
Soy Food Intake Associated with Obesity and Hypertension in Children and Adolescents in Guangzhou, Southern China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Anthropometric Measurements
2.3. Questionnaire Assessment
2.4. Definitions
2.5. Statistical Analysis
3. Results
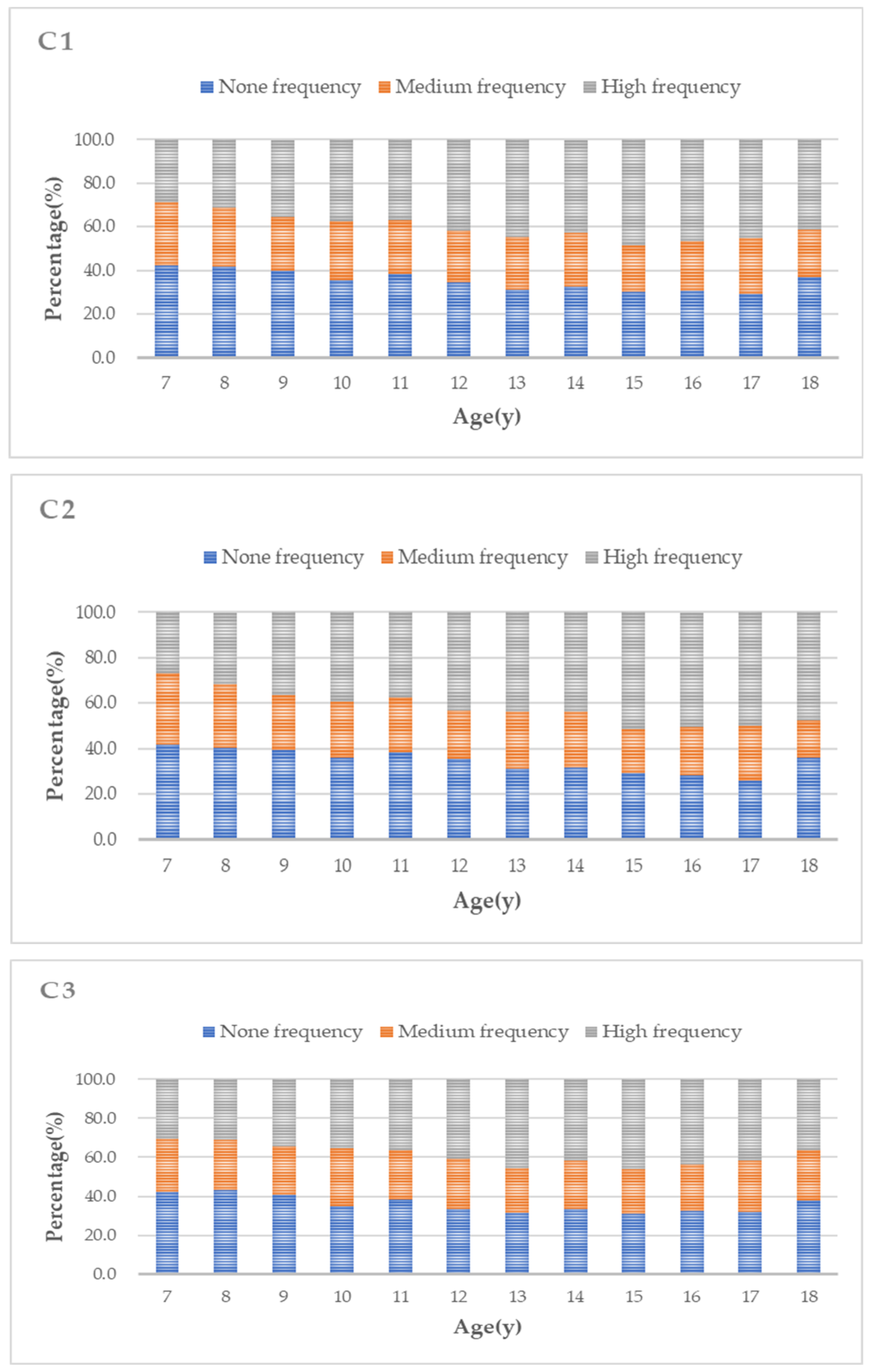
3.1. Soy Food Intake in Chinese Children and Adolescents According to Age
3.2. Characteristics of Participants by Soy Food Intake Levels
3.3. The Distribution of Obesity and Blood Pressure Stratified by Soy Food Intake
3.4. ORs (95% CIs) for Obesity and Hypertension across Soy Food Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, J.; Buys, N.; Shen, S. Dietary patterns and cardiovascular disease-related risks in chinese older adults. Front. Public Health 2013, 1, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahira, M.; Noda, K.; Fukushima, M.; Zhang, B.; Mitsutake, R.; Uehara, Y.; Ogawa, M.; Kakuma, T.; Saku, K. Randomized, double-blind, controlled, comparative trial of formula food containing soy protein vs. milk protein in visceral fat obesity FLAVO study. Circ. J. 2011, 75, 2235–2243. [Google Scholar] [CrossRef] [Green Version]
- Xi, B.; Bovet, P.; Hong, Y.M.; Zong, X.; Chiolero, A.; Kim, H.S.; Zhang, T.; Zhao, M. Recent blood pressure trends in adolescents from China, Korea, Seychelles and the United States of America, 1997–2012. J. Hypertens. 2016, 34, 1948–1958. [Google Scholar] [CrossRef] [PubMed]
- Jahan-Mihan, A.; Smith, C.E.; Hamedani, A.; Anderson, G.H. Soy protein–based compared with casein-based diets fed during pregnancy and lactation increase food intake and characteristics of metabolic syndrome less in female than male rat offspring. Nutr. Res. 2011, 31, 644–651. [Google Scholar] [CrossRef]
- Dietz, W.H. Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatrics 1998, 101, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Fuller, J.; Patterson, K.; Blair, R.; Tabor, A. Soy compared to casein meal replacement shakes with energy-restricted diets for obese women: Randomized controlled trial. Metabolism 2007, 56, 280–288. [Google Scholar] [CrossRef]
- Mohammadifard, N.; Salehi-Abargouei, A.; Salas-Salvadó, J.; Guasch-Ferré, M.; Humphries, K.; Sarrafzadegan, N. The effect of tree nut, peanut, and soy nut consumption on blood pressure: A systematic review and meta-analysis of randomized controlled clinical trials. Am. J. Clin. Nutr. 2015, 101, 966–982. [Google Scholar] [CrossRef] [Green Version]
- McCarty, M.F. Vegan Proteins May Reduce Risk of Cancer, Obesity, and Cardiovascular Disease by Promoting Increased Glucagon Activity. Med. Hypotheses 1999, 53, 459–485. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Do functional foods have a role in the prevention of cardiovascular disease? Circulation 2011, 124, 538–540. [Google Scholar] [CrossRef] [Green Version]
