
No Difference in Tolerance between Wheat and Spelt Bread in Patients with Suspected Non-Celiac Wheat Sensitivity

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Breads
2.3. Study Design and Intervention
2.4. Questionnaire-Based Symptom Evaluation
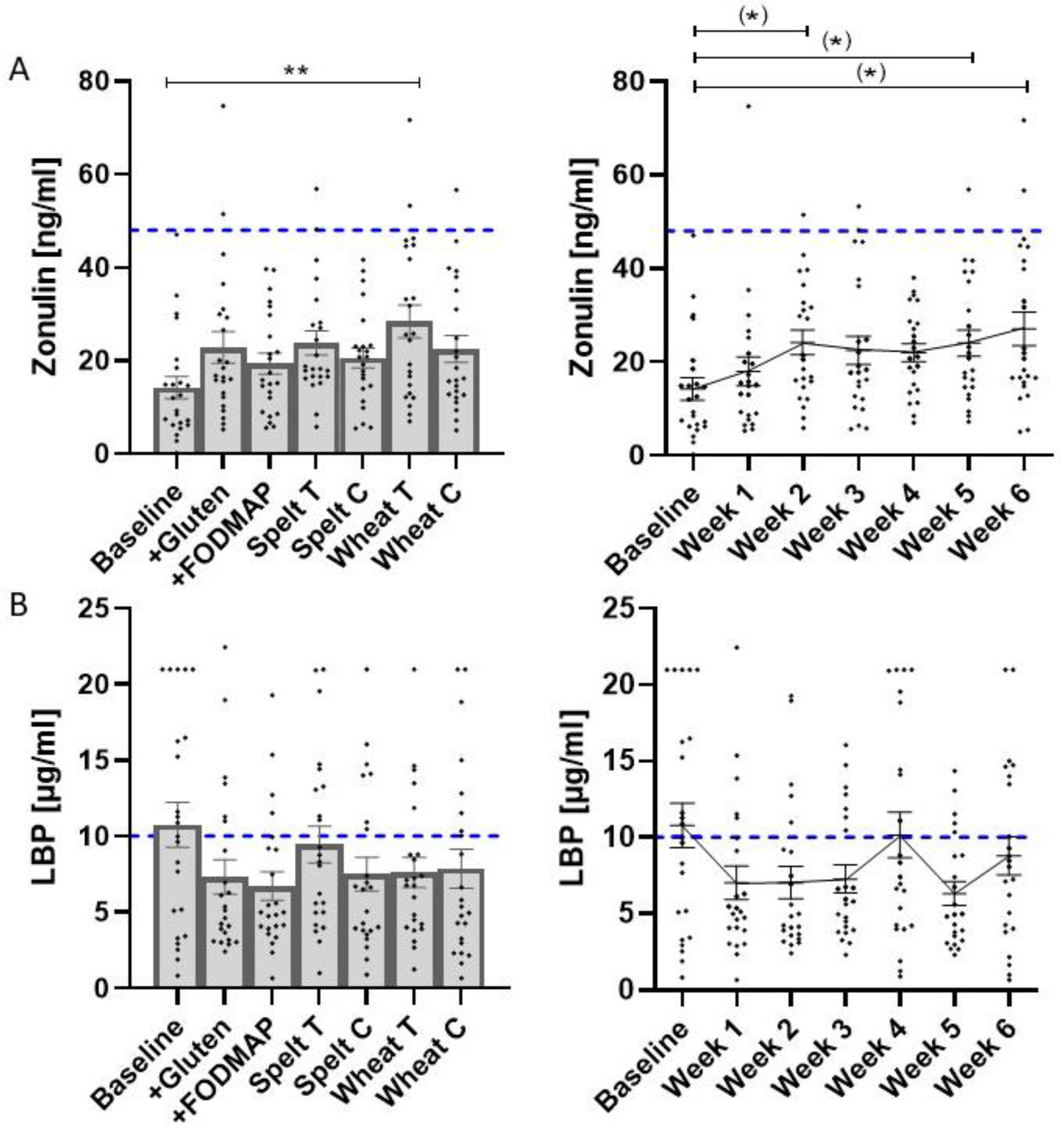
2.5. Analysis of Fecal and Serum Markers of Intestinal Permeability and Inflammation
2.6. Short-Chain Fatty Acids Analysis from Fecal Samples
2.7. Sample Size Calculation and Statistics
2.8. Compliance Testing
2.9. Ethics and Approvals
3. Results
3.1. Recruitment
3.2. Baseline Data
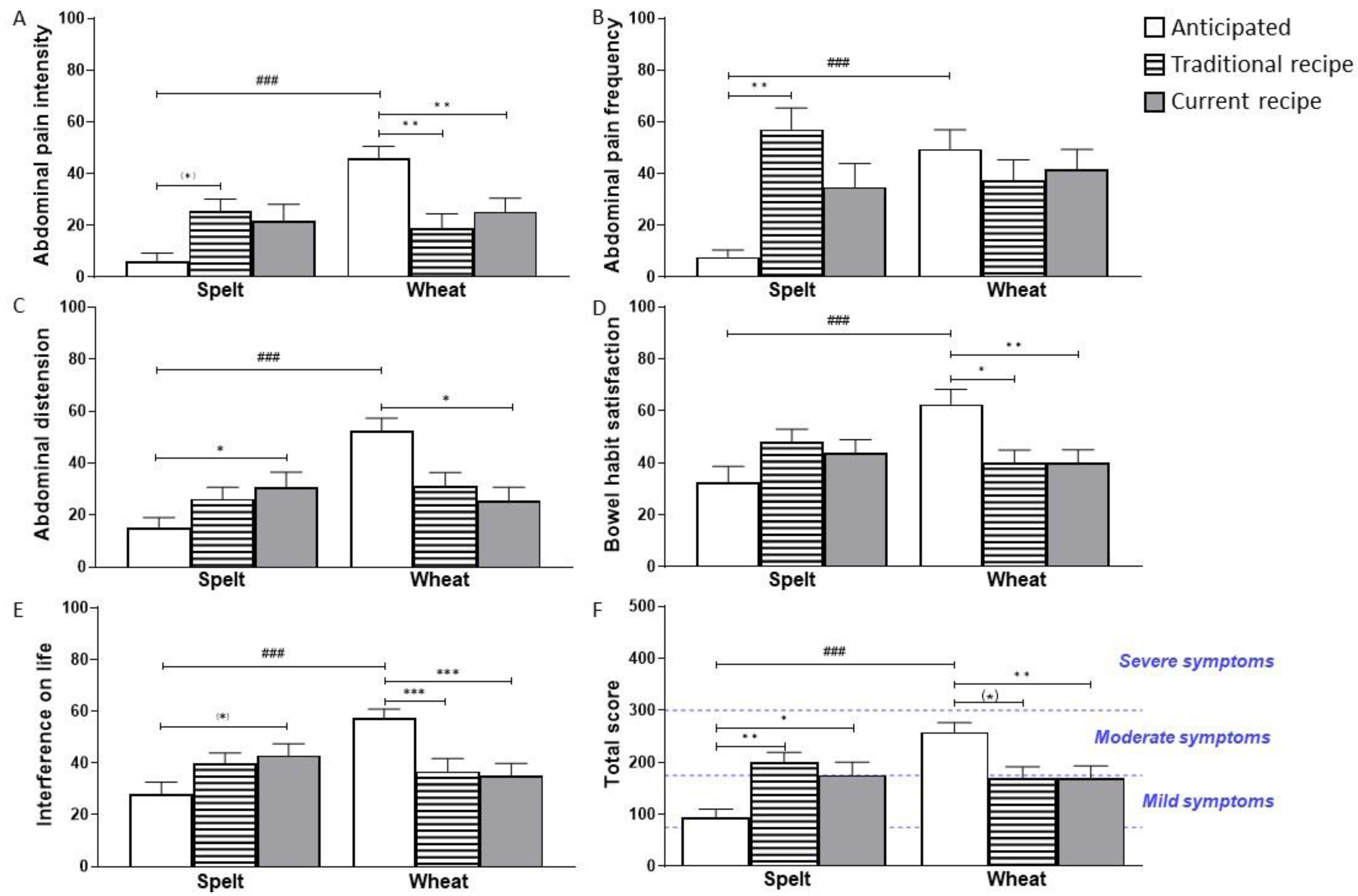
3.3. Primary Outcome
3.4. Secondary Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fasano, A.; Berti, I.; Gerarduzzi, T.; Not, T.; Colletti, R.B.; Drago, S.; Elitsur, Y.; Green, P.H.R.; Guandalini, S.; Hill, I.D.; et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch. Intern. Med. 2003, 163, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Gilissen, L.J.W.J.; van der Meer, I.M.; Smulders, M.J.M. Reducing the incidence of allergy and intolerance to cereals. J. Cereal Sci. 2014, 59, 337–353. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Santolaria, S.; Sanders, D.S.; Fernández-Bañares, F. Systematic review: Noncoeliac gluten sensitivity. Aliment. Pharmacol. Ther. 2015, 41, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Uhde, M.; Ajamian, M.; Caio, G.; De Giorgio, R.; Indart, A.; Green, P.H.; Verna, E.C.; Volta, U.; Alaedini, A. Intestinal cell damage and systemic immune activation in individuals reporting sensitivity to wheat in the absence of coeliac disease. Gut 2016, 65, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Sapone, A.; Lammers, K.M.; Casolaro, V.; Cammarota, M.; Giuliano, M.T.; De Rosa, M.; Stefanile, R.; Mazzarella, G.; Tolone, C.; Russo, M.I.; et al. Divergence of gut permeability and mucosal immune gene expression in two gluten-associated conditions: Celiac disease and gluten sensitivity. BMC Med. 2011, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Elli, L.; Tomba, C.; Branchi, F.; Roncoroni, L.; Lombardo, V.; Bardella, M.T.; Ferretti, F.; Conte, D.; Valiante, F.; Fini, L.; et al. Evidence for the Presence of Non-Celiac Gluten Sensitivity in Patients with Functional Gastrointestinal Symptoms: Results from a Multicenter Randomized Double-Blind Placebo-Controlled Gluten Challenge. Nutrients 2016, 8, 84. [Google Scholar] [CrossRef]
