
Multilevel Analysis of the Nutritional and Health Status among Children and Adolescents in Eastern China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Ethics Approval and Consent to Participate
2.3. Data Collection and Measurements
2.4. Diagnostic Criteria and Definitions
- (1)
- Abdominal obesity, where WC ≥ age- and gender-specific 90th percentile [29];
- (2)
- Elevated triglyceride (TG), where TG ≥ 1.24 mmol/L;
- (3)
- Low high-density lipoprotein (HDL), where HDL ≤ 1.03 mmol/L;
- (4)
- Elevated blood pressure, where systolic blood pressure (SBP) or diastolic blood pressure (DBP) ≥ 90th percentile for gender, age, and height [30];
- (5)
- Elevated fasting blood glucose (FBG), where glucose ≥ 6.1 mmol/L.
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Research Populations
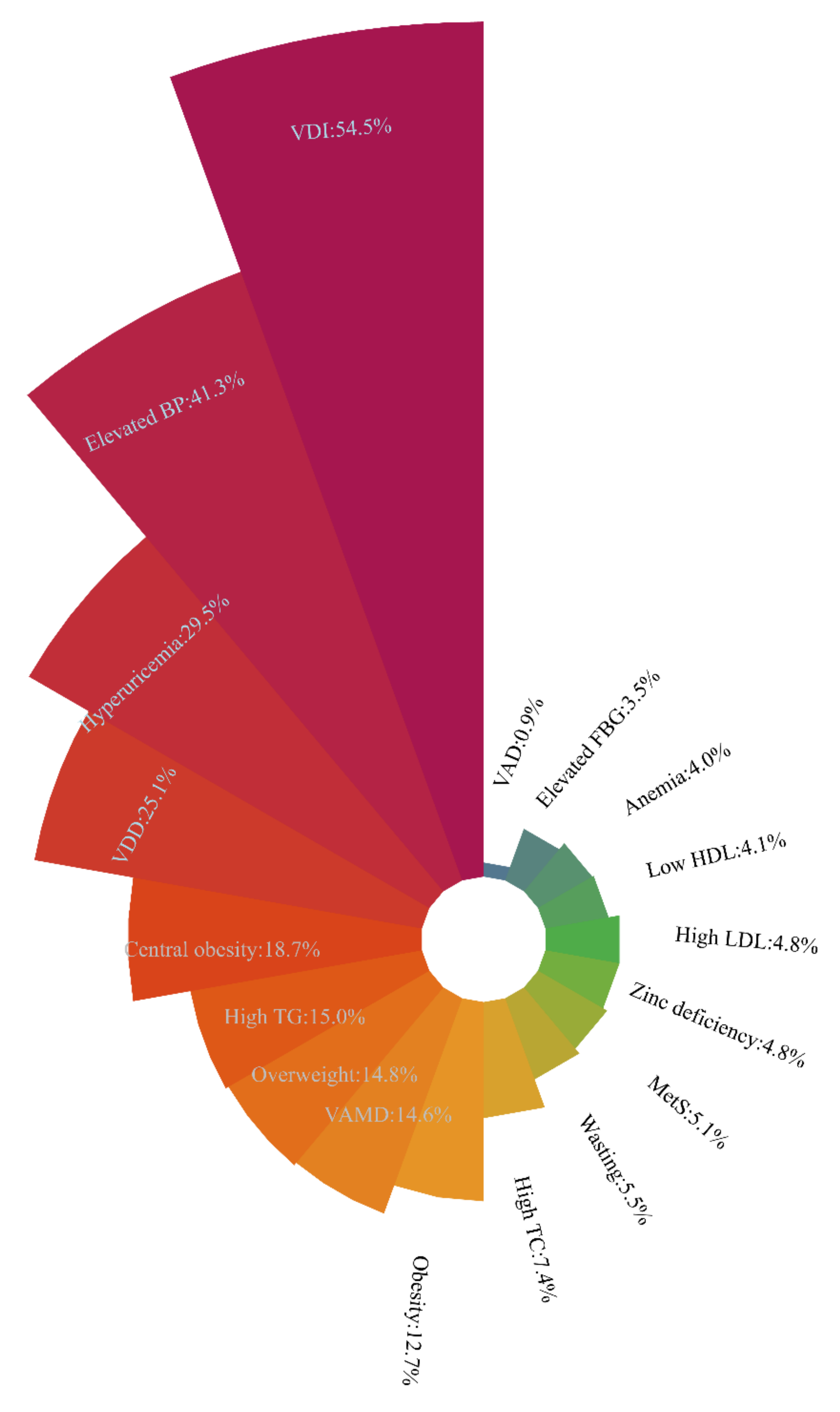
3.2. Nutritional and Health Statuses of School-Age Children and Adolescents
3.3. Related Factors Associated with Various Nutritional Diseases
3.4. The Relevant Factors of Overnutrition- and Undernutrtion-Related Disorders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Millward, D.J. Nutrition, infection and stunting: The roles of deficiencies of individual nutrients and foods, and of inflammation, as determinants of reduced linear growth of children. Nutr. Res. Rev. 2017, 30, 50–72. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.M.; Suchdev, P.S. Assessing and Improving Childhood Nutrition and Growth Globally. Pediatric Clin. N. Am. 2017, 64, 755–768. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Genovesi, S.; Parati, G. Cardiovascular Risk in Children: Focus on Pathophysiological Aspects. Int. J. Mol. Sci. 2020, 21, 6612. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.; Twig, G. The Impact of Childhood and Adolescent Obesity on Cardiovascular Risk in Adulthood: A Systematic Review. Curr. Diabetes Rep. 2018, 18, 91. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Berkley, J.A.; Bandsma, R.; Kerac, M.; Trehan, I.; Briend, A. Severe childhood malnutrition. Nat. Rev. Dis. Primers 2017, 3, 17067. [Google Scholar] [CrossRef]
- Jahan, I.; Muhit, M.; Hardianto, D.; Laryea, F.; Amponsah, S.K.; Chhetri, A.B.; Smithers-Sheedy, H.; McIntyre, S.; Badawi, N.; Khandaker, G. Epidemiology of Malnutrition among Children with Cerebral Palsy in Low- and Middle-Income Countries: Findings from the Global LMIC CP Register. Nutrients 2021, 13, 3637. [Google Scholar] [CrossRef] [PubMed]
- Perez-Escamilla, R.; Bermudez, O.; Buccini, G.S.; Kumanyika, S.; Lutter, C.K.; Monsivais, P.; Victora, C. Nutrition disparities and the global burden of malnutrition. BMJ 2018, 361, k2252. [Google Scholar] [CrossRef]
- Song, P.; Wang, J.; Wei, W.; Chang, X.; Wang, M.; An, L. The Prevalence of Vitamin A Deficiency in Chinese Children: A Systematic Review and Bayesian Meta-Analysis. Nutrients 2017, 9, 1285. [Google Scholar] [CrossRef] [Green Version]
- Huh, S.Y.; Gordon, C.M. Vitamin D deficiency in children and adolescents: Epidemiology, impact and treatment. Rev. Endocr. Metab. Disord. 2008, 9, 161–170. [Google Scholar] [CrossRef]
- Li, H.; Xiao, J.; Liao, M.; Huang, G.; Zheng, J.; Wang, H.; Huang, Q.; Wang, A. Anemia prevalence, severity and associated factors among children aged 6-71 months in rural Hunan Province, China: A community-based cross-sectional study. BMC Public Health 2020, 20, 989. [Google Scholar] [CrossRef] [PubMed]