- Ramdath, D.; Padhi, E.; Sarfaraz, S.; Renwick, S.; Duncan, A. Beyond the Cholesterol-Lowering Effect of Soy Protein: A Review of the Effects of Dietary Soy and Its Constituents on Risk Factors for Cardiovascular Disease. Nutrients 2017, 9, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beavers, K.M.; Gordon, M.M.; Easter, L.; Beavers, D.P.; Hairston, K.G.; Nicklas, B.J.; Vitolins, M.Z. Effect of protein source during weight loss on body composition, cardiometabolic risk and physical performance in abdominally obese, older adults: A pilot feeding study. J. Nutr. Health Aging 2015, 19, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Zahabi, E.; Entezari, M.H.; Maracy, M.R. Effects of Soy Flour Fortified Bread Consumption on Cardiovascular Risk Factors According toAPOE Genotypes in Overweight and Obese Adult Women: A Cross-over Randomized Controlled Clinical Trial. Clin. Nutr. Res. 2015, 4, 225. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Kim, I. Soy protein and obesity. Nutrients 2000, 16, 459–460. [Google Scholar] [CrossRef]
- Pan, A.; Franco, O.H.; Ye, J.; Demark-Wahnefried, W.; Ye, X.; Yu, Z.; Li, H.; Lin, X. Soy protein intake has sex-specific effects on the risk of metabolic syndrome in middle-aged and elderly Chinese. J. Nutr. 2008, 138, 2413–2421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simao, A.N.; Lozovoy, M.A.; Simao, T.N.; Dichi, J.B.; Matsuo, T.; Dichi, I. Nitric oxide enhancement and blood pressure decrease in patients with metabolic syndrome using soy protein or fish oil. Arq. Bras. Endocrinol. Metabol. 2010, 54, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Palanisamy, N.; Viswanathan, P.; Ravichandran, M.K.; Anuradha, C.V. Renoprotective and blood pressure-lowering effect of dietary soy protein via protein kinase C beta II inhibition in a rat model of metabolic syndrome. Can. J. Physiol. Pharmacol. 2010, 88, 28–37. [Google Scholar] [CrossRef]
- Hermsdorff, H.H.; Zulet, M.A.; Abete, I.; Martinez, J.A. A legume-based hypocaloric diet reduces proinflammatory status and improves metabolic features in overweight/obese subjects. Eur. J. Nutr. 2011, 50, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Hecker, K.D. Effects of dietary animal and soy protein on cardiovascular disease risk factors. Curr. Atheroscler. Rep. 2001, 3, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiary, A.; Yassin, Z.; Hanachi, P.; Rahmat, A.; Ahmad, Z.; Jalali, F. Effects of soy on metabolic biomarkers of cardiovascular disease in elderly women with metabolic syndrome. Arch. Iran. Med. 2012, 15, 462–468. [Google Scholar]
