
Food Reward after Bariatric Surgery and Weight Loss Outcomes: An Exploratory Study

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
2.2.1. Food Reward
2.2.2. Other Covariates
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
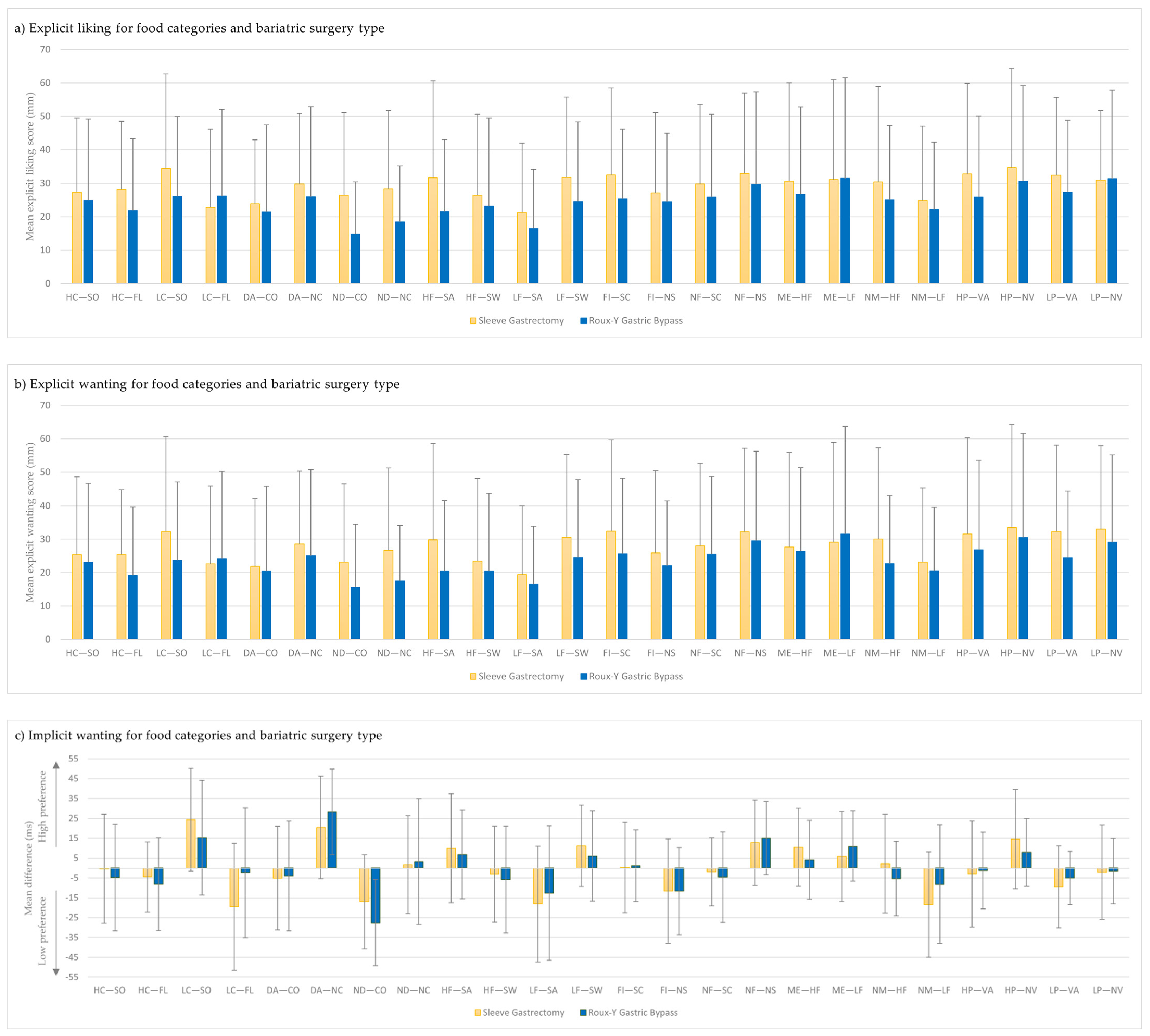
3.2. Relationship between Liking and Wanting for Foods and Type of Bariatric Surgery
3.3. Relationship between Liking and Wanting for Foods Regarding Weight Loss Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Sjöström, C.D.; Karason, K.; Wedel, H.; Ahlin, S.; Anveden, Å.; Bengtsson, C.; Bergmark, G.; et al. Bariatric Surgery and Long-Term Cardiovascular Events. JAMA 2012, 307, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, L. Review of the Key Results from the Swedish Obese Subjects (SOS) Trial—A Prospective Controlled Intervention Study of Bariatric Surgery. J. Intern. Med. 2013, 273, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Zundel, N.; Buchwald, H.; Scopinaro, N. Bariatric Surgery and Endoluminal Procedures: IFSO Worldwide Survey 2014. Obes. Surg. 2017, 27, 2279–2289. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.E.; Thornley, C.J.; Blackstone, R.P. Outcomes in Bariatric and Metabolic Surgery: An Updated 5-Year Review. Curr. Obes. Rep. 2020, 9, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; le Roux, C.W.; Silecchia, G. Food Intake and Changes in Eating Behavior After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef]
- Laurenius, A.; Larsson, I.; Melanson, K.J.; Lindroos, A.K.; Lönroth, H.; Bosaeus, I.; Olbers, T. Decreased Energy Density and Changes in Food Selection Following Roux-En-Y Gastric Bypass. Eur. J. Clin. Nutr. 2013, 67, 168–173. [Google Scholar] [CrossRef]
- Thirlby, R.C.; Bahiraei, F.; Randall, J.; Drewnoski, A. Effect of Roux-En-Y Gastric Bypass on Satiety and Food Likes: The Role of Genetics. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract. 2006, 10, 270–277. [Google Scholar] [CrossRef]
- Guyot, E.; Dougkas, A.; Bagot, S.; Nazare, J.A.; Disse, E.; Iceta, S. A Systematic Review of Food Preference Modifications after Bariatric Surgery. Obes. Rev. 2021, 22, e13315. [Google Scholar] [CrossRef]
- Peng, M.; Coutts, D.; Wang, T.; Cakmak, Y.O. Systematic Review of Olfactory Shifts Related to Obesity. Obes. Rev. 2019, 20, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Penney, N.; Darzi, A.; Purkayastha, S. Taste Changes after Bariatric Surgery: A Systematic Review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.S.; Andersen, I.N.S.K.K.; Lange, B.; Ritz, C.; le Roux, C.W.; Schmidt, J.B.; Sjodin, A.; Bredie, W.L.P.P.; Sjödin, A.; Bredie, W.L.P.P.; et al. Bariatric Surgery Leads to Short-Term Effects on Sweet Taste Sensitivity and Hedonic Evaluation of Fatty Food Stimuli. Obesity 2019, 27, 1796–1804. [Google Scholar] [CrossRef]