- Iglesias Vázquez, L.; Valera, E.; Villalobos, M.; Tous, M.; Arija, V. Prevalence of Anemia in Children from Latin America and the Caribbean and Effectiveness of Nutritional Interventions: Systematic Review and Meta-Analysis. Nutrients 2019, 11, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Piao, J.; Zhang, Y.; He, Y.; Li, W.; Yang, L.; Yang, X. Assessment of Zinc Status in School-Age Children from Rural Areas in China Nutrition and Health Survey 2002 and 2012. Biol. Trace Elem. Res. 2017, 178, 194–200. [Google Scholar] [CrossRef]
- Dong, Y.; Jan, C.; Ma, Y.; Dong, B.; Zou, Z.; Yang, Y.; Xu, R.; Song, Y.; Ma, J.; Sawyer, S.M.; et al. Economic development and the nutritional status of Chinese school-aged children and adolescents from 1995 to 2014: An analysis of five successive national surveys. The lancet. Diabetes Endocrinol. 2019, 7, 288–299. [Google Scholar] [CrossRef]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; GBD 2015 Obesity Collaborators; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- DeBoer, M.D. Assessing and Managing the Metabolic Syndrome in Children and Adolescents. Nutrients 2019, 11, 1788. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.M.; Gurka, M.J.; DeBoer, M.D. Trends in Metabolic Syndrome Severity and Lifestyle Factors among Adolescents. Pediatrics 2016, 137, e20153177. [Google Scholar] [CrossRef] [Green Version]
- Song, P.; Yu, J.; Chang, X.; Wang, M.; An, L. Prevalence and Correlates of Metabolic Syndrome in Chinese Children: The China Health and Nutrition Survey. Nutrients 2017, 9, 79. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Zhang, S.; Li, W.; Wang, L.; Liu, H.; Li, W.; Zhang, T.; Liu, G.; Du, Y.; Leng, J. Prevalence of hyperuricemia and its related risk factors among preschool children from China. Sci. Rep. 2017, 7, 9448. [Google Scholar] [CrossRef] [Green Version]
- Kumar, J.; Gupta, A.; Dev, K.; Kumar, S.; Kataria, D.; Gul, A.; Abbas, M.; Jamil, A.; Shahid, S.; Memon, S. Prevalence and Causes of Hyperuricemia in Children. Cureus 2021, 13, e15307. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; Cook, S.; Choi, H.K. Serum concentrations of uric acid and the metabolic syndrome among US children and adolescents. Circulation 2007, 115, 2526–2532. [Google Scholar] [CrossRef] [Green Version]
- Mia, M.N.; Rahman, M.S.; Roy, P.K. Sociodemographic and geographical inequalities in under- and overnutrition among children and mothers in Bangladesh: A spatial modelling approach to a nationally representative survey. Public Health Nutr. 2018, 21, 2471–2481. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, C.; Guzmán-Guzmán, I.P.; Latorre-Román, P.Á.; Párraga-Montilla, J.; Palomino-Devia, C.; Reyes-Oyola, F.A.; Paredes-Arévalo, L.; Leal-Oyarzún, M.; Obando-Calderón, I.; Cresp-Barria, M.; et al. Association between the Sociodemographic Characteristics of Parents with Health-Related and Lifestyle Markers of Children in Three Different Spanish-Speaking Countries: An Inter-Continental Study at OECD Country Level. Nutrients 2021, 13, 2672. [Google Scholar] [CrossRef] [PubMed]
- Zach, A.; Meyer, N.; Hendrowarsito, L.; Kolb, S.; Bolte, G.; Nennstiel-Ratzel, U.; Stilianakis, N.I.; Herr, C.; GME Study Group. Association of sociodemographic and environmental factors with the mental health status among preschool children-Results from a cross-sectional study in Bavaria, Germany. Int. J. Hyg. Environ. Health 2016, 219, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982-2017). China CDC Wkly. 2021, 3, 193–195. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of People’s Republic of China. Screening Standard for Malnutrition of School-Age Children and Adolescents; WS/T 456-2014; National Health and Family Planning Commission of People’s Republic of China: Beijing, China, 2014. [Google Scholar]