- Skodje, G.I.; Sarna, V.K.; Minelle, I.H.; Rolfsen, K.L.; Muir, J.G.; Gibson, P.R.; Veierød, M.B.; Henriksen, C.; Lundin, K.E.A. Fructan, Rather Than Gluten, Induces Symptoms in Patients with Self-Reported Non-Celiac Gluten Sensitivity. Gastroenterology 2018, 154, 529–539. [Google Scholar] [CrossRef] [Green Version]
- Zevallos, V.F.; Raker, V.; Tenzer, S.; Jimenez-Calvente, C.; Ashfaq-Khan, M.; Rüssel, N.; Pickert, G.; Schild, H.; Steinbrink, K.; Schuppan, D. Nutritional Wheat Amylase-Trypsin Inhibitors Promote Intestinal Inflammation via Activation of Myeloid Cells. Gastroenterology 2017, 152, 1100–1113. [Google Scholar] [CrossRef] [Green Version]
- Vu, N.; Chin, J.; Pasco, J.A.; Kovacs, A.; Wing, L.W.; Békés, F.; Suter, D.A.I. The prevalence of wheat and spelt sensitivity in a randomly selected Australian population. Cereal Res. Commun. 2015, 43, 97–107. [Google Scholar] [CrossRef] [Green Version]
- van Gils, T.; Nijeboer, P.; IJssennagger, C.E.; Sanders, D.S.; Mulder, C.J.J.; Bouma, G. Faculty Opinions recommendation of Prevalence and Characterization of Self-Reported Gluten Sensitivity in The Netherlands. Nutrients 2018, 8, 714. [Google Scholar] [CrossRef] [Green Version]
- Schober, T.J.; Clarke, C.I.; Kühn, M. Characterization of Functional Properties of Gluten Proteins in Spelt Cultivars Using Rheological and Quality Factor Measurements. Cereal Chem. 2002, 79, 408–417. [Google Scholar] [CrossRef]
- Pruska-Kedzior, A.; Kedzior, Z.; Klockiewicz-Kaminska, E. Comparison of viscoelastic properties of gluten from spelt and common wheat. Eur. Food Res. Technol. 2008, 227, 199–207. [Google Scholar] [CrossRef]
- Afzal, M.; Pfannstiel, J.; Zimmermann, J.; Bischoff, S.C.; Würschum, T.; Longin, C.F.H. High-resolution proteomics reveals differences in the proteome of spelt and bread wheat flour representing targets for research on wheat sensitivities. Sci. Rep. 2020, 10, 14677. [Google Scholar] [CrossRef]
- Ziegler, J.U.; Steiner, D.; Longin, C.F.H.; Würschum, T.; Schweiggert, R.M.; Carle, R. Wheat and the irritable bowel syndrome—FODMAP levels of modern and ancient species and their retention during bread making. J. Funct. Foods 2016, 25, 257–266. [Google Scholar] [CrossRef]
- Longin, C.F.H.; Beck, H.; Gütler, A.; Gütler, H.; Heilig, W.; Zimmermann, J.; Bischoff, S.C.; Würschum, T. Influence of wheat variety and dough preparation on FODMAP content in yeast-leavened wheat breads. J. Cereal Sci. 2020, 95, 103021. [Google Scholar] [CrossRef]