- He, J.; Gu, D.; Wu, X.; Chen, J.; Duan, X.; Chen, J.; Whelton, P.K. Effect of soybean protein on blood pressure: A randomized, controlled trial. Ann. Intern. Med. 2005, 143, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nozue, M.; Shimazu, T.; Sasazuki, S.; Charvat, H.; Mori, N.; Mutoh, M.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Inoue, M.; et al. Fermented Soy Product Intake Is Inversely Associated with the Development of High Blood Pressure: The Japan Public Health Center-Based Prospective Study. J. Nutr. 2017, 147, 1749–1756. [Google Scholar] [CrossRef] [Green Version]
- Kou, T.; Wang, Q.; Cai, J.; Song, J.; Du, B.; Zhao, K.; Ma, Y.; Geng, B.; Zhang, Y.; Han, X.; et al. Effect of soybean protein on blood pressure in postmenopausal women: A meta-analysis of randomized controlled trials. Food Funct. 2017, 8, 2663–2671. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Giannopoulos, D.; Dalais, F.S.; Hodgson, J.; McGrath, B.P. Randomised, controlled, cross-over trial of soy protein with isoflavones on blood pressure and arterial function in hypertensive subjects. J. Am. Coll. Nutr. 2006, 25, 533–540. [Google Scholar] [CrossRef]
- Ruscica, M.; Pavanello, C.; Gandini, S.; Gomaraschi, M.; Vitali, C.; Macchi, C.; Morlotti, B.; Aiello, G.; Bosisio, R.; Calabresi, L.; et al. Effect of soy on metabolic syndrome and cardiovascular risk factors: A randomized controlled trial. Eur. J. Nutr. 2018, 57, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G.; Grafenauer, S.J.; O’Shea, J.E. Cereal grains, legumes, and weight management: A comprehensive review of the scientific evidence. Nutr. Rev. 2008, 66, 171–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newby, P.K. Plant foods and plant-based diets: Protective against childhood obesity? Am. J. Clin. Nutr. 2009, 89, 1572S–1587S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmignani, L.O.; Pedro, A.O.; Da, C.L.; Pinto-Neto, A.M. The effect of soy dietary supplement and low dose of hormone therapy on main cardiovascular health biomarkers: A randomized controlled trial. Rev. Bras. Ginecol. Obstet. 2014, 36, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Akhlaghi, M.; Zare, M.; Nouripour, F. Effect of Soy and Soy Isoflavones on Obesity-Related Anthropometric Measures: A Systematic Review and Meta-analysis of Randomized Controlled Clinical Trials. Adv. Nutr. 2017, 8, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents. Zhonghua Liu Xing Bing Xue Za Zhi 2004, 25, 97–102. [Google Scholar]
- Ma, G.S.; Ji, C.Y.; Ma, J.; Mi, J.; Sung, R.Y.; Xiong, F.; Yan, W.L.; Hu, X.Q.; Li, Y.P.; Du, S.M.; et al. Waist circumference reference values for screening cardiovascular risk factors in Chinese children and adolescents. Biomed. Environ. Sci. 2010, 23, 21–31. [Google Scholar] [CrossRef]
- Mi, J.; Wang, T.; Meng, L.; Zhu, G.; Han, S.; Zhong, Y.; Liu, G.; Wan, Y.; Xiong, F.; Shi, J.; et al. Development of blood pressure reference standards for Chinese children and adolescents. Chin. J. Evid. Based Pediatr. 2010, 5, 4–14. [Google Scholar]