- National Health and Family Planning Commission of People’s Republic of China. Screening for Overweight and Obesity among School-Age Children and Adolescents; WST 586-2018; National Health and Family Planning Commission of People’s Republic of China: Beijing, China, 2018. [Google Scholar]
- Cook, S.; Weitzman, M.; Auinger, P.; Nguyen, M.; Dietz, W.H. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Arch. Pediatrics Adolesc. Med. 2003, 157, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, P.; Li, X.; Gasevic, D.; Flores, A.B.; Yu, Z. BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents. Int. J. Environ. Res. Public Health 2016, 13, 589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Ma, J.; Song, Y.; Dong, B.; Wang, Z.; Yang, Z.; Wang, X.; Prochaska, J.J. National Blood Pressure Reference for Chinese Han Children and Adolescents Aged 7 to 17 Years. Hypertension 2017, 70, 897–906. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Okumura, M.J.; Davis, M.M.; Herman, W.H.; Gurney, J.G. Prevalence and determinants of insulin resistance among U.S. adolescents: A population-based study. Diabetes Care 2006, 29, 2427–2432. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- World Health Organization. Iron deficiency anaemia: Assessment, Prevention, and Control; A guide for Programme Managers; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Liu, J.; Hanlon, A.; Ma, C.; Zhao, S.R.; Cao, S.; Compher, C. Low blood zinc, iron, and other sociodemographic factors associated with behavior problems in preschoolers. Nutrients 2014, 6, 530–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.H.; Wang, Z.H.; Yang, Z.G.; Wang, X.J.; Chen, Y.J.; Zou, Z.Y.; Ma, J. Epidemic status and secular trends of malnutrition among children and adolescents aged 7-18 years from 2005 to 2014 in China. Beijing da xue xue bao. Yi xue ban J. Peking Univ. Health Sci. 2017, 49, 424–432. [Google Scholar]
- Hu, X.; Jiang, H.; Wang, H.; Zhang, B.; Zhang, J.; Jia, X.; Wang, L.; Wang, Z.; Ding, G. Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6-17 Years: Evidence from the China Health and Nutrition Survey 2015. Nutrients 2021, 13, 3097. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007-2008 to 2015-2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Bovet, P.; Ma, C.; Zhao, M.; Liang, Y.; Xi, B. Prevalence of underweight and overweight among young adolescents aged 12-15 years in 58 low-income and middle-income countries. Pediatric Obes. 2019, 14, e12468. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A.; Min, J.; Xue, H.; Kaminsky, L.A.; Cheskin, L.J. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int. J. Epidemiol. 2020, 49, 810–823. [Google Scholar] [CrossRef]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, H.; Hu, Y.C.; Chen, J.; Yang, Z.; Zhao, L.; Yang, L. Serum Vitamin A Nutritional Status of Children and Adolescents Aged 6-17 Years—China, 2016-2017. China CDC Wkly. 2021, 3, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Shen, G.; Jiang, S.; Xu, H.; Li, M.; Wang, Z.; Zhang, S.; Yu, Y. Nutrient Status of Vitamin D among Chinese Children. Nutrients 2017, 9, 319. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.L.; Wang, H.Y.; Wen, H.K.; Tao, H.Q.; Zhao, X.W. Vitamin D status among infants, children, and adolescents in southeastern China. J. Zhejiang Univ. Sci. B 2016, 17, 545–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Hu, Y.; Li, M.; Chen, J.; Mao, D.; Li, W.; Wang, R.; Yang, Y.; Piao, J.; Yang, L.; et al. Prevalence of Anemia in Chinese Children and Adolescents and Its Associated Factors. Int. J. Environ. Res. Public Health 2019, 16, 1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Li, Y.; Liu, A.; Zhang, Q.; Hu, X.; Fang, H.