- Zimmermann, J.; Hubel, P.; Pfannstiel, J.; Afzal, M.; Longin, C.F.H.; Hitzmann, B.; Götz, H.; Bischoff, S.C. Comprehensive proteome analysis of bread deciphering the allergenic potential of bread wheat, spelt and rye. J. Proteom. 2021, 247, 104318. [Google Scholar] [CrossRef]
- El Mecherfi, K.-E.; Todorov, S.D.; Cavalcanti de Albuquerque, M.A.; Denery-Papini, S.; Lupi, R.; Haertlé, T.; Dora Gombossy de Melo Franco, B.; Larré, C. Allergenicity of Fermented Foods: Emphasis on Seeds Protein-Based Products. Foods 2020, 9, 792. [Google Scholar] [CrossRef]
- Davis, P.J.; Smales, C.M.; James, D.C. How can thermal processing modify the antigenicity of proteins? Allergy 2001, 56 (Suppl. 67), 56–60. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Reese, I.; Schäfer, C.; Kleine-Tebbe, J.; Ahrens, B.; Bachmann, O.; Ballmer-Weber, B.; Beyer, K.; Bischoff, S.C.; Blümchen, K.; Dölle, S.; et al. Non-celiac gluten/wheat sensitivity (NCGS)-a currently undefined disorder without validated diagnostic criteria and of unknown prevalence: Position statement of the task force on food allergy of the German Society of Allergology and Clinical Immunology (DGAKI). Allergo J. Int. 2018, 27, 147–151. [Google Scholar]
- van Overbeek, F.M.; Uil-Dieterman, I.G.; Mol, I.W.; Köhler-Brands, L.; Heymans, H.S.; Mulder, C.J. The daily gluten intake in relatives of patients with coeliac disease compared with that of the general Dutch population. Eur. J. Gastroenterol. Hepatol. 1997, 9, 1097–1099. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The Brief Illness Perception Questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Seethaler, B.; Basrai, M.; Neyrinck, A.M.; Nazare, J.-A.; Walter, J.; Delzenne, N.M.; Bischoff, S.C. Biomarkers for assessment of intestinal permeability in clinical practice. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 321, G11–G17. [Google Scholar] [CrossRef] [PubMed]
- Stiefvatter, L.; Lehnert, K.; Frick, K.; Montoya-Arroyo, A.; Frank, J.; Vetter, W.; Schmid-Staiger, U.; Bischoff, S.C. Oral Bioavailability of Omega-3 Fatty Acids and Carotenoids from the Microalgae Phaeodactylum tricornutum in Healthy Young Adults. Mar. Drugs 2021, 19, 700. [Google Scholar] [CrossRef]