- Guyot, E.; Dougkas, A.; Robert, M.; Nazare, J.-A.; Iceta, S.; Disse, E. Food Preferences and Their Perceived Changes Before and After Bariatric Surgery: A Cross-Sectional Study. Obes. Surg. 2021, 31, 3075–3082. [Google Scholar] [CrossRef] [PubMed]
- Berridge, K.C. Food Reward: Brain Substrates of Wanting and Liking. Neurosci. Biobehav. Rev. 1996, 20, 1–25. [Google Scholar] [CrossRef]
- Tibboel, H.; De Houwer, J.; Van Bockstaele, B. Implicit Measures of “Wanting” and “Liking” in Humans. Neurosci. Biobehav. Rev. 2015, 57, 350–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berridge, K.C.; Robinson, T.E. Parsing Reward. Trends Neurosci. 2003, 26, 507–513. [Google Scholar] [CrossRef]
- Finlayson, G.; King, N.; Blundell, J.E. Is It Possible to Dissociate “liking” and “Wanting” for Foods in Humans? A Novel Experimental Procedure. Physiol. Behav. 2007, 90, 36–42. [Google Scholar] [CrossRef]
- Oustric, P.; Thivel, D.; Dalton, M.; Beaulieu, K.; Gibbons, C.; Hopkins, M.; Blundell, J.; Finlayson, G. Measuring Food Preference and Reward: Application and Cross-Cultural Adaptation of the Leeds Food Preference Questionnaire in Human Experimental Research. Food Qual. Prefer. 2020, 80, 103824. [Google Scholar] [CrossRef]
- Goldstone, A.P.; Miras, A.D.; Scholtz, S.; Jackson, S.; Neff, K.J.; Pénicaud, L.; Geoghegan, J.; Chhina, N.; Durighel, G.; Bell, J.D.; et al. Link between Increased Satiety Gut Hormones and Reduced Food Reward after Gastric Bypass Surgery for Obesity. J. Clin. Endocrinol. Metab. 2016, 101, 599–609. [Google Scholar] [CrossRef]
- Scholtz, S.; Miras, A.D.; Chhina, N.; Prechtl, C.G.; Sleeth, M.L.; Daud, N.M.; Ismail, N.A.; Durighel, G.; Ahmed, A.R.; Olbers, T.; et al. Obese Patients after Gastric Bypass Surgery Have Lower Brain-Hedonic Responses to Food than after Gastric Banding. Gut 2014, 63, 891–902. [Google Scholar] [CrossRef] [Green Version]
- Ochner, C.N.; Kwok, Y.; Conceicao, E.; Pantazatos, S.P.; Puma, L.M.; Carnell, S.; Teixeira, J.; Hirsch, J.; Geliebter, A. Selective Reduction in Neural Responses to High Calorie Foods Following Gastric Bypass Surgery. Ann. Surg. 2011, 253, 502–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochner, C.N.; Stice, E.; Hutchins, E.; Afifi, L.; Geliebter, A.; Hirsch, J.; Teixeira, J. Relation between Changes in Neural Responsivity and Reductions in Desire to Eat High-Calorie Foods Following Gastric Bypass Surgery. Neuroscience 2012, 209, 128–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, S.; Veit, R.; Sauer, H.; Enck, P.; Friederich, H.C.; Unholzer, T.; Bauer, U.M.; Linder, K.; Heni, M.; Fritsche, A.; et al. Dopamine Depletion Reduces Food-Related Reward Activity Independent of BMI. Neuropsychopharmacology 2016, 41, 1551–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, S.; Heinze, J.M.; Fritsche, A.; Linder, K.; von Feilitzsch, M.; Konigsrainer, A.; Haring, H.