
Association between Micronutrient Intake and Breast Cancer Risk According to Body Mass Index in South Korean Adult Women: A Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
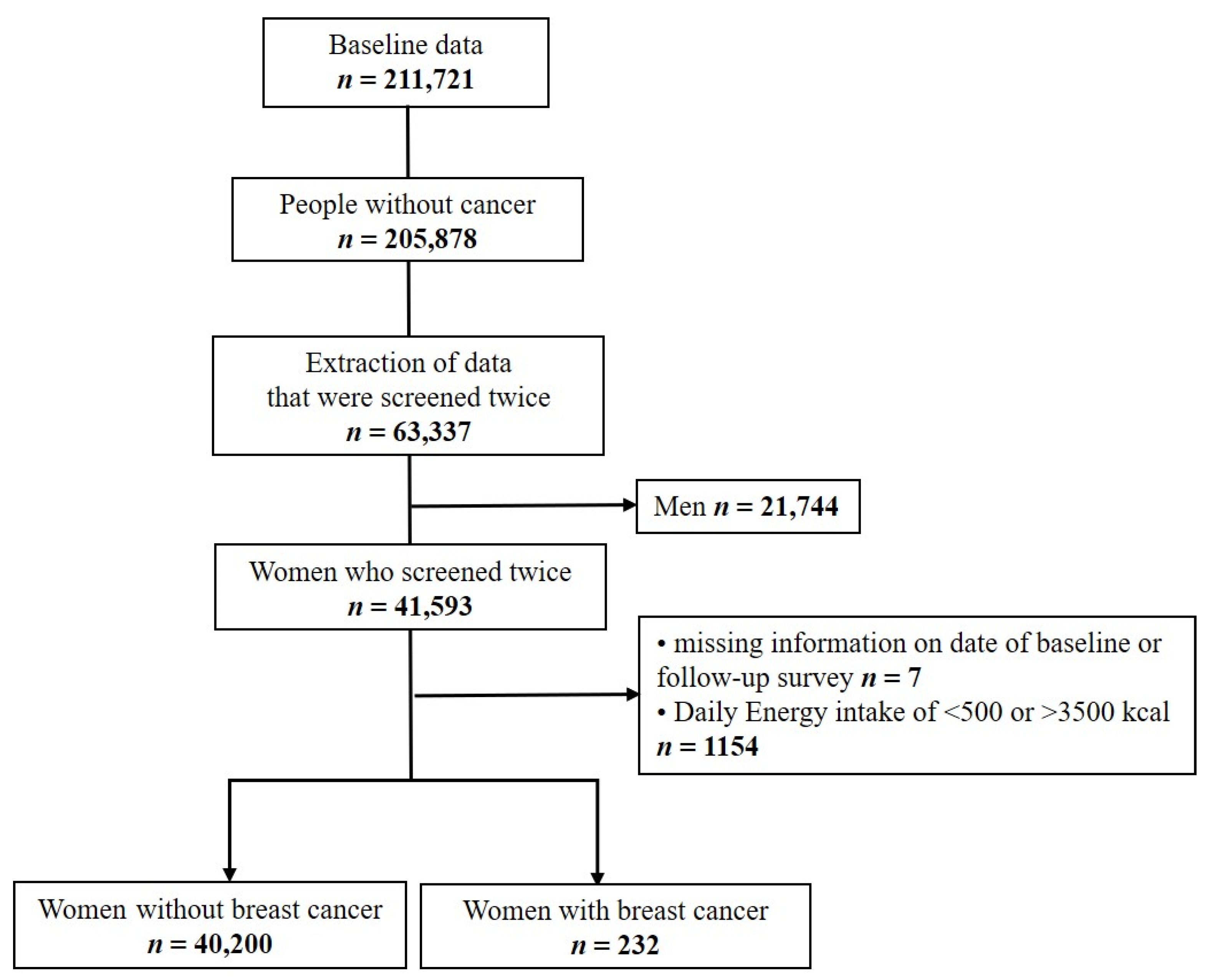
2.1. Study Design and Population
2.2. Assessment of Nutrient Intake
2.3. Breast Cancer Incidence
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Nutrient | Age Group (y) | |||
|---|---|---|---|---|
| 30–49 | 50–64 | 65–74 | ≥75 | |
| Calcium (mg) | 700 | 800 | 800 | 800 |
| Phosphorus (mg) | 580 | 580 | 580 | 580 |
| Iron (mg) | 14 | 8 | 8 | 7 |
| Potassium (mg) | 3500 | 3500 | 3500 | 3500 |
| Vitamin A (R.E.) | 650 | 600 | 600 | 550 |
| Sodium (mg) | 1500 | 1500 | 1500 | 1500 |
| Vitamin B1 (mg) | 1.1 | 1.1 | 1 | 0.8 |
| Vitamin B2 (mg) | 1.2 | 1.2 | 1.1 | 1 |
| Niacin (mg) | 14 | 14 | 13 | 12 |
| Vitamin C (mg) | 100 | 100 | 100 | 100 |
| Zinc (µg) | 8 | 8 | 7 | 7 |
| Vitamin B6 (mg) | 1.4 | 1.4 | 1.4 | 1.4 |
| Folate (µg) | 400 | 400 | 400 | 400 |
| Fiber (g) | 20 | 20 | 20 | 20 |
| Vitamin E (mg) | 12 | 12 | 12 | 12 |
| Cholesterol (mg) | 180 | 120 | 50 | 20 |
| Nutrient | No | <52 | ≥52 |
|---|---|---|---|
| aHR * (95% CI) | aHR * (95% CI) | aHR * (95% CI) | |
| >Recommended Intake (Reference: ≤Recommended Intake) ** | |||
| Calcium (mg) | 1.08 (0.54–2.16) | 0.61 (0.22–1.65) | 2.12 (0.85–5.29) |
| Phosphorus (mg) | 1.28 (0.64–2.55) | 0.98 (0.44–2.22) | 0.61 (0.28–1.33) |
| Iron (mg) | 0.73 (0.37–1.44) | 0.57 (0.30–1.10) | 0.87 (0.44–1.72) |
| Potassium (mg) | 0.62 (0.25–1.51) | 0.55 (0.20–1.53) | 2.17 (0.88–5.36) |
| Vitamin A (R.E.) | 1.42 (0.84–2.41) | 0.60 (0.29–1.22) | 1.21 (0.61–2.42) |
| Sodium (mg) | 0.77 (0.48–1.24) | 1.34 (0.70–2.57) | 0.89 (0.47–1.68) |
| Vitamin B1 (mg) | 1.02 (0.57–1.81) | 0.87 (0.42–1.80) | 2.31 (1.05–5.08) |
| Vitamin B2 (mg) | 1.05 (0.56–1.95) | 0.85 (0.39–1.83) | 2.60 (1.21–5.59) |
| Niacin (mg) | 1.12 (0.66–1.91) | 0.78 (0.40–1.51) | 1.14 (0.55–2.38) |
| Vitamin C (mg) | 0.91 (0.58–1.42) | 1.35 (0.78–2.33) | 0.83 (0.45–1.54) |
| Zinc (µg) | 0.88 (0.50–1.57) | 0.89 (0.45–1.77) | 0.83 (0.38–1.81) |
| Vitamin B6 (mg) | 1.12 (0.67–1.89) | 0.60 (0.31–1.13) | 0.84 (0.42–1.70) |
| Folate (µg) | 1.13 (0.46–2.75) | 1.19 (0.47–3.03) | 1.22 (0.39–3.79) |
| Vitamin E (mg) | 1.27 (0.65–2.46) | 0.76 (0.31–1.86) | 1.06 (0.39–2.87) |
| Cholesterol (mg) | 1.17 (0.74–1.86) | 1.06 (0.60–1.87) | 1.23 (0.67–2.26) |
| (a). Calcium—1/2pt | ||
| Study type | Title | Findings |
| Cohort study | Calcium intake is not related to breast cancer risk among Singapore Chinese women [56]. |
|
| Case-control study | Dairy Products, Calcium Intake, and Breast Cancer Risk: A Case-Control Study in China [57]. |
|
| Meta-analysis | Meta-analysis of vitamin D, calcium, and the prevention of breast cancer [58]. |
|
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| (b). Phosphorus | ||
| Study type | Title | Findings |
| Cohort study | Imbalanced Nutrient Intake in Cancer Survivors from the Examination from the Nationwide Health Examination Center-Based Cohort [60]. |
|
| Case-control study | The Intake of some Nutrients is Associated with the Risk of Breast Cancer: Results from Jordanian Case-Control Study [61]. |
|
| (c). Iron | ||
| Study type | Title | Findings |
| Cohort study | Dietary Iron and Heme Iron Intake and Risk of Breast Cancer: A Prospective Cohort Study [62]. |
|
| Case-control study | A case-control study on heme/non-heme iron and breast cancer risk breast cancer risk [63]. |
|
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| Meta-analysis | Iron intake, body iron status, and risk of breast cancer: a systematic review and meta-analysis [64]. |
|
| (d). Vitamin A | ||
| Study type | Title | Findings |
| Cohort study | A Prospective Study of the Intake of Vitamins C, E, and A and the Risk of Breast Cancer [65]. |
|
| Case-control study | Intake of Carrots, Spinach, and Supplements Containing Vitamin A in Relation to Risk of Breast Cancer [66]. |
|
| Meta-analysis | Vitamin A and Breast Cancer Survival: A Systematic Review and Meta-analysis [67]. |
|
| (e). Vitamin B1 | ||
| Study type | Title | Findings |
| Cohort study | B-Vitamin Intake from Diet and Supplements and Breast Cancer Risk in Middle-Aged Women: Results from the Prospective NutriNet-Santé Cohort [68]. |
|
| Case-control study | Nutrient Patterns and Risk of Breast Cancer among Iranian Women: a Case- Control Study [69]. |
|
| Cohort study | B-Vitamin Intake, One-Carbon Metabolism, and Survival in a Population-Based Study of Women with Breast Cancer [68]. |
|
| (f). Vitamin B2 | ||
| Study type | Title | Findings |
| Cohort study | Dietary B-Vitamin Intake and Risk of Breast, Endometrial, Ovarian and Colorectal Cancer among Canadians [70]. |
|
| Case-control study | Nutrient Patterns and Risk of Breast Cancer among Iranian Women: a Case–Control Study [69]. |