- Böhn, L.; Störsrud, S.; Liljebo, T.; Collin, L.; Lindfors, P.; Törnblom, H.; Simrén, M. Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome as Well as Traditional Dietary Advice: A Randomized Controlled Trial. Gastroenterology 2015, 149, 1399–1407. [Google Scholar] [CrossRef] [Green Version]
- Comino, I.; Real, A.; Vivas, S.; Síglez, M.Á.; Caminero, A.; Nistal, E.; Casqueiro, J.; Rodríguez-Herrera, A.; Cebolla, A.; Sousa, C. Monitoring of gluten-free diet compliance in celiac patients by assessment of gliadin 33-mer equivalent epitopes in feces. Am. J. Clin. Nutr. 2012, 95, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Aziz, I.; Lewis, N.R.; Hadjivassiliou, M.; Winfield, S.N.; Rugg, N.; Kelsall, A.; Newrick, L.; Sanders, D.S. A UK study assessing the population prevalence of self-reported gluten sensitivity and referral characteristics to secondary care. Eur. J. Gastroenterol. Hepatol. 2014, 26, 33–39. [Google Scholar] [CrossRef]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, J.; De Fazio, L.; Kaden-Volynets, V.; Hitzmann, B.; Bischoff, S.C. Consumption of Yeast-Fermented Wheat and Rye Breads Increases Colitis and Mortality in a Mouse Model of Colitis. Dig. Dis. Sci. 2022, 1–12. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Carroccio, A. Suspected Nonceliac Gluten Sensitivity Confirmed in Few Patients After Gluten Challenge in Double-Blind, Placebo-Controlled Trials. Clin. Gastroenterol. Hepatol. 2017, 15, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Tovoli, F.; Granito, A.; Negrini, G.; Guidetti, E.; Faggiano, C.; Bolondi, L. Long term effects of gluten-free diet in non-celiac wheat sensitivity. Clin. Nutr. 2019, 38, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Prandi, B.; Tedeschi, T.; Folloni, S.; Galaverna, G.; Sforza, S. Peptides from gluten digestion: A comparison between old and modern wheat varieties. Food Res. Int. 2017, 91, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Varney, J.; Barrett, J.; Scarlata, K.; Catsos, P.; Gibson, P.R.; Muir, J.G. FODMAPs: Food composition, defining cutoff values and international application. J. Gastroenterol. Hepatol. 2017, 32 (Suppl. 1), 53–61. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Not, T.; Wang, W.; Uzzau, S.; Berti, I.; Tommasini, A.; Goldblum, S.E. Zonulin, a newly discovered modulator of intestinal permeability, and its expression in coeliac disease. Lancet 2000, 355, 1518–1519. [Google Scholar] [CrossRef]