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Prevalence of the metabolic syndrome among children from six cities of China. BMC Public Health 2012, 12, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, C.; Wang, C.; Xia, F.; Liu, Z.; Mo, Y.; Shan, X.; Zhou, Y. Age and Gender-Specific Reference Intervals for Uric Acid Level in Children Aged 5-14 Years in Southeast Zhejiang Province of China: Hyperuricemia in Children May Need Redefinition. Front. Pediatrics 2021, 9, 560720. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Chen, J.; Liu, Z.; Yun, C.; Li, Y.; Piao, J.; Yang, X. Association of Vitamin A Status with Overnutrition in Children and Adolescents. Int. J. Environ. Res. Public Health 2015, 12, 15531–15539. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A. Vitamin A: Biomarkers of nutrition for development. Am. J. Clin. Nutr. 2011, 94, 658S–665S. [Google Scholar] [CrossRef] [Green Version]
- Zhong, M.; Kawaguchi, R.; Kassai, M.; Sun, H. Retina, retinol, retinal and the natural history of vitamin A as a light sensor. Nutrients 2012, 4, 2069–2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brett, N.R.; Lavery, P.; Agellon, S.; Vanstone, C.A.; Goruk, S.; Field, C.J.; Weiler, H.A. Vitamin D Status and Immune Health Outcomes in a Cross-Sectional Study and a Randomized Trial of Healthy Young Children. Nutrients 2018, 10, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wimalawansa, S.J. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J. Steroid Biochem. Mol. Biol. 2018, 175, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R.; Farajzadegan, Z.; Bahreynian, M. Association between vitamin D status and lipid profile in children and adolescents: A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2014, 65, 404–410. [Google Scholar] [CrossRef]
- Zittermann, A.; Gummert, J.F.; Börgermann, J. The role of vitamin D in dyslipidemia and cardiovascular disease. Curr. Pharm. Des. 2011, 17, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Mao, M.; Ping, L.; Yu, D. Prevalence of vitamin D deficiency and insufficiency among 460,537 children in 825 hospitals from 18 provinces in mainland China. Medicine 2020, 99, e22463. [Google Scholar] [CrossRef]
- Li, H.; Huang, T.; Xiao, P.; Zhao, X.; Liu, J.; Cheng, H.; Dong, H.; Morris, H.A.; Mi, J.; China Child and Adolescent Cardiovascular Health (CCACH) Collaboration Group. Widespread vitamin D deficiency and its sex-specific association with adiposity in Chinese children and adolescents. Nutrition 2020, 71, 110646. [Google Scholar] [CrossRef]
- Borrud, L.G.; Flegal, K.M.; Looker, A.C.; Everhart, J.E.; Harris, T.B.; Shepherd, J.A. Body Composition Data for Individuals 8 Years of Age and Older: U.S. Population, 1999–2004; Vital and Health Statistics Series 11; Data from the National Health Survey; U.S. Department of Health and Human Services: Washington, DC, USA, 2010; pp. 1–87. [Google Scholar]
- Hazell, T.J.; DeGuire, J.R.; Weiler, H.A. Vitamin D: An overview of its role in skeletal muscle physiology in children and adolescents. Nutr. Rev. 2012, 70, 520–533. [Google Scholar] [CrossRef]
- Alfredsson, L.; Armstrong, B.K.; Butterfield, D.A.; Chowdhury, R.; de Gruijl, F.R.; Feelisch, M.; Garland, C.F.; Hart, P.H.; Hoel, D.G.; Jacobsen, R.; et al. Insufficient Sun Exposure Has Become a Real Public Health Problem. Int. J. Environ. Res. Public Health 2020, 17, 5014. [Google Scholar] [CrossRef]
