
Can the Brazilian Caffeine Expectancy Questionnaires Differentiate the CYP1A2 and ADORA2A Gene Polymorphisms?—An Exploratory Study with Brazilian Athletes

 , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaires Application
2.3. Genetic Analysis
2.4. Statistical Analysis
3. Results
3.1. Sample Profile
3.2. CYP1A2 and ADORA2A Genotypes
3.3. CaffEQ-BR Full and Brief Questionnaires Agreement
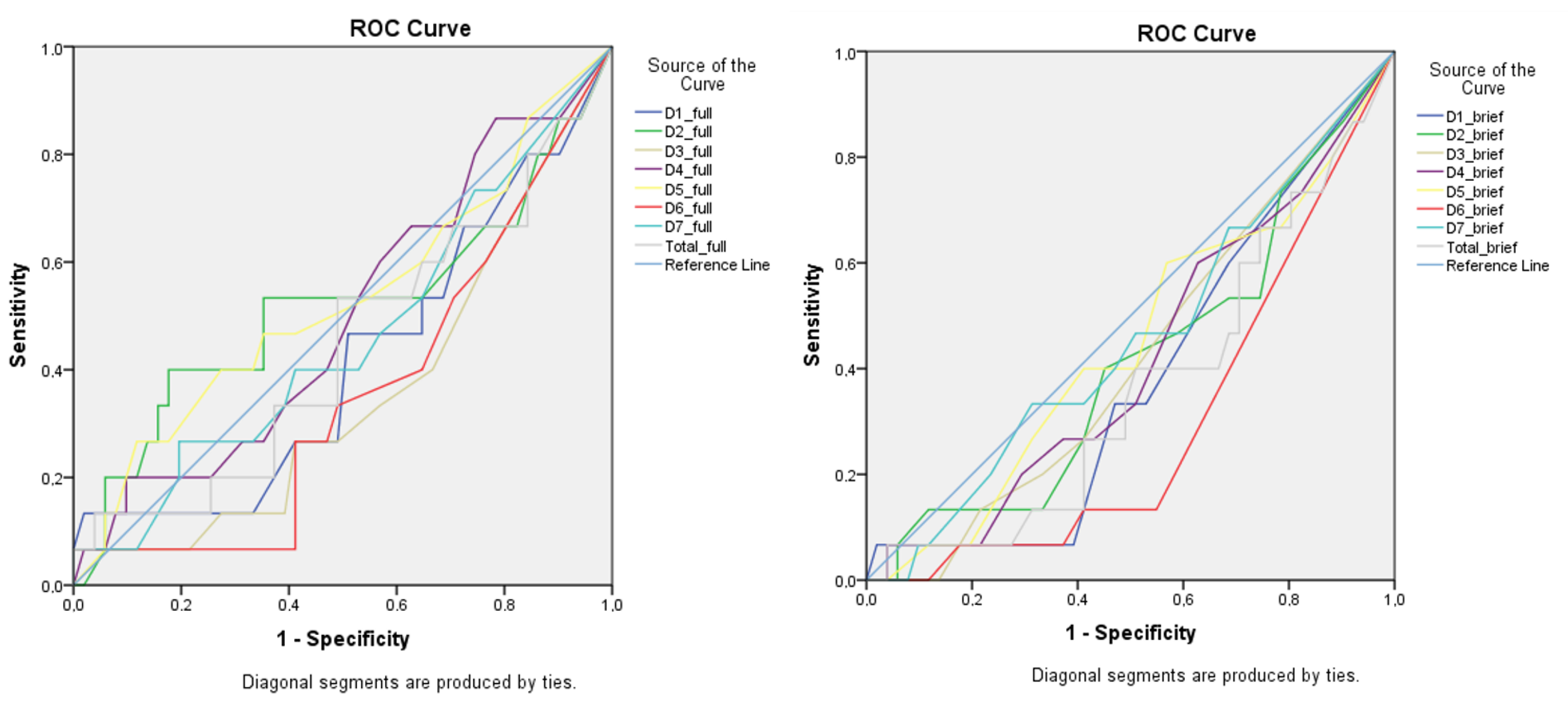
3.4. CaffEQ-BR Discriminatory Capacity for CYP1A2 and ADORA2A Genotypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reyes, C.M.; Cornelis, M.C. Caffeine in the diet: Country-level consumption and guidelines. Nutrients 2018, 10, 1772. [Google Scholar] [CrossRef]
- Wickham, K.A.; Spriet, L.L. Administration of Caffeine in Alternate Forms. Sport. Med. 2018, 48, 79–91. [Google Scholar] [CrossRef]
- Heckman, M.A.; Weil, J.; de Mejia, E.G. Caffeine (1,3,7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 28, 104–125. [Google Scholar] [CrossRef]
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. Wake up and smell the coffee: Caffeine supplementation and exercise performance—An umbrella review of 21 published meta-analyses. Br. J. Sports Med. 2019, 54, 681–688. [Google Scholar] [CrossRef]
- Grgic, J. Effects of Caffeine on Resistance Exercise: A Review of Recent Research. Sport. Med. 2021, 51, 2281–2298. [Google Scholar] [CrossRef]
- Shabir, A.; Hooton, A.; Tallis, J.; Higgins, M.F. The influence of caffeine expectancies on sport, exercise, and cognitive performance. Nutrients 2018, 10, 1528. [Google Scholar] [CrossRef]
- Lorenzo Calvo, J.; Fei, X.; Domínguez, R.; Pareja-Galeano, H. Caffeine and Cognitive Functions in Sports: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 868. [Google Scholar] [CrossRef]
- Grgic, J. Exploring the minimum ergogenic dose of caffeine on resistance exercise performance: A meta-analytic approach. Nutrition 2022, 97, 111604. [Google Scholar] [CrossRef]
- Guest, N.S.; Van Dusseldorp, T.A.; Nelson, M.T.; Grgic, J.; Schoenfeld, B.J.; Jenkins, N.D.M.; Arent, S.M.; Antonio, J.; Stout, J.R.; Trexler, E.T.; et al. International society of sports nutrition position stand: Caffeine and exercise performance. J. Int. Soc. Sports Nutr. 2021, 18, 1. [Google Scholar] [CrossRef]
