | 0.726 | 4.83 ± 1.61 | 5.05 ± 2.12 | 4.81 ± 1.54 | 0.428 |
| TG (mmol/L) a | 1.69 ± 1.44 | 2.39 ± 1.87 | 2.33 ± 1.55 | 2.41 ± 1.94 | 0.904 | 1.57 ± 1.32 | 1.72 ± 1.22 | 1.56 ± 1.33 | <0.001 |
| TC (mmol/L) a | 4.72 ± 2.04 | 5.24 ± 1.99 | 5.02 ± 1.08 | 5.30 ± 2.14 | 0.087 | 4.63 ± 2.03 | 4.74 ± 1.40 | 4.62 ± 2.08 | <0.001 |
| HDL-C (mmol/L) a | 1.57 ± 0.56 | 1.52 ± 0.59 | 1.41 ± 0.63 | 1.55 ± 0.57 | <0.001 | 1.58 ± 0.78 | 1.45 ± 0.55 | 1.59 ± 0.56 | <0.001 |
| LDL-C (mmol/L) a | 2.63 ± 0.83 | 2.84 ± 1.06 | 3.00 ± 1.83 | 2.81 ± 0.79 | 0.106 | 2.59 ± 0.78 | 2.69 ± 0.80 | 2.58 ± 0.78 | <0.001 |
| ALT (IU/L) a | 24.59 ± 13.69 | 26.00 ± 12.98 | 26.61 ± 14.17 | 25.87 ± 12.70 | 0.45 | 24.35 ± 13.80 | 23.80 ± 10.29 | 24.40 ± 14.10 | 0.033 |
| AST (IU/L) a | 30.47 ± 24.69 | 38.33 ± 28.62 | 36.34 ± 31.33 | 38.78 ± 27.97 | 0.001 | 29.12 ± 23.70 | 28.82 ± 23.96 | 29.15 ± 23.67 | 0.194 |
| GGT (IU/L) a | 19.15 ± 16.52 | 25.81 ± 19.93 | 23.74 ± 14.60 | 23.79 ± 17.37 | 0.347 | 17.62 ± 15.23 | 19.68 ± 15.23 | 18.22 ± 10.50 | 0.257 |
| SCr (mol/L) a | 71.60 ± 16.17 | 72.91 ± 16.97 | 68.94 ± 16.76 | 73.80 ± 16.90 | <0.001 | 71.38 ± 16.02 | 69.52 ± 17.45 | 71.56 ± 15.86 | <0.001 |
| eGFR (ml/min/1.73 m2) a | 108.39 ± 36.93 | 103.79 ± 38.49 | 88.39 ± 35.91 | 107.25 ± 38.21 | <0.001 | 109.17 ± 36.60 | 91.58 ± 39.09 | 110.92 ± 35.87 | <0.001 |
| CVD incidence a | 1190 (10.40) | 308 (18.32) | 882 (9.03) | ||||||
| Follow-up, years | 4.44 ± 0.78 | 4.26 ± 1.00 | 4.47 ± 0.74 | ||||||
| Group | n (%) | CVD Events | Rate * | HR (95% CI) | ||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| US | ||||||
| Non-MAFLD | 9763 (85.31) | 882 | 549.5 | Reference | Reference | Reference |
| MAFLD | 1681 (14.69) | 308 | 1160.2 | 2.12 (1.86–2.42) | 1.54 (1.36–1.76) | 1.36 (1.19–1.55) |
| FLI | ||||||
| Non-MAFLD | 8843 (77.27) | 718 | 438.7 | Reference | Reference | Reference |
| MAFLD | 2601 (22.72) | 472 | 1023.4 | 2.36 (2.10–2.65) | 1.66 (1.48–1.87) | 1.37 (1.21–1.55) |
| HSI | ||||||
| Non-MAFLD | 7626 (66.64) | 557 | 397.3 | Reference | Reference | Reference |
| MAFLD | 3818 (33.36) | 633 | 920.9 | 2.39 (2.13–2.67) | 1.54 (1.37–1.74) | 1.30 (1.15–1.46) |
| Subgroup | Non-MAFLD | MAFLD | HR (95% CI) | ||
|---|---|---|---|---|---|
| CVD Events | Rate * | CVD Events | Rate * | ||
| Sex | |||||
| male | 373 | 413.8 | 124 | 796.9 | 1.35 (1.10–1.66) |
| female | 509 | 569.1 | 184 | 1330.2 | 1.33 (1.12–1.58) |
| Age | |||||
| <35 | 183 | 190.4 | 29 | 445.4 | 1.77 (1.18–2.65) |
| ≥35 | 699 | 889.4 | 279 | 1253.4 | 1.21 (1.05–1.39) |
| Smoking | 112 | 387.7 | 29 | 561.2 | 1.11(0.73,1.68) |