- Wong, A.Y.; Chan, E.W.; Chui, C.S.; Sutcliffe, A.G.; Wong, I.C. The phenomenon of micronutrient deficiency among children in China: A systematic review of the literature. Public Health Nutr. 2014, 17, 2605–2618. [Google Scholar] [CrossRef] [Green Version]
- Ma, G.; Li, Y.; Jin, Y.; Zhai, F.; Kok, F.J.; Yang, X. Phytate intake and molar ratios of phytate to zinc, iron and calcium in the diets of people in China. Eur. J. Clin. Nutr. 2007, 61, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Bécares, L.; Chandola, T. Patterns and Determinants of Double-Burden of Malnutrition among Rural Children: Evidence from China. PLoS ONE 2016, 11, e0158119. [Google Scholar] [CrossRef] [Green Version]
- Ning, M.; Chang, H.H. Migration decisions of parents and the nutrition intakes of children left at home in rural China. Agric. Econ. 2013, 59, 467–477. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Li, X.; Li, Y.; Zhang, S.; Liu, L.; Wang, X.; Li, W. Anemia, malnutrition and their correlations with socio-demographic characteristics and feeding practices among infants aged 0-18 months in rural areas of Shaanxi province in northwestern China: A cross-sectional study. BMC Public Health 2012, 12, 1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Su, X.; Wang, C.; Zhang, L.; Zhang, X.; Wang, L.; Cui, Y. Prevalence and risk factors for stunting and severe stunting among children under three years old in mid-western rural areas of China. Child Care Health Dev. 2015, 41, 45–51. [Google Scholar] [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Wang, D.; Shen, H.; Yu, L.; Gao, Q.; Mao, L.; Jiang, F.; Luo, Y.; Xie, M.; Zhang, Y.; et al. Physical activity and health in Chinese children and adolescents: Expert consensus statement (2020). Br. J. Sports Med. 2020, 54, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Esquivel, J.H.; Guo, J.; Chesla, C.A.; Tang, S. Risk factors for obesity in preschool-aged children in China. Int. Nurs. Rev. 2018, 65, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Gan, X.; Xu, W.; Yu, K. Economic Growth and Weight of Children and Adolescents in Urban Areas: A Panel Data Analysis on Twenty-Seven Provinces in China, 1985-2014. Child. Obes. 2020, 16, 86–93. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Males (%) | Females (%) | All n = 3025 | t or χ2 Values | p Value |
|---|---|---|---|---|---|
| n= 1520 | n = 1505 | ||||
| Age (years) | 11.4 ± 3.0 | 11.4 ± 3.0 | 11.4 ± 3.0 | 0.074 | 0.941 |
| Age group | 0.089 | 0.765 | |||
| 7–12 years | 990 (65.1) | 988 (65.6) | 1978 (65.4) | ||
| 13–17 years | 530 (34.9) | 517 (34.4) | 1047 (34.6) | ||
| Living area | 0.001 | 0.982 | |||
| Urban | 1272 (83.7) | 1259 (83.7) | 2531 (83.7) | ||
| Rural | 248 (16.3) | 246 (16.3) | 494 (16.3) | ||
| Physical activity | 0.613 | 0.434 | |||
| Low | 907 (59.7) | 919 (61.1) | 1826 (60.4) | ||
| High | 613 (40.3) | 586 (38.9) | 1199 (39.6) | ||
| Screen time | 3.432 | 0.064 | |||
| Low | 1320 (86.8) | 1340 (89.0) | 2660 (87.9) | ||
| High | 200 (13.2) | 165 (11.0) | 365 (12.1) | ||
| Age of mother | 0.170 | 0.680 | |||
| ≤37 (median) | 783 (51.5) | 764 (50.8) | 1547 (51.1) | ||
| ≥38 | 737 (48.5) | 741 (49.2) | 1478 (48.9) | ||
| Age of father | 0.389 | 0.533 | |||
| ≤39 (median) | 806 (53.0) | 781 (51.9) | 1587 (52.5) | ||
| ≥40 | 714 (47.0) | 724 (48.1) | 1438 (47.5) | ||
| Education of mother | 1.900 | 0.387 | |||
| Primary school and below | 226 (14.9) | 206 (13.7) | 432 (14.3) | ||
| Middle school | 1007 (66.3) | 989 (65.7) | 1996 (66.0) | ||
| University and above | 287 (18.9) | 310 (20.6) | 597 (19.7) | ||
| Education of father | 0.908 | 0.635 | |||