- Nehlig, A. Interindividual differences in caffeine metabolism and factors driving caffeine consumption. Pharmacol. Rev. 2018, 70, 384–411. [Google Scholar] [CrossRef] [PubMed]
- Barreto, G.; Grecco, B.; Merola, P.; Reis, C.E.G.; Gualano, B.; Saunders, B. Novel insights on caffeine supplementation, CYP1A2 genotype, physiological responses and exercise performance. Eur. J. Appl. Physiol. 2021, 121, 749–769. [Google Scholar] [CrossRef] [PubMed]
- Fulton, J.L.; Dinas, P.C.; Carrillo, A.E.; Edsall, J.R.; Ryan, E.J.; Ryan, E.J. Impact of genetic variability on physiological responses to caffeine in humans: A systematic review. Nutrients 2018, 10, 1373. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Pickering, C.; Del Coso, J.; Schoenfeld, B.J.; Mikulic, P. CYP1A2 genotype and acute ergogenic effects of caffeine intake on exercise performance: A systematic review. Eur. J. Nutr. 2021, 60, 1181–1195. [Google Scholar] [CrossRef]
- Guest, N.; Corey, P.; Vescovi, J.; El-Sohemy, A. Caffeine, CYP1A2 genotype, and endurance performance in athletes. Med. Sci. Sports Exerc. 2018, 50, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Loy, B.D.; O’Connor, P.J.; Lindheimer, J.B.; Covert, S.F. Caffeine Is Ergogenic for Adenosine A 2A Receptor Gene (ADORA2A) T Allele Homozygotes: A Pilot Study. J. Caffeine Res. 2015, 5, 73–81. [Google Scholar] [CrossRef]
- Womack, C.J.; Saunders, M.J.; Bechtel, M.K.; Bolton, D.J.; Martin, M.; Luden, N.D.; Dunham, W.; Hancock, M. The influence of a CYP1A2 polymorphism on the ergogenic effects of caffeine. J. Int. Soc. Sports Nutr. 2012, 9, 7. [Google Scholar] [CrossRef]
- Muñoz, A.; López-Samanes, Á.; Aguilar-Navarro, M.; Varillas-Delgado, D.; Rivilla-García, J.; Moreno-Pérez, V.; Del Coso, J. Effects of CYP1A2 and ADORA2A Genotypes on the Ergogenic Response to Caffeine in Professional Handball Players. Genes 2020, 11, 933. [Google Scholar] [CrossRef]
- Pickering, C. Caffeine, CYP1A2 genotype, and sports performance: Is timing important? Ir. J. Med. Sci. 2019, 188, 349–350. [Google Scholar] [CrossRef]
- Kolb, H.; Kempf, K.; Martin, S. Health Effects of Coffee: Mechanism Unraveled? Nutrients 2020, 12, 1842. [Google Scholar] [CrossRef]