|
| Meta-analysis | Dietary vitamin B2 intake and breast cancer risk: a systematic review and meta-analysis [71]. |
|
| (g). Vitamin C | ||
| Study type | Title | Findings |
| Cohort study | Vitamin C intake from diary recordings and risk of breast cancer in the UK Dietary Cohort Consortium [72]. |
|
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| Cohort study | Dietary fiber, vitamins A, C, and E, and risk of breast cancer: a cohort study [73]. |
|
| (h). Zinc | ||
| Study type | Title | Findings |
| Prospective nested case-control study | Serum zinc and dietary intake of zinc in relation to risk of different breast cancer subgroups and serum levels as a marker of intake: a prospective nested case-control study [74]. |
|
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| Meta-analysis | A meta-analysis of zinc levels in breast cancer [75]. |
|
| (i). Vitamin B6 | ||
| Study type | Title | Findings |
| Nested case-control study | Plasma Folate, Vitamin B6, Vitamin B12, Homocysteine, and Risk of Breast Cancer [76]. |
|
| Nested case-control study | Association of vitamin B6, vitamin B12 and methionine with risk of breast cancer: a dose–response meta-analysis [46]. |
|
| Meta-analysis | Folate, Vitamin B6, and Vitamin B12 Intake and the Risk of Breast Cancer Among Mexican Women [77]. |
|
| (j). Folate | ||
| Study type | Title | Findings |
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| Meta-analysis | Higher dietary folate intake reduces the breast cancer risk: a systematic review and meta-analysis [78]. |
|
| Meta-analysis | Folate, Vitamin B6, and Vitamin B12 Intake and the Risk of Breast Cancer Among Mexican Women [77]. |
|
| (k). Vitamin E | ||
| Study type | Title | Findings |
| Meta-analysis | Retinol, vitamins A, C, and E and breast cancer risk: a meta-analysis and meta-regression [6]. |
|
| Case-control study | Raw and Cooked Vegetables, Fruits, Selected Micronutrients, and Breast Cancer Risk: A Case–Control Study in Germany [59]. |
|
| (l). Cholesterol | ||
| Study type | Title | Findings |
| Cohort study | Dietary Factors and Female Breast Cancer Risk: A Prospective Cohort Study [79]. |
|
| Case-control study | Dietary cholesterol intake and cancer [80]. |
|
| Meta-analysis | Updating the role of obesity and cholesterol in breast cancer [81]. |
|
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Won, Y.J.; Lee, J.J.; Jung, K.W.; Kong, H.J.; Im, J.S.; Seo, H.G. The Community of Population-Based Regional Cancer Registries Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2018. Cancer Res. Treat. 2021, 53, 301–315. [Google Scholar] [CrossRef] [PubMed]
- McPherson, K.; Steel, C.; Dixon, J. Breast cancer—epidemiology, risk factors, and genetics. Bmj 2000, 321, 624–628. [Google Scholar] [CrossRef] [Green Version]
- Thomson, C.A. Diet and breast cancer: Understanding risks and benefits. Nutr. Clin. Pract. 2012, 27, 636–650. [Google Scholar] [CrossRef] [PubMed]
- Velie, E.M.; Schairer, C.; Flood, A.; He, J.-P.; Khattree, R.; Schatzkin, A. Empirically derived dietary patterns and risk of postmenopausal breast cancer in a large prospective cohort study. Am. J. Clin. Nutr. 2005, 82, 1308–1319. [Google Scholar] [CrossRef] [PubMed]
- Fulan, H.; Changxing, J.; Baina, W.Y.; Wencui, Z.; Chunqing, L.; Fan, W.; Dandan, L.; Dianjun, S.; Tong, W.; Da, P.; et al. Retinol, vitamins A, C, and E and breast cancer risk: A meta-analysis and meta-regression. Cancer Causes Control 2011, 22, 1383–1396. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Ke, Y.; Wu, S.; Huang, S.; Li, S.; Lv, Z.; Yeoh, E.-K.; Lao, X.; Wong, S.; Kim, J.H.; et al. Association between whole grain intake and breast cancer risk: A systematic review and meta-analysis of observational studies. Nutr. J. 2018, 17, 87. [Google Scholar] [CrossRef]
- Ghoncheh, M.; Mahdavifar, N.; Darvishi, E.; Salehiniya, H. Epidemiology, incidence and mortality of breast cancer in Asia. Asian Pac. J. Cancer Prev. 2016, 17, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Turner, L.B. A meta-analysis of fat intake, reproduction, and breast cancer risk: An evolutionary perspective. Am. J. Hum. Biol. 2011, 23, 601–608. [Google Scholar] [CrossRef]
- Prentice, R.L.; Caan, B.; Chlebowski, R.T.; Patterson, R.; Kuller, L.H.; Ockene, J.K.; Margolis, K.L.; Limacher, M.C.; Manson, J.E.; Parker, L.M.; et al. Low-Fat dietary pattern and risk of invasive breast cancer: The women’s health initiative randomized controlled dietary modification trial. Jama 2006, 295, 629–642. [Google Scholar] [CrossRef]