| Primary school and below | 134 (8.8) | 119 (7.9) | 253 (8.4) | ||
| Middle school | 1027 (67.6) | 1034 (68.7) | 2061 (68.1) | ||
| University and above | 359 (23.6) | 352 (23.4) | 711 (23.5) | ||
| Household size | 6.907 | 0.009 | |||
| ≤4 members | 924 (60.8) | 844 (56.1) | 1768 (58.4) | ||
| ≥5 members | 596 (39.2) | 661 (43.9) | 1257 (41.6) |
| Variables | Males Median (IQR) | Females Median (IQR) | All Median (IQR) | Z Values | p Value |
|---|---|---|---|---|---|
| Anthropometric measurements | |||||
| Height (cm) | 152.1 (138.4, 168.0) | 152.0 (138.0, 160.3) | 152.1 (138.1, 162.6) | −5.826 | <0.001 |
| Weight (kg) | 45.0 (32.6, 59.4) | 42.2 (30.9, 52.1) | 43.5 (31.7, 55.3) | −6.791 | <0.001 |
| WC (cm) | 66.4 (59.1, 75.1) | 62.5 (56.1, 68.5) | 64.0 (57.7, 71.5) | −11.076 | <0.001 |
| SBP (mmHg) | 116.8 (108.3, 125.5) | 113.0 (105.3, 120.5) | 115.0 (106.7, 122.7) | −9.233 | <0.001 |
| DBP (mmHg) | 67.3 (62.0, 73.3) | 67.7 (62.7, 73.3) | 67.7 (62.3, 73.3) | −1.155 | 0.248 |
| Biochemical indexes | |||||
| FBG (mmol/L) | 5.29 (5.00, 5.59) | 5.16 (4.90, 5.45) | 5.22 (4.94, 5.52) | −7.172 | <0.001 |
| TG (mmol/L) | 0.77 (0.60, 1.06) | 0.83 (0.65, 1.09) | 0.80 (0.62, 1.06) | −5.747 | <0.001 |
| TC (mmol/L) | 3.95 (3.50, 4.49) | 4.03 (3.63, 4.54) | 4.00 (3.59, 4.52) | −3.282 | 0.001 |
| LDL (mmol/L) | 2.16 (1.80, 2.55) | 2.21 (1.88, 2.59) | 2.19 (1.84, 2.57) | −2.448 | 0.014 |
| HDL (mmol/L) | 1.56 (1.30, 1.84) | 1.60 (1.37, 1.87) | 1.59 (1.34, 1.86) | −2.801 | 0.005 |
| Serum uric acid (μmol/L) | 336.0 (276.0, 405.0) | 297.0 (254.0, 339.0) | 310.0 (260.0, 369.0) | −13.106 | <0.001 |
| Vitamin A (μg/mL) | 0.38 (0.32, 0.43) | 0.38 (0.32, 0.43) | 0.38 (0.32, 0.43) | −0.046 | 0.963 |
| Vitamin D (ng/mL) | 16.1 (12.8, 20.1) | 14.5 (11.4, 18.1) | 15.3 (12.0, 19.1) | −8.368 | <0.001 |
| Zinc (μg/dL) | 94.0 (87.0, 102.0) | 93.0 (85.0, 99.0) | 93.0 (86.0, 101.0) | −4.386 | <0.001 |
| Nutritional Status | Males n (%) | Female n (%) | Total n (%) | χ2 Values | p Value |
|---|---|---|---|---|---|
| Weight groups | 102.298 | <0.001 | |||
| Wasting | 96 (6.3) | 70 (4.7) | 166 (5.5) | ||
| Normal weight | 893 (58.8) | 1136 (45.5) | 2029 (67.1) | ||
| Overweight | 271 (17.8) | 176 (11.7) | 447 (14.8) | ||
| Obesity | 260 (17.1) | 123 (8.2) | 383 (12.7) | ||
| MetS | 6.215 | 0.013 | |||
| No | 1427 (93.9) | 1443 (95.9) | 2870 (94.9) | ||
| Yes | 93 (6.1) | 62 (4.1) | 155 (5.1) | ||
| Abdominal obesity | 18.075 | <0.001 | |||
| No | 1190 (78.3) | 1269 (84.3) | 2459 (81.3) | ||
| Yes | 330 (21.7) | 236 (15.7) | 566 (18.7) | ||
| High TG | 1.403 | 0.236 | |||
| No | 1304 (85.8) | 1268 (84.3) | 2572 (85.0) | ||
| Yes | 216 (14.2) | 237 (15.7) | 453 (15.0) | ||
| Low HDL | 3.160 | 0.075 | |||
| No | 95.3 (1448) | 1453 (96.5) | 2901 (95.9) | ||
| Yes | 72 (4.7) | 52 (3.5) | 124 (4.1) | ||
| Elevated BP | 0.159 | 0.690 | |||
| No | 887 (58.4) | 889 (59.1) | 1179 (58.7) | ||
| Yes | 633 (41.6) | 616 (40.9) | 1249 (41.3) | ||
| Elevated FBG | 15.868 | <0.001 | |||
| No | 1446 (95.1) | 1472 (97.8) | 2918 (96.5) | ||
| Yes | 74 (4.9) | 33 (2.2) | 107 (3.5) | ||
| Hyperuricemia | 194.297 | <0.001 | |||
| No | 897 (59.0) | 1236 (82.1) | 2133 (70.5) | ||
| Yes | 623 (41.0) | 269 (17.9) | 892 (29.5) | ||
| High LDL | 0.432 | 0.511 | |||
| No | 1451 (95.5) | 1429 (95.0) | 2880 (95.2) | ||
| Yes | 69 (4.5) | 76 (5.0) | 145 (4.8) | ||
| High TC | 7.727 | 0.005 | |||
| No | 1427 (93.9) | 1373 (91.2) | 2800 (92.6) | ||
| Yes | 93 (6.1) | 132 (8.8) | 225 (7.4) | ||
| Vitamin A | 0.049 | 0.976 | |||
| Sufficiency | 1285 (84.5) | 1272 (84.5) | 2557 (84.5) | ||