- Messina, M. Soy and Health Update: Evaluation of the Clinical and Epidemiologic Literature. Nutrients 2016, 8, 754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, L.P. Soy consumption in Taiwanese children in Taipei. J. Nutr. 2000, 130, 705S. [Google Scholar]
- Messina, M.; Nagata, C.; Wu, A.H. Estimated Asian Adult Soy Protein and Isoflavone Intakes. Nutr. Cancer 2006, 55, 12. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.S.F.; Lee, R.H.Y.; Luo, H.Y.; Kam, C.W.; Yuen, M.P.; Hjelm, M.; Lee, S.H. Growth and nutrition of Chinese vegetarian children in HongKong. J. Paediatr. Child Health 2001, 37, 247–253. [Google Scholar] [CrossRef]
- Wang, D.; Shi, Y.; Chang, C.; Stewart, D.; Ji, Y.; Wang, Y.; Harris, N. Knowledge, attitudes and behaviour regarding nutrition and dietary intake of seventh-grade students in rural areas of Mi Yun County, Beijing, China. Environ. Health Prev. Med. 2014, 19, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, M.; Rogero, M.M.; Fisberg, M.; Waitzberg, D. Health impact of childhood and adolescent soy consumption. Nutr. Rev. 2017, 75, 500–515. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.X.; Li, S.H.; Chen, J.Z.; Sun, K.; Wang, X.J.; Wang, X.G.; Hui, R.T. Effect of soy isoflavones on blood pressure: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Allison, D.B.; Gadbury, G.; Schwartz, L.G.; Murugesan, R.; Kraker, J.L.; Heshka, S.; Fontaine, K.R.; Heymsfield, S.B. A Novel Soy-Based Meal Replacement Formula for Weight Loss among Obese Individuals: A Randomized Controlled Clinical Trial. Eur J. Clin. Nutr. 2003, 57, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Gao, J.; Zhang, Q.; Fu, Y.; Li, K.; Zhu, S.; Li, D. Soy fiber improves weight loss and lipid profile in overweight and obese adults: A randomized controlled trial. Mol. Nutr. Food Res. 2013, 57, 2147–2154. [Google Scholar] [CrossRef]
- Liao, F.; Shieh, M.; Yang, S.; Lin, S.; Chien, Y. Effectiveness of a soy-based compared with a traditional low-calorie diet on weight loss and lipid levels in overweight adults. Nutrition 2007, 23, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Huang, C.; Luo, Q.; Liu, W.; Cheng, D.; Li, Y.; Xia, Y.; Li, C.; Tang, L.; Fang, J.; et al. Soy Isoflavones Ameliorate Fatty Acid Metabolism of Visceral Adipose Tissue by Increasing the AMPK Activity in Male Rats with Diet-Induced Obesity (DIO). Molecules 2019, 24, 2809. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age (y) | Liquid Soy Food (Cups/Day) Mean ± SD | Solid Soy Food (Servings/Day) Mean ± SD | All Soy Food (Times/Week) Mean ± SD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total N = 10,536 | Boys n = 5125 | Girls n = 5411 | Total N = 10,536 | Boys n = 5125 | Girls n = 5411 | Total N = 10,536 | Boys n = 5125 | Girls n = 5411 | |
