
Real-World Data of a Group-Based Formula Low Energy Diet Programme in Achieving Type 2 Diabetes Remission and Weight Loss in an Ethnically Diverse Population in the UK: A Service Evaluation

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Practitioner Training
2.2. Participant Population, Screening and Referral
2.3. Recruitment
2.4. LED Programme
2.5. LED TDR Phase (12 Weeks)
2.6. Food Reintroduction Phase (9 Weeks)
2.7. Weight Loss Maintenance (31 Weeks)
2.8. Rescue Plan
2.9. Physical Activity Recommendations
2.10. Medical Supervision and Psychological Support
2.11. Outcomes
2.12. Data Collection
2.13. Statistical Analysis
2.14. Ethics
3. Results
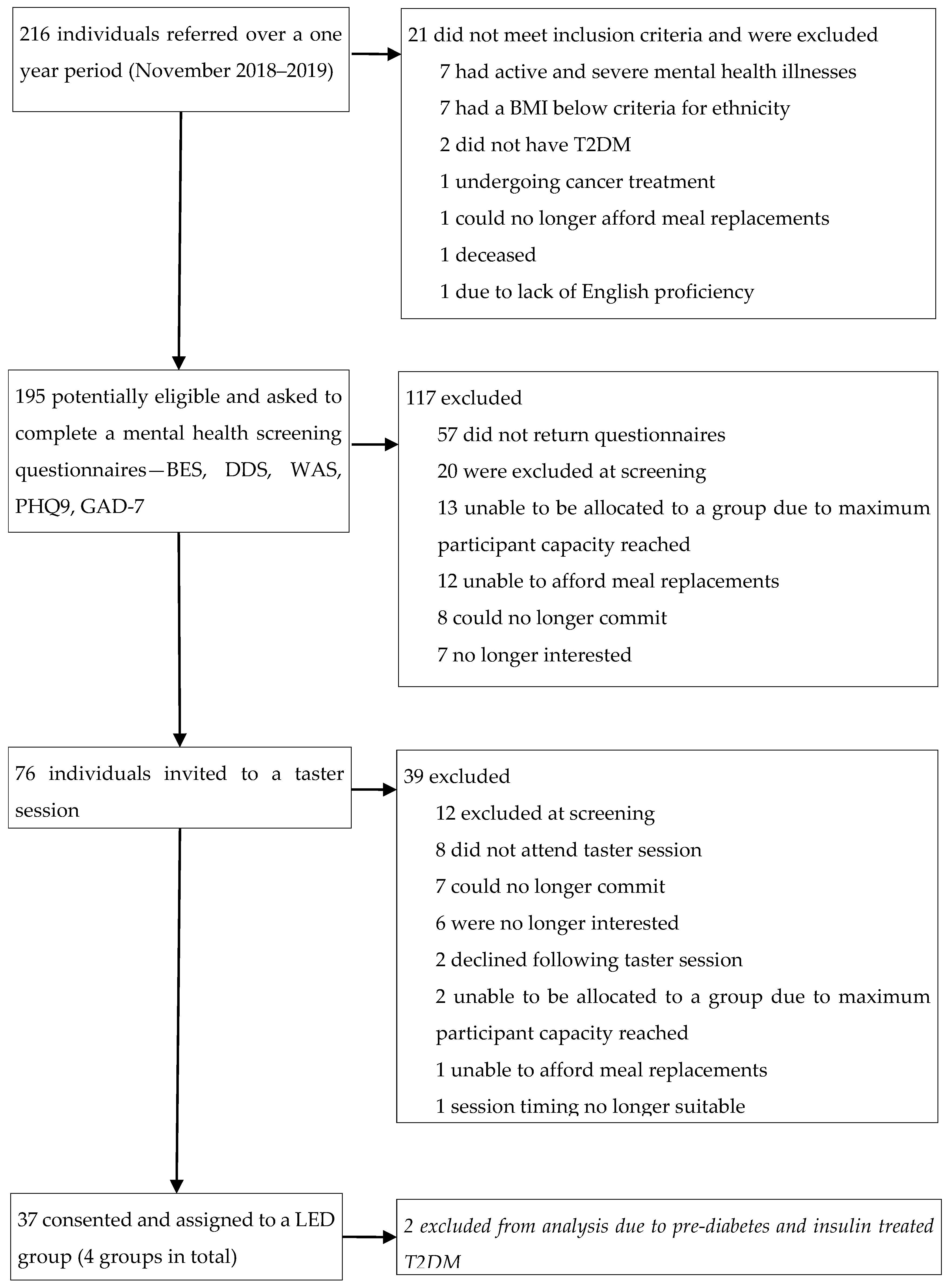
3.1. Referrals and Participants
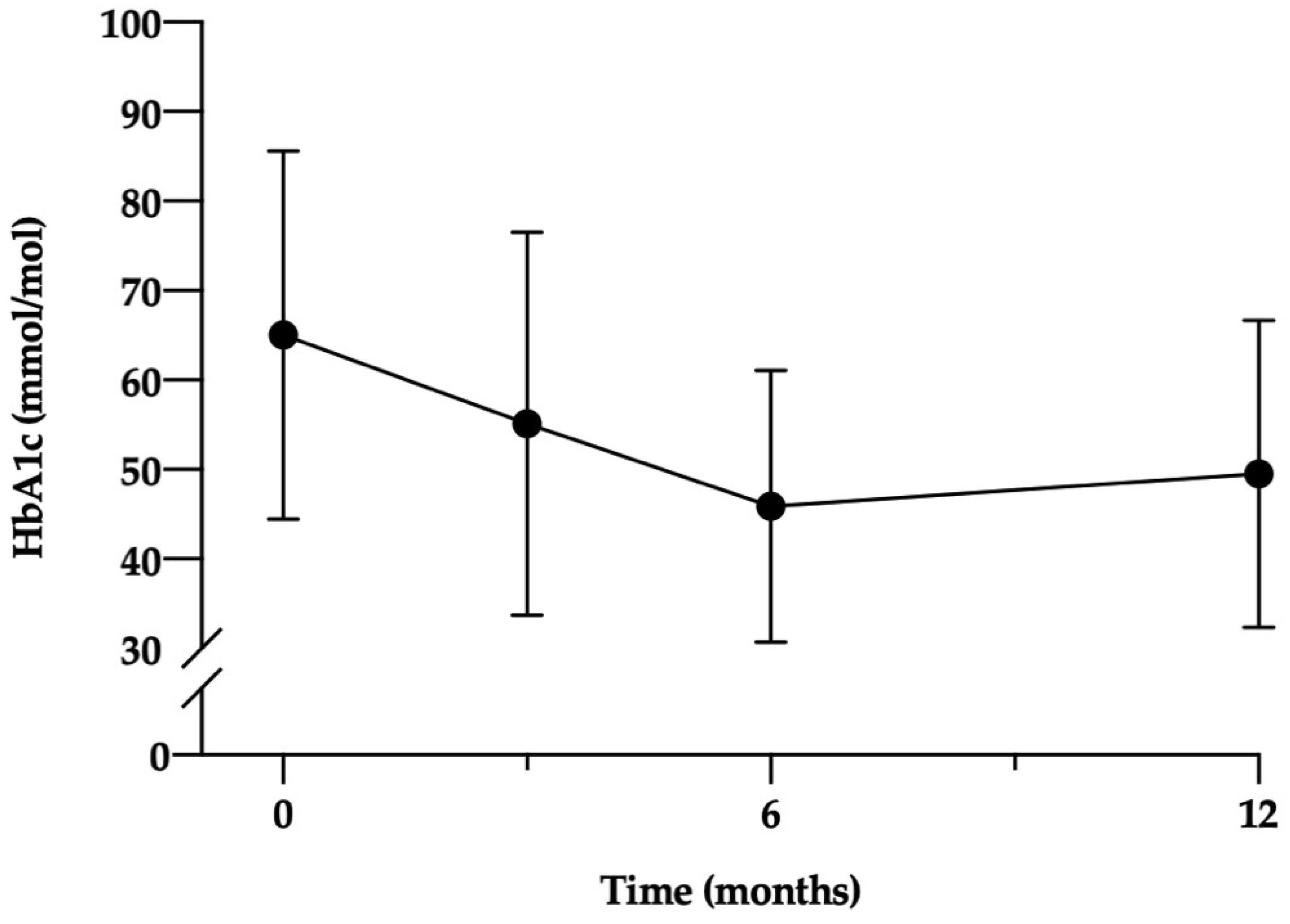
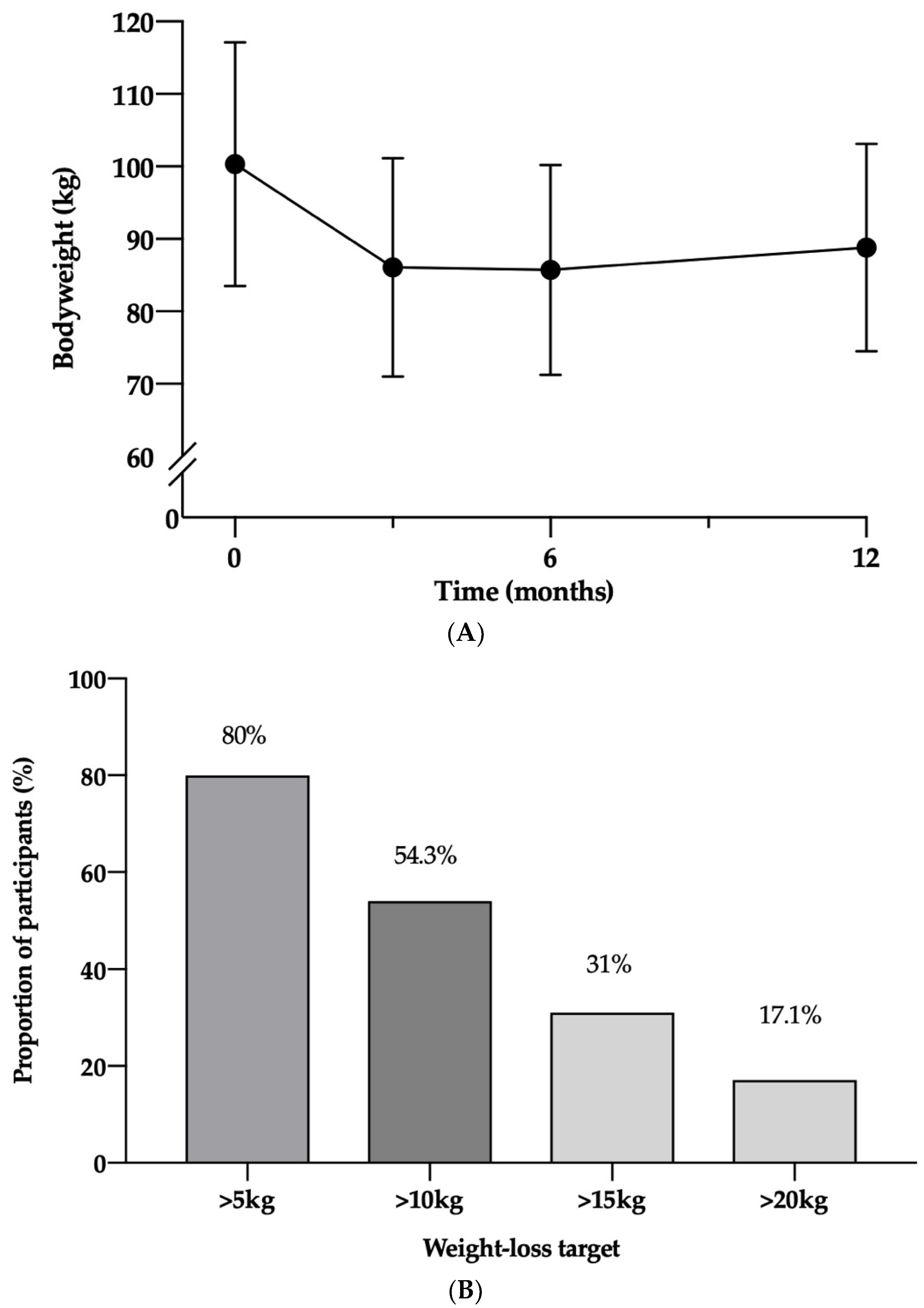
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diabetes UK. Diabetes UK Number of People with Diabetes Reaches 4.7 Million. Available online: https://www.diabetes.org.uk/about_us/news/new-stats-people-living-with-diabetes (accessed on 5 November 2020).
- International Diabetes Federation Worldwide Toll of Diabetes. Available online: https://www.diabetesatlas.org/en/sections/worldwide-toll-of-diabetes.html (accessed on 5 November 2020).