- Baltazar-Martins, J.G.; Brito De Souza, D.; Aguilar, M.; Grgic, J.; Del Coso, J. Infographic. the road to the ergogenic effect of caffeine on exercise performance. Br. J. Sports Med. 2019, 54, 618–619. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Kiely, J. Are the Current Guidelines on Caffeine Use in Sport Optimal for Everyone? Inter-individual Variation in Caffeine Ergogenicity, and a Move Towards Personalised Sports Nutrition. Sport. Med. 2018, 48, 7–16. [Google Scholar] [CrossRef]
- Martins, G.L.; Guilherme, J.P.L.F.; Ferreira, L.H.B.; de Souza-Junior, T.P.; Lancha, A.H. Caffeine and Exercise Performance: Possible Directions for Definitive Findings. Front. Sport. Act. Living 2020, 2, 202. [Google Scholar] [CrossRef]
- Huntley, E.D.; Juliano, L.M. Caffeine Expectancy Questionnaire (CaffEQ): Construction, psychometric properties, and associations with caffeine use, caffeine dependence, and other related variables. Psychol. Assess. 2012, 24, 592. [Google Scholar] [CrossRef] [PubMed]
- Mendes, G.F.; Reis, C.E.G.; Nakano, E.Y.; da Costa, T.H.M.; Saunders, B.; Zandonadi, R.P. Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR). Nutrients 2020, 12, 2248. [Google Scholar] [CrossRef] [PubMed]
- Mendes, G.F.; Reis, C.E.G.; Nakano, E.Y.; Zandonadi, R.P. Brief Version of Caffeine Expectancy Questionnaire in Brazil. Front. Nutr. 2021, 8, 695385. [Google Scholar] [CrossRef]
- Erblang, M.; Drogou, C.; Gomez-Merino, D.; Metlaine, A.; Boland, A.; Deleuze, J.F.; Thomas, C.; Sauvet, F.; Chennaoui, M. The Impact of Genetic Variations in ADORA2A in the Association between Caffeine Consumption and Sleep. Genes 2019, 10, 1021. [Google Scholar] [CrossRef]
- Spineli, H.; Pinto, M.P.; Dos Santos, B.P.; Lima-Silva, A.E.; Bertuzzi, R.; Gitaí, D.L.G.; de Araujo, G.G. Caffeine improves various aspects of athletic performance in adolescents independent of their 163 C > A CYP1A2 genotypes. Scand. J. Med. Sci. Sport. 2020, 30, 1869–1877. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- De Pauw, K.; Roelands, B.; Cheung, S.S.; de Geus, B.; Rietjens, G.; Meeusen, R. Guidelines to Classify Subject Groups in Sport-Science Research. Int. J. Sports Physiol. Perform. 2013, 8, 111–122. [Google Scholar] [CrossRef]
- Evans, J.R.; Mathur, A. The value of online surveys: A look back and a look ahead. Internet Res. 2018, 28, 854–887. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. 2014. Available online: https://www.mhinnovation.net/sites/default/files/files/WHO%20Guidelines%20on%20Translation%20and%20Adaptation%20of%20Instruments.docx (accessed on 23 June 2022).