| 7 | 0.26 ± 0.44 | 0.26 ± 0.44 | 0.27 ± 0.46 | 0.33 ± 0.47 | 0.33 ± 0.44 | 0.34 ± 0.51 | 2.01 ± 1.69 | 1.95 ± 1.60 | 2.08 ± 1.79 |
| 8 | 0.27 ± 0.38 | 0.25 ± 0.31 | 0.29 ± 0.44 | 0.35 ± 0.51 | 0.35 ± 0.46 | 0.36 ± 0.55 | 2.05 ± 1.65 | 2.06 ± 1.69 | 2.04 ± 1.60 |
| 9 | 0.31 ± 0.47 | 0.34 ± 0.57 | 0.28 ± 0.34 * | 0.47 ± 0.70 | 0.48 ± 0.74 | 0.47 ± 0.66 | 2.23 ± 1.87 | 2.26 ± 1.97 | 2.19 ± 1.75 |
| 10 | 0.35 ± 0.51 | 0.38 ± 0.55 | 0.32 ± 0.46 * | 0.52 ± 0.66 | 0.55 ± 0.69 | 0.49 ± 0.63 | 2.39 ± 2.02 | 2.49 ± 2.23 | 2.27 ± 1.76 |
| 11 | 0.38 ± 0.61 | 0.38 ± 0.64 | 0.37 ± 0.59 | 0.48 ± 0.69 | 0.52 ± 0.77 | 0.44 ± 0.58 | 2.34 ± 2.09 | 2.38 ± 2.26 | 2.29 ± 1.86 |
| 12 | 0.43 ± 0.56 | 0.48 ± 0.63 | 0.39 ± 0.49 * | 0.49 ± 0.61 | 0.51 ± 0.69 | 0.46 ± 0.52 | 2.50 ± 1.96 | 2.61 ± 1.14 | 2.40 ± 1.77 |
| 13 | 0.44 ± 0.71 | 0.46 ± 0.82 | 0.42 ± 0.61 | 0.49 ± 0.65 | 0.53 ± 0.77 | 0.47 ± 0.54 | 2.59 ± 2.07 | 2.62 ± 2.29 | 2.57 ± 1.90 |
| 14 | 0.33 ± 0.43 | 0.36 ± 0.47 | 0.30 ± 0.40 | 0.46 ± 0.60 | 0.52 ± 0.66 | 0.42 ± 0.56 * | 2.51 ± 2.06 | 2.63 ± 2.11 | 2.41 ± 2.02 |
| 15 | 0.38 ± 0.57 | 0.43 ± 0.62 | 0.35 ± 0.52 * | 0.50 ± 0.65 | 0.53 ± 0.72 | 0.47 ± 0.58 | 2.71 ± 2.14 | 2.92 ± 2.28 | 2.53 ± 2.01 * |
| 16 | 0.40 ± 0.61 | 0.43 ± 0.67 | 0.37 ± 0.56 | 0.50 ± 0.64 | 0.55 ± 0.68 | 0.47 ± 0.61 | 2.72 ± 2.18 | 2.98 ± 2.45 | 2.51 ± 1.91 * |
| 17 | 0.37 ± 0.58 | 0.42 ± 0.64 | 0.34 ± 0.52 | 0.49 ± 0.66 | 0.54 ± 0.74 | 0.46 ± 0.59 | 2.65 ± 2.04 | 2.82 ± 2.08 | 2.52 ± 2.00 * |
| 18 | 0.33 ± 0.51 | 0.38 ± 0.56 | 0.28 ± 0.44 | 0.44 ± 0.66 | 0.43 ± 0.52 | 0.46 ± 0.76 | 2.52 ± 2.20 | 2.76 ± 2.45 | 2.31 ± 1.94 |
| Total | 0.35 ± 0.54 | 0.37 ± 0.58 | 0.33 ± 0.50 * | 0.46 ± 0.63 | 0.48 ± 0.67 | 0.44 ± 0.59 * | 2.41 ± 2.00 | 2.48 ± 2.13 | 2.32 ± 1.86 * |
| Variables | Liquid Soy Food (Cups/Day) | Solid Soy Food (Servings/Day) | All Soy Food (Times/Week) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| None 1,† | Medium 1,† | High 1,† | p Value | None 2,† | Medium 2,† | High 2,† | p Value | None 3,† | Medium 3,† | High 3,† | p Value | |
| Sex, % | 0.010 b | 0.011 b | 0.127 | |||||||||
| Male | 37.3 | 28.5 * | 34.2 | 40.0 | 28.3 | 31.7 | 35.1 | 24.4 | 40.4 | |||
| Female | 35.6 | 31.2 * | 32.2 | 40.1 | 30.5 | 29.4 | 36.0 | 25.5 | 38.5 | |||
| Family income, RMB/month, % | 0.320 | 0.009 b | 0.038 b | |||||||||
| 2000 or below | 35.5 | 29.8 | 34.6 | 0.880 | 44.9 | 25.1 * | 30.1 | 0.052 | 39.7 | 21.1 * | 39.2 | 0.076 |
| 2000–5000 | 34.4 | 30.8 | 34.8 * | 0.061 | 38.7 | 29.6 | 31.7 | 0.219 | 34.3 | 26.1 | 39.6 | 0.233 |
| 5000–8000 | 36.5 | 30.9 | 32.6 | 0.416 | 38.9 | 31.2 | 29.9 | 0.115 | 36.6 | 26.2 | 37.2 * | 0.046 b |
| ≥8000 | 37.2 | 29.6 | 33.2 | 0.525 | 39.8 | 30.3 | 29.9 | 0.376 | 34.9 | 25.0 | 40.0 | 0.640 |