-U.; Veit, R.; Preissl, H.; Königsrainer, A.; et al. Neuronal Food Reward Activity in Patients with Type 2 Diabetes with Improved Glycemic Control After Bariatric Surgery. Diabetes Care 2016, 39, 1311–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coveleskie, K.; Gupta, A.; Kilpatrick, L.A.; Mayer, E.D.; Ashe-Mcnalley, C.; Stains, J.; Labus, J.S.; Mayer, E.A. Altered Functional Connectivity within the Central Reward Network in Overweight and Obese Women. Nutr. Diabetes 2015, 5, e148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stice, E.; Spoor, S.; Bohon, C.; Veldhuizen, M.G.; Small, D.M. Relation of Reward from Food Intake and Anticipated Food Intake to Obesity: A Functional Magnetic Resonance Imaging Study. J. Abnorm. Psychol. 2008, 117, 924–935. [Google Scholar] [CrossRef] [Green Version]
- Sanjur, D.; Randall, E.; Sanjur, D. Food Preferences—Their Conceptualization and Relationship to Consumption. Ecol. Food Nutr. 1981, 11, 151–161. [Google Scholar] [CrossRef]
- Stano, S.; Alam, F.; Wu, L.; Dutia, R.; Ng, S.N.; Sala, M.; McGinty, J.; Laferrère, B. Effect of Meal Size and Texture on Gastric Pouch Emptying and Glucagon-like Peptide 1 after Gastric Bypass Surgery. Surg. Obes. Relat. Dis. 2017, 13, 1975–1983. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.R.; Papantoni, A.; Veldhuizen, M.G.; Kamath, V.; Harris, C.; Moran, T.H.; Carnell, S.; Steele, K.E. Taste-Related Reward Is Associated with Weight Loss Following Bariatric Surgery. J. Clin. Investig. 2020, 130, 4370–4381. [Google Scholar] [CrossRef]
- van der Meij, B.S.; Wijnhoven, H.A.H.; Finlayson, G.S.; Oosten, B.S.H.; Visser, M. Specific Food Preferences of Older Adults with a Poor Appetite. A Forced-Choice Test Conducted in Various Care Settings. Appetite 2015, 90, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Kim, Y.J. Validation of the Alterable Weight Loss Metric in Morbidly Obese Patients Undergoing Gastric Bypass in Korea. Obes. Surg. 2018, 28, 1704–1710. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Pan, Y.; Han, J.; Pan, J.; Zhang, P.; Jia, W.; Bao, Y.; Yu, H. A Total Weight Loss of 25% Shows Better Predictivity in Evaluating the Efficiency of Bariatric Surgery. Int. J. Obes. 2021, 45, 396–403. [Google Scholar] [CrossRef]
- van de Laar, A.W.; de Brauw, L.M.; Meesters, E.W. Relationships between Type 2 Diabetes Remission after Gastric Bypass and Different Weight Loss Metrics: Arguments against Excess Weight Loss in Metabolic Surgery. Surg. Obes. Relat. Dis. 2016, 12, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Barragán, R.; Coltell, O.; Portolés, O.; Asensio, E.M.; Sorlí, J.V.; Ortega-Azorín, C.; González, J.I.; Sáiz, C.; Fernández-Carrión, R.; Ordovas, J.M.; et al. Bitter, Sweet, Salty, Sour and Umami Taste Perception Decreases with Age: Sex-Specific Analysis, Modulation by Genetic Variants and Taste-Preference Associations in 18 to 80 Year-Old Subjects. Nutrients 2018, 10, 1539. [Google Scholar] [CrossRef] [Green Version]