- Anderson, J.J.; Darwis, N.D.; Mackay, D.F.; Celis-Morales, C.A.; Lyall, D.M.; Sattar, N.; Gill, J.M.; Pell, J.P. Red and processed meat consumption and breast cancer: UK Biobank cohort study and meta-analysis. Eur. J. Cancer 2017, 90, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Farvid, M.S.; Stern, M.C.; Norat, T.; Sasazuki, S.; Vineis, P.; Weijenberg, M.P.; Wolk, A.; Wu, K.; Stewart, B.W.; Cho, E. Consumption of red and processed meat and breast cancer incidence: A systematic review and meta-analysis of prospective studies. Int. J. Cancer 2018, 143, 2787–2799. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.M.; Vieira, A.R.; Rosenblatt, D.A.N.; Vieira, R.; Greenwood, D.C.; Norat, T. Fruits, vegetables and breast cancer risk: A systematic review and meta-analysis of prospective studies. Breast Cancer Res. Treat. 2012, 134, 479–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masala, G.; Assedi, M.; Bendinelli, B.; Ermini, I.; Sieri, S.; Grioni, S.; Sacerdote, C.; Ricceri, F.; Panico, S.; Mattiello, A.; et al. Fruit and vegetables consumption and breast cancer risk: The EPIC Italy study. Breast Cancer Res. Treat. 2012, 132, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.Y.; Qin, L.Q. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: A meta-analysis of prospective studies. Breast Cancer Res. Treat. 2011, 125, 315–323. [Google Scholar] [CrossRef]
- Wu, A.H.; Yu, M.C.; Tseng, C.-C.; Pike, M.C. Epidemiology of soy exposures and breast cancer risk. Br. J. Cancer 2008, 98, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Xia, J.; Li, L.; Ke, Y.; Cheng, J.; Xie, Y.; Chu, W.; Cheung, P.; Kim, J.H.; Colditz, G.A.; et al. Associations between dietary patterns and the risk of breast cancer: A systematic review and meta-analysis of observational studies. Breast Cancer Res. 2019, 21, 16. [Google Scholar] [CrossRef] [Green Version]
- Cuenca-Micó, O.; Aceves, C. Micronutrients and Breast Cancer Progression: A Systematic Review. Nutrients 2020, 12, 3613. [Google Scholar] [CrossRef]
- Woo, H.D.; Park, S.; Oh, K.; Kim, H.J.; Shin, H.R.; Moon, H.K.; Kim, J. Diet and Cancer Risk in the Korean Population: A Meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 8509–8519. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.G. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Group, H.E.S. The Health Examinees (HEXA) study: Rationale, study design and baseline characteristics. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 1591–1597. [Google Scholar]
- Wee, J.H.; Min, C.; Park, M.W.; Byun, S.H.; Lee, H.-J.; Park, B.; Choi, H.G. The association of asthma and its subgroups with osteoporosis: A cross-sectional study using KoGES HEXA data. Allergy Asthma Clin. Immunol. 2020, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Kim, H.; Kim, J.; Hwang, J.-Y.; Lee, J.; Yoon, M.O. The development of the 2020 dietary reference intakes for Korean population: Lessons and challenges. J. Nutr. Health 2021, 54, 425–434. [Google Scholar] [CrossRef]
- Block, G. Vitamin C and cancer prevention: The epidemiologic evidence. Am. J. Clin. Nutr. 1991, 53, 270S–282S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutsenko, E.A.; Cárcamo, J.M.; Golde, D.W. Vitamin C prevents DNA mutation induced by oxidative stress. J. Biol. Chem. 2002, 277, 16895–16899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Yu, E.; Liu, L.; Zhang, W.; Wei, X.; Gao, X.; Song, N.; Fu, C. Dietary intake of vitamins A, C, and E and the risk of colorectal adenoma: A meta-analysis of observational studies. Eur. J. Cancer Prev. 2013, 22, 529–539. [Google Scholar] [CrossRef]
- Li, P.; Zhang, H.; Chen, J.; Shi, Y.; Cai, J.; Yang, J.; Wu, Y. Association between dietary antioxidant vitamins intake/blood level and risk of gastric cancer. Int. J. Cancer 2014, 135, 1444–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, T.K.; Freedman, N.D.; Fan, J.-H.; Qiao, Y.-L.; Dawsey, S.M.; Taylor, P.R.; Abnet, C. Prediagnostic plasma vitamin C and risk of gastric adenocarcinoma and esophageal squamous cell carcinoma in a Chinese population. Am. J. Clin. Nutr. 2013, 98, 1289–1297. [Google Scholar] [CrossRef]
- Bo, Y.; Lu, Y.; Zhao, Y.; Zhao, E.; Yuan, L.; Lu, W.; Cui, L.; Lu, Q. Association between dietary vitamin C intake and risk of esophageal cancer: A dose-response meta-analysis. Int. J. Cancer 2015, 138, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Bandera, E.V.; Gifkins, D.M.; Moore, D.F.; McCullough, M.L.; Kushi, L.H. Antioxidant vitamins and the risk of endometrial cancer: A dose–response meta-analysis. Cancer Causes Control 2008, 20, 699–711. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Shen, L.; Zheng, D. Association between vitamin C intake and lung cancer: A dose-response meta-analysis. Sci. Rep. 2014, 4, 6161. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Xu, P.; Li, Y.; Wei, B.; Yang, S.; Zheng, Y.; Lyu, L.; Deng, Y.; Zhai, Z.; Li, N.; et al. Association of vitamin C intake with breast cancer risk and mortality: A meta-analysis of observational studies. Aging 2020, 12, 18415–18435. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.; Wu, Z.; Li, G.; Teng, C.; Liu, Y.; Wang, F.; Zhao, Y.; Pang, D. The plasma level of retinol, vitamins A, C and α-tocopherol could reduce breast cancer risk? A meta-analysis and meta-regression. J. Cancer Res. Clin. Oncol. 2015, 141, 601–614. [Google Scholar] [CrossRef]