| Don’t know or no answer | 37.7 | 28.4 | 33.6 | 0.214 | 42.4 | 26.8 * | 30.9 | 0.009 b | 35.9 | 23.2 | 40.9 | 0.098 |
| Anthropometry, mean ± SE | ||||||||||||
| Weight (kg) | 42.62 ± 0.23 | 39.53 ± 0.26 * | 43.77 ± 0.25 * | <0.001 a | 41.21 ± 0.23 | 41.14 ± 0.26 | 44.08 ± 0.26 * | <0.001 a | 40.51 ± 0.24 | 40.83 ± 0.28 | 44.30 ± 0.23 * | <0.001 a |
| BMI (kg/m2) | 18.30 ± 0.06 | 17.78 ± 0.06 * | 18.52 ± 0.06 * | <0.001 a | 18.03 ± 0.05 | 18.07 ± 0.06 | 18.61 ± 0.07 * | <0.001 a | 17.94 ± 0.06 | 17.99 ± 0.07 | 18.63 ± 0.06 * | <0.001 a |
| WC (cm) | 64.11 ± 0.16 | 62.52 ± 0.18 * | 64.57 ± 0.16 | <0.001 a | 63.30 ± 0.15 | 63.30 ± 0.17 | 64.91 ± 0.18 * | <0.001 a | 63.04 ± 0.16 | 63.22 ± 0.19 | 64.84 ± 0.15 * | <0.001 a |
| SBP (mmHg) | 105.97 ± 0.19 | 104.91 ± 0.21 * | 106.24 ± 0.19 | <0.001 a | 105.35 ± 0.18 | 105.55 ± 0.21 | 106.44 ± 0.21 * | <0.001 a | 105.05 ± 0.19 | 105.63 ± 0.23 | 106.43 ± 0.18 * | <0.001 a |
| DBP (mmHg) | 65.81 ± 0.13 | 65.65 ± 0.15 | 65.89 ± 0.13 | 0.471 | 65.71 ± 0.12 | 65.62 ± 0.15 | 66.05 ± 0.14 | 0.082 | 65.59 ± 0.13 | 65.93 ± 0.16 | 65.87 ± 0.13 | 0.171 |
| Dietary conditions, mean ± SE | ||||||||||||
| Fruit, servings/day | 1.06 ± 0.02 | 1.09 ± 0.02 * | 1.25 ± 0.02 * | <0.001 c | 1.05 ± 0.02 | 1.08 ± 0.02 * | 1.28 ± 0.02 * | <0.001 c | 1.07 ± 0.02 | 1.09 ± 0.02 * | 1.22 ± 0.02 * | <0.001 c |
| Vegetables, servings/day | 1.84 ± 0.02 | 1.82 ± 0.03 | 2.01 ± 0.03 * | <0.001 c | 1.76 ± 0.02 | 1.79 ± 0.02 * | 2.17 ± 0.03 * | <0.001 c | 1.79 ± 0.03 | 1.90 ± 0.03 * | 1.98 ± 0.02 * | <0.001 c |
| Meat, servings/day | 1.71 ± 0.02 | 1.59 ± 0.02 * | 1.79 ± 0.03 * | <0.001 c | 1.64 ± 0.02 | 1.53 ± 0.02 | 1.94 ± 0.03 * | <0.001 c | 1.67 ± 0.02 | 1.65 ± 0.03 | 1.76 ± 0.02 * | <0.001 c |
| Milk, servings/day | 0.61 ± 0.01 | 0.59 ± 0.01 | 0.72 ± 0.01 * | <0.001 c | 0.60 ± 0.01 | 0.63 ± 0.01 * | 0.71 ± 0.10 * | <0.001 c | 0.58 ± 0.01 | 0.61 ± 0.01 * | 0.71 ± 0.01 * | <0.001 c |
| SSBs, servings/day | 0.21 ± 0.01 | 0.25 ± 0.01 * | 0.32 ± 0.01 * | <0.001 c | 0.24 ± 0.01 | 0.24 ± 0.01 * | 0.31 ± 0.01 * | <0.001 c | 0.24 ± 0.01 | 0.24 ± 0.01 * | 0.29 ± 0.01 * | <0.001 c |
| Fried food times/week | 0.62 ± 0.02 | 0.82 ± 0.02 * | 1.00 ± 0.02 * | <0.001 c | 0.67 ± 0.02 | 0.81 ± 0.02 * | 0.99 ± 0.03 * | <0.001 c | 0.68 ± 0.02 | 0.77 ± 0.02 * | 0.95 ± 0.02 * | <0.001 c |
| Liquid Soy Food (Cups/Day) | Solid Soy Food (Servings/Day) | All Soy Food (Times/Week) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | None 1,† | Medium 1,† | High 1,† | p Value | None 2,† | Medium 2,† | High 2,† | p Value | None 3,† | Medium 3,† | High 3,† | p Value | |
| BMI | 0.004 a | 0.059 | 0.105 | ||||||||||
| Normal, % | 70.6 | 72.0 | 68.8 * | 70.7 | 0.013 a | 71.2 | 70.5 | 69.8 | 0.381 | 70.5 | 70.8 | 70.4 | 0.935 |
| Overweight, % | 9.5 | 9.5 | 9.0 | 9.9 | 0.448 | 9.4 | 8.8 | 10.3 | 0.139 | 9.6 | 8.6 | 10.0 | 0.138 |