- Primeaux, S.D.; Tzeng, T.H.; Allerton, T.D.; Chiang, M.C.; Cosentino, G.; Dubin, R.L.; Varughese, A.; Moore, R.; Geiselman, P.J.; Greenway, F.L.; et al. Differences in Short-Term Food Preferences Following Vertical Sleeve Gastrectomy and Roux-En-Y Gastric Bypass Surgery. Obes. Res. Clin. Pract. 2015, 9, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Faulconbridge, L.F.; Ruparel, K.; Loughead, J.; Allison, K.C.; Hesson, L.A.; Fabricatore, A.N.; Rochette, A.; Ritter, S.; Hopson, R.D.; Sarwer, D.B.; et al. Changes in Neural Responsivity to Highly Palatable Foods Following Roux-En-Y Gastric Bypass, Sleeve Gastrectomy, or Weight Stability: An FMRI Study. Obesity 2016, 24, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Hubert, P.A.; Papasavas, P.; Stone, A.; Swede, H.; Huedo-Medina, T.B.; Tishler, D.; Duffy, V.B. Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women. Nutrients 2019, 11, 804. [Google Scholar] [CrossRef] [Green Version]
- El Labban, S.; Safadi, B.; Olabi, A. The Effect of Roux-En-Y Gastric Bypass and Sleeve Gastrectomy Surgery on Dietary Intake, Food Preferences, and Gastrointestinal Symptoms in Post-Surgical Morbidly Obese Lebanese Subjects: A Cross-Sectional Pilot Study. Obes. Surg. 2015, 25, 2393–2399. [Google Scholar] [CrossRef]
- Lewis, K.H.; Ji, M.; Bai, Y.; Arterburn, D.E.; Bhakta, B.B.; Cornejo, M.; Crawford, C.L.; Drewnowski, A.; Gray, M.F.; Moore, D.D.; et al. Bariatric Surgical Alterations in Tolerability, Enjoyment and Cravings in the Diet (BSATED) Instrument: A New Scale to Measure Food Preferences Following Bariatric Surgery. Appetite 2021, 162, 105151. [Google Scholar] [CrossRef]
- Ramadan, M.; Loureiro, M.; Laughlan, K.; Caiazzo, R.; Iannelli, A.; Brunaud, L.; Czernichow, S.; Nedelcu, M.; Nocca, D. Risk of Dumping Syndrome after Sleeve Gastrectomy and Roux-En-Y Gastric Bypass: Early Results of a Multicentre Prospective Study. Gastroenterol. Res. Pract. 2016, 2016, 2570237. [Google Scholar] [CrossRef] [Green Version]
- Simpson, S.J.; Raubenheimer, D. Obesity: The Protein Leverage Hypothesis. Obes. Rev. 2005, 6, 133–142. [Google Scholar] [CrossRef]
- Raubenheimer, D.; Simpson, S.J. Protein Leverage: Theoretical Foundations and Ten Points of Clarification. Obesity 2019, 27, 1225–1238. [Google Scholar] [CrossRef]
- Champeil-Potokar, G.; Crossouard, L.; Jérôme, N.; Ouali, C.; Darcel, N.; Davidenko, O.; Rampin, O.; Bombail, V.; Denis, I. Diet Protein Content and Individual Phenotype Affect Food Intake and Protein Appetence in Rats. J. Nutr. 2021, 151, 1311–1319. [Google Scholar] [CrossRef]