- Høverstad, T.; Midtvedt, T.; Bøhmer, T. Short-Chain Fatty Acids in Intestinal Content of Germfree Mice Monocontaminated with Escherichia Coli or Clostridium Difficile. Scand. J. Gastroenterol. 1985, 20, 373–380. [Google Scholar] [CrossRef]
- Zheng, W.; Wang, K.; Sun, Y.; Kuo, S.-M. Dietary or supplemental fermentable fiber intake reduces the presence of Clostridium XI in mouse intestinal microbiota: The importance of higher fecal bacterial load and density. PLoS ONE 2018, 13, e0205055. [Google Scholar] [CrossRef]
- Sethi, A.; Eggers, S.; Mares, J.; Christensen, K.; Gangnon, R.; Suen, G.; Watson, L.; Shirley, D.; Shukla, S.; Poulsen, K.; et al. 2582. The Association Between Dietary Fiber and Diet and Gut Colonization with Clostridium difficile. Open Forum Infect. Dis. 2019, 6, S897. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Volta, U.; Salvatore, C.; Biancheri, P.; Caio, G.; de Giorgio, R.; Di Stefano, M.; Corazza, G.R. Small Amounts of Gluten in Subjects with Suspected Nonceliac Gluten Sensitivity: A Randomized, Double-Blind, Placebo-Controlled, Cross-Over Trial. Clin. Gastroenterol. Hepatol. 2018, 13, 1604–1612.e3. [Google Scholar] [CrossRef]
- Dale, H.F.; Hatlebakk, J.G.; Hovdenak, N.; Ystad, S.O.; Lied, G.A. The effect of a controlled gluten challenge in a group of patients with suspected non-coeliac gluten sensitivity: A randomized, double-blind placebo-controlled challenge. Neurogastroenterol. Motil. 2018, 30, e13332. [Google Scholar] [CrossRef]
- Brottveit, M.; Beitnes, A.-C.R.; Tollefsen, S.; Bratlie, J.E.; Jahnsen, F.L.; Johansen, F.-E.; Sollid, L.M.; Lundin, K.E.A. Mucosal Cytokine Response After Short-Term Gluten Challenge in Celiac Disease and Non-Celiac Gluten Sensitivity. Am. J. Gastroenterol. 2013, 108, 842–850. [Google Scholar] [CrossRef]
- Bascuñán, K.A.; Roncoroni, L.; Branchi, F.; Doneda, L.; Scricciolo, A.; Ferretti, F.; Araya, M.; Elli, L. The 5 Ws of a gluten challenge for gluten-related disorders. Nutr. Rev. 2018, 76, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bread | Description | Ingredients |
|---|---|---|
| Bread for washout-phase | ||
| GF bread | Gluten-free bread based on a mixture (Dietary Food Solutions, Lana, Italy) | Corn starch, flaxseed flour, buckwheat flour, vegetable fibers (psyllium, apple, sugar beet, rice, pea), salt, rice sourdough, sugar, thickener (E464, pea protein, spices and alpha amylase) |
| Study breads | ||