| Obesity, % | 6.2 | 5.8 | 6.5 | 6.3 | 0.414 | 5.5 | 6.5 | 6.9 * | 0.032 a | 5.7 | 6.2 | 6.7 | 0.175 |
| Abdominal obesity | 0.639 | 0.143 | 0.074 | ||||||||||
| No, % | 86.1 | 86.5 | 86.0 | 85.7 | 86.4 | 86.6 | 85.1 | 86.2 | 87.2 | 85.3 | |||
| Yes, % | 13.9 | 13.5 | 14.0 | 14.3 | 13.6 | 13.4 | 14.9 | 13.8 | 12.8 | 14.7 | |||
| Hypertension HTN | 0.038 a | 0.263 | 0.116 | ||||||||||
| Normal, % | 75.6 | 75.3 | 75.3 | 76.3 | 0.569 | 75.9 | 76.1 | 74.9 | 0.528 | 76.0 | 75.2 | 75.6 | 0.750 |
| Pre-hypertension, % | 14.5 | 14.5 | 13.9 | 15.1 | 0.395 | 14.0 | 14.0 | 15.6 | 0.095 | 13.7 | 14.4 | 15.3 * | 0.142 |
| Hypertension, % | 9.9 | 10.2 | 10.8 | 8.7 * | 0.010 a | 10.1 | 9.9 | 9.4 | 0.600 | 10.3 | 10.5 | 9.1 | 0.114 |
| Overweight OR (95% CI) | Obesity OR (95% CI) | Abdominal Obesity OR (95% CI) | Pre-Hypertension OR (95% CI) | Hypertension OR (95% CI) | |
|---|---|---|---|---|---|
| Liquid soy food (cups/day) a | |||||
| Model 1 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 0.987 (0.837–1.164) | 1.179 (0.968–1.436) | 1.044 (0.911–1.197) | 0.960 (0.837–1.101) | 1.057 (0.906–1.235) |
| High servings | 1.057 (0.904–1.235) | 1.112 (0.917–1.348) | 1.064 (0.933–1.214) | 1.028 (0.903–1.171) | 0.840 (0.717–0.984) * |
| Model 2 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 0.994 (0.841–1.175) | 1.141 (0.934–1.394) | 1.026 (0.894–1.177) | 1.098 (0.954–1.263) | 1.076 (0.920–1.257) |
| High servings | 1.071 (0.915–1.253) | 1.154 (0.949–1.402) | 1.071 (0.939–1.223) | 1.000 (0.876–1.142) | 0.839 (0.716–0.983) * |
| Model 3 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 1.009 (0.852–1.239) | 1.163 (0.950–1.425) | 1.027 (0.893–1.180) | 1.123 (0.973–1.297) | 1.116 (0.949–1.312) |
| High servings | 1.072 (0.913–1.259) | 1.175 (0.964–1.431) | 1.079 (0.944–1.234) | 0.985 (0.860–1.129) | 0.804 (0.681–0.948) * |
| Model 4 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 1.067 (0.896–1.272) | 1.131 (0.918–1.394) | 1.032 (0.893–1.192) | 1.091 (0.941–1.265) | 1.112 (0.941–1.313) |
| High servings | 1.123 (0.951–1.327) | 1.194 (0.975–1.461) | 1.124 (0.979–1.291) | 0.958 (0.832–1.102) | 0.790 (0.666–0.937) * |
| Solid soy food (servings/day) b | |||||
| Model 1 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 0.944 (0.802–1.112) | 1.195 (0.981–1.455) | 0.984 (0.859–1.127) | 0.997 (0.871–1.141) | 0.975 (0.835–1.140) |
| High servings | 1.113 (0.952–1.301) | 1.287 (1.062–1.559) * | 1.118 (0.980–1.274) | 1.129 (0.991–1.286) | 0.942 (0.806–1.102) |
| Model 2 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 0.961 (0.815–1.134) | 1.220 (1.000–1.488) | 0.986 (0.861–1.130) | 1.005 (0.876–1.154) | 0.981 (0.839–1.146) |
| High servings | 1.123 (0.959–1.315) | 1.365 (1.123–1.659) * | 1.137 (0.997–1.297) | 1.027 (0.898–1.173) | 0.934 (0.798–1.093) |