- Oustric, P.; Gibbons, C.; Beaulieu, K.; Blundell, J.; Finlayson, G. Changes in Food Reward during Weight Management Interventions—A Systematic Review. Obes. Rev. 2018, 19, 1642–1658. [Google Scholar] [CrossRef]
- Lynch, A. “When the Honeymoon Is over, the Real Work Begins:” Gastric Bypass Patients’ Weight Loss Trajectories and Dietary Change Experiences. Soc. Sci. Med. 2016, 151, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Kittrell, H.; Graber, W.; Mariani, E.; Czaja, K.; Hajnal, A.; Lorenzo, P.M.D. Taste and Odor Preferences Following Roux-En-Y Surgery in Humans. PLoS ONE 2018, 13, e0199508. [Google Scholar] [CrossRef]
- Brolin, R.E.; Robertson, L.B.; Kenler, H.A.; Cody, R.P. Weight Loss and Dietary Intake After Vertical Banded Gastroplasty and Roux-En-Y Gastric Bypass. Ann. Surg. 1994, 220, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Oustric, P.; Beaulieu, K.; Casanova, N.; O’Connor, D.; Gibbons, C.; Hopkins, M.; Blundell, J.; Finlayson, G. Food Liking but Not Wanting Decreases after Controlled Intermittent or Continuous Energy Restriction to ≥5% Weight Loss in Women with Overweight/Obesity. Nutrients 2021, 13, 182. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Lindroos, A.K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D.; et al. Lifestyle, Diabetes, and Cardiovascular Risk Factors 10 Years after Bariatric Surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef]
- Rozin, P. The Socio-Cultural Context of Eating and Food Choice. In Food Choice, Acceptance and Consumption; Springer: Berlin, Germany, 1996; pp. 83–104. [Google Scholar] [CrossRef]
- Enriquez, J.P.; Archila-Godinez, J.C. Social and Cultural Influences on Food Choices: A Review. Crit. Rev. Food Sci. Nutr. 2021, 11, 1–7. [Google Scholar] [CrossRef]


{kind=link}
| Task | Studied Dimensions | Combined Food Categories |
|---|---|---|
| 1 | High carbohydrates (HC)/Low carbohydrates (LC) Solid (SO)/Fluid (FL) | HC—SO HC—FL LC—SO LC—FL |
| 2 | Dairy (DA)/Non-dairy (ND) Color (CO)/No color (NC) | DA—CO DA—NC ND—CO ND—NC |
| 3 | High fat (HF)/Low fat (LF) Savory (SA)/Sweet (SW) | HF—SA HF—SW LF—SA LF—SW |
| 4 | Fiber (FI)/No fiber (NF) Sauce (SC)/No sauce (NS) | FI—SC FI—NS NF—SC NF—NS |
| 5 | Meat (ME)/No meat (NM) High fat (HF)/Low fat (LF) | ME—HF ME—LF NM—HF NM—LF |
| 6 | High protein (HP)/Low protein (LP) Variation (VA)/No variation (NV) | HP—VA HP—NV LP—VA LP—NV |
| All n = 56 | SG n = 30 | RYGB n = 26 | p-Value | |
|---|---|---|---|---|
| Sociodemographic data | ||||
| Women (%) | 75.0 (n = 42) | 76.7 (n = 23) | 73.1(n = 19) | 0.757 |
| Age (year) | 44.0 (11.1) | 38.3 (9.6) | 50.5 (9.0) | <0.001 |