- Salminen, E.K.; Lagström, H.K.; Heikkilä, S.P.; Salminen, S.J. Does breast cancer change patients’ dietary habits? Eur. J. Clin. Nutr. 2000, 54, 844–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marseglia, L.; Manti, S.; D’Angelo, G.; Nicotera, A.G.; Parisi, E.; Di Rosa, G.; Gitto, E.; Arrigo, T. Oxidative stress in obesity: A critical component in human diseases. Int. J. Mol. Sci. 2014, 16, 378–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, P.G.; Hudis, C.A.; Giri, D.; Morrow, M.; Falcone, D.J.; Zhou, X.K.; Du, B.; Brogi, E.; Crawford, C.B.; Kopelovich, L.; et al. Inflammation and increased aromatase expression occur in the breast tissue of obese women with breast cancer. Cancer Prev. Res. 2011, 4, 1021–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heath, A.K.; Muller, D.; Brandt, P.A.V.D.; Papadimitriou, N.; Critselis, E.; Gunter, M.; Vineis, P.; Weiderpass, E.; Fagherazzi, G.; Boeing, H.; et al. Nutrient-wide association study of 92 foods and nutrients and breast cancer risk. Breast Cancer Res. 2020, 22, 5. [Google Scholar] [CrossRef]
- Schlueter, A.K.; Johnston, C.S. Vitamin C: Overview and Update. J. Evid.-Based Complement. Altern. Med. 2011, 16, 49–57. [Google Scholar] [CrossRef]
- Dehghan, M.; Akhtar-Danesh, N.; McMillan, C.R.; Thabane, L. Is plasma vitamin C an appropriate biomarker of vitamin C intake? A systematic review and meta-analysis. Nutr. J. 2007, 6, 41. [Google Scholar] [CrossRef] [Green Version]
- Vioque, J.; Weinbrenner, T.; Asensio, L.; Castelló, A.; Young, I.S.; Fletcher, A. Plasma concentrations of carotenoids and vitamin C are better correlated with dietary intake in normal weight than overweight and obese elderly subjects. Br. J. Nutr. 2007, 97, 977–986. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J. Nutr. Health Aging 2002, 6, 39–42. [Google Scholar] [PubMed]
- Ames, B.N. DNA damage from micronutrient deficiencies is likely to be a major cause of cancer. Mutat. Res. Mol. Mech. Mutagen. 2001, 475, 7–20. [Google Scholar] [CrossRef]
- Mocellin, S.; Briarava, M.; Pilati, P. Vitamin B6 and Cancer Risk: A Field Synopsis and Meta-Analysis. JNCI: J. Natl. Cancer Inst. 2016, 109. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N.; Wolk, A. Vitamin B6 and Risk of Colorectal Cancer: A Meta-analysis of Prospective Studies. JAMA 2010, 303, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.-H.; Mao, Q.-Q. Vitamin B6, vitamin B12 and methionine and risk of pancreatic cancer: A meta-analysis. Nutr. J. 2020, 19, 111. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Kang, S.; Zhang, D. Association of vitamin B6, vitamin B12 and methionine with risk of breast cancer: A dose-response meta-analysis. Br. J. Cancer 2013, 109, 1926–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, J.; Gu, Y.; Fu, H.; Liu, C.; Zou, Y.; Chang, H. Association Between one-carbon metabolism-related vitamins and risk of breast cancer: A systematic review and meta-analysis of prospective studies. Clin. Breast Cancer 2020, 20, e469–e480. [Google Scholar] [CrossRef] [PubMed]
- Clasen, J.L.; Heath, A.K.; Van Puyvelde, H.; Huybrechts, I.; Park, J.Y.; Ferrari, P.; Johansson, M.; Scelo, G.; Ulvik, A.; Midttun, Ø.; et al. A comparison of complementary measures of vitamin B6 status, function, and metabolism in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2021, 114, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Navarrete, J.M.; Jove, M.; Ortega, F.; Xifra, G.; Ricart, W.; Obis, È.; Pamplona, R.; Portero-Otin, M.; Fernández-Real, J.M. Metabolomics uncovers the role of adipose tissue PDXK in adipogenesis and systemic insulin sensitivity. Diabetologia 2016, 59, 822–832. [Google Scholar] [CrossRef] [Green Version]
- Merigliano, C.; Mascolo, E.; Burla, R.; Saggio, I.; Vernì, F. The relationship between vitamin B6, diabetes and cancer. Front. Genet. 2018, 9, 388. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Shin, A.; Song, D.; Park, J.K.; Kim, Y.; Choi, J.-Y.; Kang, D.; Lee, J.-K. Validity of self-reported cancer history in the health examinees (HEXA) study: A comparison of self-report and cancer registry records. Cancer Epidemiol. 2017, 50, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Balkwill, A.; Bradbury, K.; Reeves, G.K.; Kuan, A.S.; Simpson, R.F.; Green, J.; Beral, V. Foods, macronutrients and breast cancer risk in postmenopausal women: A large UK cohort. Int. J. Epidemiol. 2018, 48, 489–500. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Breast Cancer. 2017. Available online: Wcrf.org/breast-cancer-2017 (accessed on 20 February 2022).