| Marginal deficiency | 222 (14.6) | 219 (14.6) | 441 (14.6) | ||
| Deficiency | 13 (0.9) | 14 (0.9) | 27 (0.9) | ||
| Vitamin D | 68.349 | <0.001 | |||
| Sufficiency | 383 (25.2) | 233 (15.5) | 616 (20.4) | ||
| Inadequacy | 835 (54.9) | 815 (54.2) | 1650 (54.5) | ||
| Deficiency | 302 (19.9) | 457 (30.4) | 759 (25.1) | ||
| Anemia | 31.863 | <0.001 | |||
| No | 1490 (98.0) | 1415 (94.0) | 2905 (96.0) | ||
| Yes | 30 (2.0) | 90 (6.0) | 120 (4.0) | ||
| Zinc deficiency | 3.417 | 0.065 | |||
| No | 1458 (95.9) | 1422 (94.5) | 2880 (95.2) | ||
| Yes | 62 (4.1) | 83 (5.5) | 145 (4.8) |
| Metabolic Syndrome | Hyperuricemia | Vitamin A Insufficiency | Vitamin D Deficiency | Anemia | Zinc Deficiency | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | AOR (95%CI) | p Value | AOR (95%CI) | p Value | AOR (95%CI) | p Value | AOR (95%CI) | p Value | AOR (95%CI) | p Value | AOR (95%CI) | p Value |
| Sex | ||||||||||||
| Males (reference) | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Females | 1.20 (0.83–1.74) | 0.331 | 0.30 (0.25–0.36) | <0.001 | 0.91 (0.74–1.12) | 0.378 | 1.80 (1.51–2.15) | <0.001 | 2.95 (1.93–4.51) | <0.001 | 1.33 (0.94–1.88) | 0.102 |
| Age group | ||||||||||||
| 7–12 years (reference) | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| 13–17 years | 1.79 (1.17–2.73) | 0.007 | 5.09 (4.13–6.27) | <0.001 | 0.34 (0.26–0.45) | <0.001 | 2.53 (2.09–3.08) | <0.001 | 1.82 (1.20–2.77) | 0.005 | 0.94 (0.63–1.41) | 0.774 |
| Living area | ||||||||||||
| Urban | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Rural | 0.76 (0.43–1.34) | 0.345 | 0.97 (0.75–1.25) | 0.796 | 1.24 (0.95–1.62) | 0.116 | 1.14 (0.89–1.44) | 0.298 | 1.43 (0.89–2.31) | 0.142 | 1.80 (1.21–2.68) | 0.004 |
| Weight group | ||||||||||||
| Others (reference) | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Overweight | 7.47 (4.26–13.11) | <0.001 | 1.94 (1.53–2.46) | <0.001 | 0.63 (0.46–0.87) | <0.001 | 1.02 (0.80–1.31) | 0.877 | 0.71 (0.39–1.28) | 0.255 | 0.78 (0.46–1.32) | 0.357 |
| Obesity | 41.14 (25.05–67.56) | <0.001 | 4.38 (3.38–5.67) | <0.001 | 0.37 (0.25–0.55) | 0.005 | 0.85 (0.64–1.13) | 0.269 | 0.37 (0.15–0.93) | 0.034 | 0.81 (0.45–1.44) | 0.466 |
| Physical activity | ||||||||||||
| Low | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| High | 1.31 (0.91–1.88) | 0.146 | 1.19 (0.99–1.43) | 0.061 | 0.93 (0.75–1.16) | 0.528 | 0.69 (0.58–0.83) | <0.001 | 1.07 (0.73–1.56) | 0.746 | 1.25 (0.89–1.77) | 0.204 |
| Screen time | ||||||||||||
| Low | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| High | 0.60 (0.33–1.10) | 0.097 | 0.91 (0.69–1.19) | 0.487 | 1.45 (1.09–1.94) | 0.011 | 1.40 (1.09–1.80) | 0.008 | 1.25 (0.73–2.13) | 0.420 | 0.78 (0.46–1.32) | 0.360 |
| Age of mother | ||||||||||||
| ≤36 | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| ≥37 | 0.93 (0.55–1.55) | 0.775 | 1.46 (1.13–1.89) | 0.004 | 0.78 (0.58–1.06) | 0.113 | 1.13 (0.88–1.45) | 0.349 | 1.34 (0.78–2.29) | 0.290 | 0.88 (0.53–1.45) | 0.621 |
| Age of father | ||||||||||||
| ≤36 | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| ≥37 | 0.97 (0.58–1.63) | 0.901 | 0.94 (0.73–1.23) | 0.668 | 1.07 (0.79–1.45) | 0.662 | 1.03 (0.80–1.33) | 0.788 | 0.75 (0.44–1.27) | 0.285 | 0.82 (0.49–1.36) | 0.443 |
| Education of mother | ||||||||||||
| Primary school and below | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Middle school | 1.08 (0.58–2.03) | 0.804 | 0.94 (0.71–1.25) | 0.693 | 0.64 (0.47–0.88) | 0.005 | 0.68 (0.52–0.89) | 0.004 | 1.27 (0.70–2.29) | 0.438 | 0.95 (0.58–1.56) | 0.847 |