- Cornelis, M.C.; El-Sohemy, A.; Campos, H. Genetic polymorphism of CYP1A2 increases the risk of myocardial infarction. J. Med. Genet. 2004, 41, 758–762. [Google Scholar] [CrossRef]
- Deckert, J.; Nöthen, M.M.; Franke, P.; Delmo, C.; Fritze, J.; Knapp, M.; Maier, W.; Beckmann, H.; Propping, P. Systematic mutation screening and association study of the A1 and A2a adenosine receptor genes in panic disorder suggest a contribution of the A2a gene to the development of disease. Mol. Psychiatry 1998, 3, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Salinero, J.J.; Lara, B.; Ruiz-Vicente, D.; Areces, F.; Puente-Torres, C.; Gallo-Salazar, C.; Pascual, T.; Del Coso, J. CYP1A2 genotype variations do not modify the benefits and drawbacks of caffeine during exercise: A pilot study. Nutrients 2017, 9, 269. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- World Health Organization (WHO). Mean Body Mass Index (BMI). WHO 2017. Available online: https://www.who.int/gho/ncd/risk_factors/bmi_text/en/ (accessed on 23 June 2022).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 17 July 2022).
- Giersch, G.E.W.; Boyett, J.C.; Hargens, T.A.; Luden, N.D.; Saunders, M.J.; Daley, H.; Hughey, C.A.; El-Sohemy, A.; Womack, C.J. The Effect of the CYP1A2 −163 C > A Polymorphism on Caffeine Metabolism and Subsequent Cycling Performance. J. Caffeine Adenosine Res. 2018, 8, 65–70. [Google Scholar] [CrossRef]
- Grgic, J.; Pickering, C.; Bishop, D.J.; Schoenfeld, B.J.; Mikulic, P.; Pedisic, Z. CYP1A2 genotype and acute effects of caffeine on resistance exercise, jumping, and sprinting performance. J. Int. Soc. Sports Nutr. 2020, 17, 21. [Google Scholar] [CrossRef]
- Rahimi, R. The effect of CYP1A2 genotype on the ergogenic properties of caffeine during resistance exercise: A randomized, double-blind, placebo-controlled, crossover study. Ir. J. Med. Sci. 2018, 188, 337–345. [Google Scholar] [CrossRef]
- Schott, M.; Beiglböck, W.; Neuendorff, R. Translation and Validation of the Caffeine Expectancy Questionnaire (CaffEQ). Int. J. Ment. Health Addict. 2016, 14, 514–525. [Google Scholar] [CrossRef]
- Kearns, N.T.; Blumenthal, H.; Natesan, P.; Zamboanga, B.L.; Ham, L.S.; Cloutier, R.M. Development and initial psychometric validation of the brief-caffeine expectancy questionnaire (B-CaffEQ). Psychol. Assess. 2018, 30, 1597–1611. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.; Marticorena, F.M.; Grecco, B.H.; Barreto, G.; Saunders, B. Can I Have My Coffee and Drink It? A Systematic Review and Meta-analysis to Determine Whether Habitual Caffeine Consumption Affects the Ergogenic Effect of Caffeine. Sport. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Rowe, K.; Wham, C.; Rutherfurd-Markwick, K.; Ali, A. CaffCo: A Valid and Reliable Tool to Assess Caffeine Consumption Habits, Caffeine Expectancies, and Caffeine Withdrawal Effects in Adults. J. Caffeine Adenosine Res. 2020, 10, 154–160. [Google Scholar] [CrossRef]