- Goff, L.M. Ethnicity and Type 2 Diabetes in the UK. Diabet. Med. 2019, 36, 927–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khunti, K.; Singh, A.K.; Pareek, M.; Hanif, W. Is Ethnicity Linked to Incidence or Outcomes of COVID-19? BMJ 2020, 369, m1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ONS 2011 Census Data-Office for National Statistics. Available online: https://www.ons.gov.uk/census/2011census/2011censusdata (accessed on 6 November 2020).
- City and Hackney Public Health Team Joint Strategic Needs Assessment: Adult Health and Diabetes. Available online: https://hackneyjsna.org.uk/wp-content/uploads/2018/12/Diabetes-1.pdf (accessed on 18 November 2021).
- Pham, T.M.; Carpenter, J.R.; Morris, T.P.; Sharma, M.; Petersen, I. Ethnic Differences in the Prevalence of Type 2 Diabetes Diagnoses in the Uk: Cross-Sectional Analysis of the Health Improvement Network Primary Care Database. Clin. Epidemiol. 2019, 11, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Brown, A.; McArdle, P.; Taplin, J.; Unwin, D.; Unwin, J.; Deakin, T.; Wheatley, S.; Murdoch, C.; Malhotra, A.; Mellor, D. Dietary Strategies for Remission of Type 2 Diabetes: A Narrative Review. J. Hum. Nutr. Diet. 2022, 35, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle Weight-Loss Intervention Outcomes in Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Dornhorst, A.; McGowan, B.; Omar, O.; Leeds, A.R.; Taheri, S.; Frost, G.S. Low-Energy Total Diet Replacement Intervention in Patients with Type 2 Diabetes Mellitus and Obesity Treated with Insulin: A Randomized Trial. BMJ Open Diabetes Res. Care 2020, 8, e001012. [Google Scholar] [CrossRef] [PubMed]
- Lean, M.E.J.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Durability of a Primary Care-Led Weight-Management Intervention for Remission of Type 2 Diabetes: 2-Year Results of the DiRECT Open-Label, Cluster-Randomised Trial. Lancet Diabetes Endocrinol. 2019, 7, 344–355. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary Care-Led Weight Management for Remission of Type 2 Diabetes (DiRECT): An Open-Label, Cluster-Randomised Trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Taheri, S.; Zaghloul, H.; Chagoury, O.; Elhadad, S.; Ahmed, S.H.; El Khatib, N.; Amona, R.A.; El Nahas, K.; Suleiman, N.; Alnaama, A.; et al. Effect of Intensive Lifestyle Intervention on Bodyweight and Glycaemia in Early Type 2 Diabetes (DIADEM-I): An Open-Label, Parallel-Group, Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2020, 8, 477–489. [Google Scholar] [CrossRef]
- Odgers-Jewell, K.; Ball, L.E.; Kelly, J.T.; Isenring, E.A.; Reidlinger, D.P.; Thomas, R. Effectiveness of Group-Based Self-Management Education for Individuals with Type 2 Diabetes: A Systematic Review with Meta-Analyses and Meta-Regression. Diabet. Med. 2017, 34, 1027–1039. [Google Scholar] [CrossRef]
- McCombie, L.; Brosnahan, N.; Ross, H.; Bell-Higgs, A.; Govan, L.; Lean, M.E.J. Filling the Intervention Gap: Service Evaluation of an Intensive Nonsurgical Weight Management Programme for Severe and Complex Obesity. J. Hum. Nutr. Diet. 2019, 32, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.; Leeds, A.R. Very Low-Energy and Low-Energy Formula Diets: Effects on Weight Loss, Obesity Co-Morbidities and Type 2 Diabetes Remission—An Update on the Evidence for Their Use in Clinical Practice. Nutr. Bull. 2019, 44, 7–24. [Google Scholar] [CrossRef] [Green Version]