- Hunter, D.J.; Willett, W.C. Nutrition and breast cancer. Cancer Causes Control 1996, 7, 56–68. [Google Scholar] [CrossRef]
- Li, J.; Koh, W.-P.; Jin, A.-Z.; Yuan, J.-M.; Yu, M.C.; Butler, L.M. Calcium intake is not related to breast cancer risk among Singapore Chinese women. Int. J. Cancer 2013, 133, 680–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.-X.; Ho, S.C.; Fu, J.-H.; Cheng, S.-Z.; Chen, Y.-M.; Lin, F.-Y. Dairy products, calcium intake, and breast cancer risk: A Case-Control study in China. Nutr. Cancer 2010, 63, 12–20. [Google Scholar] [CrossRef]
- Chen, P.; Hu, P.; Xie, D.; Qin, Y.; Wang, F.; Wang, H. Meta-analysis of vitamin D, calcium and the prevention of breast cancer. Breast Cancer Res. Treat. 2009, 121, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Adzersen, K.-H.; Jess, P.; Freivogel, K.W.; Gerhard, I.; Bastert, G. Raw and cooked vegetables, fruits, selected micronutrients, and breast cancer risk: A Case-Control study in Germany. Nutr. Cancer 2003, 46, 131–137. [Google Scholar] [CrossRef]
- Park, B.; Lee, J.; Kim, J. Imbalanced nutrient intake in cancer survivors from the examination from the nationwide health examination Center-Based cohort. Nutrients 2018, 10, 212. [Google Scholar] [CrossRef] [Green Version]
- Tayyem, R.F.; Mahmoud, R.I.; Marei, L.S.; Oncologist, K.H.C.C.M. The Intake of Some Nutrients is Associated with the Risk of Breast Cancer: Results from Jordanian Case-Control Study. Curr. Res. Nutr. Food Sci. J. 2020, 8, 12–24. [Google Scholar] [CrossRef]
- Kabat, G.C.; Miller, A.B.; Jain, M.; Rohan, T.E. Dietary iron and heme iron intake and risk of breast cancer: A prospective cohort study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1306–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, A.L.; Espinosa, E.; Calderón, J.M. A case-control study on heme/non-heme iron and breast cancer risk. Ann. Clin. Nutr. 2018, 3, 1011. [Google Scholar]
- Chang, V.C.; Cotterchio, M.; Khoo, E. Iron intake, body iron status, and risk of breast cancer: A systematic review and meta-analysis. BMC Cancer 2019, 19, 543. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J.; Manson, J.E.; Colditz, G.A.; Stampfer, M.J.; Rosner, B.; Hennekens, C.H.; Speizer, F.E.; Willett, W.C. A prospective study of the intake of vitamins C, E, and A and the risk of breast cancer. N. Engl. J. Med. 1993, 329, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Longnecker, M.; Newcomb, P.A.; Mittendorf, R.; Greenberg, E.R.; Willett, W.C. Intake of carrots, spinach, and supplements containing vitamin A in relation to risk of breast cancer. Cancer Epidemiol. Biomark. Prev. 1997, 6, 887–892. [Google Scholar]
- He, J.; Gu, Y.; Zhang, S. Vitamin A and breast cancer survival: A systematic review and meta-analysis. Clin. Breast Cancer 2018, 18, e1389–e1400. [Google Scholar] [CrossRef]
- Egnell, M.; Fassier, P.; Lécuyer, L.; Zelek, L.; Vasson, M.-P.; Hercberg, S.; Latino-Martel, P.; Galan, P.; Deschasaux, M.; Touvier, M. B-vitamin intake from diet and supplements and breast cancer risk in middle-aged women: Results from the prospective NutriNet-Santé cohort. Nutrients 2017, 9, 488. [Google Scholar] [CrossRef] [Green Version]
- Fereidani, S.S.; Eini-Zinab, H.; Heidari, Z.; Jalali, S.; Sedaghat, F.; Rashidkhani, B. Nutrient patterns and risk of breast cancer among Iranian women: A case- control study. Asian Pac. J. Cancer Prev. 2018, 19, 2619–2624. [Google Scholar] [CrossRef] [PubMed]
- Arthur, R.S.; Kirsh, V.A.; Rohan, T.E. Dietary B-Vitamin intake and risk of breast, endometrial, ovarian and colorectal cancer among Canadians. Nutr. Cancer 2019, 71, 1067–1077. [Google Scholar] [CrossRef]