| +Gluten | GF bread supplemented with wheat gluten (Loryma GmbH, Zwingenberg, Germany) | Corn starch, flaxseed flour, buckwheat flour, vegetable fibers, salt, rice sourdough, sugar, thickener + 5% Wheat gluten |
| +FODMAP | GF bread supplemented with oligofructose (Beneo GmbH, Mannheim, Germany) | Corn starch, flaxseed flour, buckwheat flour, vegetable fibers, salt, rice sourdough, sugar, thickener + 1.5% Orafti®P95 |
| Spelt T | Spelt bread produced according to a traditional recipe | Spelt flour (Type 630), water, yeast, salt; fermentation for 16 h at 4 °C |
| Spelt C | Spelt bread produced according to a current recipe with bread improver | Spelt flour (Type 630); water, yeast, bread improver (Schapfenmühle, Ulm, Germany), salt; fermentation for 1 h at 20 °C |
| Wheat T | Wheat bread produced according to a traditional recipe | Wheat flour (Type 550); water, yeast, salt; fermentation for 16 h at 4 °C |
| Wheat C | Wheat bread produced according to a current recipe with bread improver | Wheat flour (Type 550); water, yeast, bread improver (Schapfenmühle, Ulm, Germany), salt; fermentation for 1 h at 20 °C |
| Parameter | Proportion of Study Participants |
|---|---|
| Female/male | 23/1 |
| Age (y), SD | 42 (±14.1) |
| Mean body mass index (kg/m2), SD | 24.8 (±6.8) |
| IBS by Rome IV criteria (%) | 67 |
| Previous gastroscopy (%) | 38 |
| Other food allergy/intolerance (%) | 54 |
| Family member with celiac disease (%) | 0 |
| Time until onset of symptoms (h) | 0–24 (Ø 5.6) |
| Duration of symptoms (h) | 0.5–72 (Ø 19.2) |
| Main symptoms after wheat consumption | |
| Abdominal pain (%) | 38 |
| Bloating (%) | 71 |
| Bowel habit abnormalities (%) | 75 |
| Systemic manifestations (%) | 71 |
| Baseline | +Gluten | +FODMAP | Spelt Bread T | Spelt Bread C | Wheat Bread T | Wheat Bread C | Wash Out Ø | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Abdominal pain intensity (max. 100) | 18.8 ± 4.0 | 22.2 ± 5.9 | 14.8 ± 4.5 | 25.7 ± 3.9 | 21.9 ± 5.5 | 19.1 ± 5.0 | 25.4 ± 4.8 | 15.1 ± 2.3 | n.s. |
| Abdominal pain frequency (max. 100) | 29.1 ± 5.3 | 42.7 ± 8.1 | 37.3 ± 8.3 | 57.1 ± 8.3 | 34.8 ± 9.1 | 37.3 ± 8.1 | 41.8 ± 7.5 | 34.1 ± 4.6 | n.s. |
| Abdominal distension (max. 100) | 32.9 ± 4.8 | 34.1 ± 5.9 | 25.0 ± 5.6 | 27.2 ± 4.4 | 30.7 ± 5.5 | 31.5 ± 4.8 | 27.1 ± 5.3 | 22.3 ± 2.4 | n.s. |
| Dissatisfaction of bowel habit (max. 100) | 46.6 ± 4.7 | 40.0 ± 5.1 | 38.3 ± 5.1 | 48.5 ± 4.7 | 44.2 ± 4.8 | 40.9 ± 4.6 | 40.4 ± 4.7 | 36.0 ± 2.7 | n.s. |