- Leslie, W.S.; Ford, I.; Sattar, N.; Hollingsworth, K.G.; Adamson, A.; Sniehotta, F.F.; McCombie, L.; Brosnahan, N.; Ross, H.; Mathers, J.C.; et al. The Diabetes Remission Clinical Trial (DiRECT): Protocol for a Cluster Randomised Trial. BMC Fam. Pract. 2016, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheyette, C.; Balolia, Y.; Francis, V.; Callaghan, S.; Turner, F. Carbs & Cals Very Low Calorie Recipes & Meal Plans: Lose Weight, Improve Blood Sugar Levels and Reverse Type 2 Diabetes; Chello Publishing: London, UK, 2017; ISBN 9781908261205. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Mundt, J.C.; Marks, I.M.; Shear, M.K.; Greist, J.H. The Work and Social Adjustment Scale: A Simple Measure of Impairment in Functioning. Br. J. Psychiatry 2002, 180, 461–464. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The Assessment of Binge Eating Severity among Obese Persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Paul, S.K.; Owusu Adjah, E.S.; Samanta, M.; Patel, K.; Bellary, S.; Hanif, W.; Khunti, K. Comparison of Body Mass Index at Diagnosis of Diabetes in a Multi-Ethnic Population: A Case-Control Study with Matched Non-Diabetic Controls. Diabetes Obes. Metab. 2017, 19, 1014–1023. [Google Scholar] [CrossRef] [Green Version]
- Gumber, A.; Gumber, L. Improving Prevention, Monitoring and Management of Diabetes among Ethnic Minorities: Contextualizing the Six G’s Approach. BMC Res. Notes 2017, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Swancutt, D.; Tarrant, M.; Pinkney, J. How Group-Based Interventions Can Improve Services for People with Severe Obesity. Curr. Obes. Rep. 2019, 8, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.; Al-Mrabeh, A.; Sattar, N. Understanding the Mechanisms of Reversal of Type 2 Diabetes. Lancet Diabetes Endocrinol. 2019, 7, 726–736. [Google Scholar] [CrossRef]
- Chew, B.H.; Vos, R.C.; Metzendorf, M.I.; Scholten, R.J.P.M.; Rutten, G.E.H.M. Psychological Interventions for Diabetes-Related Distress in Adults with Type 2 Diabetes Mellitus. Cochrane Database Syst. Rev. 2017, 2017, 1–352. [Google Scholar] [CrossRef]
- da Luz, F.Q.; Hay, P.; Gibson, A.A.; Touyz, S.W.; Swinbourne, J.M.; Roekenes, J.A.; Sainsbury, A. Does Severe Dietary Energy Restriction Increase Binge Eating in Overweight or Obese Individuals? A Systematic Review. Obes. Rev. 2015, 16, 652–665. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.H.; Barnett, A.H.; Bradbury, A.; Cappuccio, F.P.; Gill, P.S.; Hughes, E.; Imray, C.; Jolly, K.; Patel, K. Ethnicity and Cardiovascular Disease Prevention in the United Kingdom: A Practical Approach to Management. J. Hum. Hypertens. 2007, 21, 183–211. [Google Scholar] [CrossRef]
- Thom, G.; Messow, C.-M.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; McCombie, L.; Al-Mrabeh, A.; Zhyzhneuskaya, S.; Welsh, P.; Sattar, N.; et al. Predictors of Type 2 Diabetes Remission in the Diabetes Remission Clinical Trial (DiRECT). Diabetic Medicine 2021, 38, e14395. [Google Scholar] [CrossRef] [PubMed]