| Smoking status (%) | 19.6 (n = 11) | 20.0 (n = 6) | 19.2 (n = 5) | 0.942 |
| Food budget constraint (%) | 14.3 | 10.0 | 19.2 | 0.451 a |
| Anthropometric data | ||||
| BMI Before surgery(kg/m2) | 43.6 (6.0) | 45.5 (5.9) | 41.4 (4.4) | 0.011 |
| Body weight (kg) | 87.8 (17.8) | 88.2 (20.3) | 87.3 (14.7) | 0.843 |
| BMI (kg/m2) † | 31.4 (4.5) | 31.5 (4.5) | 31.2 (4.6) | 0.846 |
| %TWL | 27.7 (7.3) | 30.6 (6.3) | 24.3 (7.0) | <0.001 |
| Appetite sensations | ||||
| Mean hunger (mm) | 21.0 (25.7) | 25.2 (28.7) | 16.2 (21.5) | 0.196 |
| Mean fullness (mm) | 68.3 (28.0) | 68.7 (27.6) | 67.8 (29.0) | 0.909 |
| Mean desire to eat (mm) | 22.2 (24.8) | 25.6 (28.2) | 18.2 (19.8) | 0.252 |
| Time since last meal (min) | 134 (214) | 154 (237) | 109 (184) | 0.434 |
| Low Responders <33% | Middle Responders 33–66% | Good Responders >66% | ANOVA p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 18 | n = 19 | n = 19 | ||||||||
| Mean | SD | Mean | SD | Mean | SD | |||||
| High carb—Solid | 22.2 | ± | 20.0 | 30.1 | ± | 26.9 | 26.1 | ± | 21.9 | 0.581 |
| High carb—Fluid | 19.2 | ± | 15.7 | 29.1 | ± | 24.5 | 27.2 | ± | 21.2 | 0.323 |
| Low carb—Solid | 21.4 | ± | 23.6 | 30.4 | ± | 25.5 | 39.5 | ± | 28.1 | 0.113 |
| Low carb—Fluid | 20.3 | ± | 18.2 | 30.8 | ± | 31.4 | 21.9 | ± | 21.3 | 0.373 |
| Dairy—Color | 17.0 | ± | 14.5 | 22.3 | ± | 23.9 | 28.5 | ± | 25.7 | 0.303 |
| Dairy—No color | 21.1 | ± | 14.8 | 28.6 | ± | 27.2 | 33.7 | ± | 26.0 | 0.290 |
| Non-dairy—Color | 16.6 | ± | 19.1 | 20.4 | ± | 19.2 | 26.0 | ± | 26.0 | 0.433 |
| Non-dairy—No color | 19.3 | ± | 19.0 | 20.2 | ± | 18.8 | 31.4 | ± | 23.8 | 0.147 |
| High fat—Savory | 19.0 | ± | 23.5 | 25.2 | ± | 22.0 | 36.2 | ± | 30.2 | 0.126 |
| High fat—Sweet | 19.5 | ± | 20.1 | 26.2 | ± | 24.5 | 28.8 | ± | 29.8 | 0.521 |
| Low fat—Savory | 9.7 | ± | 10.1 | 22.4 | ± | 20.6 | 24.6 | ± | 22.3 | 0.040 a |
| Low fat—Sweet | 22.8 | ± | 19.7 | 29.3 | ± | 27.4 | 32.7 | ± | 24.4 | 0.458 |
| Fiber—Sauce | 21.3 | ± | 18.1 | 30.4 | ± | 26.4 | 35.3 | ± | 25.0 | 0.196 |
| Fiber—No sauce | 19.2 | ± | 13.6 | 29.1 | ± | 26.2 | 29.0 | ± | 24.4 | 0.309 |
| No fiber—Sauce | 21.5 | ± | 19.5 | 25.9 | ± | 24.1 | 36.1 | ± | 26.9 | 0.166 |
| No fiber—No sauce | 27.6 | ± | 26.3 | 30.5 | ± | 27.3 | 36.0 | ± | 23.6 | 0.602 |
| Meat—High fat | 18.7 | ± | 22.6 | 28.6 | ± | 27.2 | 38.7 | ± | 30.2 | 0.087 b |
| Meat—Low fat | 22.5 | ± | 24.1 | 31.5 | ± | 30.6 | 39.3 | ± | 32.9 | 0.232 |
| No meat—High fat | 18.4 | ± | 18.8 | 25.7 | ± | 21.3 | 39.3 | ± | 31.5 | 0.038 c |
| No meat—Low fat | 16.9 | ± | 15.5 | 25.6 | ± | 23.1 | 27.9 | ± | 23.2 | 0.259 |
| High protein—Variation | 18.6 | ± | 22.9 | 29.2 | ± | 25.8 | 40.3 | ± | 25.1 | 0.035 d |
| High protein—No variation | 23.9 | ± | 29.1 | 31.2 | ± | 27.2 | 42.9 | ± | 28.7 | 0.129 |