| Model 3 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 0.974 (0.823–1.152) | 1.212 (0.992–1.481) | 0.974 (0.848–1.118) | 1.000 (0.868–1.151) | 0.980 (0.834–1.152) |
| High servings | 1.132 (0.964–1.330) | 1.330 (1.092–1.620) * | 1.123 (0.983–1.283) | 0.997 (0.87–1.143) | 0.866 (0.735–1.020) |
| Model 4 | |||||
| No servings | 1 | 1 | 1 | 1 | 1 |
| Medium servings | 1.008 (0.848–1.199) | 1.189 (0.967–1.461) | 0.968 (0.840–1.116) | 0.974 (0.842–1.127) | 0.985 (0.834–1.163) |
| High servings | 1.158 (0.981–1.367) | 1.335 (1.091–1.633) * | 1.147 (1.000–1.315) | 1.006 (0.874–1.158) | 0.867 (0.732–1.027) |
| All soy food (times/week) c | |||||
| Model 1 | |||||
| No frequency | 1 | 1 | 1 | 1 | 1 |
| Medium frequency | 0.887 (0.743–1.059) | 1.086 (0.878–1.343) | 0.912 (0.787–1.056) | 1.060 (0.917–1.225) | 1.027 (0.871–1.211) |
| High frequency | 1.042 (0897–1.212) | 1.180 (0.980–1.422) | 1.076 (0.948–1.221) | 1.120 (0.986–1.271) | 0.891 (0.767–1.036) |
| Model 2 | |||||
| No frequency | 1 | 1 | 1 | 1 | 1 |
| Medium frequency | 0.894 (0.748–1.069) | 1.104 (0.891–1.368) | 0.916 (0.790–1.061) | 1.043 (0.899–1.209) | 1.027 (0.871–1.212) |
| High frequency | 1.061 (0.910–1.236) | 1.281 (1.060–1.548) * | 1.103 (0.971–1.253) | 0.972 (0.853–1.108) | 0.881 (0.757–1.025) |
| Model 3 | |||||
| No frequency | 1 | 1 | 1 | 1 | 1 |
| Medium frequency | 0.884 (0.737–1.061) | 1.119 (0.902–1.389) | 0.898 (0.773–1.043) | 1.059 (0.911–1.232) | 1.034 (0.871–1.227) |
| High frequency | 1.062 (0.909–1.241) | 1.256 (1.036–1.521) * | 1.089 (0.957–1.239) | 0.938 (0.821–1.073) | 0.827 (0.706–0.968) * |
| Model 4 | |||||
| No frequency | 1 | 1 | 1 | 1 | 1 |
| Medium frequency | 0.896 (0.743–1.081) | 1.089 (0.871–1.361) | 0.887 (0.760–1.036) | 1.072 (0.918–1.252) | 1.051 (0.881–1.254) |
| High frequency | 1.087 (0.926–1.277) | 1.302 (1.070–1.583) * | 1.119 (0.981–1.278) | 0.937 (0.816–1.075) | 0.828 (0.704–0.974) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; He, T.; Xu, S.; Li, H.; Wu, M.; Lin, Z.; Huang, F.; Zhu, Y. Soy Food Intake Associated with Obesity and Hypertension in Children and Adolescents in Guangzhou, Southern China. Nutrients 2022, 14, 425. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030425
Wang X, He T, Xu S, Li H, Wu M, Lin Z, Huang F, Zhu Y. Soy Food Intake Associated with Obesity and Hypertension in Children and Adolescents in Guangzhou, Southern China. Nutrients. 2022; 14(3):425. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030425
Chicago/Turabian StyleWang, Xiaotong, Tongtong He, Suhua Xu, Hailin Li, Miao Wu, Zongyu Lin, Fenglian Huang, and Yanna Zhu. 2022. "Soy Food Intake Associated with Obesity and Hypertension in Children and Adolescents in Guangzhou, Southern China" Nutrients 14, no. 3: 425. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030425