- Yu, L.; Tan, Y.; Zhu, L. Dietary vitamin B2 intake and breast cancer risk: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2016, 295, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, J.; Lentjes, M.A.; Greenwood, D.C.; Burley, V.J.; Cade, J.E.; Cleghorn, C.L.; Threapleton, D.E.; Key, T.J.; Cairns, B.J.; Keogh, R.H.; et al. Vitamin C intake from diary recordings and risk of breast cancer in the UK Dietary Cohort Consortium. Eur. J. Clin. Nutr. 2011, 66, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Rohan, T.E.; Howe, G.R.; Friedenreich, C.M.; Jain, M.; Miller, A.B. Dietary fiber, vitamins A, C, and E, and risk of breast cancer: A cohort study. Cancer Causes Control 1993, 4, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, Y.; Sandsveden, M.; Borgquist, S.; Manjer, J. Serum zinc and dietary intake of zinc in relation to risk of different breast cancer subgroups and serum levels as a marker of intake: A prospective nested case-control study. Breast Cancer Res. Treat. 2021, 189, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Jouybari, L.; Kiani, F.; Akbari, A.; Sanagoo, A.; Sayehmiri, F.; Aaseth, J.; Chartrand, M.S.; Sayehmiri, K.; Chirumbolo, S.; Bjørklund, G. A meta-analysis of zinc levels in breast cancer. J. Trace Elem. Med. Biol. 2019, 56, 90–99. [Google Scholar] [CrossRef]
- Zhang, S.M.; Willett, W.C.; Selhub, J.; Hunter, D.J.; Giovannucci, E.L.; Holmes, M.D.; Colditz, G.A.; Hankinson, S.E. Plasma folate, vitamin B6, vitamin B12, homocysteine, and risk of breast cancer. J. Natl. Cancer Inst. 2003, 95, 373–380. [Google Scholar] [CrossRef]
- Lajous, M.; Lazcano-Ponce, E.; Hernandez-Avila, M.; Willett, W.; Romieu, I. Folate, Vitamin B6, and Vitamin B12 intake and the risk of breast cancer among Mexican women. Cancer Epidemiol. Biomark. Prev. 2006, 15, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.; Li, C.; Li, X.; Li, J.; Chu, R.; Wang, H. Higher dietary folate intake reduces the breast cancer risk: A systematic review and meta-analysis. Br. J. Cancer 2014, 110, 2327–2338. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, J.; Jung, S.Y.; Kim, J. Dietary factors and female breast cancer risk: A prospective cohort study. Nutrients 2017, 9, 1331. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; La Vecchia, C.; de Groh, M.; Negri, E.; Morrison, H.; Mery, L. Dietary cholesterol intake and cancer. Ann. Oncol. 2011, 23, 491–500. [Google Scholar] [CrossRef]
- Garcia-Estevez, L.; Moreno-Bueno, G. Updating the role of obesity and cholesterol in breast cancer. Breast Cancer Res. 2019, 21, 35. [Google Scholar] [CrossRef] [Green Version]


| Characteristic | Total | % | Breast Cancer | p-Value * | |||
|---|---|---|---|---|---|---|---|
| No (n = 40,200) | % | Yes (n = 232) | % | ||||
| Age (years) | |||||||
| 40–49 | 14,187 | 35.1 | 14,083 | 35.0 | 104 | 44.8 | 0.012 |
| 50–59 | 17,471 | 43.2 | 17,392 | 43.3 | 79 | 34.1 | |
| 60–69 | 8409 | 20.8 | 8362 | 20.8 | 47 | 20.3 | |
| ≥70 | 365 | 0.9 | 363 | 0.9 | 2 | 0.8 | |
| Body mass index (kg/m2) | |||||||
| <25 | 29,103 | 72.0 | 28,939 | 72.0 | 164 | 70.7 | 0.855 |
| ≥25 | 11,310 | 27.9 | 11,242 | 27.9 | 68 | 29.3 | |
| Missing | 19 | 0.1 | 19 | 0.1 | 0 | 0 | |
| Diagnosis of benign breast cancer | |||||||
| No | 28,924 | 71.5 | 28,772 | 71.6 | 152 | 65.5 | 0.061 |
| Yes | 2183 | 5.4 | 2164 | 5.4 | 19 | 8.2 | |
| Missing | 9325 | 23.1 | 9264 | 23.0 | 61 | 26.3 | |
| Age at menarche (years) | |||||||
| <15 | 15,082 | 37.3 | 14,981 | 37.3 | 101 | 43.6 | 0.140 |
| ≥15 | 24,468 | 60.5 | 24,341 | 60.6 | 127 | 54.7 | |
| Missing | 882 | 2.2 | 878 | 2.1 | 4 | 1.7 | |
| Menopausal status and age (years) | |||||||
| No | 14,831 | 36.7 | 14,736 | 36.7 | 95 | 41.0 | <0.001 |
| <52 | 15,287 | 37.8 | 15,224 | 37.9 | 63 | 27.2 | |
| ≥52 | 8182 | 20.2 | 8130 | 20.2 | 52 | 22.4 | |
| Missing | 2132 | 5.2 | 2110 | 5.2 | 22 | 9.4 | |
| Breastfeeding | |||||||
| No | 4980 | 12.3 | 4935 | 12.3 | 45 | 19.4 | <0.001 |
| Yes | 33,497 | 82.9 | 33,326 | 82.9 | 171 | 73.7 | |
| Missing | 1955 | 4.8 | 1939 | 4.8 | 16 | 6.9 | |
| Smoking | |||||||
| No | 39,078 | 96.7 | 38,856 | 96.7 | 222 | 95.7 | 0.106 |
| Former | 461 | 1.1 | 455 | 1.1 | 6 | 2.5 | |
| Current | 704 | 1.7 | 702 | 1.8 | 2 | 0.9 | |
| Missing | 189 | 0.5 | 187 | 0.4 | 2 | 0.9 | |
| Drinking | |||||||
| No | 27,635 | 68.4 | 27,473 | 68.3 | 162 | 69.8 | 0.888 |
| Yes | 12,607 | 31.1 | 12,538 | 31.2 | 69 | 29.8 | |
| Missing | 190 | 0.5 | 189 | 0.5 | 1 | 0.4 | |
| Physical activity (min/week) | |||||||
| No | 18,723 | 46.3 | 18,634 | 46.4 | 89 | 38.4 | 0.002 |
| <150 | 4932 | 12.2 | 4910 | 12.2 | 22 | 9.5 | |
| ≥150 | 15,458 | 38.2 | 15,352 | 38.2 | 106 | 45.7 | |