- Beedie, C.J.; Stuart, E.M.; Coleman, D.A.; Foad, A.J. Placebo effects of caffeine on cycling performance. Med. Sci. Sports Exerc. 2006, 38, 2159–2164. [Google Scholar] [CrossRef]
- Saunders, B.; de Oliveira, L.F.; da Silva, R.P.; de Salles Painelli, V.; Gonçalves, L.S.; Yamaguchi, G.; Mutti, T.; Maciel, E.; Roschel, H.; Artioli, G.G.; et al. Placebo in sports nutrition: A proof-of-principle study involving caffeine supplementation. Scand. J. Med. Sci. Sport. 2017, 27, 1240–1247. [Google Scholar] [CrossRef]
- Shabir, A.; Hooton, A.; Spencer, G.; Storey, M.; Ensor, O.; Sandford, L.; Tallis, J.; Saunders, B.; Higgins, M.F. The Influence of Caffeine Expectancies on Simulated Soccer Performance in Recreational Individuals. Nutrients 2019, 11, 2289. [Google Scholar] [CrossRef]
- Da Cruz, C.J.G.; Porto, L.G.G.; Molina, G.E. Agreement between the Heart Rate Variability Threshold and Ventilatory Threshold in Young Women: Impact of Cardiac Parasympathetic Status and Cardiorespiratory Fitness. Meas. Phys. Educ. Exerc. Sci. 2021, 26, 179–190. [Google Scholar] [CrossRef]
- Perera, V.; Gross, A.S.; Xu, H.; McLachlan, A.J. Pharmacokinetics of caffeine in plasma and saliva, and the influence of caffeine abstinence on CYP1A2 metrics. J. Pharm. Pharmacol. 2011, 63, 1161–1168. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Categories | Total (N = 71) | ||
|---|---|---|---|
| n | % | ||
| Sex | Male | 64 | 90.1 |
| Female | 7 | 9.9 | |
| Age | <30 years | 55 | 77.5 |
| ≥30 years | 16 | 22.5 | |
| Body Mass Index (kg/m2) * | <18.5 | 2 | 2.8 |
| 18.5–24.9 | 49 | 69.0 | |
| 25–29.9 | 14 | 19.7 | |
| ≥30 | 6 | 8.5 | |
| Self-identification | Asia descendants | 5 | 7.0 |
| White | 24 | 33.8 | |
| Indigenous | 3 | 4.3 | |
| Pardo | 29 | 40.8 | |
| Black | 9 | 12.7 | |
| Without description | 1 | 1.4 | |
| Physical Exercises (≧150 min/week) ** | No | 26 | 36.6 |
| Yes | 45 | 63.4 | |
| Degree of Education | Complete elementary school | 1 | 1.4 |
| Incomplete high school | 9 | 12.7 | |
| Complete high school | 24 | 33.8 | |
| Incomplete graduated | 22 | 30.0 | |
| Graduated | 6 | 8.5 | |
| Postgraduate studies | 9 | 12.7 | |
| Income (BRL) *** | Up to 1000.00 | 12 | 16.9 |
| 1000.01 to 2000.00 | 18 | 25.4 | |
| 2000.01 to 3000.00 | 17 | 24,0 | |
| 3000.01 to 5000.00 | 15 | 21.1 | |
| 5000.01 to 10,000.00 | 5 | 7.0 | |
| Above 10,000.00 | 4 | 5.6 | |
| Self-reported chronic diseases | No | 67 | 94.4 |
| Yes | 4 | 5.6 | |
| Factors | Full | Brief | ICC * (CI 95%) |
|---|---|---|---|
| 1. Withdrawal/dependence | 2.33 (1.24) | 2.06 (1.22) | 0.851 (0.754–0.909) |
| 2. Energy/work enhancement | 3.17 (1.43) | 3.13 (1.41) | 0.879 (0.806–0.924) |
| 3. Appetite suppression | 1.87 (0.97) | 1.70 (0.93) | 0.769 (0.631–0.856) |
| 4. Social/mood enhancement | 2.62 (1.29) | 2.55 (1.34) | 0.907 (0.850–0.942) |