| Interference on life in general (max. 100) | 46.5 ± 3.9 | 39.1 ± 4.1 | 35.9 ± 5.1 | 39.7 ± 3.9 | 43.5 ± 4.4 | 37.7 ± 4.7 | 35.8 ± 4.6 | 31.3 ± 3.0 | n.s. |
| IBS-SSS total score (max. 500) | 176.3 ± 18.1 | 177.2 ± 24.8 | 149.4 ± 23.5 | 198.7 ± 18.8 | 177.7 ± 25.7 | 165.0 ± 23.1 | 167.3 ± 23.4 | 135.7 ± 17.8 | n.s. |
| Fecal SCFA (n = 24) | |||||||
|---|---|---|---|---|---|---|---|
| µmol/g DM | Baseline | Week 4 | Week 6 | p-Value | Spelt | Wheat | p-Value |
| Total SCFA | 476.7 ± 362.5 | 462.5 ± 327.8 | 512.9 ± 442.1 | n.s. | 486.8 ± 38.2 | 488.6 ± 334.8 | n.s. |
| Acetic acid | 314.0 ± 244.4 | 285.6 ± 95.6 | 326.0 ± 290.6 | n.s. | 306.0 ± 284.5 | 305.9 ± 206.5 | n.s. |
| Propionic acid | 72.0 ± 56.3 | 80.5 ± 67.0 | 86.9 ± 89.0 | n.s. | 82.4 ± 88.0 | 85.0 ± 85.0 | n.s. |
| Iso-butyric acid | 7.6 ± 3.1 | 9.7 ± 7.5 | 8.7 ± 4.9 | n.s. | 8.6 ± 4.1 | 9.82 ± 8.0 | n.s. |
| Butyric acid | 60.8 ± 61.0 | 59.3 ± 49.6 | 64.0 ± 55.0 | n.s. | 63.5 ± 61.1 | 59.8 ± 41.8 | n.s. |
| Iso-valeric acid | 10.2 ± 4.6 | 13.2 ± 10.7 | 11.1 ± 6.1 | n.s. | 11.3 ± 5.2 | 12.9 ± 11.2 | n.s. |
| Valeric acid | 8.3 ± 3.6 | 9.6 ± 9.1 | 10.3 ± 10.8 | n.s. | 10.1 ± 10.8 | 9.7 ± 9.2 | n.s. |
| Iso-Caproic acid | 0.6 ± 0.8 (a)/(c) | 0.7 ± 0.6 (a) | 1.2 ± 1.2 (b) | 0.013 * | 0.8 ± 2.2 (c) | 1.2 ± 1.2 (d) | 0.020 * |
| Hexanoic acid | 2.8 ± 2.4 | 3.1 ± 4.5 | 3.8 ± 5.5 | n.s. | 3.3 ± 5.6 | 3.6 ± 4.4 | n.s. |
| Heptanoic acid | 0.5 ± 0.4 | 0.7 ± 0.7 | 0.6 ± 0.8 | n.s. | 0.7 ± 0.8 | 0.6 ± 0.7 | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimmermann, J.; Longin, F.H.; Schweinlin, A.; Basrai, M.; Bischoff, S.C. No Difference in Tolerance between Wheat and Spelt Bread in Patients with Suspected Non-Celiac Wheat Sensitivity. Nutrients 2022, 14, 2800. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142800
Zimmermann J, Longin FH, Schweinlin A, Basrai M, Bischoff SC. No Difference in Tolerance between Wheat and Spelt Bread in Patients with Suspected Non-Celiac Wheat Sensitivity. Nutrients. 2022; 14(14):2800. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142800
Chicago/Turabian StyleZimmermann, Julia, Friedrich H. Longin, Anna Schweinlin, Maryam Basrai, and Stephan C. Bischoff. 2022. "No Difference in Tolerance between Wheat and Spelt Bread in Patients with Suspected Non-Celiac Wheat Sensitivity" Nutrients 14, no. 14: 2800. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142800