| Low protein—Variation | 24.6 | ± | 20.2 | 30.0 | ± | 22.7 | 35.2 | ± | 24.0 | 0.366 |
| Low protein—No variation | 24.3 | ± | 21.3 | 32.3 | ± | 25.0 | 36.6 | ± | 23.1 | 0.274 |
| Low Responders <33% | Middle Responders 33–66% | Good Responders >66% | ANOVA p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 18 | n = 19 | n = 19 | ||||||||
| Mean | SD | Mean | SD | Mean | SD | |||||
| High carb—Solid | 20.6 | ± | 21.5 | 29.1 | ± | 26.5 | 23.2 | ± | 21.4 | 0.532 |
| High carb—Fluid | 17.4 | ± | 15.7 | 26.5 | ± | 23.9 | 23.4 | ± | 19.1 | 0.376 |
| Low carb—Solid | 19.9 | ± | 22.8 | 26.6 | ± | 24.4 | 38.0 | ± | 29.1 | 0.103 |
| Low carb—Fluid | 18.5 | ± | 18.6 | 28.2 | ± | 31.4 | 22.9 | ± | 21.5 | 0.483 |
| Dairy—Color | 14.8 | ± | 12.8 | 21.5 | ± | 24.4 | 26.7 | ± | 26.5 | 0.288 |
| Dairy—No color | 21.1 | ± | 16.7 | 29.4 | ± | 28.8 | 29.8 | ± | 23.0 | 0.464 |
| Non-dairy—Color | 14.4 | ± | 16.8 | 21.4 | ± | 20.4 | 22.9 | ± | 26.2 | 0.460 |
| Non-dairy—No color | 17.4 | ± | 16.6 | 20.2 | ± | 21.3 | 29.4 | ± | 25.0 | 0.215 |
| High fat—Savory | 17.0 | ± | 21.8 | 24.3 | ± | 23.0 | 34.6 | ± | 29.7 | 0.110 |
| High fat—Sweet | 18.1 | ± | 21.1 | 23.8 | ± | 24.1 | 23.9 | ± | 26.6 | 0.706 |
| Low fat—Savory | 9.2 | ± | 8.5 | 21.2 | ± | 21.0 | 23.2 | ± | 22.1 | 0.052 a |
| Low fat—Sweet | 23.2 | ± | 21.1 | 27.9 | ± | 25.9 | 32.0 | ± | 25.1 | 0.547 |
| Fiber—Sauce | 22.8 | ± | 20.0 | 28.6 | ± | 27.5 | 36.1 | ± | 26.9 | 0.279 |
| Fiber—No sauce | 16.9 | ± | 13.1 | 27.8 | ± | 26.9 | 27.3 | ± | 23.5 | 0.249 |
| No fiber—Sauce | 19.5 | ± | 19.0 | 26.6 | ± | 25.3 | 34.2 | ± | 25.0 | 0.169 |
| No fiber—No sauce | 25.8 | ± | 23.2 | 31.2 | ± | 28.5 | 35.7 | ± | 24.9 | 0.510 |
| Meat—High fat | 18.4 | ± | 22.3 | 28.0 | ± | 27.3 | 34.3 | ± | 28.4 | 0.189 |
| Meat—Low fat | 22.4 | ± | 26.7 | 30.7 | ± | 32.1 | 37.2 | ± | 32.4 | 0.343 |
| No meat—High fat | 16.6 | ± | 17.1 | 25.7 | ± | 22.1 | 36.9 | ± | 29.2 | 0.038 b |
| No meat—Low fat | 14.3 | ± | 13.6 | 25.2 | ± | 23.2 | 25.8 | ± | 22.3 | 0.168 |
| High protein—Variation | 18.1 | ± | 22.3 | 32.0 | ± | 31.6 | 37.4 | ± | 26.0 | 0.092 c |
| High protein—No variation | 21.8 | ± | 27.6 | 33.1 | ± | 32.0 | 40.8 | ± | 30.6 | 0.166 |
| Low protein—Variation | 22.9 | ± | 18.5 | 30.1 | ± | 25.8 | 32.8 | ± | 25.0 | 0.423 |
| Low protein—No variation | 24.0 | ± | 19.7 | 32.9 | ± | 29.8 | 36.3 | ± | 24.8 | 0.321 |
| Low Responders <33% | Middle Responders 33–66% | Good Responders >66% | ANOVA p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 18 | n = 19 | n = 19 | ||||||||
| Mean | SD | Mean | SD | Mean | SD | |||||
| High carb—Solid | 0.94 | ± | 27.62 | −2.16 | ± | 30.98 | −5.98 | ± | 22.97 | 0.744 |
| High carb—Fluid | −7.82 | ± | 21.69 | −3.84 | ± | 21.92 | −6.92 | ± | 18.35 | 0.828 |