- Unick, J.L.; Beavers, D.; Jakicic, J.M.; Kitabchi, A.E.; Knowler, W.C.; Wadden, T.A.; Wing, R.R. Effectiveness of Lifestyle Interventions for Individuals With Severe Obesity and Type 2 Diabetes. Diabetes Care 2011, 34, 2152–2157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Marcus, M.D.; Epstein, L.H.; Salata, R. Type II Diabetic Subjects Lose Less Weight Than Their Overweight Nondiabetic Spouses. Diabetes Care 1987, 10, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; Smith, E.; Tighe, B.; Lycett, D. Group versus One-to-One Multi-Component Lifestyle Interventions for Weight Management: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. J. Hum. Nutr. Diet. 2021, 34, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Foster, D.; Sanchez-Collins, S.; Cheskin, L.J. Multidisciplinary Team–Based Obesity Treatment in Patients With Diabetes: Current Practices and the State of the Science. Diabetes Spectr. 2017, 30, 244. [Google Scholar] [CrossRef] [Green Version]
- Astbury, N.M.; Albury, C.; Nourse, R.; Jebb, S.A. Participant Experiences of a Low-Energy Total Diet Replacement Programme: A Descriptive Qualitative Study. PLoS ONE 2020, 15, e0238645. [Google Scholar] [CrossRef]
- Tudor, K.; Jebb, S.A.; Manoharan, I.; Aveyard, P. Brief Interventions for Obesity When Patients Are Asked to Pay for Weight Loss Treatment: An Observational Study in Primary Care with an Embedded Randomised Trial. Br. J. Gen. Pract. 2020, 70, E348–E355. [Google Scholar] [CrossRef] [PubMed]
- Xin, Y.; Davies, A.; Briggs, A.; McCombie, L.; Messow, C.M.; Grieve, E.; Leslie, W.S.; Taylor, R.; Lean, M.E.J. Type 2 Diabetes Remission: 2 Year within-Trial and Lifetime-Horizon Cost-Effectiveness of the Diabetes Remission Clinical Trial (DiRECT)/Counterweight-Plus Weight Management Programme. Diabetologia 2020, 63, 2112–2122. [Google Scholar] [CrossRef]
- Timpel, P.; Oswald, S.; Schwarz, P.E.H.; Harst, L. Mapping the Evidence on the Effectiveness of Telemedicine Interventions in Diabetes, Dyslipidemia, and Hypertension: An Umbrella Review of Systematic Reviews and Meta-Analyses. J. Med. Internet Res. 2020, 22, e16791. [Google Scholar] [CrossRef] [PubMed]
- Kirley, K.; Sachdev, N. Digital Health–Supported Lifestyle Change Programs to Prevent Type 2 Diabetes. Diabetes Spectr. 2018, 31, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Participants (n = 35) |
|---|---|
| Men, n (%) | 20 (57) |
| Women, n (%) | 15 (43) |
| Age, years (SD) | 50.4 (10.5) |
| Ethnicity, n (%) | |
| Black British | 7 (20%) |
| White British | 7 (20%) |
| Caribbean | 6 (17.1%) |
| African (incl. Somali) | 4 (11.4%) |
| Other Black | 3 (8.6%) |
| Pakistani (incl. British) | 2 (5.7%) |
| Bangladeshi (incl. British) | 2 (5.7%) |
| Any other mixed | 2 (5.7%) |
| Irish | 2 (5.7%) |
| Bodyweight, kg (SD) | 100.3 (16.7) |
| BMI, kg/m2 (SD) | 34.4 (4.4) |
| Waist circumference, cm (SD) | 113.2 (11.3) |
| Body fat % (SD) | 37.5 (8.6) |
| Duration of diabetes, years (SD) | 4.2 (3.6) |
| Number of diabetes medications, n (%) | |
| 0 | 8 (22.9) |
| 1 | 19 (54.3) |
| 2 | 6 (17.1) |
| ≥3 | 2 (5.7) |
| Type of treatment / diabetes medication, n (%) | |
| Diet only | 8 (22.9%) |
| Metformin | 26 (74.3%) |
| Sulfonylurea | 3 (8.6%) |
| SGLT2 inhibitor | 2 (5.7%) |
| HbA1c, mmol/mol (SD) | 65 (20.3) |
| HbA1c, % (SD) | 8 (1.9) |
| Systolic blood pressure, mm Hg (SD) | 133.6 (14.7) |
| Diastolic blood pressure, mm Hg (SD) | 88.2 (9.5) |
| Hypertension, n (%) | 18 (51.4%) |
| Number of antihypertensive medications, n (%) | |
| 0 | 14 (40.0%) |
| 1 | 13 (37.1%) |
| ≥2 | 8 (22.9%) |
| Cardiovascular disease, n (%) | 1 (3%) |
| Total cholesterol, mmol/L (SD) | 4.8 (1.5) |
| HDL cholesterol, mmol/L (SD) | 1.2 (0.4) |