| University and above | 1.09 (0.47–2.50) | 0.847 | 1.23 (0.82–1.83) | 0.315 | 0.55 (0.35–0.89) | 0.014 | 0.58 (0.40–0.86) | 0.006 | 1.03 (0.43–2.45) | 0.947 | 0.48 (0.20–1.16) | 0.104 |
| Education of father | ||||||||||||
| Primary school and below | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Middle school | 0.92 (0.45–1.87) | 0.817 | 0.86 (0.61–1.22) | 0.397 | 1.10 (0.74–1.64) | 0.626 | 1.17 (0.84–1.62) | 0.364 | 1.06 (0.51–2.20) | 0.886 | 0.72 (0.41–1.28) | 0.268 |
| University and above | 0.58 (0.24–1.40) | 0.228 | 0.63 (0.41–0.97) | 0.035 | 0.73 (0.43–1.22) | 0.223 | 0.97 (0.63–1.48) | 0.883 | 1.03 (0.51–2.20) | 0.942 | 0.47 (0.20–1.09) | 0.078 |
| Household size | ||||||||||||
| ≤4 members | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| ≥5 members | 1.20 (0.83–1.73) | 0.327 | 0.93 (0.77–1.12) | 0.465 | 1.20 (0.97–1.47) | 0.088 | 1.25 (1.05–1.49) | 0.014 | 1.10 (0.75–1.62) | 0.609 | 1.30 (0.92–1.83) | 0.136 |
| Overnutrition-Related Disorders | Undernutrition-Related Disorders | |||
|---|---|---|---|---|
| Characteristics | IRR (95%CI) | p Value | IRR (95%CI) | p Value |
| Sex | ||||
| Males (reference) | 1.00 | -- | 1.00 | -- |
| Females | 0.81 (0.51–0.85) | <0.001 | 1.33 (1.20–1.48) | <0.001 |
| Age group | ||||
| 7–12 years (reference) | 1.00 | -- | 1.00 | -- |
| 13–17 years | 1.44 (1.35–1.54) | <0.001 | 1.17 (1.04–1.32) | 0.008 |
| Living area | ||||
| Urban | 1.00 | -- | 1.00 | -- |
| Rural | 1.00 (0.91–1.08) | 0.939 | 1.21 (1.06–1.38) | 0.005 |
| Weight group | ||||
| Others (reference) | 1.00 | -- | 1.00 | -- |
| Overweight | 1.66 (1.53–1.79) | <0.001 | 0.86 (0.73–1.00) | 0.05 |
| Obesity | 2.77 (2.58–2.97) | <0.001 | 0.67 (0.55–0.81) | <0.001 |
| Physical activity | ||||
| Low | 1.00 | -- | 1.00 | -- |
| High | 1.05 (0.99–1.12) | 0.095 | 0.89 (0.80–0.99) | 0.027 |
| Screen time | ||||
| Low | 1.00 | -- | 1.00 | -- |
| High | 0.94 (0.86–1.03) | 0.202 | 1.23 (1.06–1.42) | 0.005 |
| Age of mother | ||||
| ≤37 | 1.00 | -- | 1.00 | -- |
| ≥38 | 1.07 (0.98–1.16) | 0.122 | 0.99 (0.86–1.15) | 0.946 |
| Age of father | ||||
| ≤36 | 1.00 | -- | 1.00 | -- |
| ≥37 | 0.98 (0.90–1.07) | 0.658 | 0.99 (0.85–1.15) | 0.852 |
| Education of mother | ||||
| Primary school and below | 1.00 | -- | 1.00 | -- |
| Middle school | 0.99 (0.90–1.08) | 0.759 | 0.81 (0.70–0.94) | 0.006 |
| University and above | 1.03 (0.91–1.18) | 0.631 | 0.68 (0.54–0.89) | 0.001 |
| Education of father | ||||
| Primary school and below | 1.00 | -- | 1.00 | -- |
| Middle school | 1.01 (0.90–1.13) | 0.913 | 1.04 (0.86–1.26) | 0.689 |
| University and above | 0.90 (0.77–1.04) | 0.135 | 0.83 (0.65–1.07) | 0.147 |
| Household size | ||||
| ≤4 members | 1.00 | -- | 1.00 | -- |
| ≥5 members | 1.02 (0.96–1.09) | 0.435 | 1.17 (1.05–1.29) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, T.; Wang, Y.; Xie, W.; Zhang, J.; Ni, Y.; Peng, X.; Sun, G.; Dai, Y.; Zhou, Y. Multilevel Analysis of the Nutritional and Health Status among Children and Adolescents in Eastern China. Nutrients 2022, 14, 758. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14040758
Tian T, Wang Y, Xie W, Zhang J, Ni Y, Peng X, Sun G, Dai Y, Zhou Y. Multilevel Analysis of the Nutritional and Health Status among Children and Adolescents in Eastern China. Nutrients. 2022; 14(4):758. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14040758
Chicago/Turabian StyleTian, Ting, Yuanyuan Wang, Wei Xie, Jingxian Zhang, Yunlong Ni, Xianzhen Peng, Guiju Sun, Yue Dai, and Yonglin Zhou. 2022. "Multilevel Analysis of the Nutritional and Health Status among Children and Adolescents in Eastern China" Nutrients 14, no. 4: 758. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14040758