| Missing | 1319 | 3.3 | 1304 | 3.2 | 15 | 6.4 | |
| Family history of breast cancer | |||||||
| No | 6734 | 16.7 | 6701 | 16.7 | 33 | 14.2 | 0.375 |
| Yes | 553 | 1.4 | 548 | 1.4 | 5 | 2.2 | |
| Missing | 33,145 | 81.9 | 32,951 | 81.9 | 194 | 83.6 | |
| Nutrient | Breast Cancer | p-Value * | |||
|---|---|---|---|---|---|
| No (n = 40,200) | Yes (n = 232) | ||||
| N | % | N | % | ||
| Calcium (mg) | |||||
| Mean ± SD | 453.46 ± 250.64 | 481.60 ± 311.53 | 0.171 | ||
| ≤Recommended intake ** | 36,307 | 90.3 | 205 | 88.4 | 0.316 |
| >Recommended intake ** | 3893 | 9.7 | 27 | 11.6 | |
| Phosphorus (mg) | |||||
| Mean ± SD | 870.53 ± 319.01 | 886.96 ± 360.40 | 0.489 | ||
| ≤Recommended intake ** | 6450 | 16.0 | 40 | 17.2 | 0.621 |
| >Recommended intake ** | 33,750 | 84.0 | 192 | 82.8 | |
| Iron (mg) | |||||
| Mean ± SD | 9.83 ± 4.49 | 10.11 ± 5.03 | 0.402 | ||
| ≤Recommended intake ** | 22,514 | 56.0 | 148 | 63.8 | 0.017 |
| >Recommended intake ** | 17,686 | 44.0 | 84 | 36.2 | |
| Potassium(mg) | |||||
| Mean ± SD | 2229.23 ± 990.89 | 2277.75 ± 1077.79 | 0.457 | ||
| ≤Recommended intake ** | 36,382 | 90.5 | 209 | 90.1 | 0.829 |
| >Recommended intake ** | 3818 | 9.5 | 23 | 9.9 | |
| Vitamin A (R.E.) | |||||
| Mean ± SD | 468.86 ± 321.25 | 490.82 ± 361.00 | 0.356 | ||
| ≤Recommended intake ** | 31,664 | 78.8 | 179 | 77.2 | 0.550 |
| >Recommended intake ** | 8536 | 21.2 | 53 | 22.8 | |
| Sodium (mg) | |||||
| Mean ± SD | 2370.63 ± 1319.25 | 2391.46 ± 1387.47 | 0.811 | ||
| ≤Recommended intake ** | 10,764 | 26.8 | 63 | 27.2 | 0.897 |
| >Recommended intake ** | 29,436 | 73.2 | 169 | 72.8 | |
| Vitamin B1 (mg) | |||||
| Mean ± SD | 0.96 ± 0.37 | 0.96 ± 0.39 | 0.795 | ||
| ≤Recommended intake ** | 28,657 | 71.3 | 160 | 69.0 | 0.436 |
| >Recommended intake ** | 11,543 | 28.7 | 72 | 31.0 | |
| Vitamin B2 (mg) | |||||
| Mean ± SD | 0.89 ± 0.41 | 0.92 ± 0.45 | 0.305 | ||
| ≤Recommended intake ** | 32,964 | 82.0 | 184 | 79.3 | 0.288 |
| >Recommended intake ** | 7236 | 18.0 | 48 | 20.7 | |
| Niacin (mg) | |||||
| Mean ± SD | 13.84 ± 5.28 | 13.98 ± 5.66 | 0.692 | ||
| ≤Recommended intake ** | 23,292 | 57.9 | 135 | 58.1 | 0.939 |
| >Recommended intake ** | 16,908 | 42.1 | 97 | 41.9 | |
| Vitamin C (mg) | |||||
| Mean ± SD | 110.51 ± 68.07 | 114.28 ± 76.84 | 0.456 | ||
| ≤Recommended intake ** | 21,115 | 52.5 | 122 | 52.6 | 0.985 |
| >Recommended intake ** | 19,085 | 47.5 | 110 | 47.4 | |
| Zinc (µg) | |||||
| Mean ± SD | 7.65 ± 3.05 | 7.78 ± 3.20 | 0.488 | ||
| ≤Recommended intake ** | 25,007 | 62.2 | 147 | 63.4 | 0.717 |
| >Recommended intake ** | 15,193 | 37.8 | 85 | 36.6 | |
| Vitamin B6 (mg) | |||||
| Mean ± SD | 1.55 ± 0.62 | 1.56 ± 0.64 | 0.746 | ||
| ≤Recommended intake ** | 18,816 | 46.8 | 116 | 50.0 | 0.331 |
| >Recommended intake ** | 21,384 | 53.2 | 116 | 50.0 | |
| Folate (µg) | |||||
| Mean ± SD | 216.96 ± 114.93 | 220.17 ± 116.86 | 0.672 | ||
| ≤Recommended intake ** | 37,554 | 93.4 | 212 | 91.4 | 0.212 |
| >Recommended intake ** | 2646 | 6.6 | 20 | 8.6 | |
| Vitamin E (mg) | |||||
| Mean ± SD | 7.94 ± 3.92 | 8.34 ± 4.14 | 0.121 | ||
| ≤Recommended intake ** | 35,078 | 87.3 | 199 | 85.8 | 0.500 |
| >Recommended intake ** | 5122 | 12.7 | 33 | 14.2 | |
| Cholesterol (mg) | |||||
| Mean ± SD | 161.10 ± 110.61 | 166.87 ± 134.66 | 0.515 | ||
| ≤Recommended intake ** | 19,583 | 48.7 | 113 | 48.7 | 0.998 |
| >Recommended intake ** | 20,617 | 51.3 | 119 | 51.3 | |
| Nutrient | Breast Cancer | ||
|---|---|---|---|
| No. of Events/ Person Year | cHR (95% CI) | aHR * (95% CI) | |
| Calcium (mg) | |||
| ≤Recommended intake ** | 205/177,782 | 1 | 1 |
| >Recommended intake ** | 27/20,390 | 1.17 (0.78–1.75) | 1.12 (0.72–1.76) |
| Phosphorus (mg) | |||
| ≤Recommended intake ** | 40/31,774 | 1 | 1 |
| >Recommended intake ** | 192/166,398 | 0.92 (0.65–1.29) | 0.88 (0.59–1.32) |
| Iron (mg) | |||
| ≤Recommended intake ** | 148/111,063 | 1 | 1 |
| >Recommended intake ** | 84/87,109 | 0.72 (0.55–0.95) | 0.74 (0.52–1.06) |
| Potassium (mg) | |||
| ≤Recommended intake ** | 209/177,987 | 1 | 1 |
| >Recommended intake ** | 23/20,185 | 0.99 (0.65–1.53) | 0.96 (0.59–1.57) |
| Vitamin A (R.E.) | |||