| Low carb—Solid | 15.84 | ± | 27.92 | 9.60 | ± | 30.85 | 34.78 | ± | 15.74 | 0.011 a |
| Low carb—Fluid | −8.96 | ± | 33.35 | −3.60 | ± | 34.57 | −21.88 | ± | 30.60 | 0.222 |
| Dairy—Color | −2.95 | ± | 17.49 | −7.88 | ± | 33.79 | −2.74 | ± | 26.68 | 0.804 |
| Dairy—No color | 23.14 | ± | 29.23 | 26.66 | ± | 24.16 | 22.36 | ± | 18.97 | 0.846 |
| Non-dairy—Color | −24.27 | ± | 29.86 | −13.89 | ± | 21.12 | −27.71 | ± | 15.79 | 0.163 |
| Non-dairy—No color | 4.08 | ± | 24.58 | −4.89 | ± | 29.03 | 8.10 | ± | 29.33 | 0.345 |
| High fat—Savory | 2.86 | ± | 28.82 | 2.55 | ± | 16.86 | 19.26 | ± | 25.88 | 0.071 b |
| High fat—Sweet | −4.41 | ± | 30.22 | 0.13 | ± | 24.89 | −8.23 | ± | 20.57 | 0.619 |
| Low fat—Savory | −11.87 | ± | 38.09 | −18.35 | ± | 28.48 | −16.33 | ± | 28.15 | 0.819 |
| Low fat—Sweet | 15.41 | ± | 23.65 | 6.61 | ± | 20.30 | 5.30 | ± | 20.49 | 0.321 |
| Fiber—Sauce | 0.79 | ± | 20.09 | 3.39 | ± | 17.73 | −2.34 | ± | 24.25 | 0.705 |
| Fiber—No sauce | −14.02 | ± | 26.57 | −4.94 | ± | 22.10 | −16.39 | ± | 23.48 | 0.317 |
| No fiber—Sauce | −6.13 | ± | 22.25 | −7.36 | ± | 20.55 | 3.86 | ± | 15.33 | 0.164 |
| No fiber—No sauce | 18.33 | ± | 22.80 | 8.91 | ± | 16.04 | 14.88 | ± | 20.46 | 0.359 |
| Meat—High fat | 11.10 | ± | 22.44 | 1.79 | ± | 20.95 | 10.32 | ± | 15.20 | 0.287 |
| Meat—Low fat | 11.94 | ± | 18.73 | 4.98 | ± | 24.06 | 7.98 | ± | 18.81 | 0.605 |
| No meat—High fat | −11.69 | ± | 20.54 | 0.27 | ± | 27.73 | 6.46 | ± | 13.73 | 0.046 c |
| No meat—Low fat | −5.49 | ± | 32.93 | −10.29 | ± | 29.78 | −24.75 | ± | 18.28 | 0.095 d |
| High protein—Variation | −5.30 | ± | 18.12 | −3.27 | ± | 31.69 | 1.89 | ± | 18.25 | 0.635 |
| High protein—No variation | 5.25 | ± | 18.82 | 7.18 | ± | 22.66 | 21.69 | ± | 20.87 | 0.038 e |
| Low protein—Variation | −1.93 | ± | 17.00 | −5.17 | ± | 19.67 | −14.85 | ± | 14.16 | 0.064 f |
| Low protein—No variation | 1.98 | ± | 16.08 | 1.26 | ± | 25.70 | −8.73 | ± | 17.68 | 0.206 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guyot, E.; Nazare, J.-A.; Oustric, P.; Robert, M.; Disse, E.; Dougkas, A.; Iceta, S. Food Reward after Bariatric Surgery and Weight Loss Outcomes: An Exploratory Study. Nutrients 2022, 14, 449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030449
Guyot E, Nazare J-A, Oustric P, Robert M, Disse E, Dougkas A, Iceta S. Food Reward after Bariatric Surgery and Weight Loss Outcomes: An Exploratory Study. Nutrients. 2022; 14(3):449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030449
Chicago/Turabian StyleGuyot, Erika, Julie-Anne Nazare, Pauline Oustric, Maud Robert, Emmanuel Disse, Anestis Dougkas, and Sylvain Iceta. 2022. "Food Reward after Bariatric Surgery and Weight Loss Outcomes: An Exploratory Study" Nutrients 14, no. 3: 449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14030449