| LDL cholesterol, mmol/L (SD) | 2.6 (1.1) |
| Triglycerides, mmol/L (SD) | 2.1 (2.1) |
| Psychological wellbeing and binge eating scores (SD) | |
| Rosenberg | 21.3 (5.1) |
| DDS, mean | 2.3 (0.9) |
| PHQ9 | 5.3 (4.7) |
| GAD7 | 3.7 (4.3) |
| WAS | 6.3 (6.6) |
| BES | 9.3 (5.8) |
| Mean (SD) | ||||||
|---|---|---|---|---|---|---|
| n | Baseline | 12 Months | Change | 95% CI | p Value | |
| Weight (kg) | 35 | 100.3 (16.8) | 88.8 (14.3) | 11.6 (8.9) | 8.5–14.6 | <0.001 |
| BMI (kg/m2) | 35 | 34.4 (4.5) | 30.5 (4.2) | 3.9 (2.8) | 2.9–5.0 | <0.001 |
| Waist circumference (cm) | 35 | 113.2 (11.5) | 100.3 (10.8) | 12.9 (8.9) | 9.9–16.0 | <0.001 |
| Fat mass (%) | 35 | 37.5 (8.8) | 32.2 (9.6) | 5.3 (4.9) | 3.6–7.0 | <0.001 |
| Fat free mass (%) | 35 | 62.5 (8.7) | 67.8 (9.6) | −5.3 (5.0) | 3.6–7.0 | <0.001 |
| HbA1c (mmol/mol) | 35 | 65.0 (20.6) | 49.5 (17.1) | 15.5 (19.5) | 8.8–22.2 | <0.001 |
| HbA1c (%) | 35 | 8.1 (1.9) | 6.7 (1.6) | 1.4 (1.8) | 0.8–2.0 | <0.001 |
| Number of diabetes medications (mean, SD) | 35 | 1.1 (0.8) | 0.3 (0.7) | 0.8 (0.6) | 0.6–1.0 | <0.001 |
| Systolic blood pressure (mm Hg) | 35 | 133.6 (14.9) | 124.2 (10.6) | 9.3 (16.2) | 3.8–14.9 | 0.002 |
| Diastolic blood pressure (mm Hg) | 35 | 88.2 (9.7) | 78.5 (12.0) | 9.7 (14.6) | 4.7–14.7 | <0.001 |
| Number of anti-hypertensive medications | 35 | 0.9 (1.0) | 0.6 (0.2) | 0.3 (0.5) | 0.5–3.5 | 0.001 |
| Total cholesterol (mmol/l) | 35 | 4.8 (1.5) | 4.5 (1.3) | 0.3 (1.1) | −0.8–0.6 | 0.128 |
| HDL cholesterol (mmol/l) | 35 | 1.2 (0.4) | 1.3 (0.4) | 0.1 (0.2) | −1.3–0.1 | 0.74 |
| LDL cholesterol (mmol/l) | 34 | 2.7 (1.1) | 2.6 (0.8) | 0.1 (0.8) | −0.2–0.4 | 0.617 |
| Triglycerides (mmol/l) | 35 | 2.1 (2.2) | 1.5 (1.8) | 0.7 (0.9) | 0.4–1.0 | <0.001 |
| Rosenberg | 35 | 21.3 (5.2) | 24.1 (5.0) | −2.7 (3.9) | −4.0–−1.4 | <0.001 |
| DDS Mean | 35 | 2.3 (1.0) | 1.8 (0.9) | 0.5 (0.8) | 0.2–0.7 | 0.001 |
| PHQ9 | 35 | 5.3 (4.8) | 3.4 (4.4) | 1.9 (4.7) | 0.3–3.5 | 0.021 |
| GAD7 | 35 | 3.7 (4.4) | 3.4 (4.7) | 0.3 (3.7) | −0.9–1.6 | 0.584 |
| WAS | 35 | 6.3 (6.7) | 6.5 (9.5) | −0.2 (8.2) | −3.0–2.6 | 0.869 |
| BES | 35 | 9.3 (6.0) | 7.7 (5.7) | 1.5 (6.1) | −0.6–3.6 | 0.144 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marples, O.; Resca, L.; Plavska, J.; Hassan, S.; Mistry, V.; Mallik, R.; Brown, A. Real-World Data of a Group-Based Formula Low Energy Diet Programme in Achieving Type 2 Diabetes Remission and Weight Loss in an Ethnically Diverse Population in the UK: A Service Evaluation. Nutrients 2022, 14, 3146. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14153146
Marples O, Resca L, Plavska J, Hassan S, Mistry V, Mallik R, Brown A. Real-World Data of a Group-Based Formula Low Energy Diet Programme in Achieving Type 2 Diabetes Remission and Weight Loss in an Ethnically Diverse Population in the UK: A Service Evaluation. Nutrients. 2022; 14(15):3146. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14153146
Chicago/Turabian StyleMarples, Owen, Laura Resca, Julija Plavska, Samina Hassan, Vibhuti Mistry, Ritwika Mallik, and Adrian Brown. 2022. "Real-World Data of a Group-Based Formula Low Energy Diet Programme in Achieving Type 2 Diabetes Remission and Weight Loss in an Ethnically Diverse Population in the UK: A Service Evaluation" Nutrients 14, no. 15: 3146. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14153146