| ≤Recommended intake ** | 179/155,182 | 1 | 1 |
| >Recommended intake ** | 53/42,990 | 1.08 (0.79–1.47) | 1.12 (0.80–1.56) |
| Sodium (mg) | |||
| ≤Recommended intake ** | 63/52,688 | 1 | 1 |
| >Recommended intake ** | 169/145,484 | 0.98 (0.73–1.30) | 0.98 (0.72–1.34) |
| Vitamin B1 (mg) | |||
| ≤Recommended intake ** | 160/140,297 | 1 | 1 |
| >Recommended intake ** | 72/57,875 | 1.10 (0.83–1.45) | 1.14 (0.78–1.66) |
| Vitamin B2 (mg) | |||
| ≤Recommended intake ** | 184/160,930 | 1 | 1 |
| >Recommended intake ** | 48/37,242 | 1.15 (0.83–1.58) | 1.17 (0.80–1.73) |
| Niacin (mg) | |||
| ≤Recommended intake ** | 135/114,543 | 1 | 1 |
| >Recommended intake ** | 97/83,629 | 0.99 (0.76–1.28) | 0.95 (0.67–1.33) |
| Vitamin C (mg) | |||
| ≤Recommended intake ** | 122/102,230 | ||
| >Recommended intake ** | 110/95,942 | 0.97 (0.75–1.26) | 0.95 (0.71–1.26) |
| Zinc (µg) | |||
| ≤Recommended intake ** | 147/122,609 | 1 | 1 |
| >Recommended intake ** | 85/75,563 | 0.94 (0.72–1.23) | 0.89 (0.61–1.28) |
| Vitamin B6 (mg) | |||
| ≤Recommended intake ** | 116/91,707 | 1 | 1 |
| >Recommended intake ** | 116/106,465 | 0.87 (0.67–1.12) | 0.78 (0.56–1.09) |
| Folate (µg) | |||
| ≤Recommended intake ** | 212/184,209 | 1 | 1 |
| >Recommended intake ** | 20/13,963 | 1.27 (0.81–2.01) | 1.32 (0.80–2.19) |
| Vitamin E (mg) | |||
| ≤Recommended intake ** | 199/171,659 | 1 | 1 |
| >Recommended intake ** | 33/26,513 | 1.09 (0.76–1.58) | 1.07 (0.69–1.66) |
| Cholesterol (mg) | |||
| ≤Recommended intake ** | 113/99,875 | 1 | 1 |
| >Recommended intake ** | 119/98,297 | 1.03 (0.79–1.33) | 1.11 (0.83–1.49) |
| Nutrient | BMI < 25 kg/m2 | BMI ≥ 25 kg/m2 | ||
|---|---|---|---|---|
| cHR (95% CI) | aHR * (95% CI) | cHR (95% CI) | aHR * (95% CI) | |
| >Recommended Intake (Reference: ≤Recommended Intake) ** | ||||
| Calcium (mg) | 1.00 (0.61–1.66) | 0.93 (0.53–1.62) | 1.64 (0.84–3.22) | 1.60 (0.74–3.47) |
| Phosphorus (mg) | 0.83 (0.56–1.23) | 0.74 (0.46–1.18) | 1.21 (0.60–2.45) | 1.34 (0.60–2.97) |
| Iron (mg) | 0.69 (0.50–0.96) | 0.68 (0.44–1.04) | 0.78 (0.48–1.27) | 0.90 (0.48–1.70) |
| Potassium (mg) | 0.98 (0.58–1.64) | 0.94 (0.53–1.69) | 1.03 (0.47–2.26) | 0.93 (0.38–2.31) |
| Vitamin A (R.E.) | 1.05 (0.73–1.52) | 1.09 (0.72–1.63) | 1.13 (0.66–1.96) | 1.17 (0.63–2.14) |
| Sodium (mg) | 1.01 (0.71–1.42) | 1.01 (0.70–1.47) | 0.90 (0.52–1.54) | 0.89 (0.50–1.58) |
| Vitamin B1 (mg) | 1.15 (0.83–1.59) | 1.23 (0.79–1.92) | 0.99 (0.59–1.67) | 0.97 (0.48–1.96) |
| Vitamin B2 (mg) | 1.15 (0.79–1.67) | 1.18 (0.74–1.88) | 1.14 (0.63–2.05) | 1.13 (0.55–2.35) |
| Niacin (mg) | 1.04 (0.76–1.42) | 1.02 (0.68–1.54) | 0.87 (0.53–1.41) | 0.80 (0.42–1.52) |
| Vitamin C (mg) | 1.18 (0.87–1.61) | 1.19 (0.85–1.67) | 0.60 (0.36–0.99) | 0.53 (0.30–0.92) |
| Zinc (µg) | 0.97 (0.71–1.34) | 0.93 (0.60–1.43) | 0.88 (0.53–1.44) | 0.79 (0.40–1.56) |
| Vitamin B6 (mg) | 1.01 (0.74–1.37) | 0.98 (0.66–1.45) | 0.61 (0.37–0.98) | 0.45 (0.24–0.86) |
| Folate (µg) | 1.25 (0.73–2.17) | 1.29 (0.71–2.36) | 1.31 (0.57–3.03) | 1.25 (0.49–3.19) |
| Vitamin E (mg) | 1.11 (0.72–1.72) | 1.08 (0.64–1.82) | 1.05 (0.52–2.11) | 0.98 (0.42–2.30) |
| Cholesterol (mg) | 0.96 (0.71–1.31) | 1.04 (0.73–1.47) | 1.19 (0.73–1.92) | 1.31 (0.76–2.26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, H.; Jeong, A.; Tran, T.X.M.; Lee, J.; Kim, M.; Park, B. Association between Micronutrient Intake and Breast Cancer Risk According to Body Mass Index in South Korean Adult Women: A Cohort Study. Nutrients 2022, 14, 2644. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14132644
Song H, Jeong A, Tran TXM, Lee J, Kim M, Park B. Association between Micronutrient Intake and Breast Cancer Risk According to Body Mass Index in South Korean Adult Women: A Cohort Study. Nutrients. 2022; 14(13):2644. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14132644
Chicago/Turabian StyleSong, Huiyeon, Ansun Jeong, Thi Xuan Mai Tran, Jiseon Lee, Mikyung Kim, and Boyoung Park. 2022. "Association between Micronutrient Intake and Breast Cancer Risk According to Body Mass Index in South Korean Adult Women: A Cohort Study" Nutrients 14, no. 13: 2644. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14132644