| 5. Physical performance enhancement | 3.16 (1.51) | 2.94 (1.46) | 0.891 (0.824–0.932) |
| 6. Anxiety/negative physical effects | 1.84 (0.89) | 1.53 (0.80) | 0.600 (0.356–0.751) |
| 7. Sleep disturbance | 2.58 (1.41) | 2.49 (1.38) | 0.858 (0.772–0.911) |
| Overall | 2.44 (0.98) | 2.34 (0.90) | 0.856 (0.777–0.910) |
| Factors | AUC * (CI 95%) | |
|---|---|---|
| Full | Brief | |
| 1. Withdrawal/dependence | 0.513 (0.376–0.651) | 0.496 (0.360–0.632) |
| 2. Energy/work enhancement | 0.464 (0.329–0.599) | 0.504 (0.369–0.640) |
| 3. Appetite suppression | 0.537 (0.402–0.672) | 0.443 (0.304–0.582) |
| 4. Social/mood enhancement | 0.548 (0.411–0.686) | 0.514 (0.376–0.651) |
| 5. Physical performance enhancement | 0.472 (0.336–0.608) | 0.467 (0.332–0.602) |
| 6. Anxiety/negative physical effects | 0.624 (0.492–0.757) | 0.575 (0.441–0.709) |
| 7. Sleep disturbance | 0.528 (0.391–0.665) | 0.453 (0.318–0.589) |
| Overall | 0.529 (0.393–0.665) | 0.504 (0.367–0.640) |
| Factors | AUC * (CI 95%) | |
|---|---|---|
| Full | Brief | |
| 1. Withdrawal/dependence | 0.415 (0.245–0.585) | 0.385 (0.233–0.537) |
| 2. Energy/work enhancement | 0.516 (0.324–0.708) | 0.414 (0.250–0.578) |
| 3. Appetite suppression | 0.358 (0.199–0.516) | 0.422 (0.267–0.577) |
| 4. Social/mood enhancement | 0.498 (0.330–0.666) | 0.417 (0.257–0.577) |
| 5. Physical performance enhancement | 0.529 (0.350–0.709) | 0.444 (0.279–0.609) |
| 6. Anxiety/negative physical effects | 0.356 (0.201–0.510) | 0.293 (0.155–0.431) |
| 7. Sleep disturbance | 0.461 (0.290–0.632) | 0.455 (0.289–0.621) |
| Overall | 0.443 (0.271–0.616) | 0.367 (0.211–0.522) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes, G.F.; Reis, C.E.G.; Nakano, E.Y.; Spineli, H.; Barreto, G.; Noronha, N.Y.; Watanabe, L.M.; Nonino, C.B.; de Araujo, G.G.; Saunders, B.; et al. Can the Brazilian Caffeine Expectancy Questionnaires Differentiate the CYP1A2 and ADORA2A Gene Polymorphisms?—An Exploratory Study with Brazilian Athletes. Nutrients 2022, 14, 3355. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14163355
Mendes GF, Reis CEG, Nakano EY, Spineli H, Barreto G, Noronha NY, Watanabe LM, Nonino CB, de Araujo GG, Saunders B, et al. Can the Brazilian Caffeine Expectancy Questionnaires Differentiate the CYP1A2 and ADORA2A Gene Polymorphisms?—An Exploratory Study with Brazilian Athletes. Nutrients. 2022; 14(16):3355. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14163355
Chicago/Turabian StyleMendes, Guilherme Falcão, Caio Eduardo Gonçalves Reis, Eduardo Yoshio Nakano, Higor Spineli, Gabriel Barreto, Natália Yumi Noronha, Lígia Moriguchi Watanabe, Carla Barbosa Nonino, Gustavo Gomes de Araujo, Bryan Saunders, and et al. 2022. "Can the Brazilian Caffeine Expectancy Questionnaires Differentiate the CYP1A2 and ADORA2A Gene Polymorphisms?—An Exploratory Study with Brazilian Athletes" Nutrients 14, no. 16: 3355. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14163355