| Drinking | 39 | 474.3 | 7 | 348.2 | 0.45 (0.19–1.03) |
| Overweight | 556 | 684.6 | 297 | 1088.6 | 1.27 (1.11–1.47) |
| Abdominal obesity | 743 | 590.1 | 295 | 1058.6 | 1.32 (1.15–1.51) |
| High LDL | 35 | 1052.7 | 24 | 1885.1 | 1.58 (0.92–2.70) |
| Low HDL | 118 | 923.6 | 69 | 1593.5 | 1.90 (1.40–2.57) |
| High TG | 153 | 579.5 | 119 | 940.7 | 1.55 (1.22–1.98) |
| High TC | 67 | 599.5 | 38 | 806.4 | 1.08 (0.73–1.62) |
| Subgroup | CVD Events | Rate * | HR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| MAFLD | Obesity | |||||
| − | − | 703 | 490.9 | Reference | Reference | Reference |
| − | + | 179 | 842.7 | 2.21 (1.88–2.61) | 1.60 (1.36–1.89) | 1.31 (1.11–1.55) |
| + | − | 101 | 1059.3 | 1.84 (1.49–2.27) | 1.37 (1.12–1.69) | 1.30 (1.05–1.60) |
| + | + | 207 | 1393.2 | 2.75 (2.35–3.21) | 1.86 (1.59–2.17) | 1.52 (1.30–1.79) |
| MAFLD | Dyslipidaemia | |||||
| − | − | 580 | 422.1 | Reference | Reference | Reference |
| − | + | 302 | 686.4 | 1.58 (1.37–1.81) | 1.19 (1.03–1.37) | 1.12 (0.97–1.29) |
| + | − | 135 | 1022.6 | 2.20 (1.83–2.66) | 1.46 (1.21–1.76) | 1.28 (1.06–1.55) |
| + | + | 173 | 1065.5 | 2.63 (2.22–3.12) | 1.81 (1.53–2.15) | 1.56 (1.31–1.86) |
| MAFLD | T2DM | |||||
| − | − | 812 | 465.4 | Reference | Reference | Reference |
| − | + | 70 | 1095.9 | 2.35 (1.84–3.00) | 1.40 (1.09–1.79) | 1.34 (1.05–1.71) |
| + | − | 265 | 1013.5 | 2.14 (1.86–2.46) | 1.55 (1.35–1.78) | 1.38 (1.20– 1.59) |
| + | + | 43 | 1311.6 | 2.96 (2.18–4.02) | 1.82 (1.34–2.48) | 1.64 (1.20–2.23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Yang, J.; Ma, R.; Zhang, X.; Guo, H.; He, J.; Wang, X.; Cao, B.; Maimaitijiang, R.; Li, Y.; et al. Metabolic Dysfunction-Associated Fatty Liver Disease Is Associated with the Risk of Incident Cardiovascular Disease: A Prospective Cohort Study in Xinjiang. Nutrients 2022, 14, 2361. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14122361
Guo Y, Yang J, Ma R, Zhang X, Guo H, He J, Wang X, Cao B, Maimaitijiang R, Li Y, et al. Metabolic Dysfunction-Associated Fatty Liver Disease Is Associated with the Risk of Incident Cardiovascular Disease: A Prospective Cohort Study in Xinjiang. Nutrients. 2022; 14(12):2361. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14122361
Chicago/Turabian StyleGuo, Yanbo, Jing Yang, Rulin Ma, Xianghui Zhang, Heng Guo, Jia He, Xinping Wang, Boyu Cao, Remina Maimaitijiang, Yu Li, and et al. 2022. "Metabolic Dysfunction-Associated Fatty Liver Disease Is Associated with the Risk of Incident Cardiovascular Disease: A Prospective Cohort Study in Xinjiang" Nutrients 14, no. 12: 2361. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14122361